Department of Pharmaceutical Quality Assurance, Institute of Pharmacy and Research, Badnera, Amravati, India
Type 2 diabetes mellitus (T2DM) and hypertension frequently coexist due to shared metabolic and pathophysiological mechanisms, including insulin resistance, obesity, and altered sodium handling. This coexistence significantly increases the risk of cardiovascular and renal complications, such as myocardial infarction, stroke, heart failure, and diabetic kidney disease. The combined presence of these disorders produces a synergistic effect, resulting in poorer clinical outcomes compared to either condition alone. Effective management requires an integrated approach involving lifestyle modification and pharmacological therapy. Dietary changes, regular physical activity, weight management, and sodium restriction play a vital role in early intervention; however, most patients require combination drug therapy to achieve optimal glycemic and blood pressure control. Medication non-adherence remains a major challenge due to polypharmacy and complex treatment regimens, especially in elderly populations. Emerging treatment approaches highlight the importance of combination therapy targeting both metabolic and cardiovascular pathways while reducing pill burden. Such strategies offer improved adherence and enhanced clinical outcomes by lowering cardiovascular risk and slowing disease progression.
Diabetes mellitus (DM) is a chronic metabolic disorder characterised by persistently elevated blood glucose levels due to insufficient insulin secretion or insulin resistance. Type 2 diabetes mellitus (T2DM), the most common form, arises from defective insulin secretion by pancreatic β-cells coupled with impaired insulin action in peripheral tissues, leading to hyperglycemia. Molecular mechanisms include disrupted insulin synthesis and secretion, altered cellular metabolism, and systemic inflammation.¹
Hypertension is a multifactorial condition marked by sustained elevation of arterial blood pressure, commonly driven by complex interactions involving immune system activation and vascular dysfunction. Key pathological features include increased sympathetic nervous system activity, renin-angiotensin-aldosterone system (RAAS) overactivation, oxidative stress, and chronic low-grade inflammation. Immune cells such as monocytes and macrophages contribute by releasing pro-inflammatory cytokines and reactive oxygen species, promoting vascular injury and remodelling. Endothelial dysfunction and renal sodium retention further sustain high blood pressure.² The coexistence of T2DM and hypertension results in a compounded risk for cardiovascular and renal complications.
2. Co-existing Type 2 Diabetes Mellitus and Hypertension
In India, hypertension and diabetes mellitus represent two of the most prevalent lifestyle-associated disorders, frequently coexisting due to shared pathophysiological pathways. Together, these conditions serve as major contributors to elevated cardiovascular risk.3
The simultaneous presence of hypertension and diabetes mellitus substantially intensifies the risk profile for both conditions, fostering a higher probability of adverse cardiovascular outcomes. Individuals diagnosed with hypertension face an increased chance of developing diabetes, whereas those with diabetes are notably more susceptible to hypertension. Epidemiological data indicate that a significant proportion of hypertensive patients also experience comorbid diabetes, and the majority of individuals living with diabetes may ultimately develop hypertension as the disease progresses.4 The occurrence of hypertension among diabetic individuals varies depending on multiple factors such as the type and length of the diabetic condition, demographic characteristics including age, gender, and body mass index, as well as clinical parameters like the level of glycemic control. Research indicates that advanced age, female sex, prolonged duration of diabetes, inadequate glycemic management, and higher body mass index are all linked to an increased risk of hypertension in patients with diabetes.5
The coexistence of Type 2 diabetes mellitus (T2DM) and hypertension results in an increased risk that surpasses the impact of either condition alone. Insulin resistance and obesity linked with T2DM contribute to the development of hypertension. This combination leads to a higher frequency of serious complications, including heart attacks, strokes, diabetic kidney disease, and other vascular issues. Addressing hypertension in patients with T2DM is complex due to challenges in diagnosis, setting treatment targets, and choosing appropriate medications. Effective management of individuals affected by both conditions is essential to decrease the rates of illness and death associated with these diseases .6
Insulin resistance plays a central role in the development of hypertension among patients with type 2 diabetes mellitus. Elevated insulin levels in these patients promote sodium retention in the kidneys, which, combined with increased glucose reabsorption, causes fluid buildup and raises blood pressure. Moreover, diabetes-related metabolic changes, including increased hepatic lipase activity, contribute to lipid imbalances such as high very-low-density lipoprotein (VLDL), low high-density lipoprotein (HDL), high triglycerides, and the formation of small, dense low-density lipoprotein (LDL) particles. These lipid abnormalities further drive the progression of hypertension in this population .4
2.1 Diabetes and Blood Pressure Regulation : (7-13)
DIABETES:
In T2DM, the amount of glucose in the blood is high
↓
When plasma glucose is more than 180 mg / daily, the kidneys filter excess glucose into urine
↓
Normal conditions: proximal tubule (S1 segment) has SGLT2 transporters that reabsorb 90% of glucose and sodium along with glucose (co-transport)
↓
This means more glucose filtered, more sodium reabsorbed with it
↓
Normally, the macula densa senesces sodium delivery as in T2DM, extra Na+ is reabsorbed, and less Na+ reaches the macula densa
↓
Macula densa interprets this as low perfusion
↓
Activates RAAS (renin angiotensin aldosterone system)
↓
Release angiotensin I from the liver
↓
Angiotensin converting enzyme (ACE), mainly present in the lungs, converts angiotensin I to angiotensin II,
↓
leading to vasoconstriction (Hypertension)
HYPERTENSION:
Chronic Hypertension
↓
Blood Vessel Damage + Hormonal Activation + Inflammation
↓
Endothelial Dysfunction + Oxidative Stress
↓
Insulin Resistance Develops
↓
Pancreas Compensates by Producing Extra Insulin (Hyperinsulinemia)
↓
Beta-Cell Exhaustion and Dysfunction
↓
Glucose cannot Be Controlled Normally
↓
Persistent Hyperglycemia
↓
Type 2 Diabetes
TABLE NO.1: Hypertension's Biological Effects Leading to Type 2 Diabetes Development
|
Hypertension effect |
Biological Change |
Result |
Outcome → Diabetes |
|
Blood vessel damage |
↓ Nitric oxide |
Poor insulin action |
Insulin resistance |
|
Chronic inflammation |
↑ TNF-α, IL-6 |
Insulin receptor damage |
Prediabetes → Diabetes |
|
Overactive RAAS |
↑ Angiotensin II |
Oxidative stress, belly fat |
Obesity + IR → Diabetes |
|
Stress hormones |
↑ Cortisol |
Liver releases more glucose |
Persistent hyperglycemia |
|
Reduced pancreatic blood flow |
Beta-cell damage |
↓ Insulin release |
Diabetes |
|
Some BP medicines |
Alter metabolism |
Mild sugar rise |
Higher diabetes risk |
|
Shared risk factors |
Obesity, inactivity |
Both worsen each other |
Metabolic syndrome |
TABLE NO.2: Shared risk factors in Hypertension and T2DM
|
Shared Risk Factor |
Effect on Hypertension |
Effect on Diabetes |
|
Obesity |
Increases BP, stiff arteries |
Insulin resistance |
|
Sedentary lifestyle |
Low heart fitness |
Low insulin sensitivity |
|
Unhealthy diet |
More fluid retention, ↑ BP |
High sugar → diabetes |
|
Genetics |
Family tendency |
Genetic insulin issues |
|
Stress |
↑ Cortisol → ↑ BP |
↑ Blood glucose |
|
Smoking |
Vessel damage → ↑ BP |
Insulin resistance |
|
Alcohol |
Fluid retention → ↑ BP |
Fat gain → diabetes |
|
Dyslipidemia |
Vessel damage |
Beta-cell stress |
|
Aging |
Stiff arteries |
Reduced insulin function |
3. Management of Co-existent Type 2 Diabetes Mellitus and Hypertension
In individuals with type 2 diabetes mellitus and hypertension, adopting lifestyle modifications is fundamental in early disease management. A diet abundant in fiber and potassium, while low in saturated fats, refined sugars, and sodium, can effectively lower blood pressure. Coupled with weight reduction and consistent physical activity, these changes simultaneously address both conditions, enhancing overall health outcomes. 5
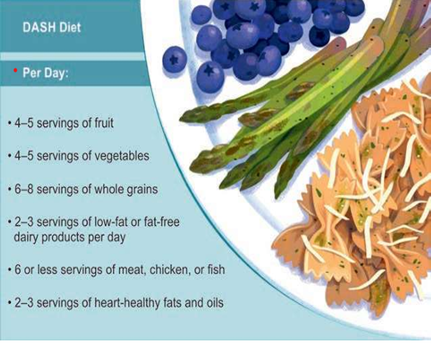
Figure No. 1: Dietary approaches to stop hypertension.

Figure No. 2: yoga as an effective lifestyle Adjunct in hypertension management for diabetic patients
TABLE NO.3: Global guideline for Hypertension management in patients with T2DM
|
Sr. no |
Society |
Year |
Target BP (mm Hg) |
|
1. |
ESC/ESH15 |
2013 |
<140/85 |
|
2. |
ADA16 |
2014 |
<140/80 |
|
3. |
American Society of Hypertension/ International Society of Hypertension17 |
2014 |
<140/90 |
|
4. |
Eighth Joint National Committee (i.e., JNC 8)18 |
2014 |
<140/90 |
|
5. |
ACC/AHA19 |
2017 |
<130/80 |
|
6. |
ESC/ESH20 |
2018 |
<140/90. If treatment well tolerated, then <130/80 |
|
7. |
ADA21 |
2020 |
<140/90, <130/80 for high-risk Individuals |
|
8. |
International Society of Hypertension22 |
2020 |
<130/80 |
|
9. |
ESH/ESC Guidelines23 |
2023 |
<130/80 |
|
10. |
ADA24 |
2024 |
<130/80 |
In cases where patients exhibit mildly elevated blood pressure without significant comorbidities, lifestyle modifications may be pursued for a period of up to three months before starting medication, provided blood pressure remains uncontrolled. Nevertheless, the majority of individuals affected by both hypertension and type 2 diabetes will eventually require pharmacological treatment to achieve blood pressure goals and reduce the risk of cardiovascular and microvascular complications. 14 Younger individuals generally tolerate more aggressive blood pressure reduction and gain greater long-term benefits in lowering the risks of cardiovascular, kidney, and retinal complications. In contrast, older or frail patients require careful consideration of potential side effects, such as low blood pressure or kidney dysfunction, which must be balanced against the advantages of treatment.5
Many patients with type 2 diabetes mellitus and hypertension require multiple medications to control their conditions, which often leads to challenges in treatment adherence. Contributing factors include the complexity of drug regimens, the high number of daily pills, medication costs, and the necessity for lifelong therapy. The issue of polypharmacy, commonly defined as the use of five or more medications, is particularly concerning among elderly patients, who may also be prescribed drugs that overlap in function or have questionable necessity. These factors combine to increase the risk of non-compliance, which can negatively impact treatment outcomes and increase the likelihood of complications. 25 One promising strategy to improve adherence is the development of fixed-dose combinations (FDCs) that contain both antihypertensive and antidiabetic agents. Such combination pills simplify regimens, reduce the number of tablets, and may lower overall cost. FDC of antihypertensive and antidiabetic agent will be revolutionary in the treatment of coexistent TTDM and hypertension as it will be a cheaper alternative to current therapy.4
Sodium–glucose cotransporter-2 (SGLT2) inhibitors represent a noteworthy class of medications for patients with type 2 diabetes mellitus and hypertension. Beyond their primary role in improving glycemic control, these drugs induce osmotic diuresis, which promotes the excretion of sodium and water, leading to a reduction in blood pressure. Clinical studies have demonstrated that SGLT2 inhibitors not only decrease the incidence of cardiovascular events but also slow the progression of kidney disease, lower mortality rates, and reduce hospitalizations due to heart failure. Their benefits extend to both diabetic and nondiabetic individuals, highlighting their expanding role in cardiovascular and renal protection. The mechanisms behind their blood pressure-lowering effects include plasma volume reduction, natriuresis, improved arterial stiffness, better endothelial function,and decreased inflammation. These multifaceted effects contribute to the robust therapeutic profile of SGLT2 inhibitors in managing cardiovascular and renal risks associated with diabetes and hypertension 5
3.1 Recent Studies on SGLT2 Inhibitors for Type 2 Diabetes and High Blood Pressure :
Recent studies have shown that medications called sodium-glucose co-transporter 2 inhibitors, like dapagliflozin, help lower blood pressure in people who have both type 2 diabetes and high blood pressure. A large analysis in 2025 combined results from 43 clinical trials and over 20,000 patients. It found that dapagliflozin reduces the top blood pressure number (systolic) by about 3 points and the bottom number (diastolic) by about 1 point compared to placebo. These changes may seem small but can significantly reduce the chance of serious heart problems by 17 % and lower the risk of hospital visits due to heart failure by 26 %. Importantly, these benefits happen even if patients are already taking other common blood pressure medicines that work on certain hormone systems in the body.
Additional information from large heart failure studies shows that dapagliflozin reduces deaths caused by heart-related problems by 25 % and overall deaths by 17%, no matter whether the patient has diabetes or not. In Indian patients, who often have different health profiles, this medicine showed even better effects in protecting the kidneys, reducing worsening kidney function by almost one-third. These findings support using sodium-glucose co-transporter 2 inhibitors as treatment that not only helps control blood sugar but also protects the heart and kidneys. This makes these medicines very important in managing type 2 diabetes along with high blood pressure.(26,27,28)
3.2 Combination of Dapagliflozin and Bisoprolol:
The combination of Dapagliflozin and Bisoprolol brings together two pharmacologically distinct agents that are effective in managing type 2 diabetes mellitus, hypertension, and elevated cardiovascular risk. This dual therapy is particularly valuable for patients suffering from heart failure with reduced ejection fraction (HFrEF), a condition characterized by impaired heart pumping ability, where the left ventricular ejection fraction is 40% or less. Evidence from clinical trials, including the DAPA-HF study, indicates that Dapagliflozin significantly lowers the risk of heart failure worsening and cardiovascular death when added to standard care, regardless of background therapy such as beta-blockers like Bisoprolol. Bisoprolol, a beta-blocker, lowers heart rate and decreases cardiac workload, further improving outcomes in HFrEF. Together, these drugs offer complementary benefits, improving heart function, controlling blood sugar, reducing hospitalization rates, and lowering cardiovascular mortality in patients with HFrEF. 29
Dapagliflozin, a sodium-glucose cotransporter-2 (SGLT2) inhibitor, functions by lowering blood glucose levels through increased urinary glucose excretion. Additionally, it reduces the reabsorption of sodium, promoting the elimination of excess sodium and water, which decreases cardiac workload and lowers blood pressure. Bisoprolol, a cardioselective beta-1 blocker, decreases heart rate and myocardial contractility, thereby reducing oxygen demand and blood pressure. The combined use of these two agents yields a synergistic effect, enhancing cardiovascular protection by improving heart function, reducing blood pressure, and providing glycemic control. This combination is particularly beneficial for patients managing hypertension, type 2 diabetes mellitus, and elevated cardiovascular risk. 30
The combination of Dapagliflozin and Bisoprolol has undergone extensive clinical evaluation, with key trials demonstrating its efficacy and safety in managing type 2 diabetes mellitus, hypertension, and heart failure with reduced ejection fraction (HFrEF). Regulatory approval for this fixed-dose combination was granted in India by the Central Drugs Standard Control Organization (CDSCO) , Following approval, the combination became available in the Indian market under various brand names given below :
3.3 Combination of Dapagliflozin and Metoprolol:
Dapagliflozin combined with metoprolol offers a comprehensive strategy for managing heart failure, especially after acute myocardial infarction. Dapagliflozin helps reduce fluid overload and cardiovascular risks by promoting sodium and water excretion, improving myocardial metabolism, and lowering blood pressure. Metoprolol, a selective β1-blocker, decreases heart rate and myocardial oxygen demand, mitigates inflammatory responses, and improves myocardial perfusion. Clinical evidence shows that their combined use significantly enhances cardiac function, reduces oxidative stress and inflammatory markers, and improves overall prognosis without increasing adverse effects. This combination has been shown to reduce the incidence of cardiovascular events such as heart failure, ventricular fibrillation, and death three months after intervention. These synergistic effects make the Dapagliflozin and Metoprolol combination a valuable option in heart failure management 31The combination of Dapagliflozin and Metoprolol has successfully undergone clinical trials, demonstrating significant improvements in cardiac function and reduction in cardiovascular events, especially for patients post-acute myocardial infarction and with heart failure. Regulatory approval for this combination has been granted, and it is now marketed in India under various brand names such,
TABLE NO.4: Fixed dose combinations approved by DCG(I)
|
Sr. no. |
FDC |
Indication |
Approval Date |
|
1. |
Metoprolol Succinate IP 47.50mg eq. to Metoprolol Tartrate 50mg (as sustained release) + Dapagliflozin Propanediol Monohydrate eq. to Dapagliflozin 10mg film-coated bilayered tablets. |
Indication in patients with heart failure post-acute myocardial infraction |
10.07.2024 |
|
2. |
Dapagliflozin Propanediol Monohydrate eq. to Dapagliflozin + Bisoprolol Fumarate IP (10mg + 5mg & 10mg +10mg) film coated tablet. |
Indicated in patients with Heart Failure with Reduced Ejection Fraction (HFrEF) |
16.08.2024 |
4. Cost-Effectiveness of Fixed-Dose Combinations in Type 2 Diabetes and Hypertension Management in India:
Fixed-dose combinations that integrate medications for both diabetes and hypertension represent an important advancement for patient care, especially in low- and middle-income countries like India. Recent health economic studies highlight that these combination therapies significantly reduce monthly treatment costs compared to the use of multiple individual pills. For instance, combination therapies generally cost between ?250 and ?350 per month, whereas taking separate drugs for diabetes and hypertension may cost nearly double, up to ?600. This cost saving has meaningful implications for patient adherence and long-term health outcomes, as lower expenses improve patients ability to consistently obtain their medications.(32,33)
TABLE NO.5: Cost and Adherence Comparison of Therapies
|
Therapy type |
Mostly cost (Rs) |
Daily pill count |
Estimated adherence (%) |
|
FDC |
250-350 |
1 |
85 % |
|
Separate pill |
450-600 |
3-4 |
55% |
5. Combinations available in the clinical trials:
Dapagliflozin and Telmisartan -
The study was designed to evaluate the safety and pharmacokinetic interaction between THP-00101 and THP-00102 in healthy adult volunteers.
Conditions: Hypertension, Diabetes Mellitus, Type 2
Other Study ID Numbers: THP-001-001
Primary Purpose: Treatment
Allocation: Randomised
Intervention / Treatment :
Drug: THP-00101 (Dapagliflozin) 10mg
Drug: THP-00102 (Telmisartan) 80mg34
Lisinopril + Metformin -
NCT03853659 — Evaluating efficacy and safety in patients with hypertension and type 2 diabetes
Outcome: Significant improvement in both blood pressure control and glycemic parameters was observed compared to monotherapy arms. The combination was generally well-tolerated with no serious adverse effects linked to the drug combination.35
Losartan + Glimepiride -
NCT02339972 — Assessing blood pressure control and glycemic control in diabetic hypertensives
Outcomes: Indicated better systolic and diastolic blood pressure reduction with concurrent glimepiride use versus hypertensive control alone. Glycemic control was improved without increased hypoglycemia incidents36
Amlodipine + Metformin -
NCT03180919 — Studying impact on cardiovascular outcomes in type 2 diabetes with hypertension
Outcomes: The combination showed synergistic cardiovascular benefit by lowering blood pressure and improving insulin sensitivity. It was associated with reduced inflammation markers versus metformin alone.37
Ramipril + Sitagliptin -
NCT02632008 — Effects on renal function and blood pressure in diabetic hypertensive patients
Outcomes: Results demonstrated improved renal function parameters and decreased albuminuria alongside blood pressure lowering. The combination was safe and efficacious in type 2 diabetic hypertensive patients.38
Olmesartan + Pioglitazone -
NCT01454552 — Evaluating cardiovascular risk markers and blood glucose control
Outcomes: This combination reduced insulin resistance and improved endothelial function. Cardiometabolic outcomes favored combination therapy, showing better arterial compliance and glucose control.39
Valsartan + Glipizide -
NCT02097727 — Trial on blood pressure and glycemic efficacy and safety profiles
Outcomes: patients had improved blood pressure and fasting glucose levels, with a low incidence of adverse effects. The fixed-dose approach increased patient adherence in diabetic hypertensive populations.40
6. Emerging Therapies for Combined Diabetes and Hypertension Management
New combination pills that mix diabetes medicines with three blood pressure drugs are showing excellent results in large trials. Early results from studies with over 12,000 patients suggest these quadruple combinations could cut heart attack and stroke risk by 45%. Another exciting development combines a new kidney-protecting drug, with dapagliflozin. The DIAMOND study with 6,400 patients found this combination reduces protein leakage in urine by 22 % and slows kidney damage by 18% , which is very important for Indian patients who often develop kidney problems early. Artificial intelligence-driven personalized dosing algorithms for fixed-dose combinations are expected by 2027, potentially improving adherence by 28% through smartphone-based monitoring.(41-44)
TABLE NO.6: Upcoming Treatment Innovations (2026-2029)
|
Treatment Type |
Current Stage |
Main Benefit |
Expected Year |
|
4- Drug Combo Pill |
Large human trials |
45% fewer heart problems |
2027 |
|
Finerenone = DAPA |
Large human trials |
22 % less kidney damage |
2026 |
|
AI Smart Apps |
Testing phase |
28% better medicine testing |
2028 |
|
Wearable Monitors |
In Development |
Personalized dosing |
2029 |
CONCLUSION:
The coexistence of type 2 diabetes mellitus and hypertension represents a major global health challenge due to their intertwined pathophysiology and synergistic impact on cardiovascular and renal outcomes. Insulin resistance, obesity, and endothelial dysfunction promote the onset and progression of both conditions, leading to heightened morbidity and mortality. Integrated management combining lifestyle modification, patient education, and pharmacological interventions remains essential. Advanced therapeutic approaches, including the use of SGLT2 inhibitors and fixed-dose combinations of antihypertensive and antidiabetic agents, show promise in improving adherence and reducing cardiovascular burden. Emphasizing individualized therapy, early intervention, and comprehensive cardiovascular risk reduction can markedly improve clinical outcomes and quality of life for patients affected by these dual cardiometabolic disorders.
ACKNOWLEDGMENT:
I express my sincere gratitude to Prof. (Dr.) S. J. Dighade, Principal, for his invaluable guidance and continuous support throughout the preparation of this review. Special thanks to Ms. Apurva U. Deshmukh mam for her encouragement and assistance. This review did not receive any specific funding.
REFERENCES

Akanksha Gharad, Dr. S. J. Dighade, Apurva Deshmukh, Dual Cardiometabolic Disorders: An Overview of Co-existing Type 2 Diabetes Mellitus and Hypertension, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 1332-1344. https://doi.org/10.5281/zenodo.19475850
 10.5281/zenodo.19475850
10.5281/zenodo.19475850
