
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Laddhad College of Pharmacy, Yelgaon, Buldhana, Maharashtra, India 443001
Buccal patches are advanced drug delivery systems designed to administer drugs through the buccal mucosa, offering an effective alternative to conventional oral dosage forms. Drug absorption through the buccal route allows direct entry into the systemic circulation, thereby bypassing hepatic first-pass metabolism. This leads to improved bioavailability and enhanced therapeutic efficacy. Buccal drug delivery systems provide controlled and sustained release of drugs, resulting in increased plasma drug concentrations and better patient compliance. The drug is placed between the cheek and gum, where it dissolves and is absorbed through the mucosal membrane into the bloodstream. Buccal formulations are available in various forms such as tablets, films, patches, and sprays, making them suitable for both local and systemic drug delivery.
The Buccal Drug Delivery System (BDDS) involves the administration of drugs through the buccal mucosa, which is the lining of the inner cheek of the oral cavity. In this system, the dosage form such as a tablet, patch, or film is placed between the upper gum and the cheek, allowing the drug to be absorbed through the mucosal membrane. The buccal mucosa is considered an ideal site for drug delivery because of its smooth surface, relatively high permeability, and extensive vascularization. Due to the presence of a rich blood supply, drugs absorbed through the buccal mucosa can rapidly enter the systemic circulation.[1]
Transmucosal drug delivery through the buccal route offers several advantages over conventional oral (peroral) administration. One of the most important benefits is the avoidance of first-pass metabolism in the liver, which often reduces the bioavailability of orally administered drugs. Additionally, buccal drug delivery prevents drug degradation caused by acidic pH and digestive enzymes present in the gastrointestinal tract. The enzymatic activity in the buccal cavity is comparatively low, which favors improved stability and absorption of drugs.[2]
Buccal drug delivery is especially useful for drugs that undergo extensive hepatic metabolism, have poor gastrointestinal stability, or require rapid onset of action. The buccal cavity allows both local and systemic drug delivery, making it suitable for treating conditions such as oral infections, pain, inflammation, and systemic diseases. Furthermore, buccal delivery enhances patient compliance because the dosage forms are easy to administer, painless, and non-invasive.[3]
Another major advantage of BDDS is that the buccal cavity is easily accessible for self-medication, making the system safe and patient-friendly. Buccal patches and films can be conveniently applied and removed, allowing immediate termination of drug delivery whenever required. This feature is particularly beneficial in case of adverse drug reactions or overdose. Due to these advantages, buccal drug delivery systems have gained significant attention as an effective alternative to traditional oral and parenteral drug delivery methods.[4]
Buccal Patches [5]
Buccal patch is a non-dissolving, thin matrix, modified-release dosage form composed of one or more polymeric films or layers containing the drug along with suitable excipients. The patch may include a mucoadhesive polymer layer that adheres to the oral mucosa, gums, or teeth, thereby ensuring controlled and prolonged release of the drug into the oral mucosa, oral cavity, or both. Buccal patches are designed to remain in position for a specified period, after which they are removed from the mouth and disposed of. A buccal patch is a small medicated adhesive system intended for placement on the buccal mucosa (inner lining of the cheek), allowing the drug to be absorbed directly through the oral mucosa into the systemic circulation, thus improving bioavailability and avoiding first-pass metabolism.
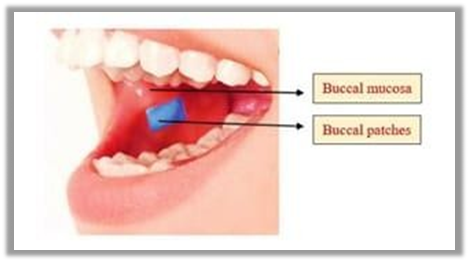
Fig no 1 Buccal patches
Structural Features of the Oral Cavity:
The oral cavity is the region of the mouth delineated by the lips, cheeks, hard palate, soft palate, and the floor of the mouth. It serves as the entry point of the digestive and respiratory systems and plays an important role in drug delivery through the oral mucosa. Anatomically, the oral cavity consists of two main regions. The outer oral vestibule is the space bounded externally by the lips and cheeks and internally by the teeth and gums. The oral cavity proper extends from the teeth and gums posteriorly to the fauces, which lead to the pharynx. The roof of the oral cavity proper is formed by the hard palate anteriorly and the soft palate posteriorly, while the tongue projects upward from the floor of the cavity.[6]
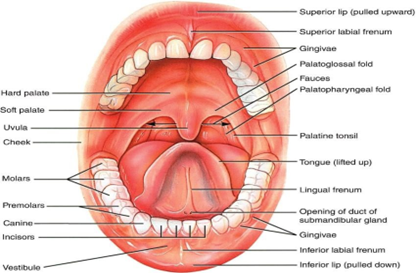
Fig. no. 2 oral cavity
Method of Preparation of Buccal Adhesive Patches [7
Two main methods are commonly used for the preparation of buccal adhesive patches, namely solvent casting and direct milling.
In this method, all patch excipients including the drug are uniformly co-dispersed in a suitable organic solvent to form a homogeneous solution or dispersion. This mixture is then coated onto a sheet of release liner. The solvent is allowed to evaporate under controlled conditions, resulting in the formation of a thin drug-loaded polymeric film. After complete solvent evaporation, a protective backing material is laminated onto the coated release liner to form a laminate. The laminate is then die-cut into patches of the desired size and shape.
In the direct milling method, buccal patches are prepared without the use of solvents, making it a solvent-free process. The drug and excipients are mechanically mixed by direct milling or kneading, usually without the addition of any liquid. After thorough mixing, the resultant mass is rolled onto a release liner until the desired thickness is achieved. A backing material is then laminated in a manner similar to the solvent casting method. Although there are minimal or no differences in the performance of patches prepared by either method, the direct milling method is preferred as it eliminates the risk of residual solvents and avoids solvent-related health and safety issues.
Materials Used in Buccal Patch [8-10]
A buccal patch is a type of oral transmucosal drug delivery system prepared using specific materials that enable adhesion to the buccal mucosa and controlled release of the drug. The materials used in buccal patches are selected based on their biocompatibility, mucoadhesive properties, flexibility, and ability to control drug release.
1. Backing Layer (Protective Layer)
The backing layer prevents the loss of drug from the outer surface of the patch and ensures unidirectional drug release toward the buccal mucosa. Common materials used include:
2. Drug-Containing Layer (Reservoir/Matrix Layer)
This layer contains the drug and controls its release. It is generally composed of hydrophilic or mucoadhesive polymers such as:
3. Mucoadhesive Polymers
These polymers help the patch adhere firmly to the buccal mucosa, prolonging the residence time and enhancing drug absorption. Commonly used mucoadhesive polymers include:
4. Plasticizers
Plasticizers improve the flexibility, elasticity, and mechanical strength of the buccal patch, preventing brittleness. Examples include:
5. Permeation Enhancers
Permeation enhancers are optional components added to increase drug penetration through the buccal mucosa. Common permeation enhancers are:
6. Other Additives
Additional excipients are incorporated to improve patient acceptability and performance of the patch, such as:
Table no 1 Formulation Table of Buccal Patch [12]
|
Sr.No. |
Ingredient |
Category |
Function |
|
1 |
Drug (e.g., Model drug) |
Active pharmaceutical ingredient |
Provides therapeutic effect |
|
2 |
HPMC |
Film-forming polymer |
Controls drug release and forms matrix |
|
3 |
Carbopol 934 |
Mucoadhesive polymer |
Enhances adhesion to buccal mucosa |
|
4 |
Chitosan |
Mucoadhesive polymer |
Improves bioadhesion and permeability |
|
5 |
Polyvinyl alcohol (PVA) |
Film former |
Improves mechanical strength |
|
6 |
Glycerin |
Plasticizer |
Improves flexibility and prevents brittleness |
|
7 |
Propylene glycol |
Plasticizer / penetration enhancer |
Enhances flexibility and drug permeation |
|
8 |
Sodium lauryl sulfate |
Permeation enhancer |
Increases drug absorption through mucosa |
|
9 |
Saccharin sodium |
Sweetening agent |
Improves taste and patient acceptability |
|
10 |
Peppermint flavor |
Flavoring agent |
Masks unpleasant taste |
|
11 |
Citric acid |
Saliva-stimulating agent |
Enhances saliva flow and drug dissolution |
|
12 |
Ethyl cellulose |
Backing layer material |
Prevents drug loss and ensures unidirectional release |
Evaluation of Buccal Patch [13-17]
1. Physical Evaluation
Physical evaluation includes weight uniformity, content uniformity, thickness uniformity, and mass uniformity. These parameters are tested using randomly selected patches from each batch to ensure batch-to-batch consistency. Patch thickness is measured at five different randomly selected points using a screw gauge or digital micrometer, and the average thickness is calculated.
2. Surface pH
The surface pH of buccal patches/tablets is determined to assess the possibility of irritation to the buccal mucosa, as acidic or alkaline pH may cause discomfort in vivo. The surface pH should be close to neutral. The method described by Bottenberg et al. is commonly used. The tablet is allowed to swell by placing it in contact with 1 mL of distilled water (pH 6.5 ± 0.05) for 2 hours at room temperature. A combined glass electrode is then brought into contact with the tablet surface and allowed to equilibrate for 1 minute before recording the pH.
3. Swelling Index
Buccal patches are individually weighed (W?) and placed in 2% agar gel plates with the core surface facing the gel. The plates are incubated at 37°C ± 1°C. At predetermined intervals of 1 hour up to 6 hours, the patches are removed, excess surface water is gently wiped using filter paper, and the swollen patches are reweighed (W?). The swelling index indicates the hydration capacity of the polymer and its role in mucoadhesion.
4. Ex Vivo Mucoadhesive Strength
Fresh buccal mucosa (sheep or rabbit) is fixed to a vial containing buffer solution. The buccal tablet is placed on the mucosal surface and allowed to remain in contact for 5 minutes. Water is then added dropwise until the tablet detaches from the mucosa. The weight of water required to cause detachment is recorded as the mucoadhesive strength.
5. Ex Vivo Mucoadhesion Time
For mucoadhesion time, the core side of the tablet is moistened and pressed onto the buccal mucosa for 30 seconds. The mucosa is then placed in a buffer solution (pH 6.8) maintained at 37°C and stirred at 50 rpm. The time required for complete detachment of the tablet from the mucosa is recorded as the mucoadhesion time.
6. In Vitro Drug Release
In vitro drug release studies of bilayered or multilayered buccal tablets are performed using phosphate buffer (pH 6.8) at 37 ± 0.5°C with a paddle speed of 50 rpm. The tablet is fixed to a glass disk using cyanoacrylate adhesive and placed at the bottom of the dissolution vessel. At predetermined time intervals, 5 mL of the dissolution medium is withdrawn and replaced with fresh buffer. The samples are filtered, suitably diluted, and analyzed using UV spectrophotometry at the selected wavelength.
7. In Vitro Drug Permeation
In vitro buccal drug permeation studies are carried out using Keshary–Chien or Franz diffusion cells at 37°C ± 0.2°C. Fresh buccal mucosa (sheep or rabbit) is mounted between the donor and receptor compartments. The buccal tablet is placed in the donor compartment with the core facing the mucosa. The receptor compartment is filled with phosphate buffer (pH 6.8), and samples are withdrawn at regular intervals to determine the amount of drug permeated through the mucosa.
8. Stability Study in Human Saliva
Stability studies of optimized bilayered or multilayered buccal tablets are performed using natural human saliva collected from healthy volunteers aged 18–50 years. The tablets are placed in Petri dishes containing 5 mL of human saliva and stored in a temperature-controlled oven at 37°C ± 0.2°C for 6 hours. At predetermined intervals (0, 1, 2, 3, and 6 hours), tablets are examined for changes in color, shape, surface integrity, tablet collapse, and drug content.
HOW TO USE BUCCAL PATCH [18-21]
A buccal patch is a medicated adhesive patch that sticks to the inside of your cheek and delivers medicine directly into your bloodstream through the oral mucosa.
1. Wash your hands
2. Rinse your mouth
3. Dry the inside of your cheek
4. Open the packet
5. Place the patch correctly
6. Press and hold
7. Do not disturb it
8. Eating and drinking
9. Removal

Fig. no. 3 HOW TO USE BUCCAL PATCH
Table no 2 Advantages of Buccal Patches[22-24]
|
Sr. No. |
Advantage |
Brief Explanation |
|
1 |
Avoids first-pass metabolism |
Drug directly enters systemic circulation |
|
2 |
Prevents acid and enzyme degradation |
Protects drug from GIT environment |
|
3 |
Easy removal in toxicity |
Therapy can be stopped immediately |
|
4 |
Good patient compliance |
Non-invasive and painless |
|
5 |
Rich blood supply |
Enhances drug absorption |
|
6 |
Controlled & sustained release |
Maintains constant drug level |
CONCLUSION
Research in drug delivery systems is essential not only for developing new pharmaceutical therapies but also for improving the safety and efficacy of existing treatments. Optimizing drug delivery in terms of controlled release, site-specific targeting, and predictable biodegradation can enhance therapeutic outcomes while reducing adverse effects. Injectable medications are often costly, inconvenient, and can carry serious risks. Therefore, there is a growing need for inexpensive, multiple-dose formulations with improved bioavailability. Transmucosal and transdermal delivery methods, including buccal adhesive systems, are particularly valuable because they eliminate the pain and complications associated with injections. Buccal patches offer numerous advantages such as easy accessibility, simple administration and removal, prolonged retention, low enzymatic degradation, cost-effectiveness, and high patient compliance, making them an effective alternative to conventional drug delivery methods.
REFERENCES

Hemantkumar Dhongade, Sakshi Rande, Avanti Girdekar, A Comprehensive Review on Formulation and Evaluation of Buccal Patches, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 2682-2689. https://doi.org/10.5281/zenodo.18360592
 10.5281/zenodo.18360592
10.5281/zenodo.18360592