
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
School of Pharmaceutical Sciences, Shri Guru Ram Rai University, Dehradun, Uttarakhand, India
Cetirizine, a second-generation antihistamine, remains a key therapeutic agent in the management of allergic disorders due to its established efficacy and favorable safety profile. This updated evidence-based review evaluates the clinical relevance of cetirizine in conditions such as allergic rhinitis, chronic urticaria, and allergic conjunctivitis. Its selective antagonism of peripheral H1 receptors provides effective symptom relief while minimizing central nervous system effects compared to first-generation antihistamines.Clinical studies and guideline recommendations consistently support its role in reducing nasal, cutaneous, and ocular symptoms, with demonstrated benefits in both adult and pediatric populations. In addition to its antihistaminic action, cetirizine exhibits anti-inflammatory effects, including modulation of cytokine release and inhibition of inflammatory cell migration, contributing to improved disease control.Recent advancements, including intravenous and topical formulations, have further expanded its therapeutic applications. Cetirizine is generally well tolerated, with a low incidence of adverse effects and limited drug interaction potential, although dose adjustment may be required in patients with renal impairment.Overall, cetirizine continues to hold significant clinical relevance in modern allergy management, supported by robust evidence and evolving therapeutic applications.
Allergic disorders represent a significant and growing global health concern, affecting individuals across all age groups and substantially impairing quality of life. Conditions such as allergic rhinitis, chronic urticaria, and allergic conjunctivitis are among the most prevalent manifestations, often characterized by symptoms including sneezing, itching, rhinorrhea, and erythema. The underlying pathophysiology of these conditions involves immunoglobulin E (IgE)-mediated hypersensitivity reactions, leading to the release of inflammatory mediators, particularly histamine, from mast cells and basophils.
Histamine plays a central role in the development of allergic symptoms through activation of H1 receptors, resulting in vasodilation, increased vascular permeability, and sensory nerve stimulation. Consequently, antihistamines targeting H1 receptors have remained a cornerstone in the pharmacological management of allergic diseases. However, first-generation antihistamines are often associated with undesirable effects such as sedation, impaired cognitive function, and anticholinergic activity, which limit their clinical utility, especially during long-term therapy.
The development of second-generation antihistamines marked a significant advancement in allergy management by offering improved receptor selectivity and reduced central nervous system penetration. Among these, cetirizine, an active metabolite of hydroxyzine, has gained widespread acceptance due to its rapid onset of action, sustained efficacy, and favorable safety profile. In addition to its antihistaminic activity, emerging evidence suggests that cetirizine exhibits anti-inflammatory properties, including the inhibition of cytokine release and modulation of inflammatory cell migration, thereby contributing to its therapeutic effectiveness.
Over the past three decades, cetirizine has been extensively evaluated in both clinical trials and real-world settings, demonstrating consistent efficacy in the management of allergic conditions across diverse patient populations. Its availability in multiple formulations, including oral, ophthalmic, and more recently intravenous preparations, has further expanded its clinical applicability.
In this context, the present review aims to provide an updated and comprehensive evaluation of the clinical relevance of cetirizine in allergy management. Emphasis is placed on its pharmacological characteristics, therapeutic applications, safety considerations, and emerging clinical evidence, with the objective of highlighting its continued importance in modern clinical practice.
2. Pharmacological Profile of Cetirizine
Cetirizine is a second-generation antihistamine derived as an active metabolite of hydroxyzine, designed to provide effective histamine blockade with minimal central nervous system (CNS) effects. Its pharmacological properties contribute significantly to its widespread clinical use in allergic disorders.
2.1 Mechanism of Action
Cetirizine acts as a potent and selective antagonist of peripheral histamine H1 receptors. By competitively inhibiting histamine binding, it effectively suppresses the early-phase allergic response, thereby reducing symptoms such as vasodilation, increased vascular permeability, and sensory nerve stimulation.
Beyond its classical antihistaminic activity, cetirizine exhibits additional anti-inflammatory effects. It has been shown to:
These properties contribute to attenuation of the late-phase allergic response, enhancing its overall therapeutic efficacy.
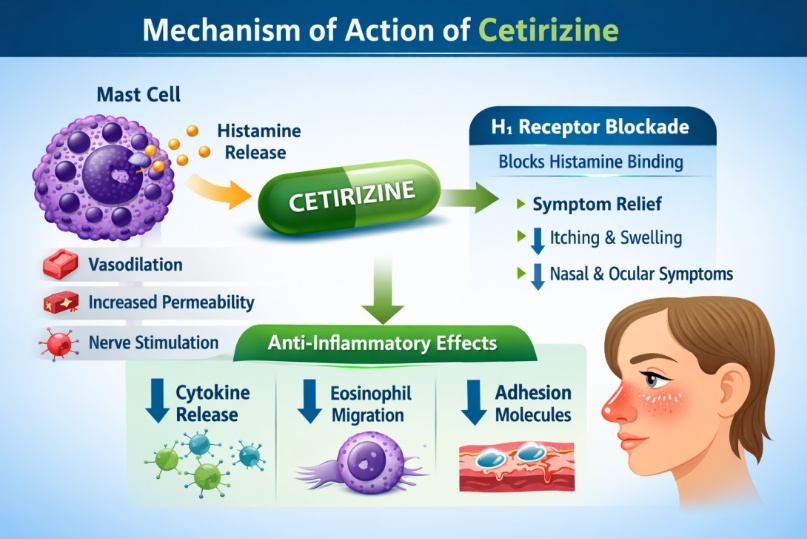
Fig1 Mechanism of Action of Cetrizine
2.2 Pharmacokinetics
Cetirizine demonstrates predictable and linear pharmacokinetics, supporting its once-daily dosing regimen.
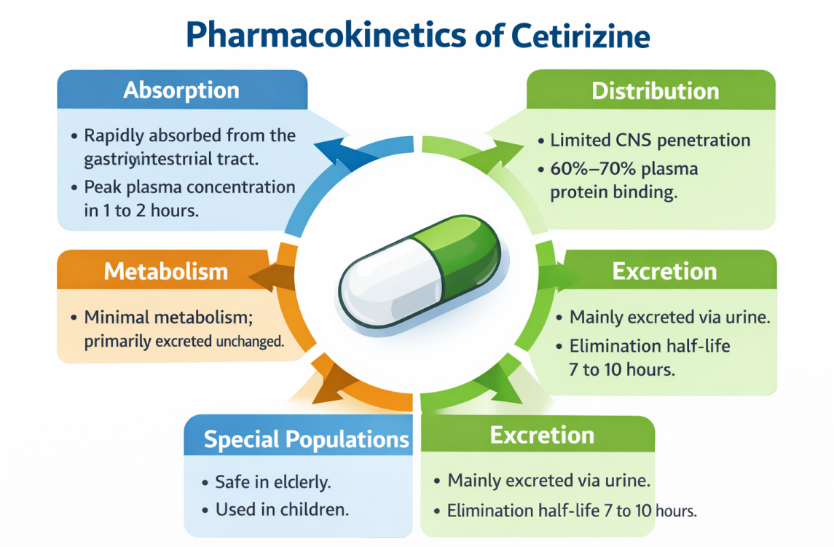
Fig2 Pharmacokinetics of Cetirizine
Table 1 Pharmacokinetics of Cetirizine
|
Parameter |
Description |
|
Absorption |
Rapid absorption with peak plasma concentration within 1 hour |
|
Bioavailability |
Approximately 70% |
|
Distribution |
Limited penetration across the blood–brain barrier |
|
Protein Binding |
~93% bound to plasma proteins |
|
Metabolism |
Minimal hepatic metabolism |
|
Elimination |
Primarily excreted unchanged via kidneys |
|
Half-life |
Approximately 8–10 hours |
The limited CNS penetration is attributed to its low lipophilicity and interaction with efflux transporters such as P-glycoprotein, resulting in reduced sedative effects compared to first-generation antihistamines.
2.3 Special Pharmacokinetic Considerations
Certain patient populations require careful consideration:
Overall, the pharmacological profile of cetirizine reflects a balance between potent antihistaminic activity and favorable safety characteristics, making it suitable for both short-term and long-term management of allergic conditions.
3. Clinical Applications of Cetirizine
Cetirizine is widely utilized in the management of various allergic conditions due to its rapid onset of action, sustained efficacy, and favorable safety profile. Its clinical applications extend across respiratory, dermatological, and ocular allergic disorders.
3.1 Allergic Rhinitis
Allergic rhinitis is one of the most common indications for cetirizine therapy. It effectively alleviates symptoms such as sneezing, nasal itching, rhinorrhea, and nasal congestion. Clinical studies have demonstrated that cetirizine provides significant improvement in both seasonal and perennial allergic rhinitis.
Its once-daily dosing and rapid onset contribute to improved patient compliance and symptom control. Additionally, cetirizine has been shown to reduce inflammatory mediators involved in nasal mucosal inflammation.
3.2 Chronic Urticaria
Cetirizine is considered a first-line agent in the treatment of chronic urticaria due to its ability to control pruritus and wheal formation. It effectively reduces histamine-induced skin reactions and improves quality of life in affected patients.
In cases of inadequate response, combination therapy with other agents may be considered. Its favorable safety profile allows for prolonged use in chronic conditions.
3.3 Allergic Conjunctivitis
Cetirizine is also effective in managing allergic conjunctivitis, particularly in reducing ocular itching, redness, and tearing. Ophthalmic formulations provide targeted action with minimal systemic exposure.
Clinical evidence supports its rapid symptom relief and good tolerability in both adult and pediatric populations.
3.4 Other and Emerging Uses
Recent research has explored additional therapeutic roles of cetirizine, including:
These emerging applications highlight its expanding clinical relevance beyond traditional indications.
Table 2: Major Clinical Uses of Cetirizine
|
Condition |
Clinical Effect |
Key Benefits |
|
Allergic Rhinitis |
Reduces sneezing, rhinorrhea, itching |
Rapid onset, once-daily dosing |
|
Chronic Urticaria |
Controls itching and wheal formation |
Suitable for long-term use |
|
Allergic Conjunctivitis |
Relieves ocular symptoms |
Local and systemic formulations |
|
Drug Hypersensitivity Prevention |
Reduces infusion-related reactions |
Alternative to sedating antihistamines |
|
Dermatological Uses |
Anti-inflammatory action |
Emerging therapeutic rol |
4. Comparative Efficacy of Cetirizine
The therapeutic effectiveness of cetirizine has been extensively compared with other first- and second-generation antihistamines in the management of allergic disorders. These comparisons are essential to determine its relative clinical value, particularly in terms of efficacy, safety, onset of action, and tolerability.
Compared to first-generation antihistamines such as diphenhydramine, cetirizine demonstrates similar or superior efficacy in symptom control while significantly reducing adverse effects such as sedation and cognitive impairment. This improved safety profile is largely attributed to its limited penetration across the blood–brain barrier.
When compared with other second-generation antihistamines, including loratadine and levocetirizine, cetirizine exhibits a balanced profile. Clinical studies suggest that cetirizine may provide a slightly faster onset of action and more pronounced symptom relief in some patients, particularly in urticaria. Levocetirizine, being the active enantiomer of cetirizine, may show enhanced potency, although the clinical differences are often minimal.
Additionally, cetirizine has demonstrated comparable effectiveness to newer antihistamines while maintaining cost-effectiveness and accessibility, making it a preferred option in routine clinical practice.
Table 3: Comparative Evaluation of Cetirizine with Other Antihistamines
|
Parameter |
Cetirizine |
Loratadine |
Levocetirizine |
Diphenhydramine |
|
Generation |
Second |
Second |
Second |
First |
|
Efficacy |
High |
Moderate–High |
Very High |
High |
|
Onset of Action |
Rapid |
Moderate |
Rapid |
Rapid |
|
Sedation |
Mild |
Minimal |
Mild |
High |
|
Duration of Action |
Long (24 hr) |
Long (24 hr) |
Long (24 hr) |
Short |
|
CNS Penetration |
Low |
Very low |
Low |
High |
|
Safety Profile |
Favorable |
Very favorable |
Favorable |
Limited |
|
Clinical Use |
Widely preferred |
Alternative |
Potent option |
Acute/emergency use |
Although newer antihistamines offer certain pharmacological advantages, cetirizine continues to maintain a strong position due to its consistent efficacy, acceptable safety profile, and widespread clinical familiarity.”
5. Safety and Tolerability of Cetirizine
Cetirizine is widely regarded as a safe and well-tolerated antihistamine, particularly when compared to first-generation agents. Its favorable safety profile is primarily attributed to its selective action on peripheral H1 receptors and limited penetration into the central nervous system. This results in reduced sedative and anticholinergic effects, making it suitable for both short-term and long-term use in allergic conditions.
5.1 Common Adverse Effects
Although generally mild, some patients may experience:
These effects are typically transient and do not require discontinuation of therapy in most cases.
5.3 Safety in Special Populations
Cetirizine has been evaluated across various patient groups:
Table 4: Safety Profile of Cetirizine
|
Category |
Details |
|
Common Adverse Effects |
Somnolence, fatigue, dry mouth, headache |
|
Rare Adverse Effects |
Hepatotoxicity, dystonia, hypersensitivity reactions |
|
CNS Effects |
Minimal compared to first-generation antihistamines |
|
Drug Interactions |
Low potential; caution with CNS depressants |
|
Pregnancy Safety |
Generally considered low risk |
|
Lactation |
Minimal excretion in breast milk |
|
Renal Impairment |
Dose adjustment required |
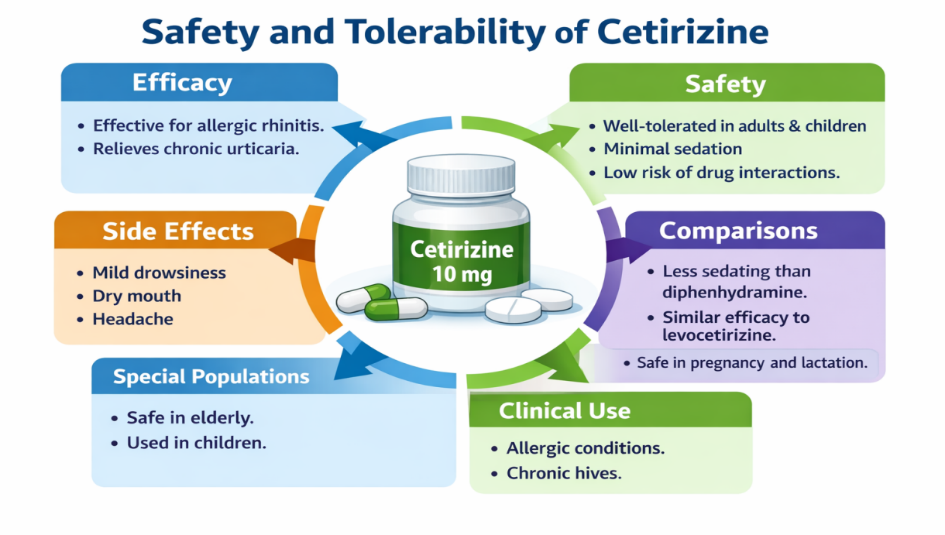
Fig 3 Safety and Tolerability of Cetirizine
6. Recent Advances and Emerging Perspectives
In recent years, the clinical utility of cetirizine has expanded beyond its conventional role as an oral antihistamine, with growing evidence supporting its use in novel formulations and broader therapeutic settings. These advances reflect ongoing efforts to enhance its efficacy, improve patient compliance, and explore additional pharmacological benefits.
6.1 Intravenous Formulation
One of the most notable developments is the introduction of intravenous (IV) cetirizine, which has been evaluated for the management of acute allergic reactions, particularly urticaria. Clinical studies have demonstrated that IV cetirizine provides rapid symptom relief comparable to diphenhydramine, with the added advantage of reduced sedation and improved tolerability.
This formulation is especially useful in emergency settings where quick onset of action and minimal central nervous system effects are desired.
6.2 Topical Applications in Dermatology
Emerging research has explored the use of topical cetirizine in dermatological conditions, including androgenic alopecia. Preliminary findings suggest that its anti-inflammatory properties and ability to modulate local immune responses may contribute to improved outcomes.
Although still in early stages, these findings indicate a promising direction for non-traditional applications.
6.3 Role in Hypersensitivity Reaction Prevention
Cetirizine has also been investigated as a preventive agent for drug-induced hypersensitivity reactions, particularly in patients undergoing chemotherapy or monoclonal antibody therapy.
Compared to sedating antihistamines, cetirizine offers effective prophylaxis with better tolerability, making it a suitable alternative in clinical practice.
6.4 Anti-inflammatory and Immunomodulatory Potential
Beyond H1 receptor antagonism, recent studies highlight cetirizine’s role in:
These properties suggest that cetirizine may contribute to disease modification rather than merely symptomatic relief, particularly in chronic allergic conditions.
6.5 Expanding Clinical Scope
The versatility of cetirizine is further reflected in its:
These evolving applications reinforce its continued clinical relevance.
“The emerging evidence on alternative formulations and extended therapeutic applications positions cetirizine as more than a conventional antihistamine, highlighting its evolving role in both acute and chronic management of allergic and inflammatory conditions.”
DISCUSSION
Cetirizine has maintained a prominent position in the management of allergic disorders due to its consistent efficacy, predictable pharmacokinetics, and favorable safety profile. The evidence reviewed in this manuscript highlights its effectiveness across a range of conditions, including allergic rhinitis, chronic urticaria, and allergic conjunctivitis, where it provides reliable symptom control and improves patient quality of life.
A key strength of cetirizine lies in its balanced pharmacological profile. Unlike first-generation antihistamines, it demonstrates minimal central nervous system penetration, thereby reducing sedation and cognitive impairment. At the same time, it retains sufficient potency to effectively antagonize peripheral H1 receptors. Comparative studies indicate that while newer antihistamines may offer marginal advantages in select parameters, cetirizine continues to deliver comparable clinical outcomes with broader accessibility and cost-effectiveness.
Another important aspect is its additional anti-inflammatory activity, which extends its therapeutic benefits beyond simple histamine blockade. The ability to modulate cytokine release and inhibit inflammatory cell migration may contribute to improved control of chronic allergic conditions. Furthermore, recent advances, including intravenous and topical formulations, suggest that cetirizine’s clinical applications are expanding, particularly in acute care and dermatological settings.
Despite these advantages, certain limitations should be acknowledged. Mild sedation, although less frequent, may still occur in sensitive individuals. In addition, dose adjustments are necessary in patients with renal impairment, and rare adverse effects such as hepatotoxicity have been reported. Continued pharmacovigilance and well-designed clinical trials are essential to further define its long-term safety and emerging roles.
Overall, the accumulated evidence supports the continued use of cetirizine as a reliable and versatile antihistamine, with evolving applications that extend beyond traditional indications.
CONCLUSION
Cetirizine remains a cornerstone in the pharmacological management of allergic disorders due to its well-established efficacy, favorable safety profile, and broad clinical applicability. Its selective H1 receptor antagonism, combined with emerging anti-inflammatory properties, contributes to effective symptom control in both acute and chronic conditions.
The availability of multiple formulations and its suitability across diverse patient populations further enhance its clinical utility. Although newer antihistamines continue to be developed, cetirizine maintains a strong position owing to its consistent performance, accessibility, and long-standing clinical experience.
Future research should focus on exploring its expanded therapeutic potential, optimizing dosing strategies in special populations, and further elucidating its anti-inflammatory mechanisms. Such efforts will help to reinforce its role in modern allergy management and support evidence-based clinical decision-making.
REFERENCES


Aditi Rana, Dr. Anuj Nautiyal, Clinical Relevance of Cetirizine in Allergy Management: An Updated Evidence-Based Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 1181-1190 https://doi.org/10.5281/zenodo.19465983
 10.5281/zenodo.19465983
10.5281/zenodo.19465983