Rashtriya College of Pharmacy, Hatnoor, Kannad, Chh. Sambhajinagar 431103
Cervical cancer ranks as the fourth most frequently diagnosed cancer among worldwide and is responsible for more than 300000 deaths each year. Persistent infection with high risk human papilloma virus (HPV) types is the primary cause, with viral oncoproteins E5, E6 and E7 working alongside host cellular factor to initiate and sustain malignant transformation. Although cervical cancer is largely preventable, early detection greatly improves survival outcome. In high income countries where screening and vaccination programs are well established, the disease has become uncommon. In contrast it remains a major cause of mortality in low and middle income nations, where limited health care resources often lead to late stage and non-treatable presentations. Current management strategies include surgery, radiotherapy, chemotherapy, or combination to this. This review outlines the development and progression and cervical cancer and provides and in depth analysis of the strength and limitations of existing treatments. It also highlights emerging therapeutic approaches1. Such as immunotherapy, targeted treatments, combinations regimens, gene based therapies that hold promise for improving patient outcome.
In 2020, an estimated 10 million cancer related deaths were reported making it on the leading causes were reported making it on of the leading causes of death globally2. Although this number is predicted to increase worldwide,the rise expected to occur predominantly in low and middle income countries [LMICs] as they currently face the greatest challenges in tackling the cancer burden2.
Cervical cancer is the cancer starts in the cells of the cervix. The cervix is the lower, narrow end of the uterus [WOMB]. The cervix connects the uterus to the vagina [birth cannel]3. Cervical cancer usually appears in the cervix, the cells of the cervix go through changes known as dysplasia, in which abnormal removed, the abnormal cells may be cancer cells and starts to a and spread more deeply into the cervix and to surrounding areas4.
Cervical cancer, the second most common malignancy in women worldwide, is almost invariably associated with infection by humam papillomavirus [HPV]. HPV 16 or 18 is commonly present in 70% of cervical cancers5. HPV positive tumor cells present antigen of the viral protein in the context of human leukotocyte antigen [HLA] class I that can be recognized by CTLs5. We have conducted a study in patients with early stage cervical cancer to assess the safety and immunological effects of vaccination with TA-HPV5.
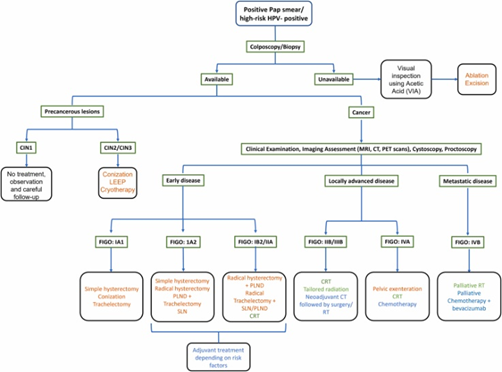
CERVICAL CANCER MANAGEMENT
Provide evidence –based, resource stratified global recommendations to clinicians and policymakers on the management and palliative care of women diagnosed with invasive cervical cancer6.
In the management of cervical cancer depends on the stage of the disease, tumor and caracteristices, and patient factors such as age and fertility wishes. Early detection through screening and HPV vaccination has significantly improved outcomes. According to saslow et al. [2020], timely diagnosis plays a crucial role in preventing progression to advance stages6.
1. Management Of Pre-Invasive Lesions [CIN]
Pre- invasive lesions such as CIN2-CIN3 are typically managed with ablative or excisional procedures7. Techniques like cryotherapy, loop electrosurgical excisions procedure [LEEP], and cold-knife conization are considered effective and fertility-preserving. As noted by wright et al. [2012], these procedure offer high cure rates while minimizing reproductive complication7.
2. Management To Early Stage Cervical Cancer [Stage 1]
Patients with early stage cervical cancer [stage IA-B1] are generally treated with surgery, including radical hysterectomy or fertility-sparing radical trachelectomy8. plante [2015] emphasizes that radical trachelectomy is now preferred for young women desiring fertility prevention, provided strict selection criteria are met8.
3. Management Of Locally Advanced Cervical Cancer [Stage IB2-IVA]
Locally advanced disease is primarily treated with concurrent chemoradiotherapy [CCRT], combining external beam radiotherapy, intracavitary, brachytherapy and weekly cisplatin – based9. According to key et al [1999], cisplatin-based CCRT significantly improves survival compared to radiotherapy alone and remains the gold – standards approach9.
4. Management Of Recurrent Or Metastatic Disease
Foe recurrent or metastic cervical cancer, systemic therapy with platinum combinations, targeted agents, or immunotherapy is recommended10. Tewari et al [2014] demonstrated that adding bevacizumab to chemotherapy improves overall survival is recurrent disease, establishing it as a standard regimen10.
5. Role Of Immunotherapy
Immune checkpoint inhibitors like pembrolizumab have emerged as promising options, especially for promising options, especially for PD-L1-positive tumors11. Chung et al [2019] reported durable responses with pembrolizumab in previously treated recurrent cervical cancer, leading to its regulatory approval11.
6. Palliative Care
Palliative care focuses on symptom relief, pain management, and psychological support, especially in advanced disease12. As highlighted by Ferris et al. [2018], integrating palliative care early improves quality of life and reduces treatment – related distress13.
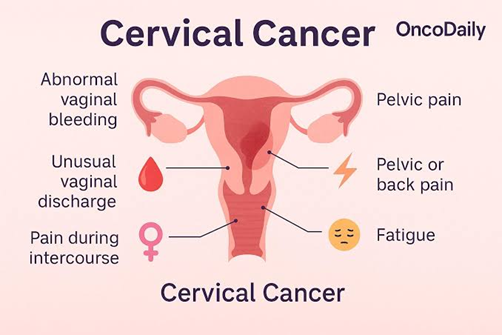
SYMPTOMS OF CURVICAL CANCER
Abnormal vaginal bleeding; This can manifest as bleeding between periods, after sexual intercourse, or post – menopause. Unusual bleeding should be evaluated by a healthcare provider, as it may indicate cervical abnormalities14.
Pelvic Pain: persistent pelvic pain or discomfort during intercourse can be sign of cervical cancer. This pain may also be accompanied by lower back pain or pain radiating to the thighs14.
Unusual Vaginal Discharge: Women with cervical cancer may experience a watery, pink, or foul – smelling discharge. This discharge can be different from the normal vaginal secretions and may increase in volume15.
Swelling Of The Legs: Advanced cervical cancer can lead to lymph node involvement, causing swelling in the legs or other areas of the body due to fluid accumulation16.
Loss Of Appetite And Weight Loss: Unexplained weight loss and a decrease in appetite can occur in advanced stages of cervical cancer, reflecting systemic effects of the disease.
RISK FACTORS FOR CERVICAL CANCER
1. Human papillomavirus [HPV] Infection:
HPV, particularly high risk types such as HPV-16 and HPV-18, is the primary cause of cervical cancer. Persistent infection with high – risk HPV strains can lead to changes in cervical cells and eventually cancer.
2. Weakened Immune System:
Conditions that compromise the immune system, such as HIV/ AIDS or the use of immunosuppressive medications, can increase susceptibility to medications, can increase suspceptibility of HPV infection and cervical cancer.
3. Smoking
Tobacco use is linked to a higher risk of cervical cancer. Chemicals in cigarettes contribute to the development of cancerous cells in the cervix.
4. Long- term Use Of Oral Contraceptives:
Women who used oral contraceptives for five or more years may have a slightly increased risk of cervical cancer. However, this risk decreases after discontinuation of the pill.
5. Family History of Cervical Cancer :
A family history of cervical cancer may increase an individual’s risk, suggesting a possible genetic predisposition.
6. Socioeconomic Factors :
Women from lower socioeconomic backgrounds may have limited access to healthcare services, including screening and vaccination, increasing their risk of cervical
DIAGNOSOSIS
Colposcopy :
Colposcopy is a procedure in which the health care provider inserts a speculum to gently open the vagina and view the cervix. A vinegar solution will be applied to cervix to help show abnormal areas. The health care provider then places an instrument called a colposcope close to the vagina. It has a bright light and a magnifiying lens and allows the health care provider to look and allows the health care provider to look closely at the cervix. A colpposcopy usually includes a biopsy.
BIOSPY:
Biopsy is a procedure in which a sample of tissue is removed from the cervix so that a pathologist can view it under a microscope to check for signs of cancer. The following types of biopsies are used are used to check for cervical cancer:
Punch Biopsy is a procedure in which a small, round piece of tissue is removed using a sharp, hallow circular instrument. Sometimes several different areas of the cervix will be punch biopsy. This procedure is usually done in the doctor’s office.
Endocervical Curettage is a procedure to collect cells or tissue the cervical canal using a curette [spoon – shaped instrument]. This procedure removes only a small amount of tissue and usually done is the doctor’s office.
Loop Electrosurgical Excision Procedure [LEEP] uses a thin wire loop, through which an electrical current is passed, to remove tissue from the cervix. LEEP may be used to diagnose cervical cancer. It also may be used to remove precancer or early-stage cancer. This procedure is typically done in a doctor’s office. it usually takes only a few minutes, and local anesthesia is used to numb the area.
Cone Biopsy is surgery to remove the larger, cone- shaped piece of tissue from the cervix and cervical canal. A cone biopsy may be used to diagnose cervical cancer. it also may be used to removed precancer or early-stage cancer. A cone biopsy is done at the hospital under general anesthesia.
Talk with your care provider to learn what to expect during and after your biopsy procedure. some people have bleeding and / or discharge after a biopsy. others have pain that feels like cramps during menstruation.
IMAGING TESTS
PET-CT SCAN combines the pictures from a positron emission tomography [PET] scan and a computed tomography [CT] scan are done at the same time on the same machine. The pictures from both scans are combined to make or more detailed picture than either test would make by itself.
For the PET scan, a small amount of radioactive glucose [sugar] is injected into vein. The scanner rotates around the scanner rotates around the body and makes a picture of where glucose is beings used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells.
For CT scan, a series of detailed X ray pictures of areas inside the body is taken from different angles. A dye may be injected into a vein or swallowed to help the organs or tissue show up clearly.
Magnetic Resonance imaging [MRI] uses in a magnet, radio waves, and a computer to make a series of detailed picture of areas inside the body. This procedure also called nuclear magnetic resonance imaging.
Ultrasound uses to high energy sound waves [ultrasound], which bounce off internal tissues or organs and make echoes. The echoes from a picture body tissues called as a sonogram.
Chest X ray in this X ray of organs and bones inside the chest. An x ray is a type of high energy radiation then can go through the body and onto film, making a picture areas inside the chest.
LAB TESTES
CBC Complete blood count is the measure blood test that measure in the following in the sample of blood.
The amount of haemoglobin [the protein that carries oxygen] in the red blood cells the portion of the blood sample made up the red blood cells.
Blood chemistry study the blood test that measure to amount of certain substance released into the blood by organ and tissues in the body, including electrolytes, lactate dehydrogenase, uric acid, blood urea nitrogen, creatinine, and liver function values. An unusual [high lower than normal] amount of a substance can be a sign a cancer spread or other disease.
VISUAL EXAMINATION
Cystoscopy is a procedure to look inside the bladder and urethra to check for abnormal areas. A cystoscope is inserted through the urethra into the bladder. A cystoscope is a thin, tube like instrument with a light and a lens for viewing. It may also have a tool to removes tissue sample, which are check under a microscope for sign of cancer.
Sigmoidoscopy uses a sigmoidoscope to like inside the rectum and sigmoid [lower] colon for abnormal areas. A sigmoidoscopy uses a sigmoidoscope to look inside the rectum and sigmoid [lower] colon for abnormal areas. A sigmoidoscopy is inserted through the rectum into the sigmoid colon.
A sigmoidscope is inserted through the rectum into the sigmoid colon.
A sigmoidoscope is a thin, tube like instrument with a light and lens for viewing. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
CURRENT TREATMENT
Treatment for cervical cancer depends on several factors, such as the stages of the cancer, other health conditions you may have and your preference. Surgery, radiation, chemotherapy or a combination of the three may be used.
SURGERY
Small cervical cancers that haven’t grown beyond the cervix are typically treated with surgery. The size of your cancer, its stage and whether you would like to consider becoming pregnant in the further will determine which operation is best for you.
Options might include :
Surgery to cut away the caner only.
For a very small cervical cancer, it might be possible to remove all the cancer with a cone biopsy. This procedure involves cutting away a cone – shaped piece of cervical tissue and leaving the rest of cervix intact. This option may make it possible for you to consider becoming pregnant in the future.
Surgery to remove to the cervix, called a trachelectomy.
A small cervical cancer might be treated with a radical trachelectomy procedure. This procedure removes the cervix and some surrounding tissue. The uterus remains after this procedure, so it may be possible to become pregnant, if you choose.
Surgery to remove the cervix and uterus, called a hysterectomy
Most cervical cancers that have not spread beyond the cervix are treated with a radical hysterectomy operation. This involves removing the cervix, uterus, part of vagina and nearby lymph nodes. A hysterectomy can often cure the cancer and stop it form coming back. But removing the uterus makes it impossible to become pregnant.
Minimally invasive hysterectomy may be an operation for very small cervical cancers that have not spread, known as microinvasive cancers. This procedure involves making several small cuts in the abdomen rather than one large cut. people who have minimally invasive surgery tend to recover faster and spend less time in the hospital. But some research has found that minimally invasive hysterectomy may be less effective than traditional hysterectomy. if you’re considering minimally invasive surgery, discuss the benefits and risks of this approach with your surgeon.
RADIATION THERAPY FOR CERVICAL CANCER
Radiation therapy uses high energy x rays to kill cancer cells. Depending on the stage of the cervical cancer, radiation therapy may be used :
As a part of the main treatment : For some stages of cervical cancer, the preferred treatment is radiation and chemo given together. [called concurrent chemo radiation] as the chemo helps the radiation work better.
To treat cervical cancer that spread or that has come back after treatment : Radiation therapy may be used to lessen symptoms caused by cervical cancers that have spread to other organs and tissues.
Types of radiation therapy
The types of radiation therapy most often used to treat cervical cancer are :
It is important to know that smoking increases the side effect from radiation and can make treatment less effective. if you smoke, you should stop.
External beam radiation
External beam radiation therapy. [EBRT] aims x ray at the cancer from a machine outside the body. Treatment is much like getting a regular x ray, but the radiation dose is stronger.
Each radiation treatment lasts only a few minutes, but getting you into place fir treatment usually takes longer. The procedure itself is painless.
When EBRT is used as the main treatment for cervical cancer, it usually takes longer. The procedure itself is painless.
When EBRT is used as the main treatment for cervical cancer, it is usually combined with chemotherapy. [called concurrent chemo radiation]. Often, a low dose of the chemo drug called cisplatin is used. other chemo drugs can be used as well. The radiation treatments are given 5 days a week for about 5v weeks. Chemotherapy is given at the same time. The schedule is determine by which drug is used. if the cancer has not spread to distant areas, brachytherapy, which is discussed below, may also be given after the concurrent chemo radiation is complete.
Possible side effects of EBRT
Short term side effects of external beam radiation therapy for cervical cancer can include :
Fatigue [tiredness]
When chemotherapy is given with radiation, the blood cell counts tend to be lower, and fatigue and nausea tend to be wore. These side effects typically improve in the weeks after treatment is stopped.
Brachytherapy [internal radiation therapy]
Brachytherapy, or internal radiation therapy, puts a source of radiation in or near the cancer. This type of radiation only travels a short distance. The type of brachytherapy used most often to treat cervical cancer is known as intracavitary brachytherapy. The radiation soure is placed in a device in the vagina [sometimes in the cervix]. Brachytherapy mainly is used in addition to EBRT as a part of the main treatment for cervical cancer. Rarely, it might be used alone in very specific cases of early stage cervical cancers.
There are two types of brachytherapy :
Low dose rate [LDR] brachytherapy is completed over a few days. During this time, the patient stays in bed in a private room in the hospital with instruments holding the radioactive material in place. while the radiation therapy is being given, the hospital staff will care for you, but also take precautions to avoid being exposed to radiation themselves.
High dose rate [HDR] brachytherapy is an outpatient procedure over several treatments [often at least a week a part]. For each treatment, the radio actives material is inserted for a few minutes and then removed. The advantages of HDR treatments is that you do not have to stay in the hospital or stay still for long periods of time.
To treat someone who still has a uterus, the radioactive material can be placed in a small metal tube [called a tandem] that goes in the uterus, along with small round metal holders [avoids] placed near the cervix. This is sometimes called tandem and avoid treatment.
Another option is called tandem and ring. For this a round holder [like a ring] is placed close to the uterus.
The choice of which option to use depends on what type of brachytherapy is planned.
CHEMOTHERAPY
Chemotherapy [also called chemo] uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. Chemotherapy may be given alone or with other types of treatment.
Chemotherapy drugs used to treat cervical cancer include :
Combination of these drugs may be used, other chemotherapy drugs not listed here may also be used.
Learn more about how chemotherapy works against cancer, how it is given, common side effects, and more in chemotherapy to treat cancer.
Chemotherapy plays a major role in the management of cervical cancer, especially in locally advanced, recurrent, and [called concurrent chemo radiation] or as palliative therapy in advanced stages.
Chemotherapy for recurrent / metastatic cervical cancer
1. First – line systemic therapy
Combination regimen [standard] :
2. Alternative Agents
Used when platinum resistance occurs :
TARGETED THERAPY FOR CERVICAL CANCER
Targeted therapy refers to drugs that block specific molecular pathway involved in cervical cancer growth –particularly angiogenesis [VEGF pathway] and immune checkpoint pathways [PD-1/PD-L1]. This agents are mainly used in recurrent, persistent, or metastatic cervical cancer
1. Anti –VEGF Trageted Therapy
Bevacizumab
Key benefits
Common Adverse Effects
IMMUNOTHERAPY [Immune Checkpoint Inhibitors]
Although technically under immunotherapy these are a molecular targeted agents because they target checkpoints proteins [PD-1/PD-L1].
Pembrolizuamb
PALLIATIVE CARE IN CERVICAL CANCER
Palliative care in cervical cancer focuses on relief of symptoms, improving quality of life, psychosocial support, and managing complications in advanced, recurrent, or metastatic disease. It is an essential part of comprehensive cancer care.
Pain management
Pain may arise from tumor infiltration, nerve compression, bone metastasis or treatment effects.
Approach
FURTHER TREATMENT OF CERVICAL CANCER
Therapeutic vaccine: Although prophylactic vaccines enhance humoral immunity, they are of on therapeutic value for patient infected with high risk HPV strains. HPV therapeutic vaccines present an area of active research and are available as live vector based vaccines, peptide and protein based vaccines, nucleic acid based vaccines, and Whole cells vaccines. 35 Most therapeutic vaccines target the HPV E6 and E7 oncoprotiens, Which are expressed in HPV infected cells drive cancer development. The goal is to activate T cells responses against these proteins, thereby eliminating infected cells and preventing cancer progression. Therapeutic vaccines on focus on HPV E5 and E7 oncoprotein in infected cells, aiming to stimulate T cell response to eliminate infected cells and halt cancer progression. MVA – E2, a top performing therapeutic vaccine, demonstrated 90% regression in high grade cervical precancerous lesions treatment.
However, a key limitation of the study was the absence of a control group to assess the natural regression rate of these lesion, 36 efficient treatments are sought for cervical cancer through the development of combination therapy involving immunotherapy drugs and vaccines. An example is the [SA101] vaccine, which showed a 33% response rate in a phase 2 study with nivolumab, a checkpoint inhibitor. However, this response was not seen in advanced cervical cancer patients, emphasizing the necessity for further optimization. Therapeutic vaccination are a significant potential adjuvant therapy to prevent invasive procedures and reduce recurrence, even if their efficacy has not yet reached the level of existing treatments. To enhance results, ongoing research aims to optimize vaccine antigens and combination regimens
PARP INHIBITOR
Poly {Adenosine diphosphate [ADP] ribose} polymerase, especially PARP inhibitor such as olaparib and veliparib prevent this repair, Which is particularly lethal to cells with defective homologous repair, Which is particularly lethal to cells with defective homologous repair, leading to cell death. A case report by Gross M and spencer RJ showed that single agent olaparib therapy demonstrated great promise in terms of response in a patient with recurrent metastatic clear cell cervical cancer. The patient had an excellent response to olaparib without disease progression for 14 months of therapy. A clinical trial evaluating the combination of veliparib with paclitaxel and cisplatin achieved a 34% objective response rate and an overall survival of 14. 5 months. However, further clinical trials are required to fully establish their clinical effectiveness.
Antibody drug conjugate
Tisotumab vedotin is an antibody drug conjugate having an antimicrotular agent and a human tissue factor. The drug attaches to tissue factor, a transmembrane protein present on the cancer cells. subsequently, it moves inside and releases the anti – microtubule agent that disrupts the cells structure, including cell death. Tisotumab vedotin has received FDA approval on September 2021 for treating patients with recurrent or metastatic cervical cancer.
RR Inhibitor
Ribonucleotide reductase [RR] is a crucial enzyme for DNA synthesis, as it catalyses the reduction of nucleoside di or triphospates to corresponding deoxnynucleotides inhibitors like hydroxyurea and triapine are being tested and used for for cervical cancer.
GOG 120 found that treatment with radiation therapy in combination with cisplatin, fluorouracil and hydroxyurea was effective for the treatment of locally advanced cervical cancer. Triapinea more potent RR inhibitor, has shown promise in animal studies and early trials suggest it sensitizes tumours to radiation to radiation, especially in cervical cancer. But further studies are needed to confirm its efficacy for cervical cancer.
Ongoing clinical trails
The ongoing clinical trails in cervical trails in cervical cancer are shaping the future of treatment paradigms with promising new approaches. Trials like INTERLACE and KEYNOTE – A18 are at the forefront, investigating the impact of induction chemotherapy and immune checkpoint inhibitors on treatment outcomes for locally advanced cervical cancer. INTERLACE has demonstrated that induction chemotherapy, while KEYNOTE – 826 and BEATcc are exploring the synergistic effect of combining immune checkpoint inhibitors with chemotherapy and anti-angiogenic agent, revealing enhanced survival. The approval of tisotumb vedotin for second line treatment in recurrent or metastatic cervical cancer marks another significant advancement. This drug, along with pembrolizumab, is being evaluated in numerous trails to determine its efficacy in various treatment settings.
Several specific trails are advancing our understanding of cervical cancer management. The phase 2 XmAb20717 trails is evaluating the efficacy of vudalimab , an investigational agent , in patient with advanced gynaecologic and genitourinary malignancies, including cervical cancer. Another key study is a randomized controlled trail comparing survival outcomes between robotic –assisted laparoscopic surgery and traditional open radical hysterectomy for early stage level cervical cancer, which aims to determine advantages of robotic assistane in surgical interventions.
Additionally, the ACCESS Trail is integrating cervical cancer screening and treatment within existing HIV care programs in nigeria, exploring the effectiveness of various implementation strategies to improve access and outcomes for underserved populations. The ACCESS trails model integrating cervical cancer care within HIV programs could streamline services and enhance access in India, particularly for underserved populations.
This approach could improve cost effectiveness and outcomes for women with both HIV and cervical cancer.
CONCLUSION
In conclusion, cervical cancer poses a significant global health challenge. While current treatment have limitations, emerging therapies like targeted therapies, immunotherapy, and gene therapies offer promising alternatives. Integration of these treatment into standard clinical practice has the potential to improves outcomes for patient. Further research and collaborative efforts are crucial to optimizing treatment regimens and translating promising therapies into effective treatments for cervical cancer.
REFERENCES


Sangram Nagargoje, Twinkal Patil, Comprehensive Review of Current and Further Treatment of Cervical Cancer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3782-3794. https://doi.org/10.5281/zenodo.18069559
 10.5281/zenodo.18069559
10.5281/zenodo.18069559
