Department of Pharmacy, KPGU Vadodara.
The rapid emergence and global spread of antimicrobial resistance (AMR) have significantly compromised the effectiveness of conventional antibiotics, posing a serious threat to public health worldwide. Multidrug-resistant (MDR), extensively drug-resistant (XDR), and pan-drug-resistant bacterial strains are increasingly associated with high morbidity, mortality, and healthcare costs. In this context, bacteriophage therapy has re-emerged as a promising alternative or adjunct to traditional antibiotic treatment. Bacteriophages are highly specific viruses that infect and lyse bacterial cells without harming normal human microbiota. Their unique properties including host specificity, self-replication at the site of infection, biofilm penetration ability, and adaptability to bacterial resistance make them attractive therapeutic agents. Historically discovered in the early 20th century, bacteriophages were widely used before the antibiotic era but declined due to limited scientific understanding and the success of antibiotics. Recent advances in molecular biology, genomic sequencing, genetic engineering, and regulatory standardization have revitalized interest in phage-based therapeutics. This review provides a comprehensive overview of bacteriophage therapy, including its historical development, biological structure, classification, mechanism of action, therapeutic applications, advantages over antibiotics, limitations, and future perspectives. Special emphasis is placed on its role in managing drug-resistant infections and its potential integration into modern clinical practice. Bacteriophage therapy, although not a complete replacement for antibiotics, represents a valuable complementary strategy in addressing the global antimicrobial resistance crisis.
Bacteriophage therapy, which uses viruses that specifically infect bacteria, was developed before the discovery of penicillin. One of its earliest applications was the treatment of infections such as Shigella dysenteriae in 1919.[1]. Bacteriophages are the most abundant living things, ecologically eliminating up to 40% of marine surface bacteria daily[2][3]. Early skepticism declined after electron microscopy in 1940.[4] Extensive antibiotic use has led to widespread resistance genes in the environment.[5] Antibiotic resistance, recognized by WHO and CDC as a major public health threat, causes millions of infections and deaths worldwide, with catastrophic impacts projected by 2050[6] [7] Carbapenems, the last line of defence, are losing effectiveness against K. pneumoniae, showing 40–50% mortality[8]. Bacteriophage therapy has re-emerged as a promising alternative, supported by advances and trials against multidrug-resistant infections[9].
What is Disease and How it Works
Defining disease is difficult, as even medical dictionaries lack a clear explanation. Since health itself is complex, disease cannot simply be its opposite. The WHO defines health as complete physical, mental, and social well-being, not merely the absence of disease.[10], A definition that has been criticized for being too idealistic [11]
Disease classification changes over time and context. Disease is shaped by ethical, cultural, and scientific frameworks as well as biology [12],[13],[14],[15],[16],[17]. It is classified as metabolic, genetic, environmental, or infectious. Metabolic syndrome combines interrelated risks like insulin resistance, type 2 diabetes, myocardial infarction, and stroke that greatly increase atherosclerotic cardiovascular disease risk.[18]. Metabolic syndrome involves central obesity, insulin resistance, hypertension, and dyslipidemia. Diagnosis requires at least three criteria: low HDL cholesterol, blood pressure ≥130/85 mm Hg, increased waist circumference, and triglycerides ≥150 mg/dL[19].[20][21], [22][23], [24][25][26]. Early intervention is crucial because timely lifestyle and treatment choices can stop disease progression and sometimes reverse it[27], [28].[29][30][31] The genetic basis of common diseases, like cardiovascular disease, involves complex inheritance, though some arise from single-gene mutations or chromosomal abnormalities[32]. The first protein-altering mutation, identified in the 1940s, involved sickle cell haemoglobin[33], [34].[35] In the 1960s, biochemical screening enabled detection of hereditary metabolic disorders like phenylketonuria without knowing genes[36].
In the 1970s–1980s, Sanger sequencing and recombinant DNA technologies emerged, enabling genetic analysis and leading to Huntington's disease sequencing in 1983[37]. Environmental factors likely cause 70–90% of acquired chronic diseases[38], [39]. Epidemiologists often rely on imprecise environmental questionnaires and GWAS, useful but limited by exposure measurement errors[40]. [41][42] [43]A “top-down” approach analysing blood for toxicants and biomarkers offers a feasible method over time. It targets classes like reactive electrophiles, endocrine disruptors, immune modulators, receptor binders, and metals[44], [45]. Studies linking blood chemicals to type 2 diabetes show exposomic effects comparable to major GWAS findings[46], [47]. [48] Infections are commonly caused by viruses, bacteria, or fungi. Viral infections range from the flu and common cold to chronic diseases like herpes. Unlike bacteria, viruses are acellular and require living host cells to replicate, taking over the host's cellular machinery to produce new viral particles. Due to this dependency, viruses are generally not viable outside a host, often breaking down within hours, whereas some bacteria can survive longer on surfaces. Viruses enter through sites like the respiratory tract, and sexually transmitted viruses, such as HIV and hepatitis C, spread via bodily fluids. Vaccination effectively prevents many viral infections, with some requiring periodic boosters for sustained protection.
Treatment
Viral diseases generally lack effective treatments, unlike bacterial infections, as antibiotics are ineffective against viruses. Some illnesses—herpes zoster, influenza, and hepatitis C have specific antivirals that reduce symptom severity and duration if administered early. Bacterial infections respond well to antibiotics, while viral infections rely on supportive care, prevention, and limited antivirals. Bacterial infections remain a major concern in clinical medicine, often arising endogenously from the host’s normal microbiota. While essential for health, this microbiota also serves as a reservoir for opportunistic pathogens. Antibiotics targeting causative organisms have been central to treatment for over 80 years. Despite the development of novel antibiotics in the 1960s and 1970s, resistant bacterial strains continue to emerge, threatening therapeutic efficacy. The spread of mechanisms like carbapenems, Metallo-beta-lactamases, and ESBLs signals a looming post-antibiotic era with limited effective treatments [49].
Bacterial Infections: An Overview of Epidemiology, Transmission, and Pathogenesis
Bacteria are ubiquitous microorganisms vital for ecological balance and environmental functions. Most are harmless, but a minority are pathogenic, posing significant public health challenges. Bacterial infections are generally more treatable than viral illnesses, yet rising antimicrobial resistance threatens therapy effectiveness. Bacteria play a dual role in human biology: many coexist as normal microbiota, while others act as opportunistic or overt pathogens. Disease manifests only in a fraction of exposures, with transmission occurring via soil, water, food, and biological vectors, depending on pathogen resilience and host vulnerability. Advances in microbiology continue to reveal new species, as seen with Lyme and Legionnaires’ diseases. Immunocompromised individuals, including those with HIV/AIDS or on immunosuppressive therapy, face heightened infection risk. Pathogenesis is multifactorial: infectivity, pathogenicity, and virulence influence disease, while host factors like age, genetics, nutrition, comorbidities and environmental conditions like pollution affect susceptibility[50].
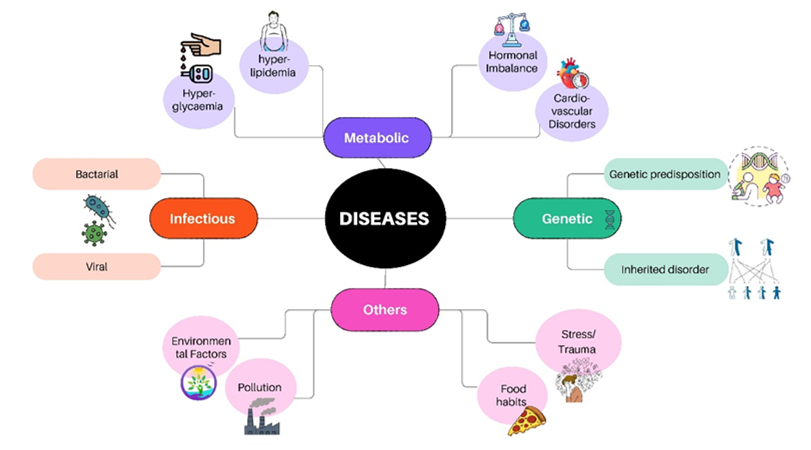
Figure 1 Types of Disease
Types of Diagnostic Tests for Identifying Infections
Microbial culture remains a fundamental laboratory method for detecting and identifying bacterial pathogens. In this process, a patient sample is inoculated onto a nutrient-rich culture plate, typically a Petri dish, designed to support bacterial growth. If bacteria are present, they multiply to form visible colonies; absence of growth indicates a negative result. Established colonies undergo further analysis through microscopy, biochemical assays, and staining procedures, such as Gram staining, to determine bacterial species based on characteristics like cell morphology and oxygen requirements. A crucial initial step in clinical diagnosis is distinguishing bacterial from viral infections, as antibiotics are ineffective against viruses. Clinical symptoms often overlap, making laboratory methods essential. Complete blood count (CBC), which measures white and red blood cells and platelets, can suggest bacterial infection when WBC levels are elevated. Specialized culture techniques vary by specimen and infection site. Blood cultures detect bacteria in the bloodstream, important for sepsis or osteomyelitis. Throat cultures identify Streptococcus pyogenes in upper respiratory infections. Sputum cultures aid in diagnosing pneumonia, tuberculosis, and sinusitis. Urine cultures isolate pathogens in urinary tract infections, while cerebrospinal fluid (CSF) cultures diagnose central nervous system infections, including meningitis and brain abscesses.
Treatments for bacterial infections are:
The discovery of antibiotics revolutionized medicine, providing effective treatment against infections that once caused high mortality. They remain central to medical practice due to their broad-spectrum activity. However, rising antibiotic-resistant bacteria, driven by misuse and overuse, along with notable adverse effects, present significant global challenges. This manuscript analyses antibiotics historically and presently, detailing classifications and side effects. It explores their complex interactions with human microbiota, including paradoxical effects on cancer, and investigates natural bioactive compounds with antimicrobial potential as promising alternatives to conventional antibiotic therapy[51].
Advanced treatment
With rising antibiotic resistance and limited new drugs, multidrug-, extensively drug-, and pan-resistant bacterial strains are emerging, raising concerns of a "post-antibiotic era" where common infections may be fatal. Nonantibiotic strategies are targeting virulence, altering the microbiome, and using bacteriophage increasingly explored. Historically, infections like endocarditis (100%)[52], meningitis (>95%)[53], pneumonia (30%)[54], and severe skin infections (10%)[55] were often fatal, underscoring WHO’s warning. Antibiotics’ declining efficacy has spurred interest in nonantibiotic treatments, excluding vaccines and immune modulation [56]. Anti-virulence strategies target bacterial factors that enable tissue invasion, cellular damage, and immune evasion, aiming to halt disease progression until clearance by the host or antibiotics. While thought less likely to induce resistance, some anti virulence drugs may still select resistant strains[57]. Toxins, including exotoxins and effector proteins, are targeted via chemical inhibitors or monoclonal antibodies, exemplified by raxibacumab against anthrax toxin, used alongside antibiotics[58]. Approval was largely based on animal studies, with limited human clinical evidence supporting optimal use. In Gram-negative bacteria, toxins produced in the cytosol are secreted through complex systems such as the type III secretion system (T3SS), which acts like a syringe to inject toxins into host cells. Because T3SS components are structurally conserved, their inhibitors may have broad-spectrum potential [59], [60]. Anti-PcrV agents showed promise: KB001 was safe but lacked clinical efficacy [61], [62]. while MEDI3902 demonstrated enhanced preclinical efficacy by targeting PcrV and Psl [63]. Multi-target anti-virulence strategies and combinations with antibiotics improved outcomes, even against resistant pathogens[64]. Biofilms further complicate treatment due to antibiotic tolerance and penetration barriers[65], [66] Although most approaches remain in preclinical development, strategies to combat biofilms primarily focus on preventing biofilm formation, disrupting established biofilms, or enhancing antibiotic susceptibility[67]. One effective preventative strategy is coating medical devices with antiadhesive materials. For instance, sulfobetaine polymer–coated catheters reduced S. aureus and E. coli colonisation in animal models[68]. While methylcellulose-coated implants inhibited biofilm formation in rat infection studies[69]. Targeting biofilm regulation pathways, such as intracellular c-di-GMP signalling and quorum sensing (QS), is another key approach. Blocking bacterial adhesins has also shown promise; the small molecule ZFH-04269 inhibited fimbriae-mediated adhesion of Uropathogenic E. coli, significantly reducing bacterial burden in murine urinary tract infection models[70]. QS inhibition, through synthetic AHL analogues or halogenated furanones, disrupts virulence gene regulation[71]. he furanone analogue C-30 reduced bacterial load in mouse lung infection models[72]. Similarly, M64, targeting P. aeruginosa MvfR, showed efficacy and synergy with ciprofloxacin[73], [74]. Two-component systems such as QseC are additional targets; LED209 suppressed virulence in several pathogens[75][76]. Transcriptional regulators like ToxT in V. cholerae were inhibited by virstatin and toxtazin B, reducing colonisation in mice[77], [78].
Bacteriophage
Introduction
Bacteriophages, sometimes referred to as bacteriophages, are viruses that only infect and proliferate within bacterial cells. Bacteriophage can be found in a wide range of environments and are believed to be the most common biological organisms on Earth [79]. The size, shape, and genome structure of bacteriophages vary remarkably. However, all bacteriophages have the same structure: a nucleic acid genome encased in a capsid of bacteriophage-encoded proteins that protects the genetic material and makes it easier for it to enter a host bacterium. A variety of bacteriophage forms, some of which resemble structures with "heads," "tails," and "legs," have been examined by scientists using electron microscopy. Bacteriophages are naturally non-motile and depend on Brownian motion to come into contact with their bacterial targets, despite these structural characteristics. Like other viruses, bacteriophages are highly specific to their hosts; they frequently only target a single species of bacteria or even specific strains of that species. A bacteriophage can start either the lytic or the lysogenic replication cycle after attaching to a suitable host [80]
Historical Background
Ernest Hanbury Hankin showed in the Annals of the Pasteur Institute in 1896 that the water from the Indian Ganga and Yamuna rivers contained a filterable agent that was fatal to cholera bacteria [81]. Frederick Twort suggested it was a secreted ferment in 1915 when he described a filter-passing agent that lysed micrococci but was unable to reproduce without bacteria. A similar agent that lysed Shiga bacilli and passed Koch's postulates was independently found by Félix d'Herelle in 1917 from patients with shigellosis. He named it a bacteriophage. Even though Bordet and Gartia were the main sources of the initial controversy[82] Clinical bacteriophage therapy, including intravenous use, was invented by d'Herelle, who also published trials all over the world [83]. Bacteriophage therapy for cutaneous infections was first reported clinically by Bruynoghe and Maisin in 1921. Although the nature of bacteriophages was still unknown in the early 20th century, scientists such as Wollman, Muller, and Macfarlane Burnet provided evidence for their viral nature. Ruska, Luria, and Anderson's EM studies visualised bacteriophages, and Schlesinger verified that they were nucleoproteins. Research was continued by Soviet and Polish institutions, but after the 1980s, interest increased internationally[84]. The bacteriophage Summit in 2004 signalled a renewed emphasis on [85], and bacteriophage-related literature has since expanded widely, covering 40 regions and 70 languages [86].
Biology and Structure of Bacteriophage
Bacteriophages are highly adapted to their local host community, according to their biology. By locating a suitable bacterial host, utilizing the metabolic resources of the host, and producing a large number of offspring that can survive until they come into contact with a new host bacterium, bacteriophages are structurally designed to efficiently carry out their biological functions. Bacteriophages are composed of single-stranded or double-stranded DNA or RNA, which is encased in a capsid protein. Bacteriophages can be classified into three main structural types: filamentous, icosahedral heads with tails, and icosahedral heads without tails [87].
Family of Bacteriophage
Small icosahedral bacteriophages belonging to the Leviviridae family infect bacteria like Pseudomonas, Acinetobacter, and Enterobacter. The coat protein, replicase, maturation protein, and lysis protein are the four vital proteins encoded by the linear, single-stranded RNA genome of these bacteriophages, which functions directly as messenger RNA [88]. This family is separated into two genera: Levivirus, which contains the species MS2 and BZ13, and Allolevivirus, which includes Qβ and F1.
The Microviridae family consists of small icosahedral bacteriophages with a single-stranded, circular plus-strand DNA genome. Inside the host cell, a complementary minus strand is produced to serve as a template for mRNA transcription. Members of this family infect obligatory intracellular bacterial parasites without a cell wall, like Spiroplasma or Chlamydia, as well as free-living enterobacteria [89]. Rod-shaped, filamentous bacteriophages with a single-stranded, circular plus-strand DNA genome are members of the Inoviridae family. Gram-negative bacteria are the main target of these bacteriophages [90]. Bacteriophages in the Cystoviridae family are distinguished by a nucleocapsid that contains segmented double-stranded RNA and is encased in a layer of lipid membrane. Pseudomonas species are the specific target of these bacteriophages[91]. Usually consisting of two icosahedral, concentric protein layers, the virion has an envelope. Double-stranded DNA bacteriophages, which are members of the Tectiviridae family, infect gram-negative bacteria. Similar to adenoviruses, they have an icosahedral capsid that encloses an internal membrane derived from the host. These bacteriophages are distinguished by the absence of tails, and the capsid is decorated with spikes at the fivefold symmetry axes[92]. The three main families of tailed bacteriophages that make up the order Caudovirales are Myoviridae, which has a long contractile tail; Siphoviridae, which has a long flexible tail; and Podoviridae, which has a short noncontractile tail. The icosahedral or prolate capsids of these Bacteriophages contain genomes made of linear double-stranded DNA [93]. Last but not least, bacteriophages with membrane envelopes that infect bacterial hosts without walls make up the Plasmaviridae family. Double-stranded DNA that is circular and supercoiled makes up their genome [94].
Mode of Action
Only a small number of studies have fully examined the pharmacokinetics of therapeutic bacteriophage preparations, despite the fact that there is a sizable body of literature on bacteriophage therapy [95]. According to the few reports that are currently available, bacteriophages can enter laboratory animals' bloodstreams after a single oral administration in as little as two to four hours, and by around ten hours after administration, they can be found in internal organs like the liver, spleen, and kidneys. Additionally, studies show that bacteriophages might stay in the body for a few days following administration.[96]. However, comprehensive pharmacological data, including in-depth toxicological evaluations, are still required before lytic bacteriophages can be approved for therapeutic use in Western medicine.
In terms of their bactericidal activity, therapeutic bacteriophages are typically thought to eradicate their target bacteria by replicating inside the host cell and lysing it through the lytic cycle. Further investigation has revealed that there are significant differences between the replication mechanisms of lytic and lysogenic bacteriophages, and that not all bacteriophages replicate in the same way. Decades of thorough research and developments like the full sequencing of the T4 bacteriophage genome (GenBank accession no. AF158101) have demonstrated that lytic bacteriophage-induced bacterial lysis is a complicated series of events controlled by several structural and regulatory genes. It is conceivable that numerous therapeutic bacteriophages adhere to a similar genetic and mechanistic pathway, since T4 is an example of a typical lytic bacteriophage. However, some might have distinct, as-yet-undiscovered genes or processes that enhance their bacteriolytic effectiveness. For example, EIBMV researchers[97] A gene from an anti-Salmonella bacteriophage that is crucial to the bacteriophage's deadly effect on Salmonella enterica serovar Typhimurium has been successfully found and cloned. In a different study [98], The ability of bacteriophage DNA to circumvent a Staphylococcus aureus host's restriction-modification systems were described as a novel mechanism. It is anticipated that further investigation into these and associated mechanisms will yield important information for the genetic engineering of extremely potent therapeutic bacteriophage formulations.
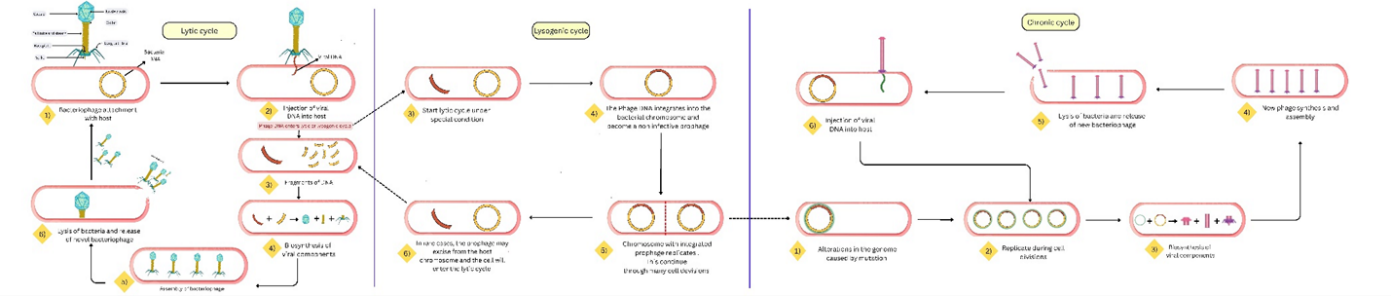
Figure 2 Mode of action of bacteriophage
Table 1. A comparative overview of antibiotics and bacteriophage based on treatment
|
Parameter |
Antibiotics |
Bacteriophages |
|
Origin |
Chemically synthesized or naturally derived from microorganisms |
Naturally occurring viruses that infect and lyse specific bacteria |
|
Mechanism of Action |
Inhibit bacterial processes (cell wall, protein or DNA synthesis) |
Infect specific bacterial cells, replicate inside, and cause cel lysis |
|
Target Specificity |
Broad- or narrow-spectrum; often non-specific |
Highly specific, typically targeting species or strains |
|
Impact on Normal Microbiota |
Can disrupt gut and skin microbiota; may cause dysbiosis |
Minimal impact due to host specificity |
|
Resistance Development |
High and growing concern due to widespread misuse |
Less likely, bacteriophages evolve alongside bactena |
|
Effectiveness Against Biofilms |
Often limited; poor penetration |
Effective; can replicate within and disrupt biofilms |
|
Side Effects |
Allergic reactions, gastrointestinal issues, organ toxicity |
Generally well-tolerated; immune responses rare |
|
Production and Formulation |
Mass-produced with standardized protocols |
Requires isolation and customizat-ion for specific bacterial strains |
|
Regulatory Status Therapeutic Role |
Approved worldwicle for clinical use First-line treatment for most |
Limited approval; mainly in research or compassionaate use |
Advantages of bacteriophage therapy over antibiotics
Decades before the discovery of penicillin, bacteriophage therapy the use of bacteriophages to treat bacterial infections began in 1919[99]. Despite their initial promise, bacteriophage therapy declined after the antibiotic revolution due to a lack of knowledge and inadequate clinical documentation. Bacteriophages are very common; there are 10³¹–10³² of them in the world [100], removing 20% to 40% of marine bacteria every day [101]. In light of the antibiotic resistance crisis, which the CDC and WHO have identified as a global health concern, their potential is resurfacing. Antibiotic-resistant infections result in at least 23,000 fatalities and $55 billion in expenses annually in the United States alone. Every year, 700,000 people worldwide pass away from resistant infections; by 2050, that number is expected to increase to 10 million [102]. More Americans are now killed by resistant pathogens like MRSA than by HIV/AIDS and TB combined [103]. Rapid resistance development has reduced pharmaceutical interest in new antibiotics; from 1983 to 1987, 16 new antibiotics were approved, but only 6 between 2010 and 2016 [104]. In the meantime, some infections now have 40% to 50% mortality rates due to increased resistance to last-resort antibiotics like carbapenems [105]. The benefits of bacteriophage therapy over antibiotics, such as its specificity, self-replication, biofilm penetration, and low toxicity, are highlighted by the renewed interest in this treatment [106]. Bacteriophage research is growing quickly thanks to developments in sequencing and microscopy, opening the door for new tactics to combat infections that are resistant to drugs [107].
Therapeutic Application of Bacteriophage in Disease Treatment
By using viruses that specifically infect and lyse harmful bacteria, bacteriophage therapy offers a promising antibacterial approach. The strong bactericidal action of lytic bacteriophages sets them apart from bacteriostatic antibiotics such as tetracycline. The therapeutic applicability of various delivery systems, such as liquids, microneedles, and electro spun fibres, has been improved by formulation advancements. Bacteriophages increase their therapeutic effect by self-replicating at infection sites. They are not very harmful to healthy plants and tissues because of their host specificity and the proteins and nucleic acids that make them up. Additionally, bacteriophages can be quickly obtained from bacterially rich environments, such as sewage, and circumvent traditional antibiotic resistance mechanisms.
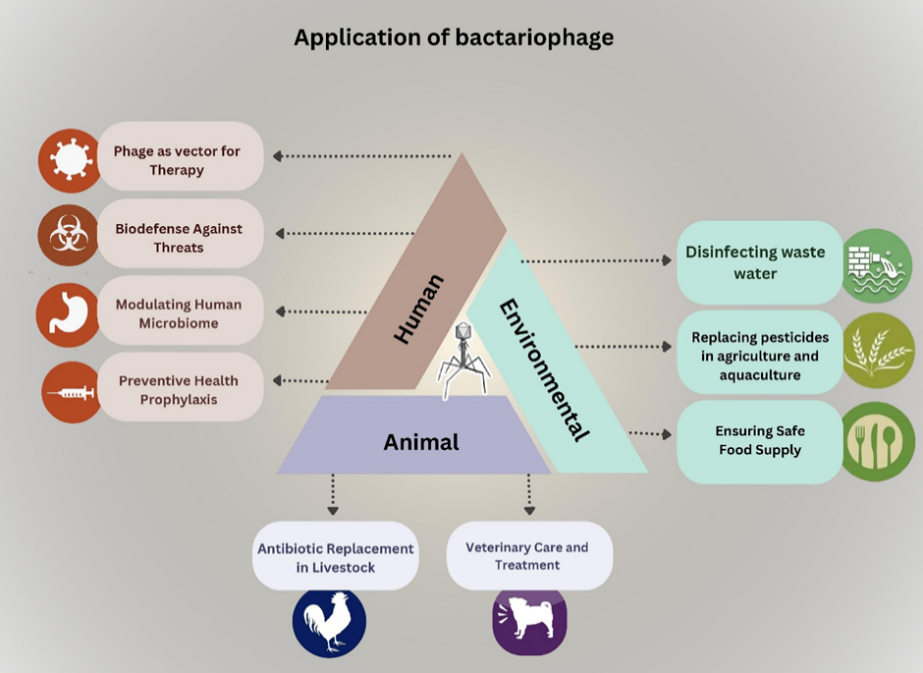
Figure 3 Application of bacteriophage
Infectious Diseases
Bacteriophage preparations were effectively used to treat cholera, bacillary dysentery, and other bacterial infections at the start of the 20th century, setting the stage for further therapeutic uses [108].Bacteriophage therapy was used to treat 1,307 patients with multidrug-resistant bacterial infections in a large clinical study at a Polish research institute; in 85.9% of cases, the patients experienced a clinical improvement or were cured[109].Faecal filtrate containing naturally occurring bacteriophages from healthy people has demonstrated efficacy in treating refractory Clostridium difficile infections in the gastrointestinal tract [110].Additionally, respiratory infections have been targeted. Dedrick and associates [111] revealed that a patient with cystic fibrosis who had Pseudomonas aeruginosa and Mycobacterium abscessus infections showed notable improvement after receiving a six-month course of treatment with a trio of bacteriophages. Regarding infections of wounds and abscesses, Schooley et al. [112] 68-year-old diabetic patient with multidrug-resistant Acinetobacter baumannii was treated. The infection was effectively managed by choosing nine bacteriophages and injecting them straight into the abscess cavity along with antibiotics. According to Bao et al., bacteriophage cocktail therapy was also successful in treating urinary tract infections brought on by sulfamethoxazole-resistant Klebsiella pneumoniae [113].Finally, Fabijan Petrovic et al. [114]used bacteriophage preparation AB-SA01 to treat 13 patients with severe Staphylococcus aureus infections, controlling the infection without causing any negative side effects. Inflammatory Bowel Disease (IBD): Patients with Inflammatory Bowel Disease (IBD) exhibit changed intestinal bacteriophage composition, such as a decrease in Faecali bacterium prausnitzii and an increase in tailed bacteriophages. This may be because bacteriophage-mediated lysis exacerbates inflammation [115].Alcoholic Hepatitis: Enterococcus faecalis, which produces cytolysin, is abundant in alcoholic hepatitis. In mouse models, bacteriophages that target these strains lessen liver damage, indicating potential for treatment [116].Diabetes Mellitus: Enterococcus faecalis, which produces cytolysin, is abundant in alcoholic hepatitis. In mouse models, bacteriophages that target these strains lessen liver damage, indicating potential for treatment [117], [118].Colorectal Cancer: Enterococcus faecalis, which produces cytolysin, is abundant in alcoholic hepatitis. In mouse models, bacteriophages that target these strains lessen liver damage, indicating potential for treatment [119].Breast Cancer: Enterococcus faecalis, which produces cytolysin, is abundant in alcoholic hepatitis. In mouse models, bacteriophages that target these strains lessen liver damage, indicating potential for treatment [120].Parkinson’s Disease A higher prevalence of virulent Lactococcus bacteriophages is associated with fewer bacteria that produce dopamine, which may accelerate the course of the illness [121].Schizophrenia: Patients with schizophrenia have higher levels of Lactobacillus bacteriophage phiadh, particularly those who do not take sodium valproate, which suggests a connection between the presence of the bacteriophage and the course of treatment[122].
Table 2 Family of bacteriophage
|
Study |
Infection(s) Treated |
Etiologic Agent(s) |
Key Findings / Comments |
|
Babalova et al. |
Bacterial dysentery |
Shigella |
Shigella specific bacteriophages succsesssfullyused for prophylaxis. |
|
Bogovazova et al. |
Skin and riasal mucose |
K. exaenee, K. rhinoscleromatis, K. pneumoniae |
Adapted bacteriophages effectively treated 109 patients. |
|
Cislo et al. |
Postoperative-infections in carrier patients |
Staphylococcus, Straptococcus, E. coli, Proteus |
74% success rate in 31 patients treated orally or topically. |
|
Kochetewicz-Kruikowcka & stopak |
Various infections |
Staphylococcus, and Pseudomonas |
84% success rate in 131 poisonings be 6% success rate for 61% success rate vs. antibiotics-resistant bacteriophage treatment. |
|
Kwarcinski et al. |
Recurrent subphrenic a bcess |
E. coli |
Successfully tried improvement with bacteriophages. 48 %6 and 830. |
|
Meladze et al. |
Intestinal dysbacteriosis |
E. coli and Proteus |
82.n recovery in 223 patients with Bacteriophage-bilditomera therapy unretrieved infection in 92% of 299. |
|
Milutina & Vonoyltseva |
Perifionitis, osteomyelitis, tongue abscesses surge infections |
Shigella and Salmonella |
Eliminating infection in 92% of 235 antibiotic-resistant infections. in 235 ammonceni-listas. |
|
Sakanedelidze |
Infectious allergises (rhinitis, pharyngeal dermatitis, dermatitis) |
Staphylococcus, E. coli, Proteus, Salmonella |
1,280 cases: 86% improvement with bacteriophages, 48 % with antibiotics, and 83% with combination therapy in 1,330 cases in 550-patients. |
|
Slope-et al. |
GI, skin, head, and neck infections |
A. pneumoniae |
Successfully interfered a new born after failed anti-biotics with bacteriophage treatment internat. |
|
Strol et al. |
GI, skin, head, and neck infections |
Staphylococcus, Pseudomonas |
Outperformed antibiotics in $8 immunosuppressed leukaemia patients with suppurative infections in 92%. |
|
Weber-Dabrowska et al. |
Suppurative infections gram-negative |
– |
Oral bacteriophages successfully treat 55 patients, reaching tream antibiotic-resist infections. |
|
Zhukov Verezhnikzv et al. |
Suppurative infections |
E. coli, and Proteus |
Comparison of patient and phiche bacteriophages superior to commercial preparations in 60 cases in Performa commercial preparations. |
Limitations of Bacteriophage Therapy (PT):
The limited host range of bacteriophages limits their effectiveness against polymicrobial infections, one of the many drawbacks of bacteriophage therapy [123]. Lysogenic bacteriophages can transfer virulence or resistance genes and prevent lysis [124]. Standardisation and quality control are hampered by the intricacy of PT formulations [125]. Clinical adoption is further complicated by regulatory gaps and a lack of standardised isolation and purification procedures [126]. Through processes like adsorption inhibition and CRISPR-Cas systems, bacteria develop resistance to bacteriophages [127]. Furthermore, dosage optimisation is made more difficult by a lack of pharmacokinetic data [128]. Safety concerns are also raised by bacteriophage-induced endotoxin release and possible immunological reactions [129], lacking enough RCTs to substantiate clinical efficacy [130].
How to overcome?
Several tactics are used to get around bacteriophage therapy's (PT) drawbacks. Bacteriophage cocktails are used to address the limited host range [131], Bacteriophage libraries as well as thorough host screening [132] By altering binding proteins, genetic engineering increases host specificity. To prevent lysogeny, lytic bacteriophages are favoured. Endolysins improve quality control and antibacterial efficacy [133]. Standardising PT procedures requires the establishment of regulatory frameworks [134]. Bacteriophage and antibiotic combination reduce resistance and produces synergistic effects [135]. Bacteriophage protection in harsh environments is achieved by optimising delivery methods through encapsulation [136]. To treat uncommon immune or endotoxin-related reactions, clinical monitoring is crucial [137].
Future Perspective
It is anticipated that future technological developments will resolve the present difficulties in patenting bacteriophage-based preparations. Such advancements could improve PT's accessibility and specificity. The creation of bacteriophages that specifically target antibiotic-resistant bacterial strains while preserving the host's commensal microbiota is made possible by genetic engineering techniques like high-throughput sequencing, CRISPR/Cas-mediated bacteriophage modification, homologous recombination, and bacteriophage genomic DNA assembly. These genetically modified bacteriophages or bacteriophage cocktails have unique properties that could make them easier to patent and sell. Many research teams and PT centres around the world are building extensive bacteriophage libraries to guarantee prompt access to therapeutic bacteriophages. Bacteriophage-based therapeutics must be manufactured using strict and verified quality control procedures, regardless of production scale, whether for customised treatment or wider clinical use. Strict evaluation is required of crucial factors like sterility, stability, and the presence of endotoxins, exotoxins, or other potentially dangerous contaminants [138], [139], [140], [141]. Researchers and clinical experts generally agree that bacteriophage therapy will not completely replace antibiotics, despite the fact that bacteriophages have been suggested as "living drugs" and potential all-purpose cures. Instead, bacteriophages are thought of as supplemental agents that can be used in conjunction with traditional antibiotics or as salvage therapy for infections that are resistant to conventional therapies. The therapeutic value of PT and other alternative antimicrobial strategies deserves renewed attention in light of the rising prevalence of multidrug-resistant (MDR) infections, which are primarily caused by the overuse and misuse of antibiotics. In particular, Bacteriophage therapy should be re-examined as a feasible alternative in contemporary Western medicine[142], [143].
CONCLUSION
Bacteriophage therapy represents a scientifically sound and clinically promising approach in the fight against antibiotic-resistant bacterial infections. With their high specificity, ability to disrupt biofilms, minimal impact on commensal microbiota, and self-amplifying nature, bacteriophages offer distinct advantages over conventional antibiotics. Despite existing challenges—such as limited host range, regulatory complexities, potential bacterial resistance to phages, and insufficient large-scale randomized clinical trials—ongoing advancements in genetic engineering, phage cocktail development, formulation technologies, and quality control standards are steadily addressing these limitations. Rather than replacing antibiotics entirely, bacteriophage therapy is best envisioned as a complementary or salvage treatment strategy, particularly for multidrug-resistant infections. As antimicrobial resistance continues to rise globally, renewed research investment, standardized regulatory frameworks, and robust clinical trials are essential to fully integrate bacteriophage therapy into modern Western medicine. With continued scientific progress, phage therapy holds substantial potential to reshape the future of infectious disease management.
REFERENCES





Jhanvi Surti, Nipurna Vora, Rutu Parmar, Jay Jivani, Sneh Sinojia, Dr. Jigar Vyas, A Brief Overview of Phage Therapy: A Resurgent Antibiotic Alternative, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3428-3448. https://doi.org/10.5281/zenodo.19245929
 10.5281/zenodo.19245929
10.5281/zenodo.19245929
