
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Swathi College of Pharmacy, Venkatachalam, Nellore
Gastritis is a common gastrointestinal condition characterized by inflammation of the gastric mucosa, resulting from multiple etiological factors such as Helicobacter pylori infection, unhealthy dietary habits, stress, medication use, and lifestyle practices. It may present in acute or chronic forms, leading to symptoms ranging from mild discomfort to severe complications including ulcers and mucosal damage. This prospective study aims to identify the major triggering factors of gastritis among patients and to evaluate current management approaches adopted to reduce symptoms and prevent complications. A total of 70 subjects were assessed to determine the prevalence of gastritis-related symptoms and contributing risk factors. Data were collected through structured questionnaires focusing on demographic characteristics, dietary behavior, lifestyle habits, symptom patterns, medication history, and previous diagnosis of gastritis. The findings reveal that females constituted the majority of cases (81.4%), with most participants falling between 19–21 years of age. Burning sensation (51.6%), loss of appetite (29%), vomiting (24.2%), and heartburn (19.4%) were the most commonly reported symptoms. Dietary triggers such as spicy foods were frequently associated with symptom aggrevation, as 57.1% consumed spicy foods sometimes and 10% consumed them frequently. Additional contributing factors included skipping meals (48.6%), consumption of carbonated drinks (54.3%), coffee or tea intake (38.6%), stress (34.3%), and self-medication (55.7%). Medication-related gastritis was less common, with only 8.6% reporting regular NSAID use. Management practices varied among participants, with many adopting home remedies (32.9%), rest (37.1%), or visiting a doctor (22.9%) for symptom relief. The study concludes that modifiable lifestyle and dietary factors play a major role in triggering gastritis, especially among young adults. Early diagnosis, appropriate medication, and long-term lifestyle modifications are essential for effective management and prevention of recurrent gastritis episodes.
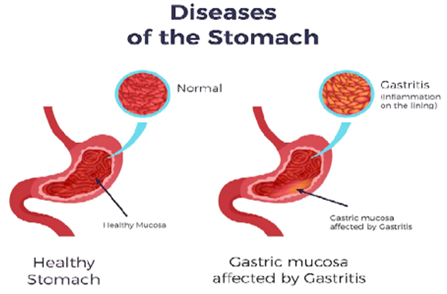
Gastritis is the inflammation of the gastric mucosa and is often used to describe the abnormal appearance of abnormal gastric mucosa on endoscopy or radiology. Gastritis encompasses infectious or immunological inflammation of the gastric mucosa and the host response. Histopathological evidence of inflammation in the stomach lining is essential to diagnose this condition. Gastropathy is a gastric mucosal disorder without inflammation, featuring epithelial injury and subsequent regeneration. Gastritis and gastropathy are not mutually exclusive conditions and might sometimes coexist. In clinical practice, gastritis may be accompanied by signs of mucosal injury, whereas gastropathy may present with an inflammatory reaction in the gastric mucosa.1
Gastritis is classified based on the acuity of the condition (acute versus chronic), the histological features of inflammation, or the etiology. Although the categorization and classification of gastritis are not universally accepted, understanding the histological characteristics and etiological factors associated with the different types of gastritis is essential. Appropriate histological evaluation is also essential in devising management plans for this disease. The primary objective is to equip treating clinicians with the ability to improve patient outcomes through early intervention.2
The membranes lining the stomach wall protect it from acid and germs. If this protective lining is irritated or damaged, it can become inflamed. Long-lasting inflammations can further damage the stomach lining and lead to stomach (gastric) ulcers. Inflammation of the stomach lining is called gastritis. It's usually caused by certain bacteria or the regular use of anti-inflammatory painkillers. There are two kinds of gastritis: acute and chronic. Acute gastritis is typically accompanied by very noticeable stomach and bowel problems that usually go away again on their own after a few days. Chronic gastritis, on the other hand, may go unnoticed or damage the lining of the stomach over time. Sometimes it is not discovered until stomach ulcers have developed, which then cause noticeable symptoms.3
Strictly speaking, the label ‘gastritis’ should only be applied to histologically-proven inflammatory lesions of the gastric mucosa. The etiological classification of gastritis is based on this histological definition. A semantic distinction between gastritis and gastropathies identifies the latter as gastric mucosal abnormalities with a minimal/focal inflammatory component. From a practical standpoint, however, subjective variability in the histological assessment of the inflammatory infiltrate makes the border between the two morphological entities hazy, and the diagnostic label of gastritis is the most often applied. In clinical practice as well as for research's purposes, gastric endoscopy couples the priority of assessing the topography/phenotype of the lesions, with the need of obtaining the mucosal samples for histological diagnosis. At endoscopy, gastric mucosal inflammation features either a reddening or edema of the gastric mucosa, but neither of these endoscopic features are pathognomonic. In a recent study on the accuracy of standard endoscopic imaging for the detection of Helicobacter pylori (H. pylori) gastritis, Okamura and coworkers reported an accuracy of 89% for nodularity, and 77% for mucosal swelling. High-definition endoscopy and virtual chromo-endoscopy (narrow-band imaging, blue light imaging, and linked color imaging) have significantly improved the accuracy of endoscopic gastritis assessment. Mucosal atrophy is considered the cancerization field of gastric malignancies development, which makes crucial its endoscopically/histological assessment .This review addresses the most frequently applied criteria in gastritis classification, the biological rationale behind the endoscopic biopsy sampling (including the biological diversity of the native gastric mucosa), the basic-phenotypes and the clinico-pathological “models of gastritis”, and, finally, the format a histological report potentially consistent with the clinical expectancies.4
SYMPTOMS
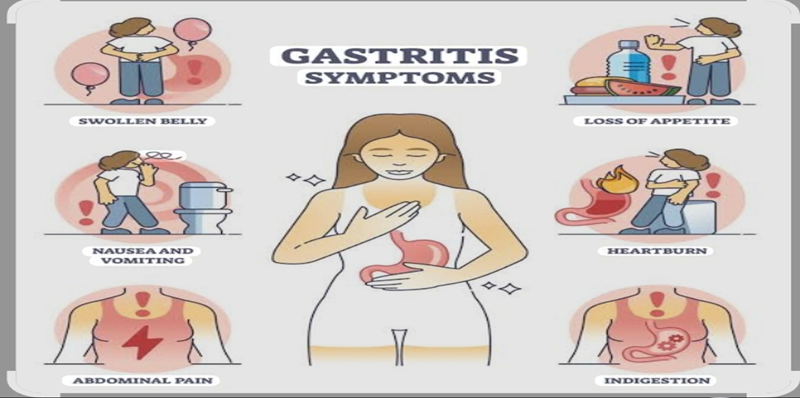
Fig -1
CAUSES
Some potential causes of gastritis may include the following
Gastritis is most commonly due to H. pylori bacteria. Around 35% of people-trusted Source in the U.S. have these bacteria in their bodies.
Reactive gastritis, which is caused by irritants, is also relatively common. It affects around 15% of people Trusted Source in the U.S. NSAIDs such as ibuprofen (Advil) and some other common pain relief drugs can cause stomach irritation and gastritis. NSAIDs represent the most common cause of stomach ulcers.5
Autoimmune conditions can lead to gastritis. In people with autoimmune a trophic gastritis, the immune system attacks the stomach lining.
Physical trauma or damage to the stomach lining can also lead to gastritis. For example, a person who has undergone surgery to remove part of their stomach may develop postgastrectomy gastritis, which causes the lining to degenerate6
Dietary factors do not usually cause gastritis, but food allergies can contribute to it. Some types of gastritis that stem from other issues include:
Eosinophilic gastritis:
This can result from an allergic reaction. This is rare. It involves the development of thick folds and cysts on the stomach wall.7
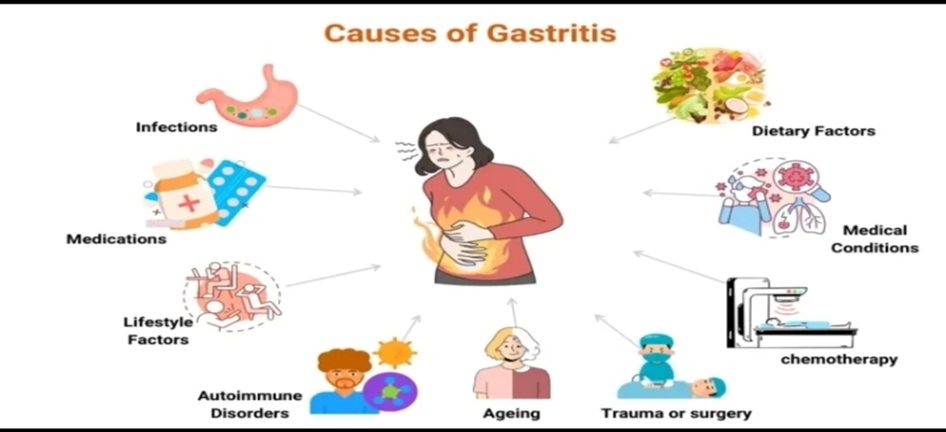
Fig - 2
RISK FACTOR
Some people, including older adults and individuals with compromised immune function, are more likely trusted Source to develop gastritis.
Some risk factors for gastritis include:

Fig - 3
CLASSIFICATION
Acute gastritis is temporary stomach lining inflammation caused by stress on the gastric mucosa, manifesting as either hemorrhagic or non-hemorrhagic symptoms. This condition can develop due to various factors, including uremia, ischemia, shock, corrosive agents, medications, radiation, trauma, severe burns, sepsis, or alkaline-bile reflux. Certain infections, such as enteroviruses, can also cause a self-limited episode of gastritis. Acute gastritis may result from reduced gastric mucus secretion, mucosal barrier disruption, or decreased mucosal blood flow, depending on the underlying cause.8
Chronic gastritis is categorized into 2 forms—atrophic and non-atrophic. The primary cause of chronic gastritis is a Helicobacter pylori infection, which typically starts with a non-atrophic morphology. The non-atrophic form of chronic gastritis can progress to atrophic without treatment. The most common cause of atrophic chronic gastritis is autoimmune gastritis, though the etiology remains unclear. Autoimmune gastritis exhibits a chronic mononuclear inflammation accompanied by severe atrophic gastritis, which usually affects the corpus, along with the presence of autoantibodies against parietal cells or the intrinsic factor. However, whether autoimmune gastritis is an independent disorder or if an H pylori infection triggers the autoimmune response in susceptible individuals is unclear.9
Reactive gastritis or gastropathy has numerous causative factors with acute gastritis. Reactive gastritis may be caused by specific medications, alcohol consumption, radiation exposure, and duodenal (bile) reflux. These causative agents lead to histological mucosal lesions characterized by low-grade inflammation of the gastric mucosa. Although usually asymptomatic, they are revealed through endoscopy, often showing multiple erosions or ulcers without signs of atrophic changes. The use of immune checkpoint inhibitors to treat various malignancies has contributed to the incidence of reactive gastritis, although the condition remains considerably rare.10
The Histological Division of the Sydney System was introduced in 1990 and has since become the most widely cited classification system for the morphological features of gastritis in endoscopic biopsies. This system conveys information about the type, severity, and extent of gastric pathology. The classification system conveys the topography of gastritis, which can be restricted to the antrum or corpus or involve the entire stomach (pan gastritis). If the etiology of the disease is known, this is added as a prefix to denote the topography. For instance, the label "autoimmune corpus gastritis" is used if the disease is autoimmune.11
The Sydney System of Classification further delineates 5 graded morphological variables that may be added as a suffix to the core topography. These variables include the type or chronicity of inflammation, gastritis activity, intestinal metaplasia, the extent of atrophy, and the presence or absence of Heliobacter pylori. The morphological features are graded as absent, mild, moderate, or severe. The Sydney System of Classification recommends at least 2 random biopsies from both the antrum and corpus, along with an additional biopsy from the incisura angularis. Although the classification system provides a standardized and concise means of documenting the extent and severity of gastritis, the method for predicting or forecasting future morphological changes is impossible.12
Classification of Gastritis Based on Etiological Factors
An alternative approach to classifying gastritis considers the etiology and chronicity of the inflammation. This approach categorizes gastritis into 3 main subtypes—acute, chronic, and special. Infectious gastritis is most commonly attributed to the global prevalence of H pylori infection. Other types of infectious gastritis include phlegmonous gastritis (caused by pyogenic bacteria), mycobacterial gastritis (caused by Mycobacterium tuberculosis), syphilitic gastritis, viral gastritis (caused by cytomegalovirus and herpes simplex virus), parasitic gastritis (caused by Anisakis, Cryptosporidium, Ascaris lumbricoides, Giardia, Toxoplasma, and Schistosoma), and fungal gastritis (caused by Candida, Aspergillus, Mucor, Coccidioides, Histoplasma, Cryptococcus neoformans, Pneumocystis carinii, and Torulosis glabrata).13
Granulomatous gastritis is a special gastritis observed in patients with Crohn disease and sarcoidosis. Lymphocytic gastritis, collagenous gastritis, and eosinophilic gastritis are additional special subtypes of gastritis with unclear etiologies. Lymphocytic and collagenous gastritis have been associated with celiac disease, whereas eosinophilic gastritis has a strong connection to atopic conditions and food allergens.14
According to the 2015 Kyoto Consensus Conference, a classification of gastritis based on etiological factors is outlined as follows:
with acute gastritis. Reactive gastritis may be caused by specific medications, alcohol consumption, radiation exposure, and duodenal (bile) reflux. These causative agents lead to histological mucosal lesions characterized by low-grade inflammation of the gastric mucosa. Although usually asymptomatic, they are revealed through endoscopy, often showing multiple erosions or ulcers without signs of atrophic changes. The use of immune checkpoint inhibitors to treat various malignancies has contributed to the incidence of reactive gastritis, although the condition remains considerably rare15.
The Sydney System of Classification for Gastritis
The Histological Division of the Sydney System was introduced in 1990 and has since become the most widely cited classification system for the morphological features of gastritis in endoscopic biopsies. This system conveys information about the type, severity, and extent of gastric pathology. The classification system conveys the topography of gastritis, which can be restricted to the antrum or corpus or involve the entire stomach (pan gastritis). If the etiology of the disease is known, this is added as a prefix to denote the topography. For instance, the label "autoimmune corpus gastritis" is used if the disease is autoimmune.16
The Sydney System of Classification further delineates 5 graded morphological variables that may be added as a suffix to the core topography. These variables include the type or chronicity of inflammation, gastritis activity, intestinal metaplasia, the extent of atrophy, and the presence or absence of Heliobacter pylori. The morphological features are graded as absent, mild, moderate, or severe.17 The Sydney System of Classification recommends at least 2 random biopsies from both the antrum and corpus, along with an additional biopsy from the incisura angularis. Although the classification system provides a standardized and concise means of documenting the extent and severity of gastritis, the method for predicting or forecasting future morphological changes is impossible.18
Classification of Gastritis Based on Etiological Factors
An alternative approach to classifying gastritis considers the etiology and chronicity of the inflammation. This approach categorizes gastritis into 3 main subtypes—acute, chronic, and special. Infectious gastritis is most commonly attributed to the global prevalence of H pylori infection. Other types of infectious gastritis include phlegmonous gastritis (caused by pyogenic bacteria), mycobacterial gastritis (caused by Mycobacterium tuberculosis), syphilitic gastritis, viral gastritis (caused by cytomegalovirus and herpes simplex virus), parasitic gastritis (caused by Anisakis, Cryptosporidium, Ascaris lumbricoides, Giardia, Toxoplasma, and Schistosoma), and fungal gastritis (caused by Candida, Aspergillus, Mucor, Coccidioides, Histoplasma, Cryptococcus neoformans, Pneumocystis carinii, and Torulosis glabrata).19
Granulomatous gastritis is a special gastritis observed in patients with Crohn disease and sarcoidosis. Lymphocytic gastritis, collagenous gastritis, and eosinophilic gastritis are additional special subtypes of gastritis with unclear etiologies. Lymphocytic and collagenous gastritis have been associated with celiac disease, whereas eosinophilic gastritis has a strong connection to atopic conditions and food allergens.20
According to the 2015 Kyoto Consensus Conference, a classification of gastritis based on etiological factors is outlined as follows:
Pathophysiology
H pylori–Associated Gastritis
H pylori is a flagellated gram-negative bacterium transmitted through environmental factors or the fecal-oral or oral-oral routes. The pathophysiology of H pylori–induced gastritis involves a complex interaction between bacterial virulence factors and the host's immune responses.21 This interplay disrupts the gastric mucosal barrier and leads to chronic inflammation. H pylori possess virulence factors that facilitate cell adhesion, cause cell damage, disrupt tight junctions, and evade the host immune response. Notably, the cytotoxin-associated gene A (CagA) is a potent inducer of inflammation and is associated with the development of gastric cancer.22
The survival and colonization of H pylori in the stomach depend on the urease produced by the bacterium. Urease catalyzes urea hydrolysis, releasing ammonia and forming a protective layer around the bacterium.23 The ammonia also helps neutralize the acidic micro environment of the stomach, allowing the bacterium to thrive in the stomach's low pH conditions. Subsequently, the flagellum and other mucolytic enzymes assist the organism in penetrating the mucus layer and reaching the gastric epithelium, which attaches to the epithelial cells.24
which is the distinguishing characteristic of gastritis. Host macrophages and activated T-cells take up various antigenic substrates from the organism.[18] The recruited T-cells are paradoxically inhibited by the expression of B7-H1 (programmed death-1 ligand 1) on gastric epithelial cells.25Studies have shown that H pylori induce B7-H1 expression on gastric epithelial cells, which is believed to contribute to the chronicity of the bacterial infection.] Further stimulation of inflammation occurs through an H pylori–induced increase in interleukin (IL)-8 production by the gastric epithelial cells.IL-8 subsequently triggers the activation of neutrophils and the recruitment of other inflammatory cells into the mucosa. Persistent inflammation ultimately leads to the depletion of gastrin-producing (G) cells and acid-producing parietal cells in the gastric mucosa. Over time, atrophy and intestinal metaplasia develop.26
Autoimmune Gastritis
Autoimmune metaplastic atrophic gastritis develops due to T-cell–mediated destruction of the oxyntic mucosa and the production of autoantibodies targeting parietal cells and the intrinsic factor.27 A proposed mechanism for this disease in patients with H pylori-induced atrophic gastritis outlines a crossover of antigenic activity directed against the bacterium and toward host antigens in the region, including parietal cells and the intrinsic factor.28 In primary autoimmune atrophic gastritis, the immune response is directed against these antigens irrespective of an H pylori infection. However, the molecular factors driving the autoimmune response and initiating the pathogenesis of the condition remain unidentified29. Over time, the immune-mediated destruction of the oxyntic mucosa leads to mucous cells and metaplastic glands within the gastric mucosa, including both intestinal and pseudo-pyloric.30
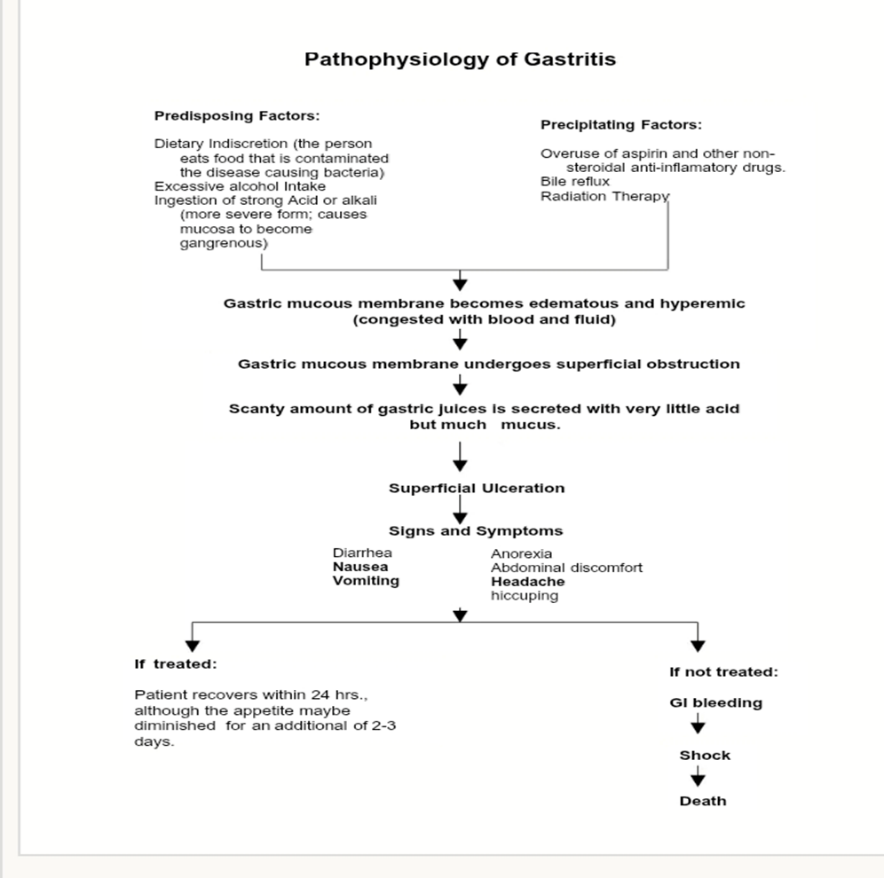
Fig - 4
TREATMENT
Gastritis is treated in various ways, depending on what the symptoms and causes are, and how severe the inflammation is
It is important to avoid alcohol and nicotine (smoking) if you have acute gastritis. Doctors commonly recommend eating food that is gentle on your stomach, like toast or porridge while avoiding coffee and foods that are greasy or spicy. Getting some rest is also advisable. They also often recommend eating either small portions or nothing at all for 1 to 2 days. There has hardly been any scientific research on whether these things can help, though.31
If you notice that stress is making your stomach problems worse, you can try coping with it differently and look for ways to relax more in your everyday life.32
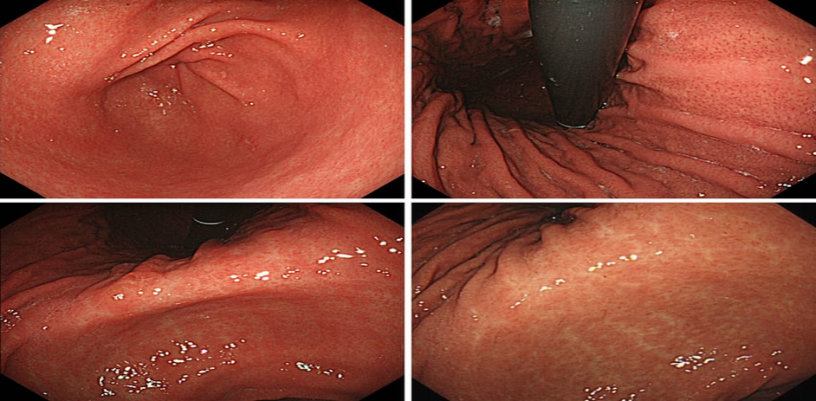
Fig - 5
If the problems don't go away or are very severe, gastritis is usually treated with medication that reduces the amount of acid. Until the symptoms go away, the following medications can be used, depending on the type and severity of the symptoms:
Antacids like aluminium hydroxide or magnesium hydroxide neutralize the acid already in your stomach.
Proton pump inhibitors (PPIs) like omeprazole or pantoprazole reduce the production of stomach acid33.
H2 blockers such as ranitidine and famotidine also reduce acid production.
If the gastritis is caused by a Helicobacter infection, proton pump inhibitors are combined with two or three antibiotics34.
RESULTS
DATA ON DISTRIBUTION OF PATIENTS ON GENDER:
Total distribution of patient with respect to the gender shows that, out of 70 patients ,57 patients (81.4) were female and male 13 patients (17.1) were resulted with ischemic stroke.
Table 1: Gender distribution of patients
|
Sr. No |
Age |
Number Of Prescriptions |
Percentage (%) |
|
1 |
Female |
58 |
81.4% |
|
2 |
Male |
13 |
17.1% |
|
Total |
|
71 |
100 |
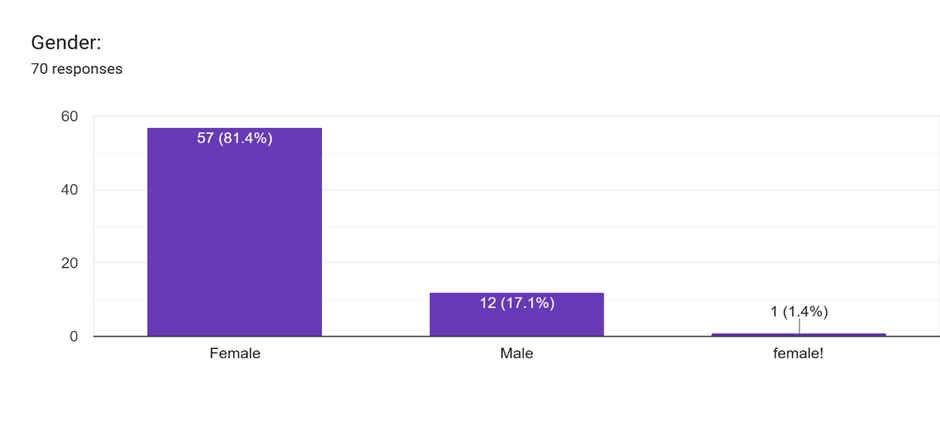
Figure 7 : Distribution of patients based on gender
DATA ON DISTRIBUTION OF PATIENTS BASED ON AGE
Total distribution of patient with respect to the age group majority of the patients were found to be between the age group of 18 year (4.3%),followed by >19 year (18.6%), and this age group >20 (38.6%),many of years are having (27%) 21-36 years.
Table 2: Age distribution of patients
|
Sr. No |
Age |
No of Prescriptions |
Percentage |
|
1 |
18 |
3 |
4.3% |
|
2 |
19 |
13 |
18.6% |
|
3 |
20 |
27 |
38.6% |
|
4 |
21 |
13 |
18.6% |
|
5 |
22 |
5 |
7.1% |
|
6 |
23 |
4 |
5.7% |
|
7 |
24 |
3 |
4.3% |
|
8 |
25 |
1 |
1.4% |
|
9 |
36 |
1 |
1.4% |
|
TOTAL |
|
70 |
100 |
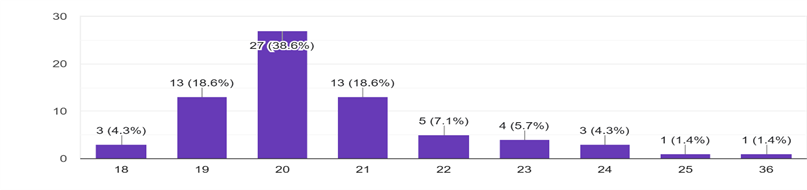
Figure 8: Distribution of patients based on age
DATA ON DISTRIBUTION BASED ON SYMPTOMS:
These symptoms are associated with the gastritis were out of 70 patients, loss of appetite is having 18 patients (29%) , burning sensation are 32 (51.6%) , vomiting are having 15 patients (24.5%), heartburn are having 12 patients (19.4%), bloating are having 5 patients (8.1%) ,acid reflux are having 4 patients (6.5%).
Table 2: Symptoms of patients
|
Sr. No |
Symptoms |
Number of Prescriptions |
Percentage |
|
1 |
Loss Of Appetite |
18 |
29% |
|
2 |
Burning Sensation |
32 |
51.6% |
|
3 |
Vomiting |
15 |
24.2% |
|
4 |
Heartburn |
12 |
19.4% |
|
5 |
Bloating |
5 |
8.1% |
|
6 |
Acid Reflux |
4 |
6.5% |
|
TOTAL |
|
86 |
100 |
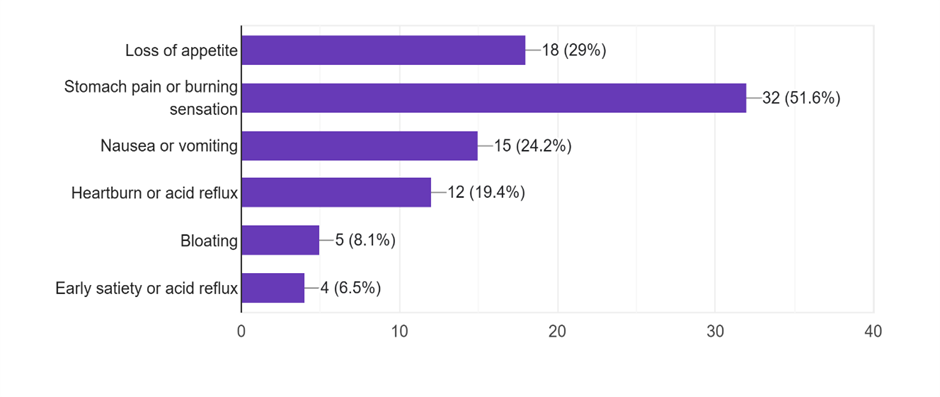
Figure 8: Distribution of prescriptions based on symptoms
DATA ON DISTRIBUTION BASED ON SPICY FOOD
Out of 70 patients are having the spicy food the rarely 25 patients (35.7%) , sometimes 40 patients (57.1%) , frequently 7 patients (10%) .
Table 3: Spicy food of patients
|
Sr. No |
Spicy Food |
Number Of Prescriptions |
Percentage % |
|
1 |
Rarely |
25 |
35.7% |
|
2 |
Sometimes |
40 |
57.1% |
|
3 |
Frequently |
07 |
10% |
|
Total |
|
72 |
100 |
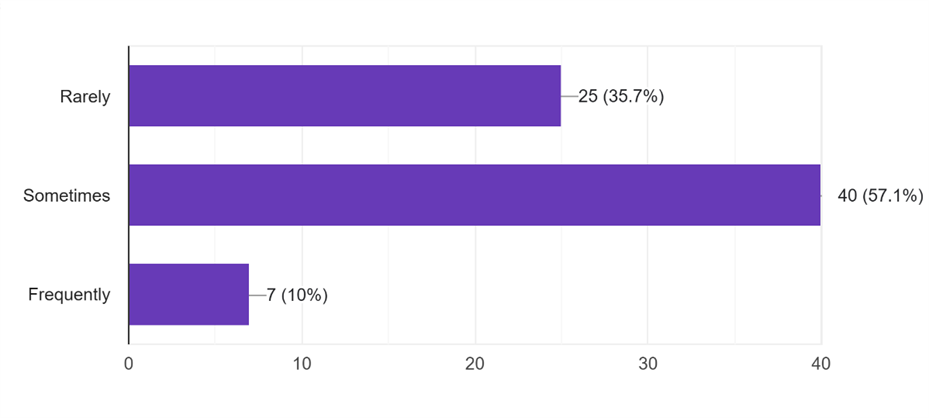
Figure 9: Distribution of prescriptions based on spicy food
DATA ON DISTRIBUTION BASED ON SKIP MEALS
Out of 70 patients are having the skip meals were having 34 patients (48.6%) to the yes , were having 37 patients (52.9%) to the no.
Table 4: Skip Meals Of Patients
|
Sr. No |
Skip Meals |
Number Of Prescriptions |
Percentage % |
|
1 |
Yes |
34 |
48.6% |
|
2 |
No |
37 |
52.9% |
|
Total |
|
71 |
100 |
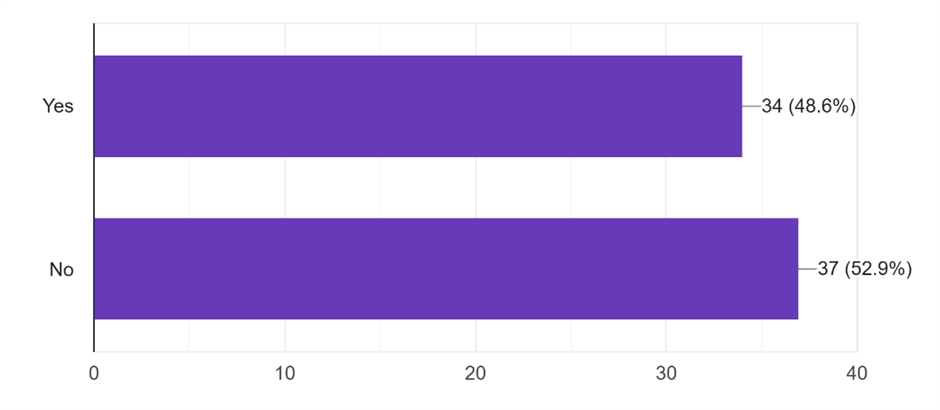
Figure 10: Distribution of prescriptions based on skip meals
DATA ON DISTRIBUTION BASED ON DRINK COFFEE / TEA
Out of 70 patients are having the drink coffee or tea , none of the 43 patients (61.5%) ,were 1-2 are having 27 patients (38.6%), were 3 or more are having 2 patients (2.9%).
Table 5: Drink Coffee and Tea
|
Sr. No |
Drink Coffee / Tea |
Number Of Prescriptions |
Percentage % |
|
1 |
None |
43 |
61.5% |
|
2 |
1-2 |
27 |
38.6% |
|
3 |
3 Or More |
2 |
2.9% |
|
Total |
|
72 |
100 |
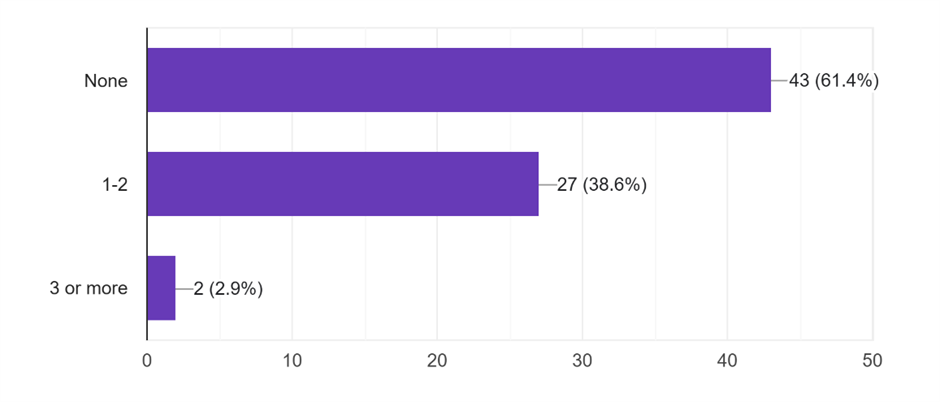
Figure 11: Distribution of prescriptions based on drink coffee / tea
DATA ON DISTRIBUTION BASED ON CARBONATED DRINKS
Out of 70 patients are having the carbonated drinks were having 32 patients (45.7%) to the no , were having 38 patients (54.3%) to the yes.
Table 6: Carbonated Drinks of Patients
|
Sr. No |
Carbonated Drinks |
Number Of Prescriptions |
Percentage % |
|
1 |
No |
32 |
45.7% |
|
2 |
Yes |
38 |
54.3% |
|
Total |
|
70 |
100 |
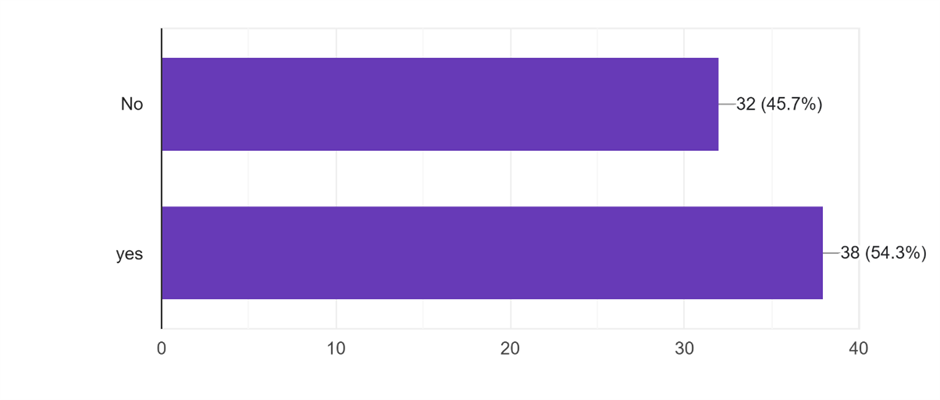
Figure 12: Distribution of prescriptions based on carbonated drinks
DATA ON DISTRIBUTION BASED ON DIAGNOSED WITH GASTRITIS
Out of 70 patients are having the diagnosed with gastritis were having 19 patients (27.1%) to the yes , were having 53 patients (75.7%) to the no .
Table 7: Diagnosed with Gastritis of Patients.
|
Sr. No |
Diagnosed With Gastritis |
Number of Prescriptions |
Percentage % |
|
1 |
Yes |
19 |
27.1% |
|
2 |
No |
53 |
75.7% |
|
Total |
|
72 |
100 |
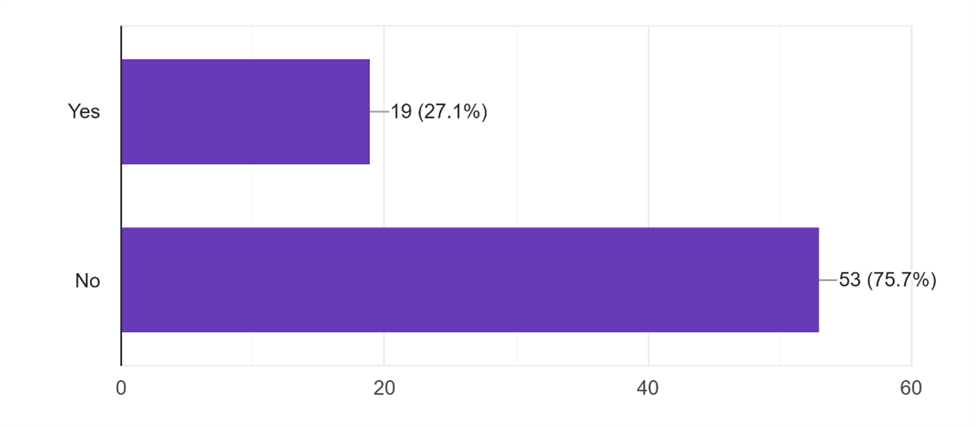
Figure 13: Distribution of prescriptions based on diagnosed with gastritis.
DATA ON DISTRIBUTION BASED ON TAKING ANY REGULARLY DRUGS
Out of 70 patients are taking the regularly drug , pain killer (NSAIDS like ibuprofen, aspirin) 6 patients (8.6%) , steroids 0 patients (0%) , antacids 5 (7.1%) , none 59 patients (84.3%) .
Table 8: Any Drug Intake
|
Sr. No |
Taking Any Regularly Drugs |
Number of Prescriptions |
Percentage % |
|
1 |
Pain Killer |
6 |
8.6% |
|
2 |
Steroids |
0 |
0% |
|
3 |
Antacids |
5 |
7.1% |
|
4 |
None |
59 |
84.3% |
|
Total |
|
70 |
100 |
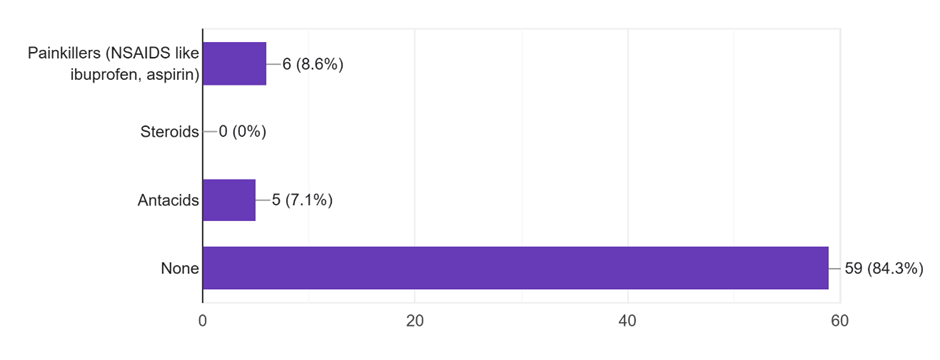
Figure 14: Distribution of prescriptions based on taking any regularly drugs
DATA ON DISTRIBUTION BASED ON SMOKE
Out of 70 patients are having the smoke were having 0 patients (0 %) to the yes , were having 69 patients (98.6%) to the no, and sometimes 1 patients (1.4%).
Table 9: Smoke of Patients.
|
Sr. No |
Smoke |
Number Of Prescriptions |
Percentage % |
|
1 |
Yes |
0 |
0% |
|
2 |
No |
69 |
98.6% |
|
3 |
Sometimes |
1 |
1.4% |
|
Total |
|
70 |
100 |
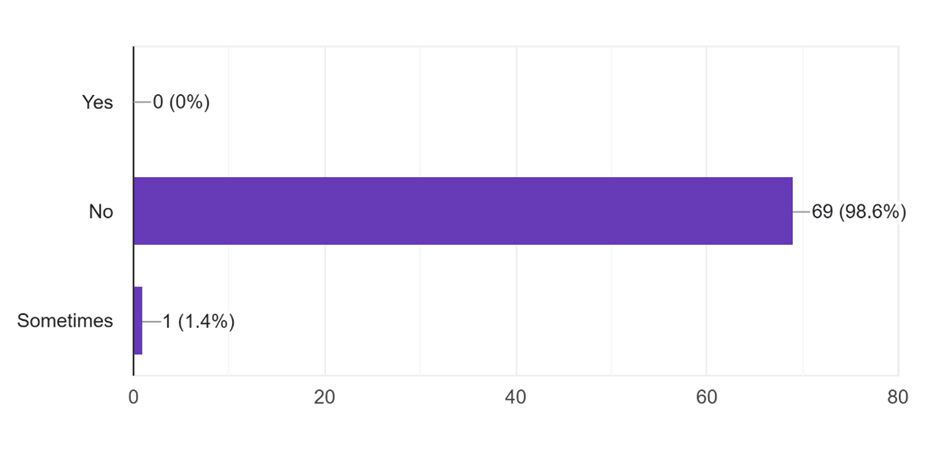
Figure 15 : Distribution of prescriptions based on smoke
DATA ON DISTRIBUTION BASED ON ALCOHOL
Out of 70 patients are having the alcohol were having 1 patients (1.4 %) to the yes , were having 69 patients (98.6%) to the no, and sometimes 1 patients (1.4%).
Table 10 : Alcohol Of Patients.
|
Sr. No |
Alcohol |
Number Of Prescriptions |
Percentage % |
|
1 |
Yes |
1 |
1.4% |
|
2 |
No |
69 |
98.6% |
|
3 |
Sometimes |
1 |
1.4% |
|
Total |
|
71 |
100 |
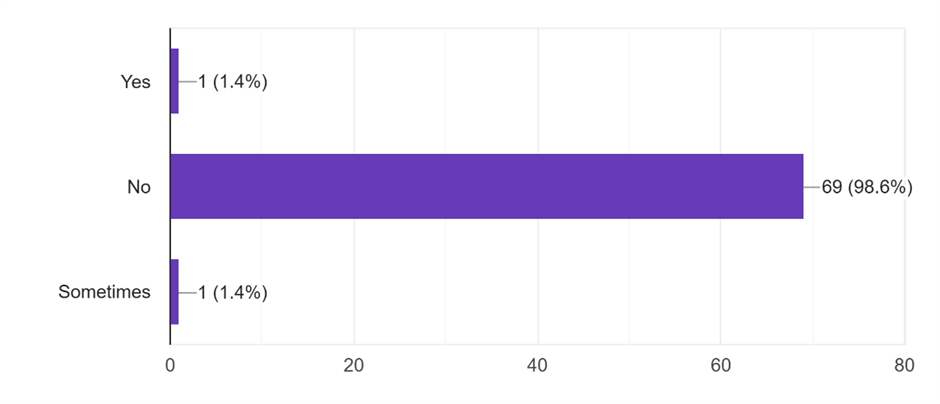
Figure 16 : Distribution of prescriptions based on alcohol
DATA ON DISTRIBUTION BASED ON STRESS FREQUENTLY
Out of 70 patients are having the alcohol were having 24 patients (34.3 %) to the yes , were having 10 patients (14.3%) to the no, and sometimes 1 patients (1.4%).
Table 11 : Stress Frequently of Patients.
|
Sr. No |
Stress Frequently |
Number Of Prescriptions |
Percentage % |
|
1 |
Yes |
24 |
34.3% |
|
2 |
No |
10 |
14.3% |
|
3 |
Sometimes |
36 |
51.4% |
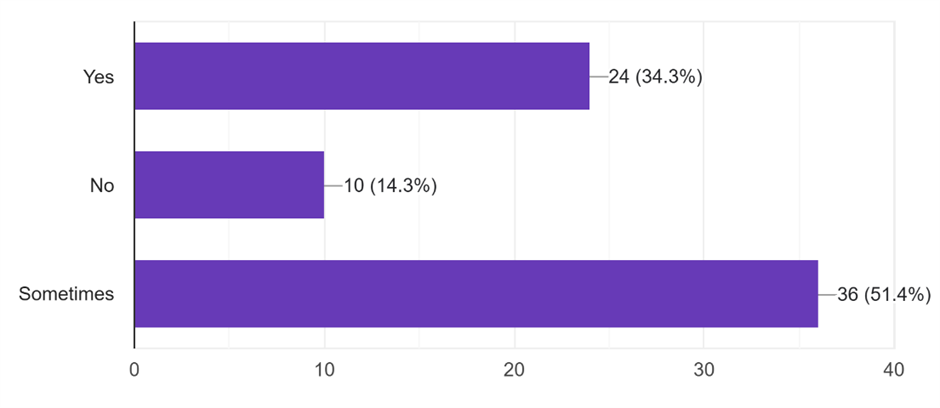
Figure 17 : Distribution of prescriptions based on stress frequently
DATA ON DISTRIBUTION BASED ON FEEL DISCOMFORT
Out of 70 patients are having the feel discomfort were having 14 patients (20%) to the yes , were having 56 patients (80%) to the no .
Table 12 : Feel Discomfort of Patients.
|
Sr. No |
Diagnosed With Gastritis |
Number of Prescriptions |
Percentage % |
|
1 |
Yes |
14 |
20% |
|
2 |
No |
56 |
80% |
|
Total |
|
72 |
100 |
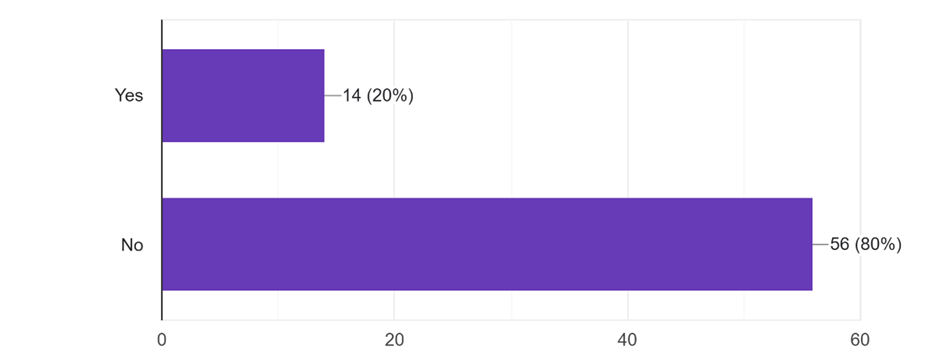
Figure 18 : Distribution of prescriptions based on feel discomfort
DATA ON DISTRIBUTION BASED ON TROUBLE SLEEPING DUE TO STOMACH DISCOMFORT
Out of 70 patients are having the feel discomfort were having 20 patients (29%) to the yes , were having 49 patients (71%) to the no .
Table 12 : Trouble Sleeping Due to Stomach Discomfort of Patients.
|
Sr. No |
Trouble Sleeping Due to Stomach Discomfort |
Number Of Prescriptions |
Percentage % |
|
1 |
Yes |
20 |
29% |
|
2 |
No |
49 |
71% |
|
Total |
|
69 |
100 |
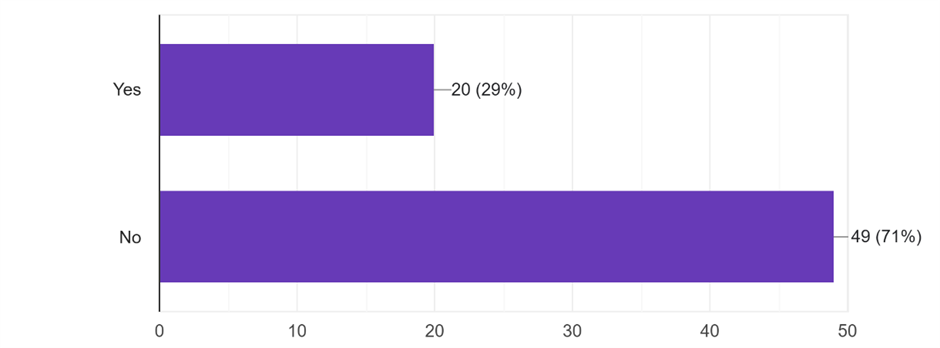
Figure 19: Distribution of prescriptions based on trouble sleeping due to stomach discomfort
DATA ON DISTRIBUTION BASED ON DIAGNOSED
Out of 70 patients are taking the diagnosed, gastritis 18 patients (25.7%), peptic ulcer 1 patients (1.4%) , stomach pain 7 patients (10%) , none 44 patients (62.9%) .
Table 13 : Diagnosed of Patients.
|
Sr. No |
Diagnosed |
Number of Prescriptions |
Percentage% |
|
1 |
Gastritis |
18 |
25.7% |
|
2 |
Peptic Ulcer |
1 |
1.4% |
|
3 |
Stomach Pain |
7 |
7% |
|
4 |
None |
44 |
62.9% |
|
Total |
|
70 |
100 |
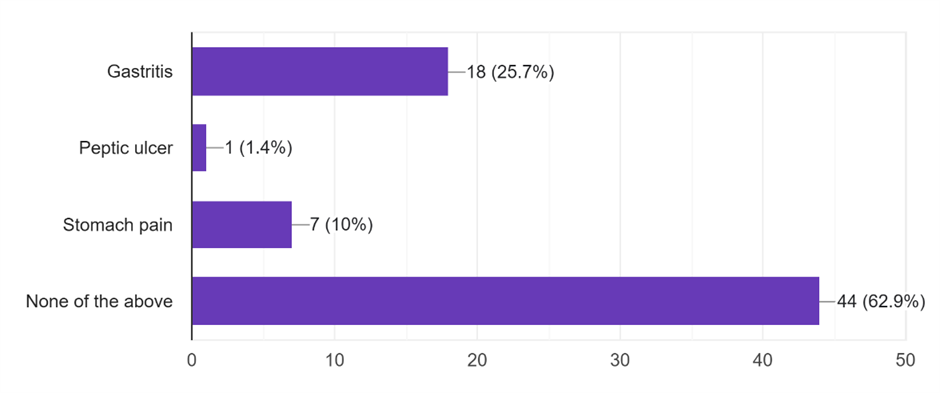
Figure 20 : Distribution of prescriptions based on diagnosed
DATA ON DISTRIBUTION BASED ON GASTRIC DISCOMFORT
Out of 70 patients are taking the gastric discomfort, ignore it 6 patients (8.6%), take medicines 13 patients (18.6%) , apply home remedies 23 patients (32.9%) , visit a doctor 16 patients (22.9%) , take a rest 26 patients (37.1%).
Table 14 : Gastric Discomfort Of Patients.
|
Sr. No |
Gastric Discomfort |
Number of Prescriptions |
Percentage % |
|
1 |
Ignore It |
6 |
8.6% |
|
2 |
Take Medicines |
13 |
18.6% |
|
3 |
Apply Home Remedies |
23 |
32.9% |
|
4 |
Visit A Doctor |
16 |
22.9% |
|
5 |
Take A Rest |
26 |
37.1% |
|
Total |
|
84 |
100 |
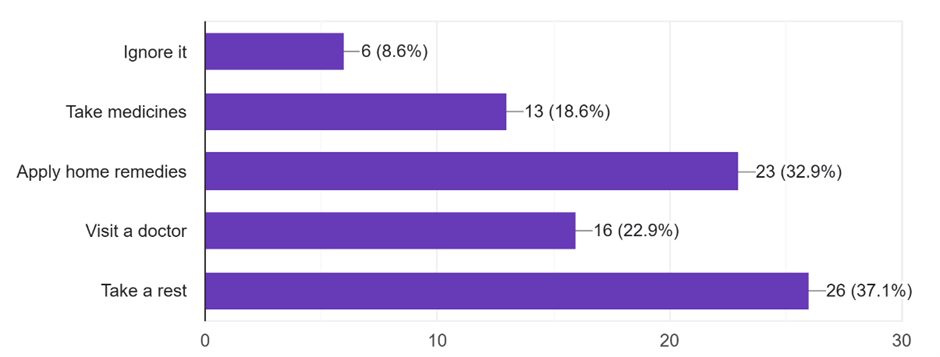
Figure 21 : Distribution of prescriptions based on gastric discomfort
DATA ON DISTRIBUTION BASED ON SELF - MEDICATED FOR STOMACH ISSUES WITHOUT CONSULTING A DOCTOR
Out of 70 patients are having the self - medicated for stomach issues without consulting a doctor were having 39 patients (55.7%) to the yes , were having 31 patients (44.3%) to the no .
Table 12 : Self - Medicated For Stomach Issues Without Consulting A Doctor Of Patients.
|
Sr. No |
Self-Medicated for Stomach Issues Without Consulting A Doctor |
Number of Prescriptions |
Percentage % |
|
1 |
Yes |
39 |
55.7% |
|
2 |
No |
31 |
44.3% |
|
Total |
|
70 |
100 |
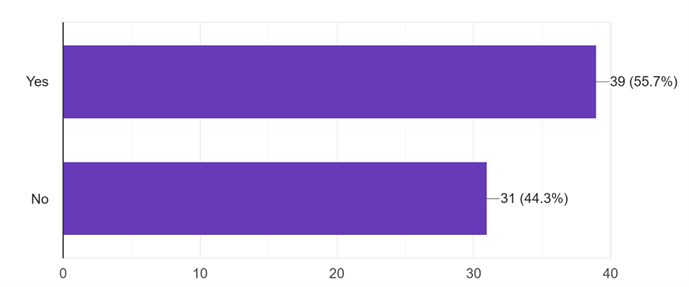
Figure 22 : Distribution of prescriptions based on self - medicated for stomach issues wthout consulting a doctor of patients
SUMMARY:
If the cause of gastritis is not known or the symptoms are severe and do not subside in a few days, one should consult the doctor to help make a diagnosis. Identifying the underlying cause is the key to treating and managing gastritis. Early and effective treatment with medications, simple lifestyle and dietary changes help prevent the complications of gastritis. Long-term lifestyle modifications are crucial in preventing gastritis episodes in the future. It may not be possible to prevent all infections that cause gastritis. However, by maintaining good personal and food hygiene, one can decrease the risk of developing gastritis from infectious agents. Emphysematous Gastritis requires a multidisciplinary approach for optimal outcomes. CT imaging remains pivotal for diagnosis, and management should be individualized based on disease severity and patient factors. While mortality remains significant, early recognition and advancements in medical care have improved survival in many cases. Gastritis research articles commonly conclude that gastritis, an inflammation of the stomach lining, is a widespread condition with diverse causes and potential complications like ulcers or even gastric cancer. Risk factors include H. pylori infection, lifestyle choices such as smoking and alcohol consumption, and the use of certain medications. While acute gastritis can be short-lived, chronic gastritis can persist and requires proper management to prevent severe outcomes.
1. Total distribution of patient with respect to the gender shows that, out of 70 patients ,57 patients (81.4) were female and male 13 patients (17.1) were resulted with ischemic stroke.
2. Total distribution of patient with respect to the age group majority of the patients were found to be between the age group of 18 year (4.3%), followed by >19 year (18.6%), and this age group >20 (38.6%), many of years are having (27%) 21-36 years.
3. These symptoms are associated with the gastritis were out of 70 patients, loss of appetite are having 18 patients (29%), burning sensation are 32 (51.6%), vomiting are 15 patients (24.5%), heartburn are having 12 patients (19.4%), bloating are having 5 patients (8.1%), acid reflux are having 4 patients (6.5%).
4. Out of 70 patients are having the spicy food the rarely 25 patients (35.7%), sometimes 40 patients (57.1%), frequently 7 patients (10%)
5. Out of 70 patients are having the skip meals were having 34 patients (48.6%) to the yes , were having 37 patients (52.9%) to the no.
6. Out of 70 patients are having the drink coffee or tea, none of the 43 patients (61.5%), 1-2 are having 27 patients (38.6%), were 3 or more are having 2 patients (2.9%).
7. Out of 70 patients are having the carbonated drinks were having 32 patients (45.7%) to the no, were having 38 patients (54.3%) to the yes .
8. Out of 70 patients are having the diagnosed with gastritis were having 19 patients (27.1%) to the yes, were having 53 patients (75.7%) to the no.
9. Out of 70 patients are taking the regularly drug, pain killer (NSAIDS like ibuprofen, aspirin) 6 patients (8.6%), steroids 0 patients (0%), antacids 5 (7.1%), none 59 patients (84.3%).
10. Out of 70 patients are having the smoke were having 0 patients (0 %) to the yes, were having 69 patients (98.6%) to the no, and sometimes 1 patient (1.4%).
11. Out of 70 patients the alcohol was having 1 patient (1.4 %) to the yes , were having 69 patients (98.6%) to the no, and sometimes 1 patient (1.4%).
12. Out of 70 patients the alcohol was having 24 patients (34.3 %) to the yes , were having 10 patients (14.3%) to the no, and sometimes 1 patient (1.4%).
13. Out of 70 patients are having the feel discomfort were having 14 patients (20%) to the yes, were having 56 patients (80%) to the no.
14. Out of 70 patients are having the feel discomfort were having 20 patients (29%) to the yes, were having 49 patients (71%) to the no.
15. Out of 70 patients are taking the diagnosed, gastritis 18 patients (25.7%), peptic ulcer 1 patients (1.4%), stomach pain 7 patients (10%), none 44 patients (62.9%).
16. Out of 70 patients are taking the gastric discomfort, ignore it 6 patients (8.6%), take medicines 13 patients (18.6%), apply home remedies 23 patients (32.9%), visit a doctor 16 patients (22.9%), take a rest 26 patients (37.1%).
17. Out of 70 patients are having the self – medicated for stomach issues without consulting a doctor were having 39 patients (55.7%) to the yes, were having 31 patients (44.3%) to the no
REFERENCES


Dr. N. Muthu Rani, B. Bhuvaneswari, G. Lokeswari, Amit, Golu, A Prospective Study on Triggering Factors of Gastritis and Its Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 3130-3151. https://doi.org/10.5281/zenodo.18390348
 10.5281/zenodo.18390348
10.5281/zenodo.18390348