Department of Pharmaceutical Chemistry, Quality Assurance and Pharmacology of Agnihotri Institute of Pharmacy, Agnihotri College of Pharmacy and Wardha Gurunanak College of Pharmacy, Nagpur.
Rheumatoid arthritis (RA) is a condition characterized by an autoimmune response. This disorder primarily affects multiple joints in the body and has a global impact, affecting numerous individuals worldwide. RA is a progressive, chronic illness that manifests in various stages. As the disease advances, joint deterioration worsens, ultimately leading to the loss of joint function. Additionally, RA can also impact other organs within the body. The development of RA is influenced by several factors, including environmental elements, age, weight, genetics, and lifestyle choices. Etiological factors such as autoantibodies, inflammatory mediators, and genes contribute to the onset of RA. Symptoms of this disease encompass swelling, pain, decreased appetite, joint inflammation, fatigue, and pericarditis. The primary objective of RA treatment is to alleviate pain and inflammation while preventing joint dysfunction and deformity. To achieve this, a variety of medications are utilized, including non-steroidal anti-inflammatory drugs, steroids, and disease-modifying anti-rheumatic drugs. However, the use of synthetic drugs is associated with potentially life-threatening side effects. Consequently, individuals seek alternative medicines for RA treatment. The focus of this study is to emphasize the utilization of herbal medicines for the benefit of RA patients. Herbal medicines and isolated phytoconstituents derived from herbal and synthetic drugs offer advantages such as affordability, accessibility, high patient acceptance, and minimal side effects. These medications also enhance the patient's overall condition and reduce stress. Numerous researchers have demonstrated the efficacy of herbal drugs and phytoconstituents in treating RA patients. Therefore, this study aims to raise awareness regarding the importance of increasing the utilization of herbal drugs for RA treatment.
Rheumatoid arthritis (RA) is a systemic autoimmune condition characterized by inflammation in the joints and other areas of the body. It is a chronic inflammatory disorder that is often caused by a combination of genetic and environmental factors, such as smoking. The condition primarily affects the synovial joints, starting in the smaller peripheral joints and progressing to the larger joints if left untreated. [1] Over time, the inflammation in the joints leads to the destruction of cartilage and bone erosion. RA can be classified as early RA if the symptoms have been present for less than six months, and established RA if the symptoms have been present for more than six months. If left untreated, RA can lead to increased morbidity and mortality. [2] [3] [4] Diagnosing rheumatoid arthritis in the early stages can be challenging as there is no definitive laboratory test for the condition. A comprehensive clinical approach is necessary to make an accurate diagnosis and prevent further joint damage. The treatment of RA involves a combination of medication and non-pharmacological therapies. Early treatment with disease-modifying anti-rheumatic drugs is considered the standard of care. However, despite treatment, many patients still experience disability and significant morbidity over time. [5] Therefore, a comprehensive approach that includes both medication and non-medication interventions, such as physical therapy, counseling, and patient education, is necessary to improve clinical outcomes. [4]

Fig No.1 Rheumatoid Arthritis
Pathophysiology
The pathophysiology of OA and RA is distinct although the primary manifestations of both involve the joints. OA is characterized by progressive cartilage loss. Increased thickness of the subchondral plate, osteophytes and subchondral bone cysts are the characteristic features. Vascular invasion and further calcification of nearby articular cartilage may occur as the disease progresses, leading to decreased thickness of articular cartilage. Bone remodeling and enhanced cartilage deterioration takes place over time. The inflammation is generally milder in severity than that observed in rheumatoid arthritis and typically involves the periarticular tissues. Rheumatoid arthritis is a chronic, autoimmune syndrome. Autoimmune inflammation is a result of a response to self-antigens. Thus, a dysregulated immune system results in autoimmune diseases. Synovial inflammation leading to cartilage and bone damage is characteristic of the disease. Persistent inflammation leads to progressive destruction of articular and periarticular structures which in turn, lead to deformity. Morning stiffness is a common problem for patients with rheumatoid arthritis. Characteristic features of RA pathophysiology are increased angiogenesis, cellular hyperplasia, influx of inflammatory cells, changes in the expression of cell surface adhesion molecules and presence of many cytokines. Tumor necrosis factor (TNF) and interleukin-1 are in abundance in the joints. They are the stimulators of proliferation, metalloproteinase expression, adhesion molecule expression, and further secretion of other cytokines. CD4 T cells, mononuclear phagocytes, fibroblasts, osteoclasts, and neutrophils play major role in pathophysiology of rheumatoid arthritis. Presence of anti-cyclic citrullinated protein antibody (ACPA) and rheumatoid factor (RF) is highly specific for RA [2].
Features of Rheumatoid Arthritis
Causes

Figure No: 2. show comparison of normal joint and joint affected by rheumatoid arthritis.
Symptoms
Diagnosis

Figure No: 3. show comparison of normal joint and joint affected by rheumatoid arthritis
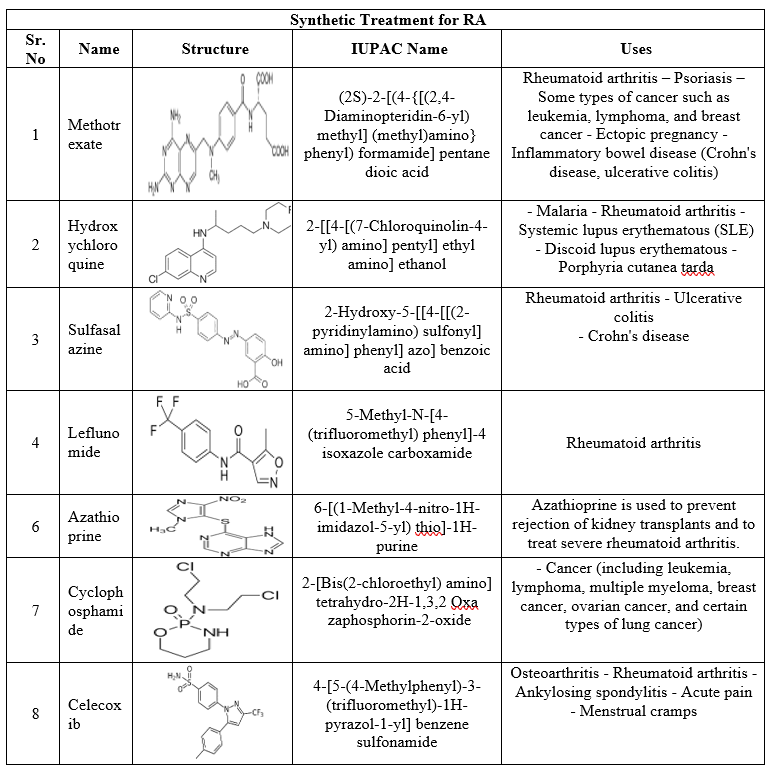
Table No.1: - Herbal Treatment for RA

Table No.2: Synthetic Treatment for RA
Home Remedies for Arthritis
Exercise Regularly: Gentle exercise can help to strengthen muscles around joints and also helps to fight fatigue.
Relax: Techniques such as hypnosis, guided imagery, deep breathing and muscle relaxation can be done to control.
Yoga: Yoga can help to improve strength and flexibility. The exercises should be performed with caution by people with rheumatoid arthritis who have spinal problems [6].
Surgery and other Treatments
In some cases, surgery may be done if other treatments have not worked. This may include:
CONCLUSION
The review article was reported and compared both type of herbal and synthetic drugs. The potential herbal drug was found to be effective as that of synthetic and thus proves more potency of herbs in the treatment of rheumatoid arthritis disorders. Given the fact that the pathophysiology of RA is still clear, the development of a curative compounds is markedly limited. This limitation is even more compounded by the unavailability of appropriately validated animal models are important in the efficient and rational development of other treated compounds for RA.
REFERENCE

Abhijit Daf*, Roshankumar Satsure, Dr. Archana Mungale, Akash Kapse, A Review on: Synthetic and Herbal Approaches for the Treatment of Rheumatoid Arthritis an Autoimmune Disorder, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 7, 1197-1203. https://doi.org/10.5281/zenodo.12750540
 10.5281/zenodo.12750540
10.5281/zenodo.12750540
