
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
The Oxford College of Pharmacy, 1st cross, Hongasandra, Bengaluru, Karnataka 560068
Hypertension is an issue rising globally owing to ageing of population, due to various life style risk factors. Multilayer, fast disintegrating tablets and nanoparticles are some of the approaches to combat hypertension. TDDS is an ideal approach to treat hypertension with several advantages like sustained release of drug, non-invasive, and increased patient compliance. Skin is a complex barrier for delivery of drug through transdermal route as it composed of many layers like epidermis, dermis and hypodermis. A transdermal patch is composed of active ingredient and various excipients which is affected by different parameters like thickness, solubility, molecular weight, age, drug content etc. Iontophoresis, electrophoresis, sonophoresis, microneedle are future aspects of transdermal drug delivery system. It also delivers biologics in various applications. With an emphasis on its potential to completely transform the treatment of numerous illnesses, the advantages and difficulties of transdermal drug delivery systems are discussed. All things considered, TDDS is major development in medication delivery that may enhance quality of life and treatment results.
Rise in blood pressure is an ailment which affects the majority of the people globally, the ideal blood pressure of a normal healthy individual is 120/80 mm/Hg. This level might increase due to various reasons like improper food habits, smoking, consumption of alcohol, lack of sleep and physical activity. Since high blood pressure is a chronic health disorder that requires long time care, so it is frequently regarded as silent killer, since it can lead to liver disorders and heart failure. The united nations agency dedicated to global health and safety estimates that raised blood pressure might be the main reason for early death globally, it is identified that by the year of 2025 1.5 billion youngsters will be living with raised blood pressure. [1]
There are different dosage forms available for treating hypertension some of them are:
Multilayer Tablet – multilayers tablets are a significant advancement in a drug delivery technology, designed for controlled release and combining different drug functions. They are significant in preventing incompatibilities, controlling release rate of drug, cost effective, precise dose. These multi-layered tablets are ideal for chronological release of two drugs from one pharmaceutical form for obtaining sustain release of drug. The outer layer serves as immediate release as loading dose, and the other layer releases the maintenance dose. [2]
Fast Disintegrating Tablets – these tablets disintegrate rapidly in the oral cavity without the need of excess water. These tablets are prepared by wet granulation technique by using super disintegrants like SSG (sodium starch glycolate), it was mainly developed for management of pediatric hypertension [2]
Nanoparticle – nifedipine is mainly used for treating hypertension but because of its short half-life and delayed onset of action it is formulated into nifedipine nanoparticle by using different polymers like Eudragit RL/RS, polyethylene glycol. [3]
Transdermal drug delivery systems (TDDS) are devices that hold the active ingredients across specific surface area, allowing for the controlled release of a set quantity of the active ingredient onto the skin’s surface at a specified rate. The market of transdermal medicine delivery is worth billions of dollars. Since the food and drug administration authorized the first transdermal medication patch about 40 years ago, a thorough analysis of the goals, industry, and technology is warranted. Patches are a novel method that enable on demand transdermal medication delivery systems. The main purpose of selecting TDD in the form of a patch is for specific biological characteristics. A drug candidate that has difficulty in administering percutaneously. Such properties include high first pass metabolism, high Lipophilicity (log P 3.97), and low molecular weight (406.5). Refers to the ability to pass through the lipophilic skin barrier. [4]
There are few advantages associated with TDDS when compared with other dosage form: Evade pre systemic metabolism, sustained release of drug from dosage form, patient conformity, enhanced availability of drug, non-invasive, minimizes needle related discomfort.[5]
Anatomy and Physiology of Skin
Our understanding regarding the skin construction is typically 2D, stable, and mostly focus on bodily functions. The integumentary system acts as a covering to the body and undercovers the blood vessels, lymphatics, nerves, and the flexor retinaculum. Skin is segregated from the craniofacial bones and subcutaneous tissues by deconstruction. Which are falsely formed through regions of connective tissues that are weakly connected, these tissues are necessary for migration across tightened muscles [6]
The skin is composed of two main layers, where the lower layer is the dermis and the upper layer is the epidermis, they are bilayered that are divided with a basement membrane[10]. The epidermis is made up of 5 layers the outermost layer is the stratum corneum, it is the layer which is exposed to the external environment deepest layer of the epidermis. Stratum corneum consist of 15 to 30 layers of dead cells which prevents penetration of organisms and dehydrates the underlined cells and tissues, these dead cells will slough periodically and are displaced by cells which are pushed from the stratum granulosum. It also consist of stratum lucidum which is restricted to only particular parts of the body like soles of the feet, palms, and the finger tips, and the other layers are stratum granulosum, the stratum basale and the Stratum Spinosum. The stratum corneum is denser as it is made up of lost cells called carneocytes that are embedded in the lipid layer which forms the formidable physical barrier. The dermis layer is further parted into two layers the stratum paillare and stratum reticulare and these are made up of thick and thin collagen fibres. [7]
Dermis is considered as the core of cutaneous system which consist of lymph vessels, blood, nerves, sweat glands, and hair follicles. The dermis layer is composed of two layers of connective tissues these connective tissues consist of fibroblasts which produces elastin and collagen fibres. [7]
The hypodermis, commonly known as subcutaneous tissue, is a layer made of elastin and areolar tissue that acts as insulator against cold temperatures, a shock absorbent, and a store of nurtients and energy. In the palms of the hands, soles of the feet, and the buttocks, the hypodermis is thickest. The thin, wrinkled appearance of aged skin is a result of the hypodermis declining with age. The skin’s immune system is made up of innate and adaptive immune cells, which includes mast cells, macrophages and advanced specialized antigen – presenting cells and epidermal dendritic cells. [6]
Our skin has variety of functions some of them are:
The importance of skin cannot be overemphasized, as it plays a crucial role in holding water and other essential molecules inside the body.
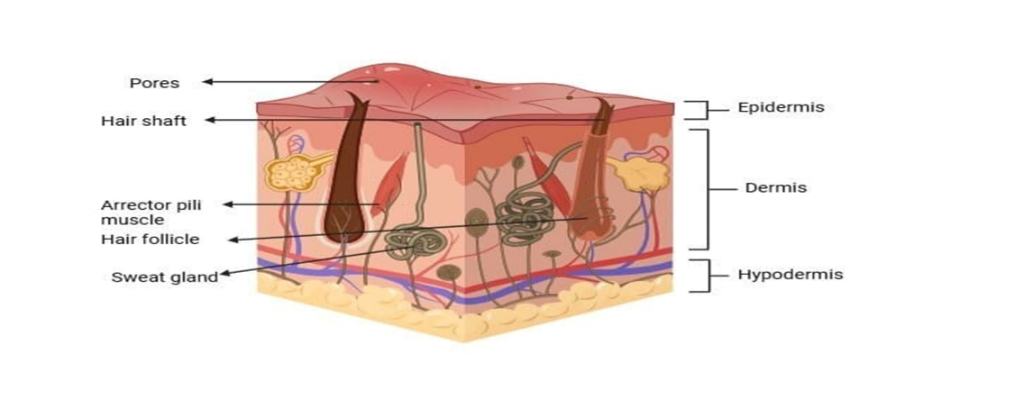
Figure 1: structure of skin (created with biorender.com)
MECHANISM OF DRUG PERMEATION THROUGH SKIN
Delivery of the drug through the skin’s topical layers is considered as the most suitable method for lifelong and universal treatment, various types of patches can be formulated which makes them ideal for delivery of dosage form for a longer period of time. A particle can penetrate through the skin by following two diffusion pathways: the trans epidermal pathways and the other pathway is appendageal. For the permeation of ions and large polar molecules the appendageal pathway is the optimal one, whereas for the permeation of unionized molecules the trans epidermal pathway is ideal. A molecule must be lipophilic in nature and must have an ideal molecular weight of (<400Da) in order to show good skin penetration. Hydrophilic drugs separate through the intercellular province, while the lipophilic drugs cross the subcutaneous layer through the intercellular province. Majority of molecules cross the stratum corneum using both ways. However permeation of most of the drug molecules is restricted due to the barrier functions of the epidermis. To overcomes these challenges penetration enhancers are used. [8]
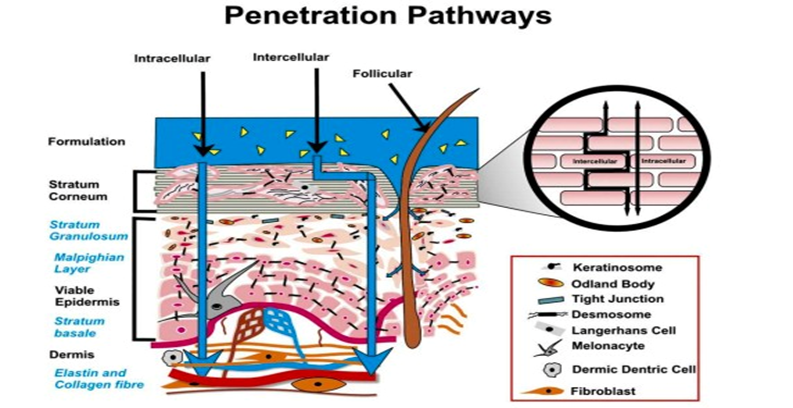
Figure 2: Mechanism of drug penetration
COMPONENTS OF TRANSDERMAL PATCH
Primary constituents of transdermal patch
Drug – the drug which will be selected for the development of transdermal patch must meet the required physiochemical and pharmacokinetic properties. Like the drugs that have t1/2 of less than 10hr and that undergoes rapid first pass metabolism, molecular weight <400 Da and melting point <200 degree Celsius are best for patch formulation. [9]
Polymer matrix – the main component for transdermal delivery are polymers, which are multi-layered polymeric laminates, where polymer matrix drug or drug reservoir is placed between the polymeric layers. The outermost layer is known as the impermeable backing layer as it prevents drug loss from its surface, and the inner layer is known as the adhesive which controls the rate and amount of drug release. The polymers which are used in the designing of transdermal patch must be selected properly and it should meet the required criteria. [9]
Various types of polymers can be used like cellulose derivatives, gelatin, waxes, gums, silicon rubber, nitrile, acrylonitrile, polyvinyl alcohol, polyvinylchloride and polyethylene etc.[9]
Permeability enhancer – in order to enhance the permeability of drug through the stratum corneum and to achieve increased therapeutic levels of drug permeation, these penetration enhancers react with the proteins and lipids of stratum corneum which will be the main structural component. These permeability enhancers are soluble and miscible in nature which has advantage of improving the transdermal permeability of hydrophilic drugs.
There are various permeation enhancers like, Nerodilol, menthol, Oleic acid, linoleic acid, ethanol and propylene glycol etc. [10]
Pressure sensitive adhesive – these PSA are mainly used to increase contact time between the skin and patch surface, the patch should adhere to the skin surface with a pressure not more the applied finger pressure, PSA must be compatible both biologically and physicochemical with the drug and must not alter the release of drug. PSA and be attached either in the front or the back of the patch. There are variety of factors like design of patch and formulation of drug based on which the adhesive must be selected. [10]
Backing laminate – backing laminates play a critical role in providing structural support. It is necessary for the backing laminate to be chemically resistant and to be compatible with the excipients, when the backing layer is not compatible with the excipients it might lead to leaching of excipients, because the drug and permeability enhancers should have a longer duration of contact with each other. Backing laminate must have moisture vapour transmission rate will be low, along with flexibility, optical elasticity and tensile strength. Some examples of backing layer are heat seal layers, aluminium vapour coated layers, plastic films such as polyvinyl chloride and polyester. [11]
Release liner – before the application of the patch on the skin a protective layer is removed and thrown that layer is known as release liner. Since the liner is in direct contact with the outermost layer of skin, hence they should be chemically stable. This liner is made up of 2 layers where one layer is non occlusive (paper fabric) and occlusive (polyethylene) which is the base layer, and the other layer is release agent which is made of silicon or Teflon. [11]
Plasticizers – 5 to 10% of plasticizers are used in the designing of transdermal patch in order to improve the tensile strength and elasticity of the film, it is also used to enhance the attachment of the film to skin’s outer layer. Most frequently used plasticizers are glycerol or sorbitol. The permeability and mechanical properties of the drug are directly proportional to the plasticizer chosen and its concentration. [11]
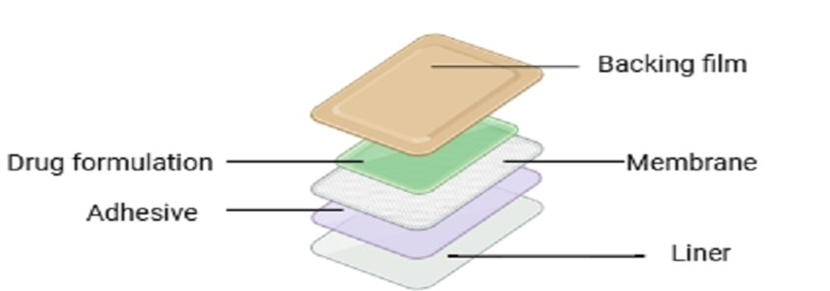
Fig 3: components of transdermal patch (created with biorender.com )
Factors Affecting Transdermal Permeability
Physical and Chemical Properties
Molecular size – drug molecular size is indirectly proportional to the transdermal flux, and the required particle size of a drug for delivery through skin is less than 400.[12]
Solubility – the ability of chemical to separate into the stratum corneum is the major factor affecting the relationship between solubility and the rate of skin absorption. A chemical will not divide into the stratum corneum primarily lipid atmosphere if it is overly hydrophilic. A chemicals solubility is often determined by how well it partitions into two immiscible liquids, like water and methanol. The most widely used metric for assessing solubility is the octanol-water partition coefficient. [12]
Charge – protiens like keratin gave the stratum corneum both positively and negatively charged groups. This property when combined with the stratum corneum’s lipid atmosphere, it creates an effective barrier against charged molecules. These ions are poorly absorbed across the stratum corneum. [12]
Volatility – it can have an significant impact on the rate and degree of skin absorption influencing how long a chemical stays in contact with the skin. the relationship between systemic toxicity and a substance’s volatility within a chemical series is especially evident for highly poisonous substances like chemical warfare agents. [12]
Hydrogen bonding – the stratum corneum’s protein and lipid composition results in an plenty of hydrogen bonding groups, if the penetrant has supportive hydrogen bonding groups, these can develop reversible bonds with chemicals as they penetrate the stratum corneum. A chemical that participates in hydrogen bonding within the stratum corneum may undergo a delay in its diffusion through that layer. [12]
Partition coefficient – log k in the range of 1-3 is ideal for intermediate drug delivery, (log k>3) is suitable for drugs are highly lipophilic in nature and (log k<1) is ideal for water attracted drugs. [12]
Melting point – the majority of organic solutes are poorly soluble at room temperature and pressure, and they have a high melting point. A lipophilic drug should have aqueous solubility are required in the majority of topical formulations, but it also penetrates more quickly than hydrophilic substances. [12]
Ionization – as stated by the pH partition hypothesis unionized drug penetrates to the skin. [12]
Diffusion coefficient – the drugs mass diffusivity discovers its permeation. The features of the drug, the dispersal medium, and their reaction discovers the drugs mass diffusivity at stable temperature. [12]
Composition of drug delivery system- compilation might not influence the release properties but might influence its permeability functionality. Methyl salicylate for example is more lipid attracted than parent acid that is salicylic acid, and its transcutaneous absorption is maximum when administered to skin in a lipid vehicle. [12]
Skin hydration – when the skin is exposed to water it increases its permeability remarkably. Moisturizing is the most necessary factor in order to enhance skin permeation. So it is necessary to use humectant for transdermal delivery. [13]
Drug concentration - transdermal flux is directly proportional to concentration difference across the barrier and the concentration difference will be more when the drug concentration will be maximum across the obstacle. [13]
Biological factors
Skin condition- solvents like chloroform, methanol might destroy the skin tissues and increases permeation through the skin. disease state might affect the skin condition, intact skin show better skin permeability. [14]
Skin age- maximum drug absorption through skin is widely observed in young childrens because their skin is high sensitive and quick to respond hence skin age is one of the important factors affecting skin permeation through skin.[14]
Blood flow – any change in the peripheral circulation of blood it will affect drug permeation through skin. [14]
Skin metabolism – some drugs, hormones, steroids, chemical carcinogens are metabolized by skin metabolites, hence skin metabolism identifies efficiency of drug penetrated through skin.[14]
Site of application- skin density, stratum corneum nature and thickness of appendages differ from one site to another. So these factors might also affect skin permeability. [14]
Challenges associated with transdermal patch
Shailesh T et al., (2011) formulated a transdermal patch for controlling blood glucose level. In this study they have used repaglinide as an anti-diabetic drug that has an half life of 1hr, due to which it needs to be administered 4 times a day. In order to overcome this disadvantage they have formulated transdermal patch. They have increased the bioavailability and provided sustained release of the drug by using different grades of HPMC polymers and concentrations of PVP by solvent casting method. It was observed that batch f6 is the optimized batch that contains HPMC K100 and PVP (1.5%) it showed drug release of 92.342% up to 12hours.[15]
Priyanka Arora et al., (2002) developed a transdermal patch were diclofenac is used as the drug in order to treat arthritis, musculoskeletal disorders and dysmenorrhea. Diclofenac has a disadvantage of undergoing rapid hepatic first pass metabolism due to which only 50% of administered dose can reach the blood stream so in order to overcome this problem they have used different of PVP and EC (ethylcellulose) by a technique called solvent evaporation. It was observed that there was variation in the in-vitro release and permeation studies of drug release among the different formulations.[16]
Prabhakar Prabhu et al., (2011) designed domperidone transdermal patch which is a dopamine antagonist that gives antiemetic activity. Domperidone has a low bioavailability of 15%, which indicates that it must be administered frequently in order to increase the bioavailability and reduce dosing frequency they formulated patches by using the polymers polyvinylpyrolidone and HPMC, Carboxymethyl cellulose in combination. It was observed that the prepared patch release 33% of drug at the end of 24hours.[17]
Bazigha K et al., (2021) developed transdermal patch that contains dimenhydrinate which is a drug that is used to provide relief from nausea, vertigo, and vomiting caused by motion sickness. This drug has low bioavailability because of its rapid hepatic first pass metabolism so in order to increase the bioavailability, reduce dosing frequency and increase patient compliance it is fabricated into a patch.[18]
Monika Bhairam, et al., (2023) formulated transdermal patch by using the drugs Losartan Potassium and Glipizide in combination so that dual effect can be achieved. The main objective of this research is to formulate a single dosage form which can be used to treat both the conditions at the same time. By using the polymers HPMC, ethyl cellulose, EG L100 and poly vinyl pyrolidone matrix type patches were prepared by solvent evaporation method. It was concluded that Glipizide and Losartan potassium combined in a transdermal delivery system may be a game changer for the management of hypertension and diabetes.[19]
Long Mo, et al., (2022) developed carvedilol incorporated transdermal patch, carvedilol undergoes rapid hepatic first pass metabolism which results in low bioavailability in order to overcome this problem they have fabricated transdermal patch by using solvent evaporation technique by using the polymers EU RS 100 and span 80 was used as permeation enhancer. The result obtained from this research was observed that formulation 7 showed maximum drug release of 100.29 within 12hr and it also showed highest bioavailability and maximum drop in BP at 6 hr.[20]
Ibrahim Alissa, et al., (2023) designed an adhesive transdermal patch, which is used to provide relief from pulmonary arterial hypertension. The drug which is used in the patch formulation is treprostinil that has a low bioavailability due to which it needs to be administered frequently in order to overcome this problem they have developed a transdermal patch. Comparing transdermal therapy to oral dosing, the former led to greater treprostinil ansorption (p<0.0001) and relative bioavailability (237%). All things considered, the findings show that medication created for the adhesive patch may efficiently transfer terprostinil through the skin and may be a viable treatment for pulmonary arterial hypertension.[21]
V.Vijayan, et al., (2010) designed transdermal patch containing the drug losartan potassium, it was prepared by using aquaphilic and aquaphobic polymers by solvent evaporation method. This drug is rapidly metabolised by the liver due to which it has a bioavailability of 33% in order to increase the bioavailability and reduce dosing frequency and increasing patient compliance they have formulated it into a patch by using the excipients like HPMC, Eudragit RS100, tween 80 and span 80. It was observed that the patch containing the polymers Eudragit RS100 and HPMC exhibited adequate drug release.[22]
Rabinarayan Parhi, et al., (2016) formulated diltiazem HCL transdermal patch by using solvent casting technique. In this study different ratios of polymers like HPMC K4M and Eudragit RS100 were used. DTH has a half life of only 3-5hours and it is rapidly metabolised by the liver which indicated a low bioavailability of only 40%, so to increase the bioavailability they fabricated it into a patch. It was concluded that f9 formulation containing the polymers HPMC K4M and Eudragit RS100 showed constant arterial blood pressure for 10hr and it also improved permeation profile for longer period of time and therefore enhancing patient compliance.[23]
Future Prospects of Transdermal Patch
Iontophoresis – in order to enhance the permeability of drug that is applied topically, iontophoresis technique is used where low electric current is applied either indirectly through the dosage form or directly to the skin surface. There are two main mechanisms (electro-pertubation for uncharged solutes and electro-osmosis for charged solutes that is responsible for increasing the drug permeability. Iomed Inc., developed the Phoresor device which is one of the iontophoretic systems that is undergoing development commercially.[25]

Fig 4 : schematic diagram of iontophoresis[26]
Electroporation – it is a technology where high voltage current is applied to the skin surface which results in formation of temporary pores, the treatment duration is restricted to milliseconds with a high voltage of 100V. waveform, rate and number are the electrical factors which forms the main characteristics of pulse which influence the permeability rate. This technique is applied to enhance the skin permeation for those molecules which vary in their lipophilicity and molecular size including biopharmaceutical molecules which have high molecular weights of more than 7k Da for example proteins, oligonucleotides, peptides.[27]
Abrasion – the abrasion technique is mainly used to remove the outermost layers of epidermis so the medicament which is applied topically permeates into the skin. dermatologist use microdermabrasion to treat skin imperfections like scars, acne and hyperpigmentation.[24]
Microneedle – based devices – this system has a micron scale array of length up to 1000 micrometer, these microneedles are enclosed in a substarte for transdermal delivery with obstructing the dermis. Water soluble molecules permeate the dermis layer because micropores are formed by puncturing of microneedles in order to reach the systemic circulation. The selection of excipients for microneedle formulation dominates the unique features and uses of the device. [28]
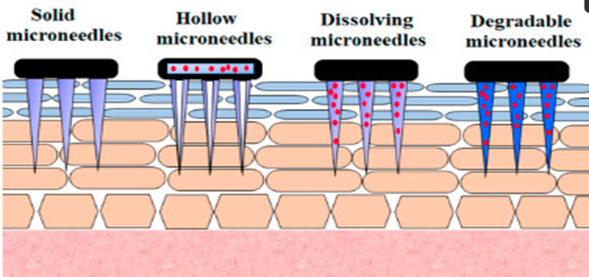
Fig 5: schematic diagram of microneedle [28]
Sonophoresis – to mitigate the likelihood of accidental needle injuries and the spread of infectious diseases, advanced non- invasive drug administration techniques have been engineered, such sonophoresis TDD. The mechanical impact of acoustic cavitation have been proven to amplify skin penetrability by adjusting the lipid composition of stratum corneum, forming diffusion avenues and microjets that mechanically crack lipid layers. Sonophoresis can be integrated with other methods, such as nanopracticles or dual – frequency sonophoresis, for highly effective drug delivery. However, its necessary to remember that raising frequency may also bring thermal effects, potentially leading to skin damage, including burns, epidermal peeling, and tissue death, especially when a high thermal index is calculated. As a result, care must be taken when applying ultrasound based TDD.[24]
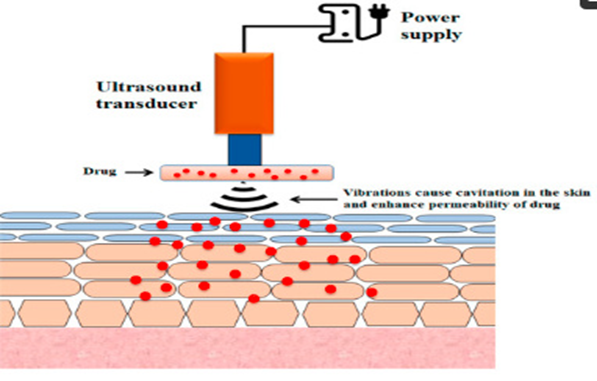
Fig 6 : Schematic diagram of sonophoresis[24]
High pressure based-devices – recently, high pressure devices like jet injections, have been added to the arsenal of transdermal delivery enhancement techniques. The development of these devices was prompted by the need to deliver large quantities of therapeutics at faster speed. The needle free jet injector is a compelling substitute for needle based injections. It uses a power source, such as compressed gas or a spring, to create high speed jets of liquid or powder jet injections that puncture the skin and deliver medications.[27]
Microneedles – have gained considerable attention due to their painless nature and user- friendliness of patients. Microneedles were initially suggested for the drug delivery many years ago, but they only became the focus of significant research in the mid 1990s, when microfabrication technology made them feasible. This technology was created to provide a delivery method that was a dependable as hypodermic needles but free from pain and other associated issues.[26]
Nanocrystals – particle size engineering is arguably one of the oldest and most researched techniques for improving drug bioavailability. The enhancement of the drug dissolution rates due to their elevated surface area resulting from smaller paticles size has been well established and the micronization of pharmaceutical powders remains one of the most prevalent methods for achieving a more advantageous drug release profile. Utilizing nanocrystals as a formulation approach can be considered the newest version of particle size engineering to enhance drug bioavailability.[29]
Marketed transdermal patches
Table 1: list of marketed transdermal patches [30]
|
Brand name |
Drug |
Manufacturer |
Indications |
|
Alora |
Estradiol |
Thera Tech/Protcol and Gamble |
Postmenstrual syndrome |
|
Androderm |
Testosterone |
Thera Tech/GlaxoS mithKline |
Hypogonadism in males |
|
Catapres TTSR |
Clonidine |
Alza/ Boehinger Ingelheim |
hypertension |
|
Climaderm |
Estradiol |
Ethical Holdings/Wyeth-Ayerest |
Postmenstrual syndrome |
|
Climara |
Estradiol |
3M Pharmaceuticals/B erlex Labs |
Postmenstrual syndrome |
|
Deponit |
Nitroglycerin |
Schwarz-Pharma |
Angina pectoris |
|
Duragesic R |
Fentanyl |
Alza/Janssen Pharmaceutical |
Moderate/severe pain |
|
Estraderm |
Estradiol |
Alza/Novartis |
Postmenstrual syndrome |
|
Matrifen R |
Fentanyl |
Nycomed |
Pain relief patch |
|
Minitran |
Nitroglycerin |
3M Pharmaceuticals |
Angina pectoris |
|
Nicoderm R |
Nicotine |
Alza/GlaxoSmithK line |
Smoking cessation |
|
Nicotinell R |
Nicotine |
Novartis |
Pharmacological smoking cessation |
Evaluation of Transdermal Patch
Drug Content Determination – circular samples with a diameter of 1cm were excised from the films and dissolved in 10ml of pH 7.4 phosphate buffer solution (PBS) using a ultrasonic bath for 30minutes. The resulting solutions were then diluted to a final volume of 25ml, filtered paper no. 42, and analysed using a spectrophotometer at a wavelength of 266.5nm (shimadzu UV-1601 spectrophotometer, Japan) to assess the drug content.[31]
Folding endurance – A uniformly sliced patch with a radius of 2cm and a diameter of 4cm was folded repeatedly until it broke. It is calculated by counting how many times the film is folded in the same spot, either breaking it for causing visible cracks to appear. It is important to determine the ability of sample to withstand folding. It also gives an idea about the brittleness of the patch.[32]
Tensile strength- The tensile strength of the patch was measured with a tensiometer ( Erection and instrumentation, Ahmedabad), which consists of two grips for load cells. The lower grip was stationary, while the upper grip was adjustable. Film strips sized 2×2cm were positioned between the grips, and force was gradually applied until the film ruptured. The tensile strength was then determined based on the dial reading in kilograms.[33]
Weight uniformity – A designated section of the patches was meticulously cut into various portions and subsequently measured using a digital balance (Shimadzu AUW22OD). From the individual weights, the mean weight and standard deviation were computed.[34]
Thickness- The thickness of the drug-loaded patch is measured at various locations using a screw gauge or Vernier calipers on different sections of the film. Measurements were taken at five different points four at the corners and one at the centre of the patch. [35,36]
Moisture absorption- percentage of moisture absorbed accurately weighed patches placed in a desiccators for 72h. after 72h, the patches were reweighed and the percentage moisture absorption was calculated using the formula.[37]
% Moisture content= initial weight-final weight initial weight ×100

Water vapour transmission rate – The desiccant used was 1g of melted calcium chloride. Polymeric patch and vials secured to the vial using adhesive tape. Place the vial in the humidity chamber at a weight and temperature. At 300°C, the relative humidity is 80%. The vial was then taken out. Weighed on a regular basis.[38]
Flatness – Longitudinal strips were cut from the patches of each formulation, with one strip taken from the centre and another from the opposite side. The length of each strip was recovered, and the differences in length due to the lack of uniform flatness were assessed. A constriction of 0% was considered equivalent to 100% flatness. Flatness was determined using the formula [39]
I1 initial weight of each strip-I2 (length of the cut film)I2 (cutted film length)×100

Thumb tack test – it involves quickly removing a patch after applaying light pressure on it for about five seconds. By altering the pressure and tack given the duration of contact and the challenge of removing the thumb from the adhesive, it was feasible to estimate the ease, speed and strength with which the adhesive adhered to the skin. [40]
In-vitro drug permeation study- The skin permeation of the prepared polymer patches are examined using a modified Keshary Chien diffusion cell, with the dialysis membrane [41] The receptor compartment of the diffusion cell was filled with phosphate buffer at pH 7.4 and placed on a magnetic stirrer, which contained Teflon bead for even mixing. The patches were positioned between the donor and receptor compartments, ensuring that the drug-releasing surface faced the receptor compartment. [42] Samples were taken at various time intervals and analysed for drug content using spectrophotometry. The analysis was conducted at a wavelength of 276nm, using phosphate buffer pH 7.4 as the blank. [43] After each sample withdrawal, the receptor phase was replenished with an equal volume of phosphate buffer Plotting the cumulative release curve per centimetre of the patch versus time allowed for the comparison of permeation characteristics across the epidermis. Temperature should be maintained at 37±2°C. [44,45]
In-vitro dissolution test – The paddle over disc technique (USP apparatus V) can be utilized for evaluation of the drug’s release from the patch. [46] Drug films with a specified thickness were trimmed into a specific shape, weighed, and secured onto a glass disc with a sticky substance. The glass plate was subsequently positioned. In 500ml of the solution medium or phosphate buffer (pH7.4) and the equipment was adjusted to 32±0.5°C [47] The paddle was subsequently positioned at a distance of 2.5cm from the glass surface and functioned at a rate of 50rpm. Samples (5ml positions) may be taken at suitable time spans of upto 24 hours were examined using UV spectrophotometer or high-performance liquid chromatography. The trial was conducted in threes and the average value was determined. [48]
CONCLUSION
TDDS has shown remarkable potential in enhancing the management of hypertension. These Antihypertensive drugs in the form of patches offer improved bioavailability, reduced side effects and increased patient compliance compared to the conventional dosage forms. Transdermal patches are composed of different excipients and their concentration has an impact on patch development. The main route through which the drug reaches the systemic circulation is by passing through different layers of the skin like the epidermis, dermis and hypodermis, and the mechanism through which the drug permeates through skin is mentioned above, and there are some factors which affect the skin permeability like molecular weight of drug, solubility, age, hydrogen bonding, charge etc. over the years what are the challenges experienced in the development of transdermal patch a brief review is mentioned and future prospects of transdermal drug delivery system is mentioned in this comprehensive review.
REFERENCES



Priya Rajkumar, Vikram T Choudhary, Dr. Gururaj S Kulkarni, A Comprehensive Review of Transdermal Drug Delivery Systems for Antihypertensive Medications, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 639-653. https://doi.org/10.5281/zenodo.17531576
 10.5281/zenodo.17531576
10.5281/zenodo.17531576