
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Anuradha College of Pharmacy, Chikhli, Buldhana, Maharashtra 443001
Wound management is a complex process that requires a thorough understanding of the healing process, specific techniques such as primary, secondary, or tertiary closure, and an individual approach tailored to patient needs. Key strategies involve comprehensive assessment, meticulous cleaning with saline solutions, and the selection of suitable dressings that ensure an optimal healing environment while accounting for nutritional support. The management process begins with wound assessment, which includes an initial inspection for signs of redness, warmth, swelling, discoloration, drainage, and the condition of sutures. Understanding wound characteristics is crucial; this involves identifying the type of wound (acute or chronic), determining its size and depth, and checking for any infection or necrotic tissue. It is also essential to consider patient-specific factors such as overall health, nutritional status, and any underlying medical conditions, as these can significantly impact the healing process. Wound healing is a complex biological process of recovering devitalized cellular structures with four overlapping phases involving hemostasis, inflammation, proliferation, and remodeling. Effective therapies for wound healing using natural products are highly beneficial for patients due to their easy accessibility and low cost. This work proposed a comprehensive review of natural products for wound healing based on bioactivities from plants and animals, providing an overall picture of the chemical origin of natural products to biological wound healing mechanisms. The main four primary bioactivities of natural products, including anti-inflammation, anti-oxidant, antibacterial, and collagen promotion, are utilized to classify and investigate the targeting phases. Data tables containing detail of origin, bioactivity, targeting phase, experimental model, and type of wound were also provided for readers.
Wound management is a complex process that requires a thorough understanding of the healing process, specific techniques such as primary, secondary, or tertiary closure, and an individual approach tailored to patient needs (1). Key strategies involve comprehensive assessment, meticulous cleaning with saline solutions, and the selection of suitable dressings that ensure an optimal healing environment while accounting for nutritional support. The management process begins with wound assessment, which includes an initial inspection for signs of redness, warmth, swelling, discoloration, drainage, and the condition of sutures (2). Understanding wound characteristics is crucial; this involves identifying the type of wound (acute or chronic), determining its size and depth, and checking for any infection or necrotic tissue. It is also essential to consider patient-specific factors such as overall health, nutritional status, and any underlying medical conditions, as these can significantly impact the healing process (3). Wound healing can occur through three primary processes: primary closure, where wound edges are sutured surgically together; secondary intention, in which the wound is left open to heal naturally through granulation and re-epithelialization; and tertiary intention, where the wound is initially open for cleaning and is closed surgically after a period of secondary healing (4, 5). Effective wound cleaning is vital; saline solutions should be used carefully around the wound edges to promote healing without causing harm. For wounds that accumulate excess fluid, drainage systems such as Penrose, Hemovac, or Jackson-Pratt drains may be necessary. Additionally, nutritional support plays a critical role, particularly for patients with extensive wounds, who may require enhanced protein and calorie intake to support healing. Wound dressings serve several purposes, including protecting the wound, maintaining a moist environment conducive to healing, and absorbing any exudates (6). Various types of dressings are available, such as highly absorbent foam and alginate dressings for heavy exudation, hydrogel dressings that assist in the autolysis of necrotic tissue, and iodine or silver dressings used specifically for infection management. The choice of dressing must align with the wound characteristics and the patient's specific needs, with frequent changes necessary for heavily exuding wounds to prevent maceration of surrounding skin. Infection management involves regular monitoring of the wound for signs of infection and adapting treatment strategies accordingly (7). Occlusive dressings should be avoided in infected wounds, and specific antimicrobial treatments may be warranted. Patient education is also essential, as it empowers patients and caregivers to recognize infection signs and seek timely treatment (8, 9). The wound healing process is a cascade of synchronized events aimed at restoring skin integrity. This article aims to present an overall outline of the acute cutaneous wound healing process while other articles within this series will address chronic wounds, experimental skin substitutes, and abnormal wound healing (keloids and hypertrophic scars) (10-11).
2. PHASES OF WOUND HEALING
Overall wound healing involves three overlapping phases: hemostasis and inflammation, proliferation, and remodeling. Each of these processes is critical; deficiencies in any phase can impair the body’s ability to heal wounds (Figure 1).
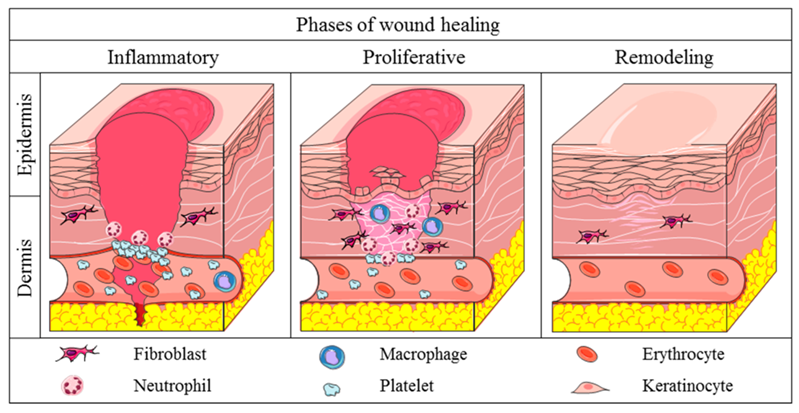
Figure 1: Phases of Wound Healing
The hemostasis phase begins immediately after skin injury, characterized by blood vessel constriction and platelet activation upon contact with exposed collagen. This activation releases granules that promote further platelet aggregation and initiate the coagulation cascade, leading to the formation of a provisional fibrin matrix within the wound. Concurrently, activated platelets secrete cytokines such as transforming growth factor-β (TGF-β) and platelet-derived growth factor to attract neutrophils and macrophages, signaling the onset of the inflammatory phase (12-14). Neutrophils are the first responders in this phase, although research indicates that healing can proceed without them, unlike macrophages, which are essential for effective wound healing. Derived from activated monocytes, macrophages support phagocytosis and secrete additional cytokines and growth factors that drive fibroblast proliferation, angiogenesis, and keratinocyte migration. In diabetic wounds, dysregulated macrophage function has been linked to impaired healing. The proliferative phase starts within 2 to 3 days post-injury, lasting up to 3 weeks, during which fibroblasts arrive at the wound site, producing disorganized collagen predominantly made of immature type III collagen (15). Cytokines can induce fibroblasts to convert into myofibroblasts, enhancing collagen production and wound contraction. Numerous signaling pathways, including those involving angiotensin II and TGF-β, are implicated in regulating this phase. In the final remodeling phase, granulation tissue transitions to a permanent scar, with net collagen production continuing for 4 to 5 weeks and type III collagen being replaced by type I collagen over the course of a year. Zinc-dependent matrix metalloproteinases, secreted by epidermal cells, play a crucial role in the remodeling process. The tensile strength of the healed tissue increases from 3% at one week to 20% at three weeks, peaking at 80% of uninjured skin strength after three months, without ever returning to full strength (16-18).
3. MANAGEMENT OF WOUND
Wound management involves a systematic approach to treating wounds aimed at promoting healing through actions such as cleaning, debriding, and dressing the wound. The primary goals are to maintain a clean and moist environment, which facilitates faster healing and minimizes scarring. Key considerations in wound management include assessing the wound's size, depth, and severity to identify the appropriate treatment strategy, selecting suitable dressings based on the wound's characteristics, and ensuring proper hygiene when changing dressings to prevent infection. One of the fundamental principles is to keep the wound clean and moist, as this environment encourages healing. Regular monitoring for signs of infection—such as increased swelling, redness, pus, or other abnormal drainage—is crucial for successful wound management. Different types of wounds require specialized attention. For example, minor burns should be cooled with water and cleaned gently, while chronic wounds may necessitate specific treatments like compression therapy. Puncture wounds often require an open drainage approach and should be kept moist per medical advice. Professional and advanced treatment options include surgical closure methods like sutures, staples, or medical glue for wounds that can be closed. Delayed primary closure is an approach for high-risk wounds, where cleaning is performed initially, and closure follows once the wound appears infection-free. Moreover, negative pressure wound therapy (NPWT) employs a vacuum-assisted system to enhance healing in complicated cases. In more severe circumstances, hyperbaric oxygen therapy can be administered, providing 100% oxygen in a pressurized context, known to assist in the healing of complex wounds. Overall, effective wound management necessitates a careful assessment, regular follow-up, and, when necessary, consultation with healthcare professionals for advanced interventions (19-21).
4. HERBAL MANAGEMENT OF WOUNDS
From the literature search, we collected a list of 137 research articles relating natural compounds for wound healing. We classified them into groups regarding their bioactivities (i.e., anti-inflammation, anti-oxidant, antibacterial, collagen promotion, etc.)(22-24) . The origin of those compounds (i.e., plant and animal) was also considered. Among bioactivities, anti-inflammation, anti-oxidant, anti-bacterial, and collagen promotion are studied the most. Therefore, in this study, we focused our discussion on natural compounds regarding these bioactivities. A data table containing a list of those literature and the compounds were provided in the Supplementary (25-27).
4.1 Myricetin
Myricetin (Myr) is a flavonoid that has been reported for wound healing. Myricetin is present in many fruits and has many biochemical properties such as antioxidant, anti-allergic, anti-inflammation, and immunomodulatory function. Myr affects inflammatory cytokines such as tumor necrosis factor-α (TNF-α), cluster of differentiation 68 (CD68), as well as interleukin-1β (IL-1β). Myr also showed increased expression of serum proinflammatory cytokines (e.g., IL-1β and TNF-α) and decreased expression of macrophage CD68. The above findings suggest that Myr could be used therapeutically in wound healing by enhancing inflammatory cytokines and systemic reorganization. Other than that, Sklenarova et al. investigated Myr’s ability to heal wounds. This study showed the inhibition of proinflammatory cytokines production (e.g., IL-6 and IL-8) in skin cells by Myr.
4.2 Calophyllolide (CP)
Calophyllolide (CP) is isolated from Calophyllum inophyllum Linn and has been reported with anti-inflammatory, anti-microbial, and anti-coagulant activities. Nguyen et al. studied the long-lasting anti-inflammatory effects of CP in the healing process. They showed that CP treatment suppresses prolonged inflammation by downregulating IL-1β, IL-6, TNF-α, and upregulating IL-10. Moreover, CP inhibits MPO activity and increases M2 macrophage bias through upregulating M2-associated gene expression, leading to benefits in wound healing.
4.3 Steroidal Glycoside
Steroidal glycoside is extracted from Lilium longiflorum Thunb. Di et al. confirmed that wound treatment with steroidal glycosides would upregulate early inflammatory genes such as IL2, IL4, IL10, CD40LG, IFNG, and CXCL11, remodeling genes like CTSG, F13A1, FGA, MMP and PLG). Concurrently, wound treatment with steroidal glycosides also displayed a selective downregulation of genes regarding inflammation (CXCL2 and CCL7) and regeneration (MMP7 and PLAT). The above findings suggest an impact of wound treatment with steroidal glycosides on wound healing, leading to early termination of the inflammatory response and shortening the early stages of tissue regeneration.
4.4 Curcumin
Curcumin is mainly extracted from turmeric (Curcuma longa L.) and has shown several bioactive properties such as anti-inflammatory, antioxidant, and anti-coagulant. Several studies demonstrated curcumin’s wound healing effects as an antioxidant. Phan et al. confirmed that curcumin protects human dermal fibroblasts and epidermal when exposed to hydrogen peroxide and superoxide radicals. Gadekar et al. evaluated the protective potential of curcumin against keratinocytes and fibroblasts in H2O2-induced injury. Through the antioxidant activity, Bonte et al. also demonstrated that curcumin protects human keratinocytes from xanthine oxidase damage [202]. Mohanty et al. reported the ability of curcumin to reduce ROS and lipid peroxidation, thereby reducing the activation of antioxidant enzymes after wound treatment in rats.
4.5 Catechin
Catechin is a flavonoid with good antioxidant activity; it plays a beneficial role in physiological activity. Baek et al. prepared a PCL/(+)-catechin/gelatin film and evaluated its applicability for wound treatment. The results show that PCL/(+)- catechin/gelatin film prevents harmful factors from the outside, and reduces oxidative stress at the wound effectively to help the wound heal. Zhao et al. confirmed that the EGCG-3-acrylamido phenyl boronic acid-acrylamide (EACPA) hydrogel has antioxidant, antibacterial, antiinflammatory, and proangiogenic effects, and modulates macrophage polarity to accelerate wound healing, also facilitates easy dressing change.
5. CONCLUSION
Wound healing is a complex biological process of recovering devitalized cellular structures with four overlapping phases involving hemostasis, inflammation, proliferation, and remodeling. Effective therapies for wound healing using natural products are highly beneficial for patients due to their easy accessibility and low cost. This work proposed a comprehensive review of natural products for wound healing based on bioactivities from plants and animals, providing an overall picture of the chemical origin of natural products to biological wound healing mechanisms. The main four primary bioactivities of natural products, including anti-inflammation, anti-oxidant, antibacterial, and collagen promotion, are utilized to classify and investigate the targeting phases. Data tables containing detail of origin, bioactivity, targeting phase, experimental model, and type of wound were also provided for readers.
6. CONFLICT OF INTEREST
None
REFERENCES

Divya Utkar, Dr. Kailash Biyani, Dr. Pavan Folane, A Comprehensive Review on Wounds and its Herbal Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3656-3662. https://doi.org/10.5281/zenodo.18062100
 10.5281/zenodo.18062100
10.5281/zenodo.18062100