Ashokrao Mane College of pharmacy, Peth-Vadgaon, Shivaji University 416112, Maharashtra, India.
Gene therapy has emerged as a promising approach for the treatment of rare and monogenic diseases by directly correcting or modulating genetic defects. Advances in viral and non-viral delivery systems, genome-editing technologies, and in vivo and ex vivo therapeutic strategies have significantly improved the safety and effectiveness of gene-based treatments. This review summarizes the historical development of gene therapy, key therapeutic strategies, and recent clinical applications in rare diseases, including blood, neuromuscular, neurological, and ocular disorders. Despite encouraging clinical outcomes, challenges such as immune responses, high manufacturing costs, and regulatory complexities continue to limit widespread adoption. Ongoing technological innovation and regulatory harmonization are essential to translate gene therapy into an accessible and sustainable therapeutic option.
Since its inception, gene therapy—a groundbreaking strategy treating human diseases—has seen advancements [1].
This study seeks to fill this gap by evaluating researcher's perspectives on the potential use of genetic therapies in treating rare genetic disorders[2].
Rare diseases represent a diverse collection of disorders, with nearly 7,000 conditions currently recognized[3]. Although each individual disease affects a relatively small number of people, their combined global burden is substantial, involving approximately 300 million individuals. In China, the patient population is estimated at about 20 million, with over 200,000 newly diagnosed cases each year [4]. Approximately 80% of rare diseases arise from inherited genetic abnormalities, and a similar proportion of patients show clinical symptoms early in life[5]. The scarcity of effective therapeutic options has intensified the demand for innovative treatment approaches, positioning rare diseases as one of the most pressing challenges in modern medicine[6].
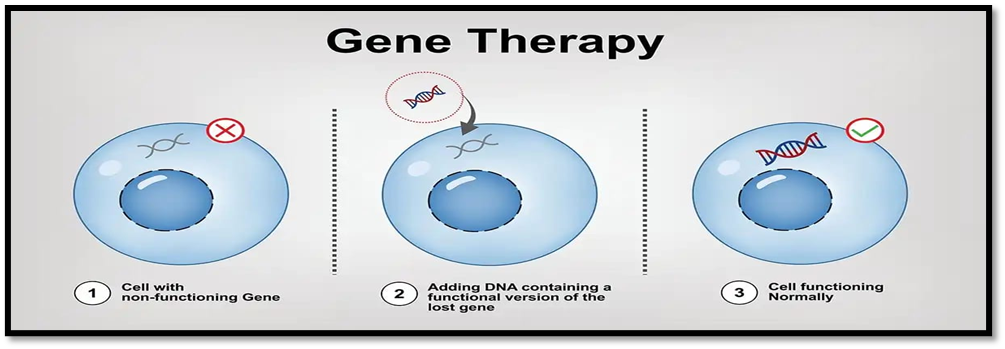
Figure 1 GENE THERAPY
HISTORY:
Human gene therapy trials were initiated in the 1980s; however, early progress was significantly limited due to serious adverse effects and ethical issues. In clinical studies involving X-linked severe combined immunodeficiency (SCID-X1), 5 out of 20 patients who received autologous bone marrow cells modified with a retroviral vector carrying the common γ-chain of cytokine receptors developed leukaemia[7]. This outcome raised major safety concerns regarding gene therapy. Subsequent investigations revealed that the therapeutic gene had integrated near the LMO2 oncogene, leading to uncontrolled proliferation of the modified cells. Beyond cancer development, additional safety challenges emerged during a clinical trial for ornithine transcarbamylase (OTC) deficiency, in which a patient died following a severe immune response to a recombinant adenoviral vector used for gene delivery[8]. Significant advancements in gene therapy research did not emerge until the early 2000s, when the field began to demonstrate more encouraging outcomes. Over the past decade, many of the safety concerns associated with gene therapy—an essential consideration in the development of any novel medical treatment—have been systematically addressed. This progress has resulted in an increasing number of gene-based therapies that have been demonstrated to be both safe and effective, and several are now available for clinical use [9]. In Europe, the first approved gene therapy, Glybera (uniQure), received market authorization in 2012 for the treatment of lipoprotein lipase deficiency, a rare metabolic condition characterized by extremely high triglyceride levels and an elevated risk of recurrent pancreatitis[10].Although the therapy had previously been granted orphan drug status in 2004, it was withdrawn from the market in 2017 due to limited commercial demand, largely driven by its high cost. Despite this, Glybera’s approval played a crucial role in stimulating further innovation in the field of gene therapy[11] . Following decades of foundational research, gene therapy has also gained recognition at the highest scientific level. In 2020, the Nobel Prize in Chemistry was awarded to Dr Emmanuelle Charpentier and Dr Jennifer Doudna for the development of CRISPR/Cas9, a revolutionary gene-editing technology often referred to as “genetic scissors” [12] .This precise method enables targeted removal and correction of defective genes and has significantly accelerated the translation of gene therapies from laboratory research to clinical application [13] .
Overview of gene therapy development :
Gene therapy was first proposed in the 1970s as a promising approach for treating inherited diseases through the introduction of healthy DNA to compensate for defective genes. The use of viral vectors for gene delivery into mammalian cells was later established in the 1980s. This progress culminated in the first approved gene therapy trial in 1990, in which a viral vector was used to deliver the adenosine deaminase (ADA) gene to a child suffering from X-linked severe combined immunodeficiency (SCID-X1) caused by ADA deficiency [14].
Despite initial success and widespread enthusiasm, the field faced major setbacks due to serious adverse events in subsequent trials. Adenoviral vector–mediated treatment for ornithine transcarbamylase deficiency resulted in fatal systemic toxicity in one patient Additionally, gamma-retroviral gene therapy for SCID-X1 led to insertional mutagenesis, activation of the LMO2 proto-oncogene, and abnormal T-cell proliferation in several patients. These incidents led to a temporary halt in gene therapy clinical research[15].
Which diseases can be treated with gene therapy?
Numerous congenital genetic disorders—including metabolic conditions, spinal muscular atrophy, cystic fibrosis, severe dyslipidaemias, cardiomyopathies, and congenital blindness—are rare diseases, affecting fewer than 1 in 2,000 individuals. These conditions usually appear in childhood and are associated with reduced quality of life and shortened survival. They also represent a significant burden for patients, families, and healthcare systems. While many of these disorders lack effective symptomatic therapies, gene therapy has shown potential as a disease-modifying treatment for selected conditions[16].
Gene therapy mainly targets monogenic disorders caused by mutations in a single gene within the human genome[17]. However, it is currently not applicable to diseases with complex polygenic origins or chromosomal defects involving numerical or structural abnormalities . Conversely, CAR T-cell therapy provides a targeted cancer treatment approach that is effective regardless of the specific mutational combinations driving malignancy[18].
In vivo Vector-Mediated Gene Therapy:
Gene therapy vectors are generally divided into viral and non-viral categories. Viral vectors, particularly adenoviral, adeno-associated viral, and retroviral or lentiviral systems, are most frequently used because of their high transduction efficiency, established safety, and regulatory acceptance. The primary goal of gene transfer is either to correct loss-of-function mutations by supplying a functional gene or to reduce the expression of toxic gain-of-function genes using RNA-based approaches such as shRNA, siRNA, miRNA, or antisense RNAVector pharmacokinetics and tissue targeting play a critical role in determining therapeutic efficacy[19].
Vector specificity is determined by the selected delivery system, its surface protein composition, and cis-acting regulatory elements such as promoters[20]. Adenoviral vectors were among the earliest platforms used due to their high transduction efficiency in both dividing and non-dividing cells, large transgene capacity, and low incidence of genomic integration[21]. Despite improvements in vector design, issues related to pre-existing immunity and strong innate and adaptive immune responses remain. These concerns have limited the use of Ad vectors in clinical trials targeting CNS diseases .In contrast, adenoviral vectors remain valuable in applications such as vaccination and oncolytic therapies, where immune activation may be advantageous or less restrictive[22].
The Retroviridae family has given rise to both gamma-retroviral and lentiviral vectors for gene therapy applications[23]. While gamma-retroviral vectors were used initially, lentiviral systems—especially those based on HIV-1—are now preferred[24]. This preference is due to their ability to integrate into the host genome and achieve durable gene expression in both dividing and non-dividing cells , their low tendency to induce immune responses, and their capacity to carry larger genetic inserts, enabling the expression of multiple genes within a single vector[25]. Compared with gamma-retroviral vectors, lentiviral vectors integrate less frequently near oncogene transcription start sites, thereby reducing oncogenic risk and improving overall safety[26]. Additional vector modifications have been introduced to limit or redirect genomic integration toward heterochromatin regions, minimizing unintended effects on gene regulation and enabling safe transduction of non-dividing cells or transient expression in proliferating cells (Lentz et al., 2012). Over time, lentiviral vectors have evolved into self-inactivating, replication-incompetent systems[27]. Pseudotyping strategies using alternative glycoproteins have further expanded their tissue specificity, allowing efficient targeting of the retina and hematopoietic stem and progenitor cells . Consequently, lentiviral vectors have been widely validated in clinical studies and are now preferred for many ex vivo gene therapy applications[28].
Ex vivo Cell Transduction Gene Therapy:
Ex vivo HSPC transduction gene therapy (HSPC-GT) has played a central role in the development of gene therapies, as mentioned above, with the successful treatment of ADA-SCID with γRV based vectors and later with the unfortunate occurrence of genotoxic events in SCID X1 patients disrupted the immediate success[29]. This led to the increased usage of LVs derived from the human immunodeficiency virus (HIV), which are believed to possess a safer integration profile and much lower risk of insertional mutagenesis[30]. In general, gene transfer into autologous HSPCs has the potential to provide permanent therapeutic gene expression as a selective treatment in monogenic inherited disorders, and can be exploited as cell vehicles to deliver proteins into the circulation and tissues, including the CNS[31]. Briefly, patients’ own cells are collected and stem cells are isolated to be mixed and transduced with a viral vector encoding a desired therapeutic gene. The transduced stem cells are later re-infused in the patient engrafted in the tissue, aiming at restoring a healthy phenotype[32].Thus, applying autologous HSPCs has become a viable treatment option for some patients with inborn errors of metabolism, providing enduring effect while reducing the risk of allogenic treatment-related toxicities and development of graft-vs.-host-disease as seen with donor HSPCs from healthy individuals[33]. HSPCs have lifelong ability to self-renew and to differentiate into The ability of HSPCs to generate diverse cell lineages makes them particularly suitable for gene therapy strategies. Despite incomplete characterization, HSPCs can be isolated ex vivo using surface marker expression, specifically the presence of CD34 and the absence of CD38. This CD34?CD38? profile allows reliable enrichment and purification of patient-derived stem cells [34].
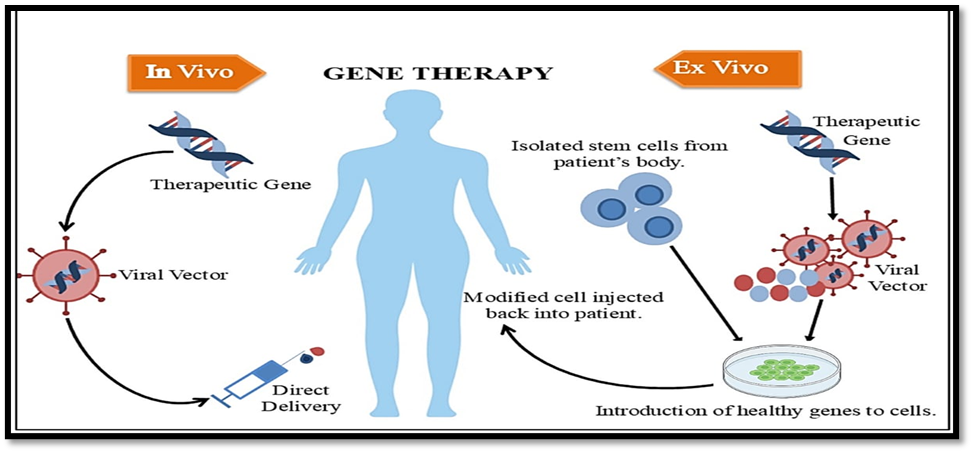
Figure 2 : In vivo & Ex vivo Gene Therapy
THERAPY STRATEGIES:
Gene therapy represents an advanced therapeutic approach for the treatment of both inherited and acquired diseases through the delivery of genetic material into specific target cells. The primary objective is to correct pathological conditions resulting from genetic defects or dysregulated gene expression[35]. This is achieved by introducing, modifying, or regulating genes to restore normal biological function or suppress disease-causing activity. The scope of gene therapy has expanded beyond gene correction to include applications such as vaccine development, cancer immunotherapy, and gene-silencing technologies based on oligonucleotides and RNA interference (RNAi)[36].
1. Gene Replacement Therapy
Gene replacement therapy involves the introduction of a functional gene to compensate for the loss or inactivation of an endogenous gene and is particularly effective in treating recessive monogenic disorders[37]. Adeno-associated virus (AAV) vectors are widely utilized in gene replacement strategies due to their small genome size, low immunogenicity, absence of known pathogenic effects in humans, and ease of genetic manipulation. Despite these advantages, gene replacement therapy is not universally applicable, as it is ineffective for dominant genetic disorders, polygenic conditions, and diseases involving genes that exceed vector packaging limits[38]. Notably, partial restoration of protein expression, even at levels below physiological norms, can be sufficient to achieve meaningful clinical benefits. In certain disease contexts, gene delivery to a limited population of affected cells is adequate to elicit therapeutic outcomes. Numerous clinical trials have reported encouraging results for gene replacement therapies, including those targeting inherited retinal disorders such as retinitis pigmentosa and choroideremia[39].
2. Gene Delivery Systems
Successful gene therapy depends on efficient systems capable of transporting therapeutic genetic material into target cells.Nucleic acids and proteins used in gene-based treatments are highly vulnerable to enzymatic degradation within biological environments[40].Delivery vectors serve as protective carriers, preserving the integrity of DNA, RNA, or protein payloads while enabling their passage through extracellular barriers and complex intracellular pathways.Consequently, the design and selection of gene delivery vectors are fundamental to the effectiveness of gene therapy.These delivery platforms are broadly categorized into viral and non-viral systems[41].Viral delivery systems have been extensively explored due to their high gene transfer efficiency.Retroviral vectors, which originate from RNA viruses, are commonly employed in gene therapy.Lentiviruses, a specialized subgroup of retroviruses, possess the ability to accommodate relatively large genetic sequences and integrate them into the host genome[42].This feature has made lentiviral vectors particularly suitable for gene transfer into hematopoietic stem cells.Adeno-associated viruses (AAVs) are small, single-stranded DNA viruses belonging to the Parvoviridae family[43]. Recombinant AAV vectors used in clinical applications are engineered from naturally occurring viruses and retain favorable biological traits such as efficient cellular entry and stable gene delivery without causing known human diseases. In parallel with viral approaches, substantial progress in material science has accelerated the development of non-viral gene delivery platforms[44]. These systems offer advantages including lower production costs, simplified manufacturing processes, reduced immunogenicity, and flexible design options.Non-viral vectors encompass a wide range of carriers, such as lipid-based assemblies, synthetic polymers, and inorganic nanostructures[45].Owing to their safety profile and adaptability, these vectors are increasingly used for the intracellular delivery of messenger RNA, particularly to antigen-presenting cells, highlighting their growing relevance in gene-based therapeutics[46].
3. Genome Editing Technologies
Genome editing refers to a collection of molecular techniques that enable deliberate and precise modification of DNA sequences within living cells[47]. These technologies function by creating targeted breaks in the DNA double helix, which subsequently activate endogenous DNA repair mechanisms[48]. Through these repair pathways, specific genes can be inserted, disrupted, or altered at predetermined genomic locations, allowing for highly targeted therapeutic interventions[49]. Genome editing offers the ability to eliminate pathogenic mutations, silence malfunctioning genes, or restore normal gene function, thereby directly addressing disease at the molecular level[50]. Earlier genome editing strategies relied heavily on homologous recombination techniques in embryonic stem cells to achieve targeted genetic alterations[51]. With continued technological advancement, genome editing has emerged as a transformative tool in biomedical research and clinical therapy. Its applications now extend beyond single-gene disorders to include complex diseases such as cancer, cardiovascular conditions, and infectious diseases[52]. Despite its considerable therapeutic potential, challenges remain, particularly the risk of unintended genetic modifications at non-target sites, which continue to be a critical focus of ongoing research and optimization efforts[ 53].
4. Gene Addition
Gene addition is an emerging therapeutic approach designed to manage both complex inherited disorders and acquired diseases by introducing supplementary genetic material into target cells[54].This strategy can influence disease progression through multiple mechanisms, including the delivery of neuroprotective factors in neurological conditions and the modification of key cellular signaling pathways[55].Recombinant adeno-associated virus (rAAV) vectors are commonly employed in gene addition approaches to deliver genes encoding therapeutic proteins, such as recombinant antibodies capable of neutralizing HIV-1, thereby mimicking the protective effects of an effective vaccine[56] . Despite its therapeutic promise, the clinical effectiveness of gene addition may be constrained by immune reactions elicited against rAAV vectors.Consequently, additional research is required to optimize this approach, particularly for its application in the treatment of ocular disorders[57].
5. Gene Silencing
Gene silencing strategies are mainly employed for the treatment of monogenic disorders caused by gain-of-function or toxic gene mutations. At present, RNA interference (RNAi)–based approaches delivered through recombinant adeno-associated virus (rAAV) vectors represent the most widely used gene-silencing platforms[58]. In addition, CRISPR-Cas13a technology has emerged as a versatile tool for selectively suppressing gene expression at the messenger RNA (mRNA) level in mammalian cells, offering new possibilities for therapeutic development. Gene transcription can also be effectively suppressed using dual AAV8 vector systems[59].
In the field of ophthalmology, small interfering RNA (siRNA)–based gene-silencing therapies are under active development, particularly for ocular conditions such as neovascular age-related macular degeneration (AMD) and glaucoma, with several candidates currently undergoing clinical evaluation[60]. Furthermore, preclinical studies using rAAV-mediated gene silencing targeting the vascular endothelial growth factor (VEGF)–phosphatidylinositol 3-kinase (PI3K)–protein kinase B (Akt) signaling pathway have demonstrated encouraging outcomes in diabetic retinopathy models, including reduced retinal vascular permeability in experimental animals[61]. Despite these promising findings, gene-silencing therapies face significant limitations, such as instability of RNA molecules, limited bioavailability, potential toxicity, and unintended off-target effects. To date, no ocular gene-silencing therapy has progressed beyond phase III clinical trials[62].
Challenges in Gene Therapy
Despite notable progress and encouraging outcomes in clinical investigations, gene therapy continues to face a range of scientific, technical, ethical, and economic obstacles. Unlike conventional pharmacological treatments, gene therapy is a rapidly evolving medical technology that raises complex ethical and legal considerations, particularly with respect to long-term safety and risk management. In addition, many gene-based medicines are currently developed for rare disorders and certain cancers, resulting in extremely high treatment costs that limit patient access[63].
Manufacturing challenges represent a major barrier to the widespread application of gene therapy. The production and purification of viral vectors, especially adeno-associated virus (AAV) vectors, remain inefficient and difficult to scale. Existing manufacturing systems often suffer from low yield, complicated purification procedures, limited stability, and challenges in maintaining product consistency during large-scale production. Beyond manufacturing complexity, viral vectors also present inherent limitations, including restricted genetic payload capacity, variable levels of transgene expression, and concerns related to immunogenicity[64].
To overcome these limitations, future gene therapy strategies must achieve high specificity and efficiency in targeting appropriate cells and tissues while allowing precise control over gene expression. This requirement is particularly critical in the treatment of complex diseases. For example, therapeutic approaches involving insulin gene expression in diabetes must incorporate regulatory elements capable of sensing blood glucose levels and adjusting insulin production accordingly. Furthermore, for gene therapy to become broadly applicable, treatment costs must be significantly reduced, transforming current high-cost therapies into affordable options for the majority of patients[65].
In parallel with technological advancements, the regulatory framework governing gene therapy must continue to mature. Strengthening quality control systems, accelerating the development of independent third-party testing facilities, and enhancing collaboration between pharmaceutical developers and regulatory authorities are essential steps toward safe and effective clinical translation. With coordinated global efforts from research institutions, industry, and regulatory bodies, gene therapy has the potential to overcome existing challenges and achieve a transformative impact on modern medical practice[66].
Clinical Applications of Gene Therapy in Rare Diseases
In recent years, gene therapy has advanced rapidly, with significant improvements in both therapeutic efficacy and safety. Following encouraging outcomes in preclinical animal studies, gene therapy strategies have progressively moved into human clinical trials. Advances in genetic diagnostics for rare disorders, together with the development of precise gene-editing technologies, have positioned gene therapy as a central research focus for rare disease treatment. By employing delivery vectors to introduce corrective genetic material into specific target cells, gene therapy aims to repair underlying genetic defects and, in some cases, achieve long-lasting or potentially curative effects through a single intervention[67].
1. Blood Disorders
Inherited blood diseases caused by defects in single genes that affect blood cells or plasma proteins are well suited for gene replacement or gene-editing approaches. Hemophilia is a rare hereditary disorder characterized by impaired blood coagulation, often leading to spontaneous bleeding into joints or muscles, progressive disability, and life-threatening hemorrhage. As a monogenic condition, hemophilia represents an ideal target for gene-based treatment[68].Gene therapy offers a one-time therapeutic strategy by introducing a functional copy of the deficient gene, enabling affected cells to resume the production of essential clotting factors. Viral vectors, particularly adeno-associated viruses (AAVs), are commonly used for gene delivery. Early clinical studies employing AAV-mediated transfer of the factor IX gene for hemophilia B demonstrated favorable safety outcomes and sustained gene expression over several years following treatment[69].
2. Neurodegenerative Disorders
A large proportion of monogenic disorders manifest with neurological symptoms, and numerous genetic mutations associated with neurodegenerative conditions have been identified. Diseases such as Alzheimer’s disease, Parkinson’s disease, and amyotrophic lateral sclerosis are characterized by progressive neuronal dysfunction and loss[70]. Gene therapy approaches for these conditions often focus on promoting neuronal survival, enhancing neurite outgrowth, or restoring defective molecular pathways. AAV vectors are particularly advantageous for central nervous system applications due to their ability to deliver genes to neurons and supporting cells following a single administration, resulting in prolonged therapeutic expression. Clinical studies in neurological disorders, including Parkinson’s disease, have confirmed the long-term safety and sustained efficacy of AAV-based gene therapies, highlighting their substantial potential in the treatment of neurodegenerative diseases [71].
3. Ocular Diseases
AAV-mediated gene therapy has shown exceptional promise in ophthalmology, largely due to the identification of causative genes for many inherited eye disorders. The unique anatomical features of the eye—its small, enclosed structure and suitability for localized administration—facilitate precise gene delivery. Additionally, the presence of the blood–retinal barrier contributes to the immune-privileged status of the eye, reducing systemic immune responses to gene therapy vectors. The success of ocular gene therapy marked a major milestone in the field[72]. In 2008, multiple independent studies demonstrated the safety and therapeutic benefit of subretinal delivery of AAV encoding the RPE65 gene, effectively revitalizing clinical interest in gene therapy. This progress ultimately led to the regulatory approval of Luxturna, the first AAV-based gene therapy, for the treatment of Leber congenital amaurosis. Currently, several AAV-based treatments for ocular disorders, including achromatopsia and retinitis pigmentosa, have progressed to early-stage clinical trials. While no severe vector-related adverse effects have been reported and some patients have experienced visual improvement, treatment responses vary, and long-term durability remains under investigation. In certain cases, therapeutic benefits decline over time, possibly due to continued retinal degeneration or activation of innate immune mechanisms [73].
4. Muscular Disorders
Neuromuscular diseases encompass a broad range of inherited and acquired conditions that impair motor neurons, neuromuscular junctions, or skeletal muscle tissue. Many of these disorders, including Duchenne muscular dystrophy and spinal muscular atrophy, arise from well-defined genetic defects and exhibit single-gene inheritance patterns, making them suitable candidates for gene therapy[74]. AAV-based gene delivery has demonstrated particularly impressive results in clinical trials for infantile spinal muscular atrophy. In these studies, children receiving a single intravenous dose of AAV-mediated gene therapy exhibited markedly improved survival rates, enhanced motor function, and, in some cases, achieved independent ambulation. These outcomes underscore the transformative potential of gene therapy for severe neuromuscular diseases [75].
CONCLUSION:
Gene therapy has emerged as a powerful and evolving therapeutic approach for the treatment of rare and monogenic diseases. Advances in viral vector design, genome-editing technologies, and ex vivo and in vivo delivery strategies have significantly improved the safety and efficacy of gene-based interventions. Clinical successes in blood, neuromuscular, neurological, and ocular disorders demonstrate the potential of gene therapy to provide long-term or curative outcomes with single-dose treatments. Despite these achievements, challenges related to immune responses, manufacturing complexity, high treatment costs, and long-term safety remain. Continued technological innovation, regulatory harmonization, and cost-reduction strategies will be essential to translate gene therapy into a widely accessible and sustainable treatment modality in modern medicine.
REFERENCES



Siddhi Desai, Vaidehi Mane, Prachi Somavase, Tejashree Khamkar, Gene Therapy in Rare and Monogenic Diseases: Progress, Strategies, and Clinical Applications, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1954-1967. https://doi.org/10.5281/zenodo.18623026
 10.5281/zenodo.18623026
10.5281/zenodo.18623026
