Department of Pharmacy Practice, Vignan Pharmacy College, Vadlamudi, Guntur 522213
The integration of artificial intelligence (AI) into neuro-oncology has transformed the methods used for diagnosing, predicting outcomes, and treating brain tumors. This review explores both current and emerging AI-based techniques in the neuro-oncology field, with a focus on imaging, clinical decision-making, and personalized therapies. Advanced machine learning (ML) and deep learning (DL) algorithms are enhancing the interpretation of neuroimaging by enabling precise tumor segmentation, classification, and progression monitoring. Radiomics and radio genomics further link imaging characteristics with molecular profiles, offering noninvasive diagnostic and prognostic insights. In terms of treatment planning, AI supports surgical navigation, optimizes radiation therapy, and aids in the discovery of targeted drugs. Additionally, predictive models help forecast outcomes and adaptively adjust therapies. Despite these promising developments, challenges such as data standardization, model generalizability, and ethical concerns remain. Continued interdisciplinary collaboration is essential to fully leverage AI's potential in delivering more precise, efficient, and personalized care in neuro-oncology.
The National Cancer Institute reports that brain and nervous system cancers resulted in 18,330 fatalities, alongside an estimated 24,820 new diagnosis. This cancer type occurs marginally more often in men than in women and is also more frequently seen in those with specific genetic syndromes. In 2025, it was the ninth leading cause of cancer-related deaths in the United States (1). Central nervous system tumors, which come under the neuro-oncology department, are the leading cause of mortality in most of the populations; mostly diffuse gliomas, like meningiomas, represent the most common intracranial tumors. Currently, there is no established standard of care for the treatment of refractory meningiomas (2)(3). In the field of neuro-oncology, various diagnostic and treatment parameters are included. Contrast-enhanced MRI is recognized as the gold standard imaging modality, which plays a crucial role in guiding surgical and radiotherapy treatments, as well as in monitoring therapeutic response and disease progression. Additionally, several novel systemic therapy options, including targeted therapy and immuno-oncology approaches, are emerging. Neuro-oncology faces significant challenges beyond differential diagnosis, particularly in optimizing the care of patients with primary brain tumors. (4,5). Artificial Intelligence (AI) is transforming neuro-oncology in innovative ways. Advanced AI technologies such as machine learning (ML), deep learning (DL), and natural language processing (NLP) are increasingly being used in both clinical and research contexts. These articles highlight various AI algorithms used in diagnosis, prognostication, and treatment planning. Examples of AI applications in brain tumor detection demonstrate how these techniques improve diagnostic accuracy, efficiency, and prognosis assessment, as well as support the development of individualized treatment regimens. AI enables more precise tumor characterization, risk stratification, and therapeutic decision-making, ultimately leading to better patient outcomes in neuro-oncology. (6,7). The significance of various diagnostic and treatment parameters employed by algorithms to enhance patient quality of life (see fig. 1) was included in this article. Role of AI in neurosurgical oncology.
Artificial intelligence (AI) models have demonstrated the capability to predict patient survival by analyzing early indicators of tumor recurrence through the integration of imaging modalities and clinical data. This predictive capacity facilitates the identification of patients suitable for specific clinical trials, aligning treatment strategies with individual tumor profiles. However, the accuracy and reliability of these AI-driven predictions are contingent upon access to large, diverse, and high-quality datasets.
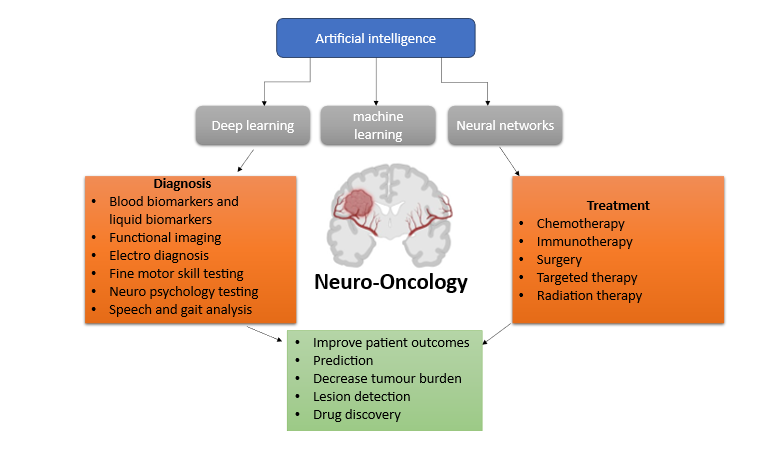
Fig. 1: The diagnosis and treatment approaches have been significantly enhanced by the integration of artificial intelligence (AI), leading to improved patient outcomes and quality of life.
TABLE 1: AI MODELS USED IN CLASSIFICATION OF BRAIN TUMORS
|
SR. NO |
TYPE OF BRAIN TUMOURS |
ML AND DL ALGORITHMS |
|
1. |
meningioma |
Optimized ANN; Logistic regression (LR); SVM; CNN |
|
2. |
Astrocytoma |
Learning Vector Quantization (LVQ); Naive Bayes; SVM |
|
3. |
Brain stem gliomas |
ML; DL; k-means clustering for segmentation; SVM |
|
4. |
Ependymomas |
Radiomics; CNN; ML; RF; ANN (artificial neural network); Tree bagger (TB); Gradient boosting (GB) |
|
5. |
Oligodendrogliomas |
T2WI-only network (MGMT-net); 3D U-Net architecture; CNN; Random survival forest (RSF); SVM; Network-based statistics (NBS) |
|
6. |
Optic pathway gliomas |
DL; U-Net+ResNet architecture |
|
7. |
oligo-astrocytomas |
CNN (conventional neural network); DL (deep learning) |
|
8. |
Primitive neuroectodermal |
2-phase deep learning algorithm; LR; RF; Decision tree |
|
9. |
Pituitary tumours |
CRNN (DenseNet+ResNet); Support vector machine; Deep neural network (DNN); Naive Bayes; LR; RF; XGboost |
|
10. |
Pineoblastoma |
radiomics; Gaussian Naïve Bayes; Support Vector Machine Classifier (SVC); Multilayer Perceptron (MLP); CatBoost |
|
11. |
Choroid plexus |
DL; ChP architecture |
|
12. |
Medulloblastoma |
CNN; Topographic independent component analysis (TICA); SVM |
This table presents the various types of brain tumors alongside the artificial intelligence algorithms employed for their detection, which are crucial for diagnosis, treatment planning, and surgical predictions. The algorithms include SVM (Support Vector Machine), DL (Deep Learning), CNN (Convolutional Neural Network), ANN (Artificial Neural Network), LR (Logistic Regression), LVQ (Learning Vector Quantization), ML (Machine Learning), RSF (Random Survival Forest), RF (Random Forest), TB (Tree Bagger), GB (Gradient Boosting), NBS (Network-Based Statistics), and TICA (Topographic Independent Component Analysis).
2. AI IN EARLY DIAGNOSTICS AND PROGNOSTICATION
Artificial intelligence has significantly enhanced neuroimaging techniques, including MRI, PET, and CT scans, facilitating the precise identification of Alzheimer's disease biomarkers. Machine learning models analyze these images to discern patterns indicative of early cognitive decline. Additionally, AI algorithms are employed to identify genetic and proteomic biomarkers, thereby supporting early intervention (8). Khalifa and Albadawy investigated AI's role in advancing clinical prediction. Through an examination of 74 experimental studies, they determined that AI is capable of recognizing subtle and complex patterns in X-rays, MRIs, and CT scans that may elude human observers. This capability is particularly crucial for the early detection of diseases such as cancer, where timely intervention can substantially improve prognosis. (9)
Conversely, a delayed diagnosis often results in the disease advancing to more severe stages, necessitating more aggressive treatment strategies and leading to a poorer prognosis. Artificial intelligence methodologies, including fuzzy logic, artificial neural networks (ANNs), recurrent neural networks (RNNs), and logistic regression (LR), have been successfully utilized to identify complex health conditions with high precision. Convolutional neural networks (CNNs) have become the benchmark for image-based diagnostics, such as tumor detection in radiological scans. Similarly, ensemble methods like random forest and gradient boosting enhance diagnostic accuracy by integrating data from multiple sources, thereby addressing the limitations of individual models. (10,11)
TABLE 2: AI IN DRUG DISCOVERY & PRECISION NEURO-ONCOLOGY: TARGETED THERAPY AND DRUG DEVELOPMENT
|
Domain |
Specific area |
AI applications |
AI methods/ tools |
Impact in neuro-oncology |
|
Target identification |
Identifying oncogenic drivers |
AI examines datasets from genomics, transcriptomics, and proteomics to identify new therapeutic targets that are specific to brain tumors such as glioblastoma and astrocytoma. |
DeepMind AlphaFold, IBM Watson for Genomics |
improves specificity of treatment targets |
|
Pathway mapping |
Understanding tumor signaling |
ML maps out dysregulated pathways (e.g., PI3K/AKT, EGFR, IDH1/2) driving tumor progression and resistance. |
Ingenuity Pathway Analysis + ML models |
Identifies critical nodes for multi-target therapy strategies |
|
Biomarker discovery |
Patient stratification |
AI identifies molecular signatures that predict response or resistance to therapies through integration of omics and clinical outcome data. |
Deep Genomics, Tempus, Guardant Health |
Facilitates personalized therapy; enhances clinical trial design |
|
Molecular design |
De novo drug development |
Generative AI develops new molecules that are tailored for effective brain penetration and demonstrate minimal toxicity. The models consider factors such as blood-brain barrier permeability and central nervous system selectivity. |
Insilico Medicine |
Produces brain-targeted drugs tailored to unique tumor genetics |
|
Radiogenomics |
Imaging-genomics correlation |
AI links MRI/CT phenotypes with genomic alterations, aiding in non-invasive diagnosis and therapy prediction. |
Radio genomic ML platforms, Deep Radiology |
Enables real-time, non-invasive tumor profiling |
|
Clinical trial design |
Adaptive trial modeling |
Predictive AI forecasts which patients will benefit most from therapies and optimizes trial arms, endpoints, and cohort selection. |
Unlearn.AI, IBM Clinical Development |
Improves trial efficiency and reduces drop-out rate |
|
Treatment personalization |
Dynamic therapy adjustment |
AI utilizes longitudinal data, including imaging, genomics, and symptoms, to adjust treatment plans over time. Reinforcement learning customizes both the dosage and selection of drugs. |
BioXcel Therapeutics, Tempus One |
Maximizes efficacy while minimizing side effects in high-risk brain tumor patients |
|
Toxicity prediction |
Neurotoxicity screening |
AI evaluates potential neurotoxicity, encompassing effects on the blood-brain barrier, mitochondrial stress, and adverse reactions specific to the CNS. |
DeepTox, Tox21, AIDD (AI-Driven Drug Safety) |
Helps eliminate toxic compounds early; ensures safer CNS drugs |
|
Multi-omics integration |
Holistic patient modeling |
Utilizes AI to integrate genomics, epigenomics, transcriptomics, metabolomics, and imaging data, creating detailed tumor profiles. |
Multi-omics fusion via AutoML, data lakes + ML |
Creates a detailed biological map of each tumor for hyper-targeted treatment |
|
Precision immunotherapy |
Tumor microenvironment analysis |
Ai models predict immune cell infiltration, t-cell recognition, and checkpoint expression from rna-seq and histology data. |
Immuai, pathai, neoantigen ml models |
Supports development of personalized cancer vaccines and car-t cell therapies |
In neuro-oncology, artificial intelligence is significantly advancing precision treatment and medication development. It aids in the development of brain-specific medications, the discovery of new targets, and an understanding of tumor behavior.AI also enhances therapy response prediction and patient selection. A summary of AI uses in targeted therapy and brain tumor medication development may be found in table -2.
2.1 Early Tumor Detection:
These abnormal cells grow and divide in the tissue in which they originated, resulting in a mass of cells called a tumor. Early tumor detection is recognized as a key priority by the World Health Organization (WHO) and the International Alliance for Cancer Early Detection (ACED). In the analysis of unstructured clinical data, a frequently employed technique in both oncology and broader medical fields is natural language processing (NLP).
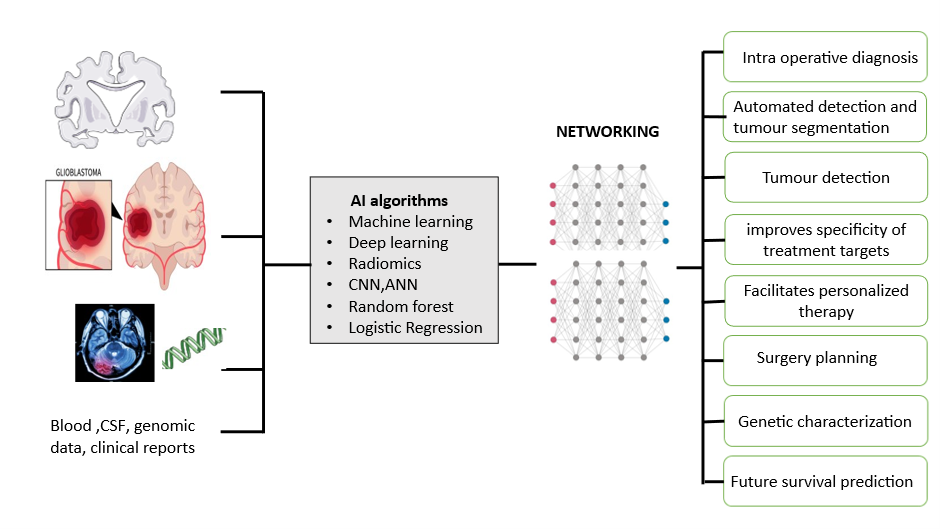
Fig. 1: Various applications of machine learning
2.2.1 AI algorithms in meningioma
Prognostication and surgical planning for WHO grade I versus grade II meningioma necessitate careful consideration. The authors employed conventional statistical models alongside a range of machine learning algorithms to predict atypical meningioma based on radiologist-interpreted preoperative MRI findings (12). Laukamp et al. utilized a multiparametric deep-learning model (DLM) on routine MRI data, which included images from 249 glioma cases, to achieve accurate automated detection and segmentation of meningioma tissue. This approach may enhance and facilitate therapy planning and monitoring of this prevalent tumor entity (13).
Machine learning (ML) has demonstrated significant promise in the quantitative and qualitative characterization of both normal and pathological structures. ML techniques are now widely recognized and employed in addressing brain-related conditions such as Alzheimer’s disease, dementia, schizophrenia, multiple sclerosis, cancer, and various infectious and degenerative diseases (14). Chen et al. utilized texture analysis-based ML algorithms, including linear discriminant analysis (LDA) and support vector machine (SVM), to develop a non-invasive imaging biomarker for the accurate classification of meningiomas. The LDA-based models exhibited superior diagnostic performance compared to the SVM-based models in classification tasks (15). The study aimed to evaluate the efficacy of preoperative multiparametric magnetic resonance imaging (mpMRI)-based clinical-radiomic analysis combined with ML algorithms in predicting the expression of the Ki-67 proliferative index and p53 tumor suppressor protein in patients with meningioma. The area under the curve (AUC) and accuracy for high Ki-67 expression were 0.820 and 0.867 in the internal test and 0.666 and 0.773 in the external test, respectively. For p53 positivity, the AUC and accuracy were 0.858 and 0.857 in the internal test and 0.684 and 0.718 in the external test, respectively, providing a novel non-invasive strategy for assessing cell proliferation (16). Azam et al. (2025) conducted a study aimed at enhancing the histopathological diagnosis of meningioma and solitary fibrous tumors (SFTs) using a Vision Transformer (ViT)-based neural network model. The ViT architecture, known for its robust performance across various image classification tasks, was employed in a weakly supervised framework to analyze whole slide images (WSIs). These WSIs were stored in the SVS format and processed into three hierarchical resolution levels—Level 0, Level 1, and Level 2—corresponding to different magnification scales in a pyramid structure.
To assess the model’s robustness and generalizability, two validation strategies were implemented: a conventional train-test split and a 4-fold cross-validation (CV). The results indicated variation in diagnostic performance across the different pyramid levels. In the train-test setup, Level 0 yielded the highest accuracy (90.64%), accompanied by excellent sensitivity (93.97%) and solid specificity (86.74%). Level 1 followed closely with an accuracy of 89.26%, showing a slightly better balance in sensitivity (86.01%) and specificity (93.07%). Conversely, Level 2 demonstrated a marked decline in performance, particularly in sensitivity (42.36%) and overall accuracy (68.74%), although it maintained high specificity (99.70%).
Notably, a composite approach integrating predictions from all three levels improved the overall model performance, achieving an accuracy of 92.27% and specificity of 97.55%, with balanced sensitivity and specificity metrics.
In the 4-fold cross-validation analysis, Level 0 maintained stable results with 89.20% accuracy, 88.76% sensitivity, and 89.70% specificity. Level 1 slightly outperformed Level 0, reaching 89.67% accuracy, along with balanced sensitivity (89.73%) and specificity (89.61%). While Level 2 still underperformed in terms of accuracy (85.35%), it showed improved sensitivity (92.82%) and favorable ROC and F1-score metrics. The integrated multi-resolution strategy again proved superior, boosting accuracy to 94.68%, sensitivity to 96.05%, and the F1-score to 95.07%.
These findings emphasize the diagnostic advantage of combining multiple resolution levels in a transformer-based model, offering enhanced accuracy and reliability in differentiating between meningioma and SFT on histopathology.
According to the 2016 World Health Organization (WHO) Classification of Tumors of the Central Nervous System, astrocytoma is categorized into low-grade astrocytoma (LGA, WHO II) and anaplastic astrocytoma. Astrocytoma is among the most prevalent intracranial tumors. A study involving 175 patients was conducted to evaluate the diagnostic capability of radiomics-based machine learning in distinguishing atypical low-grade astrocytoma (LGA) from anaplastic astrocytoma (AA). The study employed AI algorithms, including Linear Discriminant Analysis (LDA), Support Vector Machine (SVM), and Random Forest (RF), to identify the sensitivity, specificity, accuracy, and areas under the receiver operating characteristic curve (AUC) for each model. The results were promising, indicating the potential of these methods in reliably differentiating atypical LGA from AA (17). The study also aimed to identify key trends among various supervised machine learning algorithms, their performance, and their application in disease risk prediction, thereby assisting researchers in selecting appropriate algorithms for their studies. The findings revealed that the Support Vector Machine (SVM) algorithm was most frequently applied (in 29 studies), followed by the Naïve Bayes algorithm (in 23 studies). However, the Random Forest (RF) algorithm demonstrated superior accuracy, achieving the highest accuracy in 9 out of 17 studies where it was applied, equating to 53%. This was followed by SVM, which achieved the highest accuracy in 41% of the studies considered (18). In the current study, the potential use of serum miRNAs as biomarkers for diagnosis and prognosis was investigated in a cohort of 73 Chinese astrocytoma patients. The biomarker, composed of 9 miRNAs, exhibited high sensitivity, specificity, and accuracy in diagnosis and prognosis, indicating the potential of serum miRNAs as novel diagnostic and prognostic biomarkers for human astrocytoma (19). Recently, IDH1 and IDH2 mutations have been identified as early mutations in diffuse astrocytic tumors, and determining the IDH status through immunohistochemistry or sequencing has become standard in diagnosing these tumors. The IDH status was also confirmed by performing 450k/EPIC analysis, receiving the readout of "methylation group astrocytoma IDH mutant" via a recently developed classifier tool, which predicts IDH-mutant astrocytoma with high specificity and sensitivity (20). The study correlated aberrant gene expression in pediatric PA with CNAs or gene promoter hypermethylation to identify and characterize cellular pathways involved in tumor development and growth, using methylation-specific PCR (MSP) and bisulfite sequencing to investigate alternative mechanisms of transcriptional silencing in PA. These genes have previously been reported as methylated in astrocytoma or other tumors, identifying two key signaling pathways (PI3K and MAPK) that contribute to tumor development. Large regions of chromosome alterations were not identified in PA, although 97 individual BAC clones and a small region on chromosome 7 were lost and/or gained (21).
The World Health Organization has recently emphasized the integration of genetic information in the study of gliomas. Brain CT scans are crucial for detecting and diagnosing various neurological conditions, including tumors, strokes, and traumatic brain injuries. Several feature extraction methods, such as Local Binary Patterns (LBP), Local Directional Patterns (LDP), Discrete Wavelet Transform (DWT), Hough Transform, Discrete Fourier Transform (DFT), and Binary Wavelet Transform (BWT), have been employed to systematically extract key features. Numerous machine learning algorithms, including CatBoost, Random Forest, SVM, Decision Tree, and XGBoost, have been applied to evaluate the model's effectiveness in image classification. The results indicated that CatBoost achieved the highest accuracy at 96.91%, followed by KNN with 93.82%, XGBoost with 93.44%, and Random Forest with 92.28%, while Naïve Bayes underperformed with an accuracy of 72.59%. These methods provide more interpretable and clinically useful tools for healthcare professionals (22,23). In this study, a convolutional neural network was trained to classify isocitrate dehydrogenase 1 (IDH1) mutation status, 1p/19q codeletion, and O6-methylguanine-DNA methyltransferase (MGMT) promoter methylation status to independently predict underlying molecular genetic mutation status in gliomas with high accuracy and to identify the most predictive imaging features for each mutation. The classification achieved high accuracy: IDH1 mutation status at 94%, 1p/19q codeletion at 92%, and MGMT promoter methylation status at 83%. Each genetic category was associated with distinctive imaging features, such as tumor margin definition, T1 and FLAIR suppression, extent of edema, extent of necrosis, and textural features (24). Blanc-Durand et al. demonstrated that amino-acid positron emission tomography (PET) is increasingly utilized in the diagnostic workup of patients with gliomas, including differential diagnosis, evaluation of tumor extension, treatment planning, and follow-up. They demonstrated the feasibility of an automated 18F-fluoro-ethyl-tyrosine (18F-FET) PET lesion detection and segmentation using a full 3D U-Net Convolutional Neural Network (CNN), proposing the first full 3D automated procedure for segmentation of 18F-FET PET brain images of patients with different gliomas using a U-Net CNN architecture (25). The current study leverages advanced image analysis and machine learning algorithms to identify complex and reproducible imaging patterns predictive of overall survival and molecular subtype in glioblastoma (GB).
3. AI IN TREATMENT PLANNING:
TABLE 3: TARGETED THERAPIES IN NEURO-ONCOLOGY
|
Drug name |
Molecular target(s) |
Tumor type(s) |
Mechanism of action |
Clinical status |
|
Bevacizumab |
VEGF-A |
Glioblastoma (GBM) |
Anti-angiogenic; inhibits blood vessel formation |
FDA-approved for recurrent GBM |
|
Osimertinib |
EGFR (T790M, exon 19 deletions) |
EGFR-mutant gliomas |
EGFR tyrosine kinase inhibitor (TKI) |
Off-label use, under investigation |
|
Dabrafenib + trametinib |
BRAF V600E + MEK1/2 |
BRAF-mutant gliomas (LGG, GBM) |
BRAF + MEK inhibition |
Approved for BRAF V600E+ tumors (incl. LGG) |
|
Larotrectinib |
NTRK gene fusions |
High- and low-grade gliomas with NTRK fusions |
TRK inhibitor |
FDA-approved for NTRK fusion-positive tumors |
|
Entrectinib |
NTRK, ROS1, ALK |
Gliomas with relevant fusions |
Multi-kinase TRK/ ALK/ROS1 inhibitor |
FDA-approved for NTRK fusions |
|
Abemaciclib |
CDK4/6 |
Recurrent glioblastoma |
Cell cycle inhibitor |
Clinical trials ongoing |
|
Selinexor |
XPO1 nuclear export protein |
Recurrent high-grade gliomas |
Inhibits nuclear export of tumor suppressor proteins |
Investigational (Phase II/III) |
|
Marizomib |
Proteasome |
Glioblastoma |
Irreversible proteasome inhibition; crosses BBB |
Phase I/II trials |
|
Eflornithine (dfmo) |
Ornithine decarboxylase (ODC1) |
Diffuse intrinsic pontine glioma (DIPG) |
Inhibits polyamine synthesis |
Investigational |
|
Vorinostat |
HDAC (Histone deacetylases) |
Pediatric brain tumors, gliomas |
Epigenetic modulation, reactivates silenced genes |
Clinical trials |
The capacity of tailored therapy to influence particular genetic and molecular changes present in brain tumors has drawn interest in neuro-oncology in recent years. These treatments aim to stop the growth of tumors by targeting important proteins, gene mutations, or signaling pathways that contribute to the development of cancer. A number of targeted medications are now being investigated or utilized in clinical settings to treat brain tumors, including gliomas. In neuro-oncology, the main targeted therapies, their molecular targets, tumor types, mechanisms of action, and clinical status are summarized in Table 3.
3.1 personalized treatment protocols
3.1.1. Molecular and Genetic Profiling in Gliomas
Understanding the molecular and genetic details of gliomas is crucial for personalized treatment in brain cancer care. This helps doctors diagnose more accurately, predict disease progression, and select the best treatments. Key biomarkers include IDH mutations, 1p/19q co-deletion, MGMT promoter methylation, and EGFR amplification. These markers help classify gliomas and predict treatment response. IDH Mutations Changes in the IDH1 and IDH2 genes are common in lower-grade gliomas and secondary glioblastomas. Tumors with these mutations usually grow slower, and patients often live longer than those with normal IDH genes. These tumors produce a chemical called D-2-hydroxyglutarate, which affects cancer development but also offers new treatment options. Studies show that patients with IDH mutations respond better to treatments like radiation and chemotherapy, especially with drugs like temozolomide(26)1p/19q Co-deletion When both the short arm of chromosome 1 (1p) and the long arm of chromosome 19 (19q) are missing in tumor cells, it is called a 1p/19q co-deletion. This is a key feature of oligodendrogliomas. Patients with this marker respond well to combined radiation and chemotherapy and often live longer. If a tumor has both IDH mutations and this co-deletion, it provides doctors with better information about the tumor type and likely outcomes.(27) EGFR Amplification In glioblastoma multiforme (GBM), having too many copies of the EGFR gene is common. This makes the tumor grow and spread more aggressively and is linked to a worse outlook for the patient. EGFR is important in how these tumors behave and are categorized. Because of its significance, scientists are studying EGFR as a potential target for new cancer treatments.(28)
3.1.2. Advanced Neuroimaging Integration in Personalized Glioma Treatment Planning
New imaging techniques have greatly improved how doctors plan personalized treatment for people with gliomas. Tools like MRI, fMRI, DTI, and PET scans give detailed information about the tumor—such as its size, location, and how it affects important areas of the brain. Using these methods together helps doctors carefully plan surgery and radiotherapy based on each patient’s unique condition.
Magnetic Resonance Imaging (MRI)
MRI is the most commonly used imaging method in brain tumor care. It shows the size and shape of the tumor. More advanced types of MRI—like DWI, PWI, and SWI—help doctors check how dense the tumor is, how much blood it gets, and the condition of its blood vessels. These details are useful in telling whether a tumor is growing or if the changes are due to side effects of treatment like swelling or dead tissue (29)
Functional MRI (fMRI)
fMRI looks at blood flow changes in the brain to find areas involved in key functions such as speaking or moving. This helps doctors avoid damaging those areas during surgery. It also supports radiotherapy planning by making sure important parts of the brain aren’t harmed by radiation (30)
Diffusion Tensor Imaging (DTI)
DTI tracks the movement of water in the brain to show white matter pathways—like the ones used for movement and thinking. This is especially helpful for planning surgery near important brain structures. Including DTI in treatment planning helps protect the patient’s ability to move and think properly (31)
Positron Emission Tomography (PET)
PET scans look at how active the tumor cells are by using special chemicals (called tracers) that highlight living tumor tissue. This helps doctors see which parts of the tumor are still active, especially when MRI images are unclear. Using PET in planning can improve both surgery and radiation treatment by targeting the tumor more precisely (32)
Combining Multiple Imaging Methods
Using different imaging tools together gives a more complete picture of the tumor and its effect on the brain. For example, combining fMRI and DTI helps map both how the brain works and how it’s connected. PET and MRI together can more accurately show tumor borders, which is very helpful for safer and more effective treatment planning (33)
3.1.3 Biomarker-Guided Chemotherapy in Gliomas
In recent years, doctors have started using molecular biomarkers to help decide which chemotherapy treatments will work best for glioma patients. Two of the most important biomarkers are MGMT promoter methylation and IDH gene mutations. These markers not only guide treatment choices but also help predict how well a patient might respond and how long they might survive. MGMT Promoter Methylation and Response to Temozolomide: The MGMT gene plays a role in fixing damaged DNA in cells. When the promoter region of this gene is methylated (a type of chemical change), its ability to repair DNA is reduced. As a result, tumor cells with methylated MGMT are more likely to be damaged and killed by chemotherapy drugs like temozolomide (TMZ). However, MGMT methylation does not always guarantee a better response to TMZ. A study by Egaña et al. (2020) found that some patients with methylated MGMT still did not respond well to TMZ, which suggests that other biological factors might also play a role in how effective the treatment is (34)
IDH Mutations and Their Impact on Prognosis
Mutations in the IDH1 and IDH2 genes are often found in low-grade gliomas and in secondary glioblastomas. These genetic changes are usually linked to better outcomes, including longer survival and stronger responses to chemotherapy. According to Houillier et al. (2010), patients with IDH-mutant gliomas responded better to TMZ and had improved survival compared to those without the mutation (35). When both IDH mutation and MGMT promoter methylation are found in the same tumor, the prediction of treatment response becomes even more accurate. Christensen et al. (2011) showed that this combination helps doctors better estimate how patients with secondary glioblastomas will respond to TMZ therapy (26). Using molecular biomarkers like MGMT methylation and IDH mutations allows for a more personalized approach to glioma treatment. These markers help identify which patients are more likely to benefit from chemotherapy, especially temozolomide, and help improve overall treatment planning.
3.1.4 Liquid Biopsies and Monitoring in Glioma Treatment:
Liquid biopsy is a new and less risky way to learn about brain tumors. Instead of using surgery to get tumor tissue, doctors can test body fluids like blood or cerebrospinal fluid (CSF) to find tumor-related substances such as DNA or RNA. This method is helpful because it can be done multiple times to keep track of the tumor and how it responds to treatment.
Evaluating Treatment Effectiveness Doctors can check ctDNA levels regularly to see whether a treatment is working or if it needs to be changed (36). Detecting Early Recurrence This method can sometimes find signs that the tumor is coming back before it shows up on traditional scans (37). Why CSF Might Be Better Than Blood: It is because although drawing blood is easier, CSF samples usually give more accurate results in brain tumors like gliomas. This is because the blood-brain barrier limits how much tumor DNA can move into the blood. Since CSF is closer to the brain, it often contains more tumor material (38).. Even though liquid biopsy is a promising tool, there are still some issues—such as improving the sensitivity of tests and making the methods consistent across different labs. Scientists are actively working on these problems so that liquid biopsies can become a regular part of glioma treatment in the future (39).
3.2 Artificial Intelligence in Neuro-Oncology Radiotherapy
AI in Tumor Mapping and Brain Function Preservation Artificial intelligence is significantly improving the accuracy and efficiency of identifying tumor regions for radiotherapy. Traditionally, this process was time-consuming and varied clinicians. With AI, tumor boundaries can be outlined more consistently and quickly, reducing errors and enhancing treatment planning.
Whole brain radiotherapy (WBRT) is commonly used for patients with multiple brain tumors. However, it can unintentionally affect healthy regions such as the hippocampus, a critical area for memory. Radiation to the hippocampus may lead to memory loss. To address this, deep learning algorithms have been developed to design treatment plans that avoid irradiating the hippocampus. These AI-generated plans can be created in under 10 minutes, improving both the speed and safety of care (40)
Personalized Radiotherapy for Glioblastoma:
Glioblastoma is an aggressive brain tumor that spreads rapidly into nearby tissues, making it difficult to treat using traditional methods. AI tools now combine advanced imaging techniques, such as MRI and FET-PET, with tumor growth prediction models. This integration allows doctors to better understand how a tumor may evolve and to create personalized radiation plans that effectively target the tumor while preserving surrounding healthy brain tissue. (41)
AI in Dose Prediction and Quality Assurance:
Accurate radiation dosing is crucial in cancer therapy. Deep learning models like the 3D Dense Dilated U-Net can predict how radiation doses will be distributed using CT images and existing treatment plans. These systems also help detect low-quality or potentially unsafe plans at an early stage, enabling healthcare providers to make informed adjustments (42). For quality assurance, AI has streamlined the verification process, making it faster and more reliable. Research indicates that AI tools can save around 16 minutes during plan review and detect more than half of the safety issues before treatment begins (43).
AI in Brachytherapy (Internal Radiotherapy):
AI is also being applied in brachytherapy, a form of internal radiation therapy. It assists in tumor outlining, dose calculation, and outcome prediction. These tools help reduce manual effort and accelerate the overall process. However, widespread clinical use requires thorough validation and constant human supervision to ensure patient safety (44).
Importance of Human Oversight:
Despite the many advantages AI brings to radiotherapy, it should not replace human expertise. AI systems may carry biases from their training data and lack the ability to understand a patient’s unique health needs or personal values. Human judgment remains essential to ensure that treatment plans are safe, ethical, and tailored to each individual. Radiation oncologists provide the necessary experience, insight, and empathy that AI cannot replicate (45).
3.3 AI-Assisted Surgical Planning in Brain Tumor Treatment
Surgery for brain tumors, especially glioblastoma, requires careful planning. If surgery won't improve patient outcomes, it might cause more harm than good, so doctors must assess each case individually. AI and Machine Learning tools now help doctors make these decisions by offering personalized insights beyond traditional scoring systems. ML models predict survival chances based on age, tumor type, and tumor count(46). 1. Predicting Survival and Tumor Progression AI tools are improving survival and tumor behavior prediction: Deep learning and radiomics estimate post-surgery survival in glioblastoma with 74.5% accuracy. ML models predict tumor recurrence using pre-surgery scans. Connectome-based AI predicts genetic features like IDH mutation from MRI scans, with AUC scores of 0.76-0.94. Voxel-based ML tools predict tumor regrowth locations for better surgical planning(47). 2. Assessing Whether Tumor Can Be Removed For complex cases like glioblastoma, AI systems evaluate tumor removal feasibility through MRI images. Marcus et al. developed an AI tool to rate tumor complexity, while Kommers et al. created GSI-RADS for consistent tumor descriptions(48). 3. AI for Tumor Segmentation and Resection Assessment Zanier et al. used U-Net deep learning to analyze glioma scans, mapping tumors and assessing removal extent. The RANO Resect Group advocates AI for measuring remaining tumor volume. Fathi Kazerooni et al. used AI to differentiate tumor areas for personalized removal strategies(49). 4. Using Brain Network Maps (Connectome) for Surgery Quicktome™ maps brain functions for safer surgeries. Luckett et al.'s 3D CNN models map language and movement areas with 96% accuracy. ML tools help surgeons identify critical brain areas, even when displaced by tumors(50)
4. AI FOR PRE-SURGICAL PLANNING
Once surgery is an option, AI tools make the planning process faster and more accurate:
CNN-based tools can outline important brain parts much faster than humans—up to 30 times quicker. AI can also help plan the direction and angle of radiation therapy by modelling how tissues will move during treatment. The ROBOCAST project uses AI to create detailed surgical roadmaps, already tested in procedures like brain biopsies. In summary, AI is transforming how brain tumor surgeries are planned and performed. It helps doctors predict patient outcomes, plan safe surgeries, and protect critical brain functions. As the technology grows, AI is expected to become an essential tool in providing safer and more personalized care for brain tumor patients.
5. AI IN NEUROSURGICAL ONCOLOGY
Neurosurgical oncology is a specialized discipline that integrates the expertise of neurosurgeons, oncologists, radiologists, and other specialists to deliver comprehensive care for patients with benign and malignant tumors of the brain and spine. Its primary objectives include maximizing safe tumor resection, alleviating symptoms, improving quality of life and survival outcomes, and advancing research and innovation. Surgical intervention is indicated for tissue diagnosis, cytoreduction, relief of mass effect with potential neurological improvement, and enhancement of survival and quality of life. In glioma management, MGMT gene methylation status has emerged as an important prognostic biomarker predicting responsiveness to alkylating agents. Additionally, the Response Assessment in Neuro-Oncology (RANO) criteria were developed to objectively differentiate treatment-related changes from true tumor progression in both low- and high-grade gliomas. Overall, neurosurgical oncology plays a pivotal role in glioma care through diagnosis, symptom control, and enabling direct therapeutic delivery that bypasses the blood–brain barrier.(51)
Laser interstitial thermal therapy (LITT) is an adjuvant treatment for intracranial lesions that are treatment refractory or in deep or eloquent brain. Initial studies of LITT in surgical neuro-oncology are limited in size and follow-up. The result shows A total of 91 patients underwent 100 LITT procedures; 61% remain alive with 72% local control at a median 7.2-mo follow-up. (52)
Artificial intelligence (AI) has been explored for its potential applications in the field of neurosurgery. Recent research indicates that machine learning (ML) offers considerable promise in neuro-oncological care, spine surgery, epilepsy management, and other neurosurgical domains. It is imperative for clinicians to familiarize themselves with the various forms of AI, as a comprehensive understanding of these technologies, rather than blind trust, is crucial for their appropriate and safe integration into patient care (53).
Parduzi et al. investigated artificial intelligence–based intraoperative neurophysiological monitoring (IONM) to improve preservation of motor pathways during complex neurosurgical procedures. Using machine learning and deep learning models trained on large multicenter datasets of motor-evoked potentials (MEPs), the study demonstrated high accuracy in muscle classification, with random forest and convolutional neural networks showing strong performance. Explainable AI techniques revealed that frequency components and peak latencies are key features for accurate MEP interpretation. These findings suggest that AI-assisted IONM may reduce muscle mislabeling, support the development of standardized warning criteria, and ultimately enhance intraoperative patient safety.
(54).
Deep brain stimulation (DBS) has emerged as a key neurosurgical therapy for movement and certain psychiatric disorders. Traditionally, optimal DBS target localization relies on either a direct method, which visualizes the target nucleus on MRI, or an indirect method based on geometric calculations using the anterior commissure–posterior commissure (AC–PC) reference system. However, current evidence is limited by small sample sizes, preventing definitive conclusions about the reliability and clinical superiority of AI-assisted approaches. Although AI applications in DBS are still at an early stage and lack statistically robust validation, emerging tools, including large language models such as ChatGPT and Gemini, show promise in text-based tasks. Their role in image-based analysis—critical for neurosurgical planning and target localization—remains underexplored and requires further investigation.(55)
5.1 Robot-assisted neurosurgery:
Robot-assisted neurosurgery, commonly referred to as robotic surgery, allows physicians to execute a diverse array of intricate procedures with enhanced precision, flexibility, and control compared to traditional techniques. Typically, robotic surgery is performed through small incisions to enable minimally invasive procedures within the brain, although it is occasionally utilized in open surgeries as well. Several robotic systems are employed, including
PUMA-200 (Programmable Universal Manipulation Arm or Programmable Universal Machine Assembly). The PUMA 200 was also employed for holding and manipulating surgical retractors while achieving radical excision of thalamic astrocytomas in six children in 1991.
da Vinci: This is the most widely used master-controlled console-based robotic system. Its application in neurosurgery has yet to become widespread due to factors such as the system's large size and the limited number of instruments.
SOCRATES: This was the first tele-mentoring system in neurosurgery, wherein a robotic arm is controlled by a mentor from another institution.
Robotic Stereotactic Assistance (ROSA): Also known as a robotic operating surgical assistant, this single-arm robot provides excellent dexterity and accuracy, thereby reducing operative time in procedures such as DBS, stereo electroencephalography (SEEG), and repetitive nerve stimulation (RNS), among others (56). These various systems are employed in neurosurgery to enhance the quality of surgery and improve success rates.
6. CHALLENGERS AND FUTURE DIRECTIONS
Artificial intelligence (AI) in neuro-oncology encounters several challenges, including issues related to data quality and diversity, model interpretability, ethical considerations, and the necessity for robust legal frameworks. Ethical considerations in the integration of AI for brain tumor diagnosis, prognosis, and treatment encompass data privacy, algorithmic fairness, legal liability, and social implications. This focus includes diagnostic AI models for key genomic markers, predictive AI models for response assessment before and after therapy, and the differentiation of true disease progression from treatment-related changes, which remains a significant challenge in current clinical neuro-oncology practice (7,57). Ethically, it is imperative to balance technological advancement with patient consent, dignity, and privacy, ensuring the responsible use of AI tools. Legally, AI in healthcare must navigate complex regulations governing patient data and medical decision-making. Clinicians require substantial training to interpret AI results, and these systems must undergo rigorous testing for accuracy and reliability using extensive datasets. Ultimately, the advancement of AI technology depends on continuous development and innovation to enhance its efficacy in the diagnosis, treatment, management, and research of brain tumors and other malignancies. There is an urgent need for further exploration and the development of novel algorithms and tools across various domains, including imaging techniques, computational models, and data fusion strategies (58).
7. CONCLUSION:
Artificial intelligence is transforming the detection, diagnosis, and treatment of brain cancers by improving imaging interpretation, enabling early tumor detection, and supporting personalized treatment planning. Through machine learning and deep learning, AI enhances accuracy in surgery and radiation therapy, improves safety with robotic assistance, and accelerates drug discovery by identifying patients most likely to benefit from specific therapies. While AI offers major advances in precision and efficiency of brain cancer care, its full potential requires further research, robust validation, appropriate infrastructure, and careful attention to data privacy, fairness, and transparency.
REFERENCES

Siva Krishna Konda, Madhuri Kokkonda, Sumayya Qatun Mohammed, Sushma Kottapalli, AI-Driven Approaches in Neuro-Oncology: From Imaging to Treatment, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 801-819. https://doi.org/10.5281/zenodo.19421818
 10.5281/zenodo.19421818
10.5281/zenodo.19421818
