1,2Department of Pharmacy, Annamalai university, Chidambaram, Tamilnadu.
3Professor, Department of General Surgery, Government Cuddalore Medical College and Hospital, (GCMCH), Chidambaram, Tamil Nadu.
Background: In mixed surgical populations, surgical site infections are fewer in laparoscopic surgery than in open surgery. It is not clear if this is also the case for obese patients, who have a higher risk of surgical site infections than nonobese patients. Objective: To compare surgical site infections rate in obese patients after laparoscopic surgery with open general abdominal surgery. Methods: A Prospective study was conducted in government Cuddalore Medical Collage and Hospital, Chidambaram, involving patients who underwent laparoscopic surgery and open surgery. Data were collected on demographics variables, clinical features, treatment duration, time to clinical improvement hospital stay length, adverse events, and overall treatment outcomes. Comparative statistical analysis were performed to assess differences between the two groups. Result: Laparoscopic Surgery is Associated with Lower risk of Surgical Site Infections (SSIs): Compared to open surgery, laparoscopic surgery is linked to a reduced risk of SSIs. Significant reduction in SSI rates: The analysis revealed a statistically significant decrease in SSI rates in patients undergoing laparoscopic surgery. Greatest benefit in Colorectal Surgery: Subgroup analysis showed that the benefit of laparoscopic surgery was most pronounced in patients undergoing colorectal surgery. Implications: Surgical practice: The findings suggest that laparoscopic surgery should be considered as a preferred approach to reduce SSI rates. Patient outcomes: The reduced risk of SSIs associated with laparoscopic surgery may lead to improved patient outcomes, including reduced morbidity and mortality. Conclusion: In this retrospective cohort study comparing the outcomes of laparoscopic and OS, it was clearly demonstrated that laparoscopic procedures offered statistically significant advantages over traditional open surgeries in terms of shorter operative times, less blood loss, and shorter hospital stays following surgery.
Surgical site infections (SSI) are the commonest health care associated infections (HCAI). They are severely compromised patient safety, are a significant burden on healthcare resources and have an adverse impact on patient quality of life. The incidence of SSI’s can be as high as 10% after colorectal procedures. The first series of laparoscopic colorectal surgery was reported in 1991. Numerous multicentre randomised controlled trials (RCTs) carried out internationally have now established the efficacy of the laparoscopic approach for colorectal procedures. A laparoscopic approach is being increasingly used to undertake colorectal procedures. It provides advantages over the traditional open approach with smaller incisions, a shorter hospital stays and equal oncological outcomes. Additional benefits of minimally invasive surgery include significant quality improvement in terms of reduced morbidity and suffering for the patient with all the associated inconvenience and cost. There is a significant improvement in the functioning of the health system if these quality improvements lead to sustained reduction in return to hospital and to the operating theatre. These include improved patient flow in hospitals with the capacity created by avoiding unexpected, non-elective returns to hospital, reduced primary care con saltation’s and medication prescriptions and better antibiotic governance. Since its inception, laparoscopic surgery has represented a paradigm transformation in surgical techniques. It quickly acquired traction as a preferred alternative to traditional open surgical techniques due to its minimal invasiveness, smaller incisions, and reputation for reduced postoperative pain. However, as with any medical advancement, continuous evaluation of its relative advantages and disadvantages is required. Surgical site infections (SSIs) are one of the most prevalent postoperative complications. In addition to posing a hazard to patient safety, they increase healthcare costs, prolong hospitalization, and diminish the patient's comfort. Historically, traditional OS, with its larger incisions and increased exposure, has been associated with higher SSI rates. Nonetheless, with the ongoing refinement of surgical procedures and improved aseptic measures, it is essential to determine whether laparoscopic techniques truly reduce the risk of infection. Since the late twentieth century, laparoscopic procedures, including cholecystectomy, appendectomy, and hernia correction, have gained widespread acceptance. In the 2000s, laparoscopic appendectomy, which has been performed since the 1980s, became the standard treatment for appendicitis. The advantages of this technique, such as improved diagnostic capability, superior cosmetic results, reduced postoperative complications, and expedited recovery, are noteworthy. There are, however, contradictory findings regarding morbidity and infection rates following surgery. While some studies indicate com parable or even lower rates of complications such as intraabdominal abscesses in laparoscopic procedures, others indicate increased risks, especially in more com plex surgical cases. Recovery outcomes, a crucial aspect of our research, are multidimensional. They include not only the duration of physical recovery, but also parameters such as postoperative pain intensity, hospitalization length, and the timeframe for a patient's return to routine activities. A quicker recovery not only improves the patient's experience but also reduces the societal and financial burdens associated with a protracted convalescence. And even though laparoscopic surgery is frequently promoted for its rapid recovery advantage, empirical evidence is required to support such claims in comparison to traditional OS.
A retrospective cohort study was conducted at a tertiary care centre. Focusing on patients who underwent either laparoscopic or traditional OS, during the study period.
This study was conducted in the Department of General Surgery, Government Cuddalore Medical College and Hospital, Chidambaram, Tamil Nadu, a tertiary care referral centre catering to a vast rural and semi-urban population in and around the Cuddalore district.
The duration of the study was six months, from October 2024 to March 2025.
The study included a total of 180 patients, with a diverse range of ages, backgrounds, and health statuses. The cohort was divided into:
The decision for laparoscopic over OS was not standardized but was generally influenced by surgical experience, patient preference, and surgical condition. Patient data, encompassing preoperative assessments, operative outcomes, and postoperative complications, were retrospectively retrieved from a prospective database.
A structured case record form (CRF) was employed to capture data on demographic information, Clinical profile, characteristic of operation reports, and follow-ups assessments performed by the surgical team.
Wound assessment:
Follow-up:
All the quantitative variables in the present study were analysed using MS Excel, SPSS, JSAP, MS Word. Categorical variables were presented as numbers and percentages, while continuous variables as means ± standard deviation. The chi-square test was used for categorical data, and the student’s t-test for continuous data analysis, utilizing SPSS version 25.0. Statistical significance was set at a p-value < 0.05.
Various parameters were evaluated in the comparative analysis of patients enduring laparoscopic surgery (n= 105) versus OS (n = 75). In the laparoscopic group, the mean age was 42.3 ± 11.1 years, whereas in the OS group, the average age was 47.2 ± 12.0 years (p > 0.05). In terms of gender distribution, a laparoscopic group comprised 33 men and 72 women, while the OS group comprised 47 men and 28 women (p < 0.05). This disparity was statistically significant. The laparoscopic group had a mean BMI of 25.14 kg/m2, while the OS group a had BMI of 24.01 kg/m2 (p > 0.05), without showing a significant difference. The period of complaint prior to surgery was marginally longer in OS group, at 1.3 months than in the laparoscopic surgery group, at 1.1 months (p > 0.05). In terms of associated comorbidities, 8 patients (7.61%) in the laparoscopic group had diabetes, as contrasted to 4 patients (5.33%) in OS group (p > 0.05). Hypertension was found in 21 patients and 14 patients, respectively, indicating a non-significant difference between the two groups. Six patients (5.71%) in laparoscopic group and 4 (5.33%) in the OS group reported prior surgical interventions (Table 1).
Table 1. Demographics and baseline characteristics of the study patients.
|
Parameter |
Laparoscopic group (n = 105) |
Open surgery (OS) group (n = 75) |
χ2 |
p-value |
|
Age (mean ± SD) |
42.3 ± 11.1 |
47.2 ± 12.3 |
3.13 |
0.077 |
|
Gender (Male/Female) |
33/72 |
47/28 |
10.57 |
0.0001* |
|
Mean BMI (kg/m2) |
25.14 ± 3.13 |
24.01 ± 2.92 |
2.06 |
0.151 |
|
Period of complaint(months) |
1.1 ± 0.13 |
1.3 ± 0.24 |
0.97 |
0.323 |
|
Diabetic patients n (%) |
8 (7.61) |
4 (5.33) |
0.68 |
0.415 |
|
Hypertensive patients n (%) |
21 (20.0) |
14 (18.66) |
0.13 |
0.729 |
|
Previous surgeries n (%) |
6 (5.71) |
4 (5.33) |
0.023 |
0.878 |
In the laparoscopic group, 82 patients (76.19%) were classified as Class I, while 23 were classified as Class II. In contrast, in the OS group, 49 patients in Class I (65.33%) and 26 patients in Class II (34.67%) were classified (p < 0.05). The corresponding p-values were 0.0321 and 0.0154, both of which were statistically significant, indicating a genuine distinction between the two surgical techniques in terms of wound classification (Figure 1). The average operative time for the laparoscopic group was 57.19 minutes. In contrast, in OS group had a significantly prolonged average operative time of 85.10 ±15.18 minutes (p < 0.05). Eighteen patients (17.14%) required a drainage system in the laparoscopic and 26 (34.66%) in the OS group (p< 0.05). In the Laparoscopic group, mean blood loss was 120.76 ±13.3 mL and 170.01 ± 17.19 mL in the OS group (p < 0.05). These all parameters significantly highlighted the prospective advantages of laparoscopic surgery over OS (Table2).
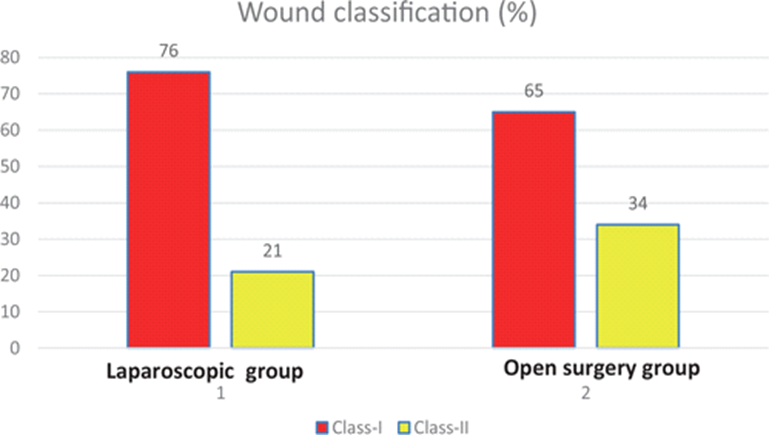
Figure 1
Table 2. Comparative clinical and operative outcomes between laparoscopic and OS groups.
|
Parameter |
Laparoscopic group (n = 105) |
OS group (n = 75) |
χ2 |
p-value |
|
Wound classification (%) |
||||
|
Class-I |
82 (76.19) |
49 (65.33) |
4.65 |
0.0321* |
|
Class-II |
23 (21.90) |
26 (34.67) |
6.02 |
0.0154* |
|
Average operative time (minutes) |
57.19 ± 10.13 |
85.10 ± 15.18 |
17.77 |
0.00001* |
|
Use of drainage system (%) |
18 (17.14) |
26 (34.66) |
9.39 |
0.00021* |
|
Estimated blood loss (mL) |
120.76 ± 13.81 |
170.01 ± 17.19 |
16.06 |
0.00001* |
*Indicated that the value is significant (p < 0.05).
Comparing the postoperative outcomes of laparoscopic (n = 105) and OS (n = 75) cohorts, the laparoscopic cohort had substantially (p < 0.05) shorter average hospital stay (2.1 ± 1.1 days vs. 4.4 ± 2.1 days). In addition, a greater proportion of laparoscopic patients were discharged within 24 h (20.95 vs. 10.66%) (p < 0.05). The use of prophylactic antibiotics was nearly statistically significant in the OS cohort (92% vs. 83.90%) (p < 0.05). Significantly more postoperative complications (p < 0.05) occurred in the group undergoing OS (50.66 vs. 25.71%). This study indicated that laparoscopic surgery has advantages in terms of shorter hospital stays and fewer complications, whereas the use of prophylactic antibiotics is more prevalent in OS (Table 3).
Table 3. Comparative clinical outcomes and treatment measures.
|
Parameter |
Laparoscopic group (n = 105) |
OS group (n = 75) |
χ2 |
p-value |
|
Average length of stay (days) |
2.1 ± 1.1 |
4.4 ± 2.1 |
25.25 |
0.00001* |
|
Discharged in <24 h (%) |
22 (20.95) |
8 (10.66) |
4.53 |
0.0031* |
|
Stayed >7 days (%) |
3 (2.85) |
5 (6.66) |
2.89 |
0.0976* |
|
Use of prophylactic antibiotics (%) |
88 (83.90) |
69 (92.0) |
3.76 |
0.0512* |
|
Complications (%) |
27 (25.71) |
38 (50.66) |
13.14 |
0.00001* |
* Indicated that the value is significant (p < 0.05).
On the 14th day after surgery, the Wound Asepsis Score showed a modest difference, with the laparoscopic group bearing mean score of 8.8 ± 3.1 and the OS group with a mean score of 9.0 ± 5.9 (p > 0.05). SSIs were observed in 5 patients (4.76%) in the laparoscopic group and 7 patients (9.33%) in the OS group within 30 days after surgery (p < 0.05). Patients in the laparoscopic group resumed their normal activities on average 6.40 ± 2.09 days after surgery (p < 0.05). On the 14th day following surgery, VAS pain scores revealed that the laparoscopic group a had mean score of 1.8 ± 0.23, while the OS group reported a 2.7 ± 1.27, bearing a significant difference in pain perception (p < 0.05). These findings suggested that laparoscopic surgery was associated with faster recovery, reduced pain scores, and Wound Asepsis Scores than OS (Table 4).
Table 4. Comparative analysis of postoperative outcomes between laparoscopic and OS procedures.
|
Outcome measure |
Laparoscopic group (n = 105) |
OS group (n = 75) |
χ2 |
p-value |
|
Wound asepsis score on 14th day (mean ± SD) |
8.8 ± 3.1 |
9.4 ± 5.9 |
2.80 |
0.165 |
|
Surgical site infections in 30 days (%) |
5 (4.76) |
7 (9.33) |
3.99 |
0.043* |
|
Time to return to activities (mean days ± SD) |
6.4 ± 2.09 |
13.10 ± 5.44 |
18.44 |
0.00001* |
|
VAS pain score on 14th day (mean ± SD) |
1.8 ± 0.23 |
2.7 ± 1.21 |
21.19 |
0.00001* |
* Indicated that the value is significant (p < 0.05).
Comparing the surgical indications of the laparoscopic (n = 105) and OS (n = 75) groups, appendicitis was the rationale for surgery for 39 patients in the laparoscopic group (37.14%) and 33 patients in the OS group (44.0%) (p > 0.05). Gallstones were the most prevalent reason for surgery in the laparoscopic group, with 45 patients (42.8%) versus 21 patients (28.0%) in the OS group (p < 0.05). 13 (12.38%) and 15 patients (20%) underwent surgery for hernias, respectively (p > 0.05). Other indications for surgery were present in 8 patients (7.61%) in the laparoscopic group and 6 patients (8.0%) in the OS group (p > 0.05). While gallstones were substantially more common indications for laparoscopic surgery (p < 0.05), appendicitis, hernia, and other conditions showed non-statistically significant differences between the two surgical approaches (Figure 2).
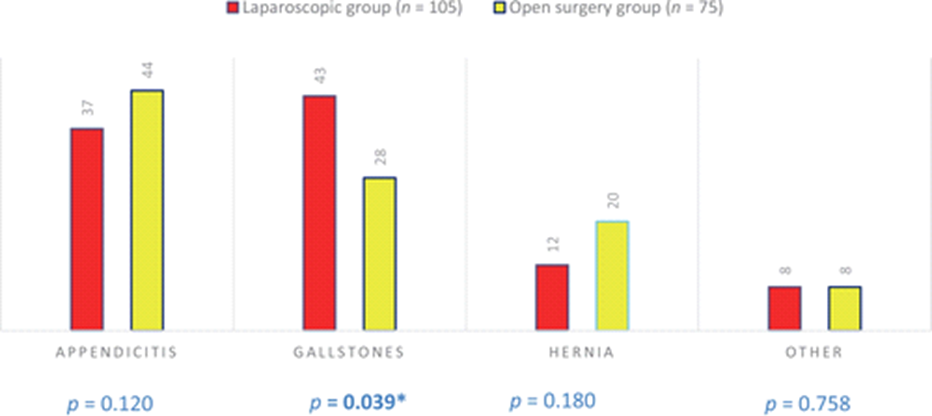
Figure 2
Comparing postoperative complications, wound infection rates were comparable: 10.47% for laparoscopic and 13.33% for OS (p > 0.05). The incidence of haemorrhage was significantly higher in OS group (6.66%) than laparoscopic (1.90%) (p < 0.05). The incidence of organ damage was low and comparable across the groups (p > 0.05). However, the OS group exhibited a substantially higher rate of other complications at 9.33% (p < 0.05) compared to 2.85% in the laparoscopic group. Both cardiovascular and pulmonary complications were comparable between the two groups. However, postoperative abscess formation was considerably higher in the OS group than in the laparoscopic group (p < 0.05). Re-intervention and mortality rates were comparable between both groups (Table 5). The attendance of patients revealed that 94.28% of the laparoscopic and 94.66% of the OS group attended their initial follow-up, with no statistically significant difference (p > 0.05). 17.33% of patients in the OS group compared to 9.52% in laparoscopic required more than three follow-ups (p < 0.05). As for those who did not attend any follow-up, the rates were similar for both groups: 1.90 percent for laparoscopic and 1.33 percent for OS (p > 0.05). While initial follow-up attendance was comparable between groups, patients in OS the group were more likely to require multiple follow-ups than laparoscopic group (Figure 3).
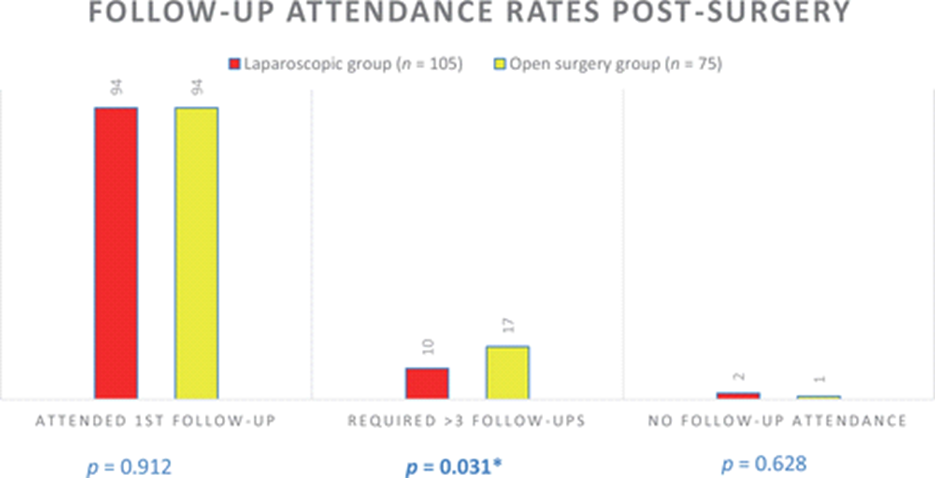
Figure 3
Upon comparing postoperative complications between the study groups, the following trends were discovered: There was no statistically significant difference between the incidence of seroma formation between these groups (p > 0.05). Similar rates of incisional hernia were observed in both groups (0.95% for laparoscopic and 1.30% for OS) (p > 0.05). Deep vein thrombosis was reported in 1.90 percent of patients in the laparoscopic group and in 5.33 percent of patients in OS group (p > 0.05). In short, the incidences of seroma formation, incisional hernia, and deep vein thrombosis were comparable between the two surgical techniques (Figure 4).
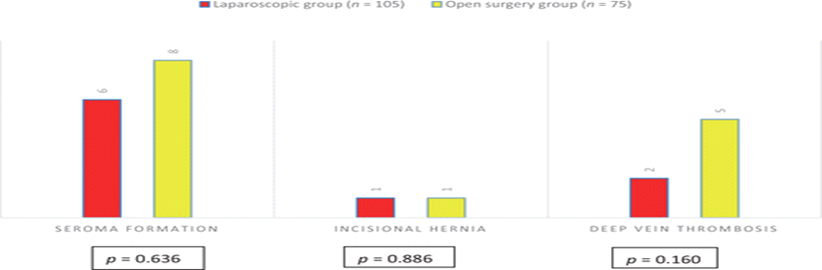
Figure 4
Table 5. Comparative analysis of complications and management.
|
Complication |
Laparoscopic group (n = 105) |
OS group (n = 75) |
χ2 |
p-value |
|
Wound infection (%) |
11 (10.47) |
10 (13.33) |
0.72 |
0.413 |
|
Bleeding (%) |
2 (1.90) |
5 (6.66) |
4.87 |
0.032* |
|
Organ injury (%) |
1 (0.95) |
1 (1.33) |
0.10 |
0.771 |
|
Superficial incisional SSI |
3 (2.85) |
4 (5.33) |
1.67 |
0.232 |
|
Deep incisional SSI |
2 (1.90) |
4 (5.33) |
2.87 |
0.091 |
|
Organ or space SSI |
2 (1.90) |
3 (4.00) |
1.28 |
0.289 |
|
Other complications (%) |
3 (2.85) |
7 (9.33) |
5.67 |
0.029* |
|
Pulmonary complications |
2 (1.90) |
3 (4.00) |
1.38 |
0.292 |
|
Cardiovascular complications |
1 (0.95) |
2 (2.66) |
0.92 |
0.398 |
|
Re- hospitalization |
6 (5.71) |
8 (10.66) |
3.72 |
0.076 |
|
Postoperative abscess |
7 (6.66) |
10 (13.33) |
4.10 |
0.045* |
|
Re- intervention |
1 (0.95) |
2 (2.66) |
0.78 |
0.390 |
* Indicated that the value is significant (p < 0.05).
Patients from both groups were evaluated on days 1, 3, and 7 using VAS to measure postoperative pain. On the first postoperative day, patients in laparoscopic group reported a substantially lower mean VAS score than patients in OS group (p < 0.05). On day 3, laparoscopic group reported mean pain score of 1.80 ± 0.68, which was still lower than 2.98 ± 0.95 observed in OS group (p < 0.05). Laparoscopic group's mean VAS score on seventh day was 1.10 ± 0.56 that was consistently lower than OS group's mean VAS score of 2.14 ± 0.77 (p < 0.05). Overall, the laparoscopic group consistently reported lower pain scores than OS group on all evaluated postoperative days (Table 6).
Table 6. Postoperative pain scores on Day 1, 3, and 7.
|
Day & Score (VAS) |
Laparoscopic group (n = 105) |
OS group (n = 75) |
χ2 |
p-value |
|
Day 1 (mean ± SD) |
5.35 ± 1.10 |
6.87 ± 1.90 |
12.76 |
0.00001* |
|
Day 3 (mean ± SD) |
1.80 ± 0.68 |
2.98 ± 0.91 |
10.60 |
0.00001* |
|
Day 7 (mean ± SD) |
1.10 ± 0.56 |
2.14 ± 0.77 |
8.34 |
0.0041* |
* Indicated that the value is significant (p < 0.05).
4. DISCUSSION:
This study compared the wound infection rates and postoperative recovery outcomes between two surgical modalities. Our research highlighted several vital findings. First, despite comparable demographic profiles, there were statistically significant differences in gender distribution between the two groups. Importantly, our research revealed the prospective benefits of laparoscopic surgery in a few parameters. The classification of wounds revealed a substantial difference in the severity of wounds between the two techniques, with OS resulting in a greater proportion of Class-II wounds. In addition, operative periods for laparoscopic procedures were significantly reduced, confirming that laparoscopic procedures may be less time-consuming and potentially less invasive. The decreased operative time in the laparoscopic group can be attributed to the technological advancements of laparoscopy, which allow for a more streamlined procedure, less tissue manipulation, and smaller incisions. In addition, postoperative outcomes favoured laparoscopic surgery, with patients requiring shorter hospital stays and experiencing fewer complications. These results were consistent with the existing literature, which demonstrated that the reduced invasiveness of laparoscopic procedures results in less postoperative discomfort and a quicker recovery. Comparison to open hepatectomy (OH), laparoscopic hepatectomy (LH) has lower rates of overall and significant complications, postoperative mortality, and improved 1- year, 2-year, and 5-year overall survival rates. LH was also associated with secondary outcomes such as diminished blood loss, shorter hospital stays, and fewer complications such as liver failure and ascites. However, operation duration and transfusion rates did not differ substantially between groups but in minor liver resections, LH demonstrated favourable outcomes. Similar research examined 14 retrospective cohorts containing 1767 patients. The two surgical approaches showed no significant variance in immediate postoperative complications. In contrast, laparoscopic excision patients demonstrated significant improvements in long-term and total postoperative complications, intraoperative blood loss, transfusion requirements, time to initial feeding, and hospital stay duration. Laparoscopic cyst excision and Roux-en-Y hepaticojejunostomy demonstrated equivalent or superior intraoperative and postoperative outcomes than open excision for children with Choledochal cysts. While the Wound Asepsis Scores on the fourteenth day after surgery were comparable between the two groups, the reduced rates of SSIs and the quicker return to daily activities among laparoscopic patients highlighted the prospective advantages of this modality. This may be a result of the smaller incision diameters and reduced tissue manipulation associated with laparoscopic techniques, resulting in faster wound healing and decreased infection risk. Gallstones emerged as the most frequent indication for laparoscopic surgery. While some parameters, such as wound infection rates, were comparable between the two groups in terms of postoperative complications, there were significant differences in others. The higher incidence of postoperative bleeding and abscess formation in the OS group may be indicative of the technique's increased invasiveness. Nevertheless, certain complications like seroma formation, incisional hernia, and deep vein thrombosis remained consistent between both groups, highlighting that some risks were inherent to the surgical procedure itself, regardless of the technique employed. In a similar study published in Nature, laparoscopic cholecystectomy was compared to conventional laparoscopic cholecystectomy (CLC). It was concluded that single-incision laparoscopic cholecystectomy emerged as a viable and complication-free alternative to CLC for benign gallbladder surgery, particularly in younger female patients who have not undergone abdominal surgery previously. The consistent reporting of reduced pain scores among laparoscopic patients throughout the evaluated postoperative days was a factor requiring attention. This may be due to the minimally invasive nature of laparoscopy, which resulted in less tissue trauma, smaller incisions, and consequently less discomfort. Laparoscopic appendectomy (LA) performed better than open appendectomy (OA) in terms of reduced pain on the first day, fewer wound infections, shorter hospital stays, and a speedier return to regular activities, despite a slightly higher incidence of intra-abdominal abscesses. Laparoscopic surgery has well- known short-term benefits for surgical patients. In oncological procedures, laparoscopy ensures important technical objectives, such as adequate margin clearances and lymph node retrieval, both of which are essential to cancer outcomes. Although recurrence and survival rates are essentially unaffected by laparoscopy, laparoscopic liver resections may indicate an improvement in overall survival rates. In addition, while this study provided significant insights into the relative advantages of laparoscopic and OS, certain limitations remain. Regional differences in surgical expertise, apparatus, and patient populations can lead to varying outcomes in other areas. The long-term effects and outcomes of both surgical techniques, particularly regarding patient quality of life, should be investigated in greater depth. Such studies would provide a more holistic perspective on the relative benefits and drawbacks of the two surgical modalities. In conclusion, while both laparoscopic and open surgical techniques have their advantages and disadvantages, our findings strongly suggested the potential superiority of laparoscopic procedures in terms of shorter operative times, shorter hospital stays, quicker recovery, and fewer complications. In determining the optimal surgical approach, it is crucial for clinicians to consider these factors, along with patient preferences and specific surgical conditions. However, it is crucial to recognize the retrospective nature of the study, and the inherent biases associated with its design. Future prospective randomized controlled trials are suggested to provide a more conclusive comparison of the two methodologies.
5. CONCLUSION:
In this retrospective cohort study comparing the outcomes of laparoscopic and OS, it was clearly demonstrated that laparoscopic procedures offered statistically significant advantages over traditional open surgeries in terms of shorter operative times, less blood loss, and shorter hospital stays following surgery. The marginally reduced incidence of SSIs was observed in the laparoscopic group. Additionally, the laparoscopic approach was associated with a quicker recovery, reduced postoperative discomfort, and fewer complications. Although surgical indications differed between groups, gallstones were notably more prevalent in the laparoscopic group. The rates of specific postoperative complications such as seroma formation, incisional hernia, and deep vein thrombosis were comparable for both techniques. However, the OS group required a greater number of follow-up visits. In addition to highlighting the significance of patient-specific factors in surgical decision-making, this study highlighted the potential advantages of laparoscopic surgery, advocating its consideration as a preferable option for certain surgical procedures.
REFERENCES
\url{https://link.springer.com/article/10.1007/s00464-012-2436-5}
\url{https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003474.pub3/full}
\textit{The American Journal of Surgery}, \textit{169}(2), 208-212. \url{https://www.ncbi.nlm.nih.gov/pubmed/7847428}
\url{https://www.karger.com/Article/Abstract/97087}
\url{https://academic.oup.com/bjs/article-abstract/81/1/33/276569}
\textit{BMJ}, \textit{337}. \url{https://www.bmj.com/content/337/bmj.a745}
\textit{British Journal of Surgery}, \textit{83}(12), 1630-1633. \url{https://academic.oup.com/bjs/article- abstract/83/12/1630/282216}
\url{https://link.springer.com/article/10.1007/BF00289748}
\textit {7} (1), 1-13. \url{https://bmcsurg.biomedcentral.com/articles/10.1186/1471-2482-7-11}
\url{https://link.springer.com/article/10.1007/s00464-012-2436-5}
\url{https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003474.pub3/full}
\textit{The American Journal of Surgery}, \textit{169}(2), 208-212. \url{https://www.ncbi.nlm.nih.gov/pubmed/7847428}
\url{https://www.karger.com/Article/Abstract/97087}
\url{https://academic.oup.com/bjs/article-abstract/81/1/33/276569}
\textit{BMJ}, \textit{337}. \url{https://www.bmj.com/content/337/bmj.a745}
\textit{British Journal of Surgery}, \textit{83}(12), 1630-1633. \url{https://academic.oup.com/bjs/article- abstract/83/12/1630/282216}
\url{https://link.springer.com/article/10.1007/BF00289748}
\textit {7} (1), 1-13. \url{https://bmcsurg.biomedcentral.com/articles/10.1186/1471-2482-7-11}

Arivazhagan M., Priyadharshini J., Dr. N. Junior Sundresh*, Comparative Analyses on Laparoscopic Surgery Versus Open Surgery in Reducing Surgical Site Infection, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1462-1475 https://doi.org/10.5281/zenodo.17115435
 10.5281/zenodo.17115435
10.5281/zenodo.17115435
