
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Rashtriya College of Pharmacy Hatnoor, Kannad, Chh. Sambhajinagar 431103
According to studies canker sore or mouth ulcer is the most common condition that we encounter. Clinically the lesion is the single or multiple superficial and deep sealed and are associated with microbial invasions. India has used its knowledge of traditional or herbal medicine to prevent and cure diseases. Herbal medicines have been used since ancient times to treat various oral diseases or maintain oral hygiene. As the mouth ulcer is healing, it frequently causes pain and discomfort and may change the person’s eating preferences. A mouth ulcer is an open sore on the skin or mucous membrane characterized by detachment of inflammatory dead tissue. This articale specifically addressed the management of mouth ulcers, often known as canker sores. These uncomfortable sores appear on the oral cavity’s mucous membranes. The use of herbal gel to treat these ulcers is the main topic of conversation. A gel is a soft, solid or solid-like material which consists of at least two components, one of them being a liquid, present in substantial quantity. There are number of synthetic gels in the market as compared to herbal or natural gel, but synthetic gels have some harmful effects on skin like irritation and dryness of skin. The herbal oral gel of Ocimum sanctum, Aloe Vera, Psidium guajava Linn leaves, and Curcuma longa Linn rhizomes to treat mouth ulcer. The traditional medical study is an integral part of the culture and the interpretation of health by indigenous population in almost world. This review explores the potential of a using. Tulsi for mouth ulcer recovery. The plants have been used in traditional medicines for their anti-inflammatory, antimicrobial, and wound-healing properties. Guava leaves have been usually used to govern several diseases such as rheumatism, diarrhea, diabetes mellitus, wound sore throat, cough and it also gives good antimicrobial, antifungal, anticancer activity. Guava comprises some essential phytoconstituents such as tannins, hyperin, quercetin, guaijaverin. Oleanolic acid, and ursolic acid antimutagenic, antioxidant properties. Turmeric contains a large variety of phytochemicals such as curcumin, cyclocurcumin, demethoxycurcumin, eugenol, tannis, alkaloids, terpenoids and curcunol.
A large number of Indian herbal medicinal plant are attributed with medicament preparation. Over three fourths of world population depend mainly on the plants and plants derived from herbal medicines. 30% of the plant species are used for medicinal purposes [1]. Thus, the economic importance of medicinal plant in India is much more than rest of the world. These countries contribute two third of the plant used in modern system of medicine and the indigenous system of medicine provides health care system rural population [2]. The word “gel” is derived from “gelatin” and both “gel” and “jelly” can be drawn back to the Latin gelu for “frost” and gel are, meaning “freeze” or “congeal” [3]. Gel is mainly semi-solid formulation having a liquid phase that has been thickened with some other components. Topical gel preparation is used for the skin application or percutaneous penetration of medicament or local action to certain mucosal surfaces [4]. Mouth ulcers are also known as canker sore -painful lesions that develop in mouth at base of your gum. Aphthous stomatitis or mouth ulcer is an ulcerative condition that is related to the oral mucosa and is characterized by repeating ulcers in the throat and oral cavity. They can cause problems during eating, drinking and talking uncomfortable. Gum, lips, inner check and plate ulcers can develop in the mouth. A mouth ulcer is the loss or erosion of the mucosal membrane the fragile tissue that lines the mouth Nutritional deficiencies, such as iron deficiency, vitamin deficiencies, particularly B12 and C, poor dental hygiene, infection, stress, indigestion, mechanical damage, food allergies, hormonal imbalance, skin conditions, etc. [5]. Mouth ulcers are yellowish or white depression with red margination in the mucus cavity characterized by inflammation and pain.

Fig No: 1
Synthetic and semi-synthetic medicaments are suggested to treat mouth ulcers like antibiotics and antiseptics, local anesthetics, local analgesics, steroidal and non-steroidal anti-inflammatory drugs [6]. The treatment of mouth ulcers are topical gels, mouth washes, oral liquids, cream, ointments, patches, lozenges and tablets. Jasminum grandiflorum is a medicinal plant belonging to family Oleaceae. The leaves of this plant have therapeutic application in ayurveda for managing wounds. This plant is well known for aromatic flowers [7]. Ocimum Tenuiflorum also known as Tulsi is a medicinal plant with numerous health benefits belonging to family Lamiaceae[8]. Psidium guajava known as Guava, is a medicinal plant belonging to the family Myrtaceae. Psidium Guajava is a well-known traditional medicinal plant used in various indigenous system of medicine. Several studies have reported the use of plant parts or rhizomes Turmeric Curcuma longa which belongs to the family Zingiberaceae. Azadirachta Indica known as Neem leaves is a medicinal plant belonging to the family Meliaceae. Piper betel commonly known as Paan belonging to family Piperaceae, have had several applications in India Folk and traditional medicine. It contains important phytoconstituents such as Tannis, alkaloids, phenols, flavonoids: quercetin, pentacyclic triterpenoid: saponins, carotenoids, lectins, ellagic acids. Various studies on biological effects of the presence of leaves indicated the presence of Anti-ulcer, Anti-fungal, Antibacterial, Antioxidant and Anti-inflammatory activities.[9]
Pathophysiology:
The underling source of the aliment determines how it develops specially. Xerostomia, or dry mouth brought on by a reduction in saliva production, is one of the simple mechanisms that raises the risk of oral trauma and ulcers. The mouth lining may become more vulnerable to damage if saliva production is reduced because it typically lubricants the mucous membrane and aids in bacterial control [10]. Ulceration frequently coexists with stomatitis, a condition that refers to inflammation in mouth. They are common conditions that affects most people at some point in their lives. The anatomical characteristics make the mouth cavity susceptibility to many conditions that impact the gastrointestinal system and skin. Some conditions can only manifest in the mouth, even though they often impact entire digestive system.[11] The clinical picture is further complicated by the increased risk of secondary infections in these ulcers due to the high bacterial presence in the mouth.
Mechanism of action:
The mechanism of action a mouth ulcer is primarily the disruption of the oral mucosa’s protective lining, which is a complex process triggered by various factors including trauma, infection, and systemic conditions. Trauma form physical injury or irritants is a direct cause, while infections can trigger ulcer formation through microbial interactions. Additionally, conditions like stress, vitamin deficiencies, autoimmune disorders, and hormonal changes can weaken the mouth’s defenses, leading to ulcer development.
Trauma: Mechanical, thermal, or chemical irritant breach the protective epithelial barrier, Examples including; Biting the inside of the cheek, Sharp or ill-fitting dental work, Irritating foods
Infection: Viral infection, like herpes simplex virus (HSV), can lead to the formation of painful ulcers after a vesicle breaks down. A disruption in the balance of oral microbes (dysbiosis) can lead to opportunistic infection that may cause ulceration.
Weakened mucosal defenses: Dry mouth (xerostomia): Saliva normally lubricates the mouth and controls bacteria. Without it, the lining becomes more fragile and susceptible to injury. Epithelial atrophy: A thinning of the mouth’s lining, which can occur after radiotherapy, makes it more vulnerable.
Type of mouth ulcers:
Minor Ulcers:
Major Ulcers:
Herpetiform Ulcers:
Causes of Mouth Ulcers:
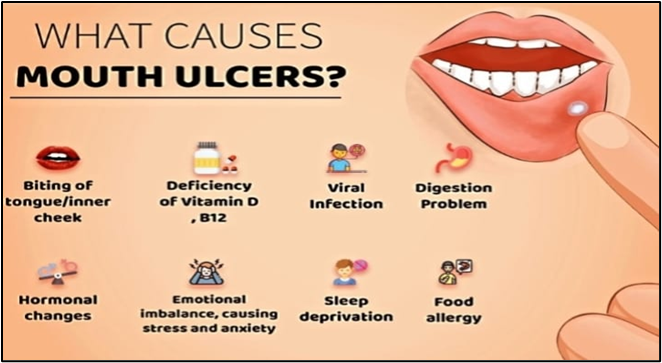
Fig no: 2
Deficiencies in essential nutrients such as iron, vitamin B12, folic acid and vitamin C are known to contribute to the development of mouth ulcers.[15] B12 is essential for DNA synthesis and maintaining healthy nerve and blood cells.
Inadequate oral can lead to bacterial growth and inflammation, increasing the risk of ulcers. Infrequent brushing and flossing can lead to the accumulation of bacteria and other microorganisms in the mouth, which can cause mouth ulcers.[16]
Psychological stress has been associated with an increased frequency of mouth ulcers, potentially due to its effects on the immune system. Stress can trigger mouth ulcers in some individuals.
Certain foods, including acidic or spicy items, can trigger or aggravate mouth ulcers in sensitive individuals. Food containing gluten, including chocolate, coffee, almonds, tomatoes, cereals, peanuts, strawberries, cheese, and wheat flour, may cause aphthous ulcers.[17]
It appears from a variety of studies, some of which are contradictory, that a small subset of women with RAU experience cyclical oral ulceration in relation to the start of menstruation or the luteal phase of the menstrual cycle.[18] Fluctuations in hormones, particularly during menstruation or pregnancy, have been linked to an increased occurrence of mouth ulcers.[19]
Skin conditions like eczema or psoriasis can sometimes cause mouth ulcers as secondary symptoms. Mouth ulcers have a multi factorial etiology, with nutritional deficiencies, infections, stress mechanical injuries, and other factors contributing to their onset.[20]
Accidental bites, rough dental work, or ill-fitting dentures can cause mouth ulcers The brushing too hard or using a hard toothbrush, or using poorly fitting dental appliance can lead to ulcers.[21] Lack of sufficient saliva may contribute to the emergence of RAS by failing to lubricate and shield the mouth mucosa from antigenic exposures.[22]
Tobacco smoke and heat can irritate the sensitive lining inside your mouth. Repeated exposures can damage the mucosa, making it more prone to ulceration. People who don’t smoke are typically more susceptible to RAS, and heavy smokers are less likely than moderate smokers to experience the condition in its most extreme forms.[23]
The ulcer can penetrate deeper into the tissue, causing damage to the underlying lamina propria and leading to the formation of a crater-like lesion.[24]
Symptoms:
A painful sore or sore on the inside of the mouth, including the lips, cheeks, tongue, or roof of the mouth. Mouth ulcers can be painful and tender to the touch.
The affected area may become red and swelling of the tissue surrounding the ulcer. Blood vessels in the surrounding tissue dilate to bring more blood and immune cells to the area to help heal the ulcer.
Mouth ulcers can make it challenging to eat certain foods, especially spicy or acidic ones.
A burning or tingling sensation may occur in the area before the sore appears.
Factor affecting of mouth ulcers:
Mechanical trauma from aggressive tooth brushing, poor injuries. Studies show that continuous trauma can compromise the mucosal barrier, leading to ulcers and chronic oral pain.[25]
Genetics plays a role in susceptibility to conditions like canker sores, oral cancer, and certain gum diseases. Individuals with a family history of these conditions are more likely to experience similar oral health issues.[26]
Bacterial infection like gingivitis and periodontitis are caused by a buildup of bacteria in the oral cavity. Streptococcus mutants and Porphyromonas gingivalis are common culprits.[27] In addition, viral agents, including herpes simplex and HIV, and gastroesophageal reflux disease (GERD) can cause oral dryness, infection, and increased vulnerability to ulcers.
Allergy’s reaction to ingredients in oral care products, such as flavoring agents or preservatives, can lead to conditions like stomatitis (Inflammation of the mouth). Some patients also exhibit sensitives to sodium lauryl Sulfate (SLS), leading to mucosal irritation.[28]
Viral infections like Herpes Simplex Virus (HSV) cause cold sores, and the varicella-zoster virus can lead to shingles in the mouth. Additionally, the Human Papillomavirus (HPV) can cause oral warts. These infections affected the oral mucosa and can cause painful lesions.[29]
Autoimmune diseases such as lupus and Behest’s disease can manifest with oral ulcers and sores. Similarly, conditions like diabetes, HIV, and gastroesophageal ulcer.[30]
Limitation:
Current treatments for common mouth ulcers (such as recurrent aphthous stomatitis) primarily focus on symptom relief (pain reduction, inflammation control) rather than addressing the underlying causes, and several challenges exits:
Most current over the counter and prescription medication (gels, mouthwashes, steroids) offer temporary relief and promote healing but do not prevent future occurrence.
For conditions like recurrent aphthous stomatitis (RAS), episodes often return, indicating an unmet need for long-term preventing solutions.
The dynamic and moist oral environment, with constant saliva flow and physical actions like chewing, makes it difficult for topical medication to adhere to the ulcer site for a sufficient duration to provide sustained relief and effective healing.
There is no single therapy that works for every patient due to the multifactorial nature of the condition (cause range from stress and nutrition to genetics and underlying systemic diseases), making generalized treatment difficult.
Diagnosing the root cause of persistent or unusual ulcers can be difficult, sometimes requiring ulcers can difficult, sometimes requiring biopsies to rule out more serious conditions like oral cancer or more or autoimmune disorders.
Some medications, especially long term or systemic use of corticosteroids or certain antibiotics, can have side effects (e.g., increased risk of oral yeast infections, gastrointestinal issues).
Future Prospects:
Future prospects in mouth ulcer treatment focus on innovative drug delivery, regenerative medicine, and non- pharmaceutical therapies to improve efficacy and patient quality of life.
Innovation like mucoadhesive patches and nanofiber films are being developed to adhere strongly to the oral mucosa, providing localized, controlled, and sustained drug release directly to the ulcer site, thus enhancing efficacy and reducing the frequency of application.
Research into using advanced biomaterials and stem cell biology aims to promote actual tissue regeneration and scar -free healing, potentially leveraging the oral mucosa’s inherent ability to heal quickly and without scarring.
A deeper understanding of the biological mechanism and signaling pathways involved in ulcer formation (e.g., specific fibroblast lineages, inflammatory response) is expected to lead to novel agents that target the root causes of the condition, rather than just the symptoms.
There is a growing consumer and market demand for natural ingredients (e.g., aloe vera, honey, curcumin) with anti-inflammatory and wound-healing properties, prompting manufactures to invest in developing effective, natural products lines with minimal side effects.
Advancements in genetics in genetics and genomics may enable personalized treatment strategies based on an individual’s ulcer triggers.
Various Dosage form used for the Treatment of Mouth Ulcers:
Herbal Gel:
Herbal gels for mouth ulcers use plant extracts with anti-inflammatory, anti-microbial, and wound healing properties to relieve pain, inflammation and promote healing. The natural ingredients like Guava leaves, Tulsi leaves, Betel leaves, Neem leaves, Turmeric. These combined ed with gelling agents like Carbopol. These gels are formulated to be mucoadhesive, meaning they adhere to the oral mucosa to remain on the ulcer site, providing prolonged relief and effective treatment for conditions like aphthous stomatitis. Gels are composed of small number of solids dispersed in relatively large amount of liquid, yet they possess more solids-like than liquid-like character. The characteristics of gel is the presence of some form of cutaneous structure, which provides solid-like properties.[31]
Classification of gel:
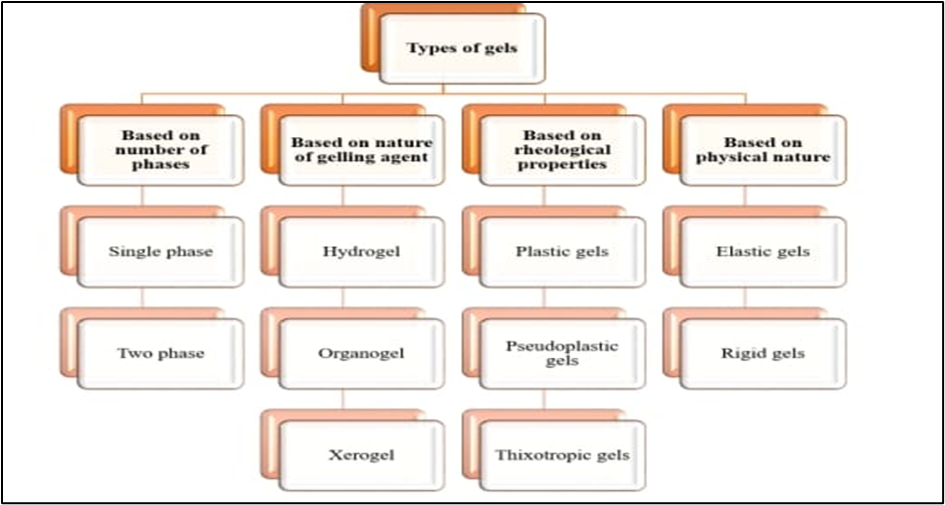
Fig No: 3
Properties of Gels:
Characteristics of Gels:
Gel can swell, griping liquid with an increase in volume. This can be observed on as the initial phase of dissolution. Solvent penetrates the gel matrix so that gel-gel relations are replaced by gel-solvent interactions. Limited swelling is usually the result of some grade of cross-linking in the gel matrix that prevents total dissolution. Such gel swells significantly when the solvent mixture possesses a solubility behavior comparable to that of the gellant.[33]
Many gels system undergo shrinkage upon standing. The interstitial liquid is expressed, collecting at the surface of the gel. This process stated to as syneresis, is not limited to organic hydrogels, but has been seen in organogels and inorganic hydrogels as well. Typically, syneresis, becomes more pronounced as the concentration of polymer decreases. The mechanism of contraction has been related to the relaxation of elastic stresses established during the setting of the gel. As these stresses are relived, the interstitial space existing for solvent is reduced, forcing the expression of fluid.[34]
This process is referred to as ageing. Colloidal system usually exhibits slow spontaneous aggregation. In gels, ageing results in the slow formation of a dense network of the gelling agent. This process is like to the original gelling process and continues after the initial gelation, since the fluid medium is lost form the afresh formed gel structure. The nature of the particles and the kind of force that is responsible for the linkages determine the structure of the network and the properties of the gel.[35]
Solution of the gelling agents and dispersion of flocculated solid are pseudo plastic i, e., showing non-Newtonian flow performance, characterized by a reduction in viscosity with an increase in shear rate. The tenuous structure of inorganic particles dispersed in water is disrupted by applied shear stress due to breaking down of interparticle association, exhibiting a greater tendency to flow.[36]
Uses of Gel:
Advantages of Gel:
Drug Profile:

Fig No:4
Psidium guajava Linn. Commonly called guava belongs to the family Myrtaceae and genus Psidium, Guava is often hailed as the “Queen of fruits” due to its rich nutrient profile. It is recognized for high proteins and fiber content, as well as its lack cholesterol. Similar to others fruits, guavas are concentrated source of essential vitamins and minerals.[39] The abundant presence of macro and micronutrients in guava contributes to its numerous health benefits, including the maintenance of ocular health, regulation of thyroid function, and other positive effects. For the herbal treatment of a number of oral conditions, including toothaches, sore throats, inflamed gums, and ulcers, Psidium guajava has been utilized.
Mechanism of action:
In controlling infection diarrhoea and compare it with quercetin, one of the most reported active. Guava leaves help with mouth ulcers by providing anti-inflammatory and antimicrobial effects, along with wound healing properties. These actions are attributed to compounds like flavonoids, tannins, and polyphenols, which reduce inflammation, fight bacteria, and promote tissue repair. This can lead to pain reduction and faster healing of the ulcer.
Taxonomy classification:
Fig No: 5
|
Synonym: |
Psidium guajava |
|
Kingdom: |
Plantae |
|
Family: |
Myrtaceous |
|
Origin: |
India |
|
Genus: |
Psidium |
|
Divisions: |
Spermophyte |
|
Class: |
Dicotyledons |
|
Sub-divisions: |
Angiospperm |
Biological source:
The biological source of guava leaves is the plant species consist of fresh and dried leaves Psidium guajava Linn. A member of the Myrtaceae (myrtle) Family, which is native to the tropical Americans and widley cultivated in tropical and subtropical regions. These are known for its economic and commercial importance, the high nutritional value of its fruits, which are high in vitamins A, B, and C, the numerous medicinal applications for which its fruits, leaves, flowers, bark roots, and stems are used, as well as the profitability of its cultivation.[40]
Geographical Distribution:
Guava leaves are distributed globally in topical and sub-tropical regions where the guava tree (Psidium guajava) in native, primarily in Mexico central America, the Caribbean, and Northern south America. This fruit was carried across the Pacific by the Spanish to the Philippines, and by the Portuguese to India, and it was rapidly adopted as a crop in Asia and some areas of Africa; it is now found in Egypt, Palestine, Algeria, and the French Mediterranean cost. India, Brazil, the Philippines, Mexico, Colombia, Peru, Ecuador, South Africa, the United States of America, Venezuela, Costa Rica, Cuba, and Puerto Rico are the primary producers of this fruit. The majority of the varieties sold in Europe are imported from south Africa and Brazil.
Morphology characteristics:
The better understanding morphology guava to better knowledge of plants part like Roots, stem, tree size, leaves, flowers, and fruits. Guava leaves exhibit an oblong to oval shape, measuring and average of 7-15 cm in length and 3-5 cm in width. The leaves have prominent parallel veins that originate from the midrib and extend towards the edges. Arranged oppositely on the stem, which short petioles connecting them, to the emerge from the same point. This deep green leaves have a wide and leathery surface, featuring faint white veins and occasional light brown patches. When crushed, they emit and aromatic scent reminiscent of the guava fruit growing on a small tree with wide spreading branches, the guava leaves compliment the tress coppered colored, flacking bark, revealing green base.[41]
Chemical Constituents:
Guava leaves are rich in bioactive compound including phenolic compounds like gallic acid and glycoside other flavonoids like such as quercetin, guaijaverin, kaempferol. They also contain tannins, terpenoids, triterpenes like oleanolic acid and ursolic acid, saponins, alkaloids, vitamins, carotenoids, glycoside and essential oils caryophyllene oxide. Total Lipids of Proteins, The Dietary fiber moisture essential polysaccharides, minerals.[42]
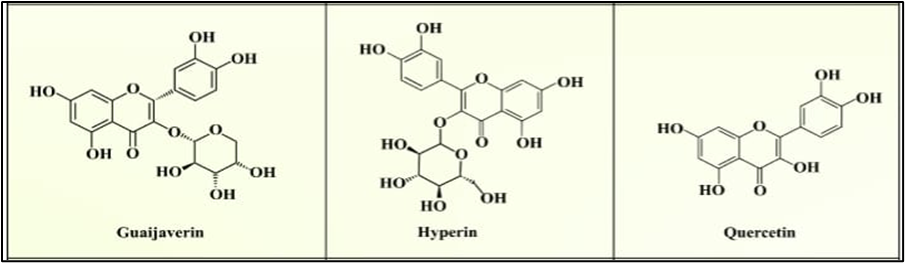
Fig No: 6
Properties of Guava leaves:
Guava leaves contain compound that can help prevent secondary bacterial and fungi infections at the ulcer site. The nanogel maintains effective local concentration of this antimicrobial agent, protecting the ulcer form further infection. Plant derived bioactive compounds are promising sources of antimicrobials. This compound act by the inhibition of microbial cell wall development, disruption, and lysis, hampering biofilm formation, repression of DNA replication and transcription, impeding adenosine triphosphate (ATP) production, suppression of bacterial toxins, and the generation of reactive oxygen species (ROS). Prevent secondary bacterial infection by inhibiting the growth of bacteria like staphylococcus aureus and E. coli. Furthermore, tannins in guava leaves promote wound healing by forming a protective layer over damaged tissues, accelerating recovery and reducing pain.
The bioactive compounds form the guava leaves reduce the production and release of inflammatory mediators at the ulcer site. This leads to decreased swelling and pain, helping to alleviate of the discomfort associated with mouth ulcers. These make them particularly useful for conditions such as mouth ulcers and gum infections.
The antimicrobial and anti-inflammation properties of guava leaves help in wound healing by preventing infection and reducing inflammation. They have been used traditionally for cuts, burns and even mouth ulcers. It accelerates the healing process of the damaged oral mucosa.
The triterpenoids and flavonoids in guava leaves have shown potential in preventing and treating certain types of cancer by inhibiting the growth of cancerous cells. Cancer is a complex health disorder which is identified by the development of cell proliferation or a decrease, causing apoptosis.
Guava leaves are rich in antioxidants like flavonoids and phenolic compounds, which help neutralize free radicals in the body and protect cells form oxidative damage. This can promote general health and prevent chronic diseases. The antioxidants present in guava leaves neutralize free radicals generated during tissue injury. This minimizes oxidative damage to surrounding healthy cells and supports a faster healing process.
Diabetes is a major disease and about 10% of the world’s population suffer from blood glucose metabolic disorder, mainly characterized by a hyperglycemic condition. Instead of beneficial, mouth ulcers are a common and painful complication of diabetes, especially when blood sugar is poorly managed. The systemic effects of diabetes on your body also affect your oral health, leading to more frequent infection, inflammation. and delayed healing.
Uses:
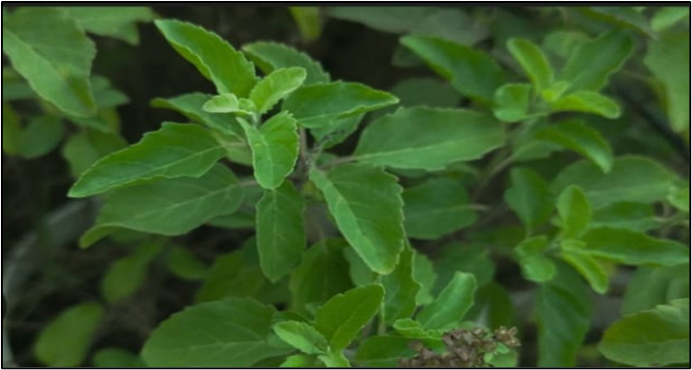
Fig No:7
Tulsi Ocimum sanctum linn, commonly known as holy basil or Tulsi, aromatic perennial plant in the family Lamiaceae. It native to the India a subcontinent and has been used in Ayurvedic medicine for more than three millennia. Its kwon to advance the life span of life in the Ayurveda framework, tulsi is frequently used as a “Solution of Life” for its mending powers and has been known to treat a wide range of basic wellbeing conditions. Tulsi is the most well-known family plant in India and it is hallowed in Hindu custom. In the India Materia Medicate Tulsi plant are widely brought to use for relieving different illnesses, for example, the basic cold, irritation, intestinal sickness, coronary illness, migraines, stomach issue, kidney stones, heart issue, and some more.[43] It has potent anti-ulcerogenic and ulcer-healing properties and could be an effective treatment of mouth ulcer.
Mechanism of action:
The primary mechanism of action for tulsi (holy basil, Ocimum sanctum) on mouth ulcers involves its powerful anti-inflammatory, antibacterial, antioxidant, and cytoprotective properties. The therapeutic effects are mainly attributed to rich composition of phytochemicals, especially eugenol. The anti-inflammatory action of tulsi directly targets the pain and swelling associated with mouth ulcers. Tulsi fights microbial infections that can cause or complicate mouth ulcers. | By neutralizing free radicals, tulsi helps protect oral tissues form damage and promotes healing. Tulsi provides direct protection to the cells lining the mouth and helps regulate the body’s immune response.
Taxonomical classification:
Fig No:8
|
Synonyms: |
Ocimum sanctum |
|
Kingdom: |
Plante |
|
Family: |
Lamiales |
|
Origin: |
India |
|
Genus: |
Ocimum |
|
Class: |
Magnoliopsida |
|
Division: |
Magnoliophyta |
|
Order: |
Lamiales |
Biological Source:
The biological source of tulsi is the fresh or dried leaves of the plant Ocimum sanctum linn, also known as holy basil. It has ordinarily developed in gardens and in the outskirts of sanctuaries. It has an impactful taste and fragrant smell. It is the main plant that can retain carbon dioxide for a mind-blowing duration. It discharges the oxygen in the early morning which is useful for the individuals in breathing disorders. A significant variety of species, subspecies, variation, and strains have developed as a result of the species’ high degree of polymorphism and high level of cross-pollination, which makes botanical classification quite challenging.
Geographical Source:
It is an annual herbaceous plant with several branches that may be found all throughout India and is revered by Hindus. The plant is frequently planted in gardens and is also found close to temples. It is spread by seeds. For volatile oil, Tulsi is now commercially grown. [44] The (holy basil) is native to the India subcontinent, with its primary geographical source being India, and is now cultivated and naturalized in other tropical regions worldwide. It thrives in moist soils in various climates, form sea level up to an altitude of 2000 meters.
Morphology characteristics:
The appearance of a plant, including its roots, stems, leaves, branches, flowers, fruit, and seeds, is studied in morphology. The morphology of the Ocimum Sanctum plant reveals a dark brown exterior root system, while the interior is violet. Tulsi leaves are hairy and sub-quadrangular, ranging from dark purple to black on the outside and cream-colored inside. It is elliptical or oblong or oblique or acute, entire or entire or serrated, pubescent on both side; the petiole is slender, 1.5-3cm long and hairy, with an aromatic perfume and peculiar flavour.[45] It stands erect with an elliptical or oblong shape, sometimes oblique or acute, either or serrated, and pubescent on both sides. The corollas are around 4 mm long, pubescent, and aromatic, with a nectar-like substance.
Chemical constituents:
The chemical constituents of tulsi leaves that aid in treating mouth ulcers including eugenol, carvacrol, and Rosmarinus acids. Eugenol: A major component of tulsi’s essential oil, eugenol is a powerful antiseptic and pain reliever. It effective against various oral pathogens and helps to reduce inflammation. Carvacrol this phenolic compound has strong antibacterial properties that help fight the germs that can cause oral infection. Ocimum sanctum, a well-known plant in India herbal medicine, can be found in a variety of varieties, including the one indicated below. It is possible to make teas and infusions form the flowers and leaves of this plant, which contain a high concentration of essential oils. The isolated phenolic compounds are isothymusin, Ursolic acid circimaritin, cirsilineol, apigenin, and rosameric acid.
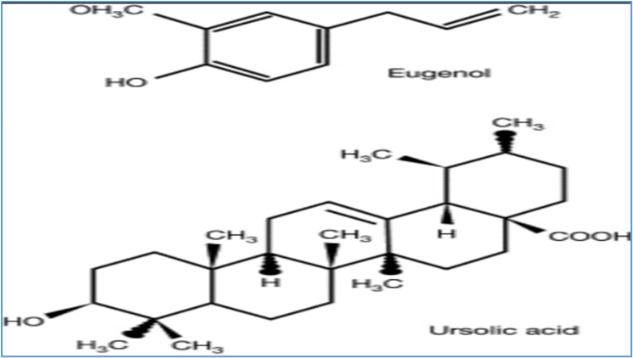
Fig No: 9
Properties Tulsi Leaves:
Tulsi compounds like eugenol, Rosmarinic acid, and various flavonoids that have antioxidant properties. These antioxidants protect the body against damage form free radicals, which can lead to chronic diseases and aging. Excess of oxidation in the body also causes the cell damage. This acid prevents the formation of excess oxidation. Tulsi leaves possess strong antioxidant properties that, along with their antimicrobial, anti-inflammatory, and analgesic effects, make them a traditional remedy for the mouth ulcers. The bioactive compounds in tulsi (Ocimumsanctum) protect oral tissues, fight bacteria, and reduce pain, which all contribute to the healing process.
Tulsi has been shown to have broad-spectrum antimicrobial activity against a range of bacteria, viruses, fungi, and protozoa. This property can help in preventing and treating infection. Tulsi exhibits significant antimicrobial activity against various pathogenic bacteria, making it a natural substitute for synthetic drugs. Tulsi (Ocimum sanctum) confirms its antimicrobial properties, which have a therapeutic effect on mouth ulcers. Tulsi has antimicrobial properties that help combat mouth ulcers due to its rich composition of compounds like eugenol and ursolic acid. These compounds help to inhibit the growth of bacteria that can cause or complicate mouth ulcers, such as Streptococcus mutants.
The phytochemicals in tulsi, such has eugenol and Ursolic acid, exhibits anti-inflammatory properties. Tulsi beneficial in reducing inflammation and can help in the management of inflammatory conditions such as arthritis. The anti-inflammatory activity for the mouth ulcers comes from reducing the inflammatory response through topical steroids, non-steroidal anti-inflammatory drugs (NSAIDs), and natural remedies. Clinical studies have shown that topical applications of tulsi paste can significantly reduce the burning sensation and inflammation in the oral mucosa. This analgesic effect provides relief form the pain commonly associated with
Tulsi can modulate the immune system, enhancing immune response. This makes it beneficial in fighting off infections and boosting overall immunity. Most mouth ulcers, or aphthous ulcers, are thought to involve a T-cell mediated immune response. Tulsi’s bioactive compounds can modulate this immune response, healing the body to heal the ulcer more effectively. Tulsi leaves that help heal mouth ulcers, the connection is based on traditional use and observed effects rather than clinical trials specifically for its immunomodulatory impact on typical moth ulcers.
The radioprotective effect of OS was firstly reported in the year 1995. Two isolated flavonoids, viz., orientin and vicenin form OS leaves showed better radioprotective effect as compared with synthetic radioprotectives. They have shown significant protection to the human lymphocytes against the clastogenic effect of radition and low, nontoxic concentrations.
Intra-peritoneal administration of Ocimum sanctum fixed oil evoked high antiulcer activity antiulcer activity against Indomethacin, Reserpine, serotonin, alcohol, histamine, aspirin, and stress instigated ulcers in rodents. Lipoxygenase inhibition, antisecretory, and histamine antagonistic effects present in fixed oil significant amount possessed antiulcer activity. [46]
Uses:

Fig No: 10
Curcumin is the principal curcuminoid and the most active component in turmeric. Analgesic, antioxidant, antiseptic, antibacterial, anti-inflammatory, and immunomodulatory are just a few of curcumin’s listed medical benefits. The researchers found that turmeric can be utilized to treat mild RAS, although triamcinol one cannot be recommended for the ongoing treatment of mouth ulcers. Curcumin gel was compared to a placebo for the treatment of mild aphthous ulcers by manifer et al in a comparable randomized. Curcumin was found to be marginally more effective than honey for the treatment of aphthous ulcers.
Mechanism of action:
Curcumin works on a molecular level to reduce the swelling and pain associated with oral ulcer Inhibits NF-kB: Curcumin blocks the activation of Nuclear Factor kappa B(NF-kB), a protein complex that acts as a transcription factor for genes that produce pro-inflammatory cytokines such as TNF-a, IL-1B.and IL-6. Ulcers are often associated with oxidative stress, and curcumin’s antioxidant properties help counteract this damage. The mechanism of turmeric’s action for mouth ulcers is primarily driven by its active compound, curcumin, which provides antioxidant, anti-inflammatory, and antimicrobial effects. This helps to soothe symptoms, control i9nfection, and promote faster healing of the oral tissue.
Taxonomical classification:
Fig No: 11
|
Synonyms: |
Curcuma longa |
|
Kingdom: |
Plantae |
|
Divisions: |
Angiosperm |
|
Class: |
Magnoliopsida |
|
Family: |
Zingiberaceae |
|
Origin: |
India |
|
Genus : |
Curcuma |
|
Order: |
Zingiberales |
Biological source:
The biological source of turmeric of the consist rhizomes of curcuma longa which belongs to family: Zingiberaceae. Turmeric has been done for gastric and duodenal antiulcer activity. Volatile oil curcuma longa possesses anti-inflammatory and anti-arthritics activities. Curcumin strong antioxidant activity comparable to vitamins C and E.
Morphology characteristics:
Turmeric is a perennial herbaceous plant that reaches up to 1 m tall. Highly branched, yellow to orange, cylindrical, aromatics rhizomes are found. The leaves are alternate and arranged in two rows. They are divided into leaf sheath, petiole, and leaf blade. Form the leaf sheaths, a false stem is formed. The petiole 50 to 115 cm long. The simple leaf blades are usually 76 to 115 cm long and rarely up to 230 cm. They have a width of 38 45 cm and are oblong to elliptical, narrowing at the tip plant part used rhizomes and stem.
Geographical source:
The primary geographical source of turmeric is India, Which India, major cultivation states include Telangana, Maharashtra, Karnataka, and Tamil Nadu, with Telangana and Maharashtra being leading producers. Turmeric is also cultivated in other countries like Thailand, China, other Southeast Asia nations, Central and Latin America, and Twain. The plant is a native to southern Asia and is cultivated extensively in temperate regions. It is grown on a larger on a scale in India, China, East Indies and Pakistan.
Chemical constituents:
Phytochemical components of turmeric include diaryl heptanoids, a class including numerous curcuminoids, such as curcumin, demethoxycurcumin, and bisdemethoxycurcumin. Some essential oils are present in turmeric, among which turmerone, germacrone, atlantone, and zingiberene are major constituents.[47]
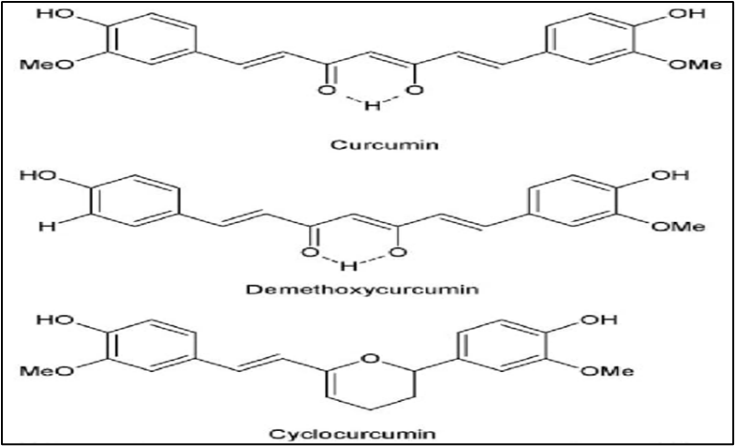
Fig No: 12
Properties of Turmeric:
Curcumin reduces inflammation associated with mouth ulcers, which helps lower pain and swelling. Turmeric can help with mouth ulcers inflammation because its active compound, curcumin, has powerful anti-inflammatory and antimicrobial properties.
Turmeric inhibits the early stages of carcinogenesis due to its antioxidant and free radical properties. It has effect on several biological pathways involved in mutagenesis, oncogene expression, cell cycle regulation, apoptosis, turmorigenesis, and metastasis.
Uses:

Fig No: 13
Mechanism of action: Aloe vera promotes the healing of mouth ulcers through a multi-mechanism approach that includes anti-inflammatory, immunomodulatory, antimicrobial, antibacterial, antifungal, antiviral, and wound-healing effects. Aloe vera contains compound such as C-glucosly chromone, anthraquinones, and plant steroids (lupeol, campesterol, that inhibit the cyclooxygenase (COX) pathway, thereby reducing the production of inflammatory mediators like enzyme bradykinase, which breaks down the pain-inducing inflammatory substances bradykinin. In essence, aloe vera herbal gel provides a safe, multi-targeted approach to treating mouth ulcers by managing pain and inflammation, fighting infection, and actively promoting the body natural healing processes.
Taxonomical classification:
Fig No: 14
|
Synonyms: |
Aloe barbadensis |
|
Kingdom: |
Plantae |
|
Division: |
Magnoliophyta |
|
Class: |
Liliopsida |
|
Family: |
Aloaceae |
|
Genus: |
Aloe L |
|
Order: |
Liliales |
|
Origin: |
India |
Biological source:
The biological source of Aloe Vera is Aloe barbadensis. Aloe is dried latex of leaves of aloe vera. It belonging to the family Xanthorrhoeaceae.
Morphology characteristics:
Aloe Vera is a stemless or very short stemmed plant growing to 60-100cm (24-39) tall, spreading by offsets. The leaves are thick and fleshy, green to grey-green, with some varieties showing white flecks on their upper and lower stem surfaces. The margin of the leaf is serrated and has small white teeth. The flowers are produced in summer on a spike up to 90 cm (35in) tall, each flower being pendulous, with a yellow tubular corolla 2-3cm (0.8-1.2 in) long. Like other Aloe species, Aloe Vera forms Arbuscular mycorrhiza, a symbiosis that allows the plant better access to mineral nutrients in soil. Plant part used: Leaves, Flowers, stems, roots, fruits, seed.
Chemical constituents:
The chemical constituents in AoleVera anthraquinones, saccharides, prostaglandins and fatty acids. Others enzymes, amino acids, vitamins, minerals. Other compound Cholesterol, triglycerides, steroids, uric acid, lignins, betasitosterol, gibberellin, emodin, aleosin, aloin, salicylic acid.[48]
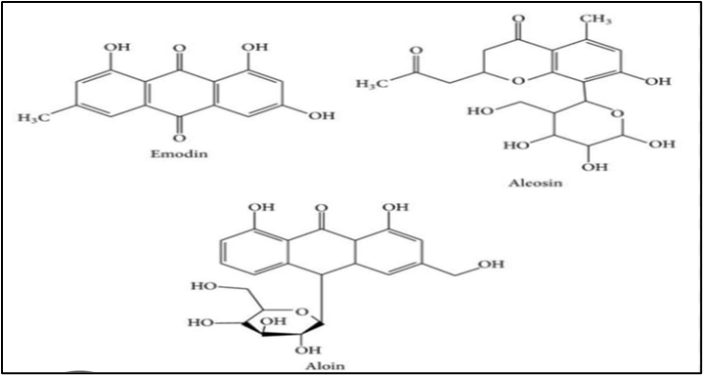
Fig No: 15
Properties of Aloe Vera:
Uses:
CONCLUSION:
In conclusion, the combination of Psidium guajava, Ocimum tenuiflorum (tulsi), a Turmeric and Alovea offers a promising natural solution for managing mouth ulcer. This review provides the information of treatment of ulcer by different herbal medicinal p-lant and give information of its family, kingdom, chemical constituents, use etc. According to old study, the mouth ulcer is mainly coursed by acid secretion and the main aim of this article to decrease the acid secretion so autonomically decrease the ulcer. In the perception that they are safer and have fewer adverse effects than synthetic medication, natural therapies are more accepted. This review also provides; this herb has introduced a good protocol for treatment of various mouth ulcer. The dual therapy addresses multiple aspects of the condition such as pain relief, inflammation reduction and infection prevention, making it comprehensive and effective treatment option.
REFERENCES

Viddya Pattiwale, Snehal Chaudhari, Sanket Patil, A Comprehensive Review on Herbal Gel for the Management of Mouth Ulcer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 554-574. https://doi.org/10.5281/zenodo.17803821
 10.5281/zenodo.17803821
10.5281/zenodo.17803821