
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Sgrs College Of Pharmacy Saswad
Skin pigmentation disorders like hyperpigmentation, melasma, dark spots, and post-inflammatory pigmentation affect millions worldwide, often triggered by UV exposure, hormonal changes, inflammation, and aging. While conventional depigmenting agents like hydroquinone and kojic acid are effective, they can cause skin irritation and sensitivity, leading to a demand for safer alternatives. Herbal ingredients have gained attention for their natural skin-brightening and healing properties. Botanicals such as turmeric, aloe vera, licorice, alum, honey, vitamin E, glycerin, and rose water show potential in reducing pigmentation while nourishing the skin. Among these, alum, known for its astringent and skin-tightening effects, remains underexplored for its depigmenting potential. The synergistic action of these natural compounds may inhibit melanin production, promote cell renewal, and enhance overall skin health.
Skin hyperpigmentations, which are common in the Indian population, are one of the main dermatological conditions affecting people with pigmented skin phototypes. Treatments typically use topical depigmenting chemicals to reduce the amount of melanin or ray technology. The aspect of exposure to sunlight is still often overlooked. Native saturation varies widely around the world, and some skin tones—particularly among Asian and Indian subjects—are said to be more vulnerable to saturation diseases than other mortality groups. 1,2) The Indian population's skin saturation and variety, as well as related pigmentary illnesses, are the main topics of this review. Using rebuilt skin models that may be used to decipher the underlying mechanisms, the impact of ultraviolet (UV) exposures on skin saturation and their role in pigmentary illnesses will be compared with perceptivity in UV-confirmed biomarkers that were first connected. Similarly, photoprotective techniques and therapy approaches for saturation disorders are covered. One of the most common dermatological conditions, especially in those with pigmented skin phototypes, is skin hyperpigmentation, which is especially common in Indians. Colorful treatment approaches, including topical depigmenting agents and ray technologies, have been extensively used to reduce melanin content and manage saturation diseases. still, the significant part of solar exposure in the development and exacerbation of these conditions is frequently overlooked( 3). The variability in native saturation across different ethnical groups is well- established, with certain populations, particularly Asian and Indian subjects, being more prone to saturation diseases compared to others( 2). These individualities frequently parade increased vulnerability to conditions similar as melasma,post-inflammatory hyperpigmentation( PIH), and sun- convinced dark spots. The impact of ultraviolet( UV) radiation on skin saturation is a critical factor contributing to these diseases, as dragged exposure can spark melanin overproduction and oxidative stress, leading to patient saturation issues( 2,3). This review primarily focuses on skin saturation variations and associated pigmentary diseases within the Indian population. also, it explores the influence of UV exposure on saturation changes, emphasizing its part in the pathogenesis of colorful pigmentary conditions. perceptivity into UV- convinced biomarkers linked using repaired skin models will be bandied to crack the underpinning mechanisms of saturation diseases. also, this paper examines current treatment strategies, including the efficacity of topical agents, ray- grounded interventions, and Page 1 of 2 the significance of photoprotective measures in precluding and managing hyperpigmentation( 2,3).
Pay attention to the Indian script. Studies on the differences in Indian skin tones across diverse geographic regions and their susceptibility to prevalent saturation disorders are included in this section. More than 80 percent of people, regardless of age or gender, have a variety of skin tones on their faces, according to a large sample research conducted across four Indian metropolises.4 Hyperactive pigmented patches, melasma, poorly defined pigmented macules, and dark circles are the main causes of this variety. Additionally, these various lesions often attend. Hypopigmentary disorders are less common in this study. similar as vitiligo, pityriasis alba, pityriasis versicolor, hypopigmented leprosy, nevus achromicus, and albinism and some hyperactive- pigmentary diseases similar as idiopathic guttate and confluent hypermelanosis, and lichen amyloidosis.. Pigmentary diseases cause mental torment and have a detrimental effect on a person's quality of life5. The pathophysiology of three significant hyperpigmentary illnesses in India—melasma, actinic lentigines, postinflammatory hyperpigmentation (PIH), and videlicet—will be discussed in length here, with a focus on the role that UV exposure plays.
Causes:-
Melasma develops due to a combination of factors, with ultraviolet( UV) exposure being one of the most significant triggers. Dragged sun exposure stimulates inordinate melanin product, with studies indicating that further than 25 of melasma cases are linked to UV radiation(6). Hormonal changes, particularly increased estrogen situations during gestation or due to oral contraceptive use, play a pivotal part in its onset. also, inheritable predilection makes individualities with a history of melasma more susceptible of developing the condition( 7). Other contributing factors include phototoxic medicines, which increase skin perceptivity to light, and underpinning health conditions similar as ovarian dysfunction, thyroid diseases, and liver conditions, all of which have been associated with melasma(7).
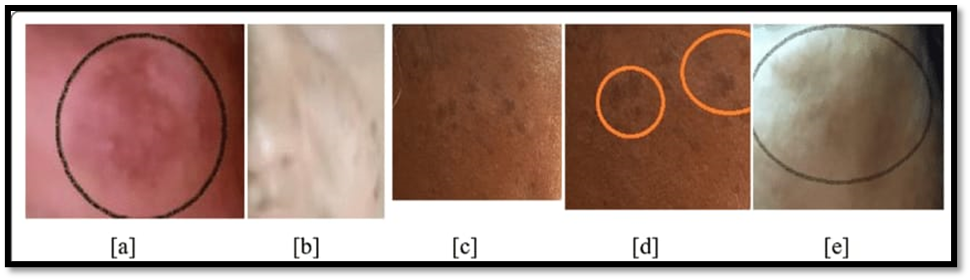
Fig no 1. signs of hyperpigmentation of the skin. hyperpigmentation following a. inflammation. b PIH was caused by acne. Melsama's face. Melsama location. Face age spots.8
Symptoms:-
Melasma is characterized by hyperpigmented patches that range from brown to gray - brown, primarily appearing on the cheeks, forepart, upper lip, and chin( 7). These patches frequently show a symmetrical distribution, affecting both sides of the face equally.However, melasma can suffer progressive worsening, especially with continued sun exposure, If left undressed. Grounded on the depth of saturation, melasma is classified as epidermal( superficial), dermal( deep), or mixed, which can be determined through histological or necessary analysis. Since UV exposure is a crucial aggravating factor, proper sun protection is essential for managing and precluding the condition.
Causes:-
Actinic lentigines are a clinical indicator of photoaging and are mostly brought on by prolonged sun exposure. They are also referred to as solar lentigines or lentigo senilis. They serve as a gauge of cumulative UV radiation exposure, which also increases the risk of skin cancer, and their frequency rises with age. Fair to medium photoaged skin types are more likely to have these lesions, and their frequency in India is comparable to that of other Asian nations. A large- scale study in India set up that one- third of women around 50 times old and half of the population over 70 times old are affected( 1). While inheritable predilection and natural aging may contribute, UV exposure remains the dominant factor in their development.

Figure 2 . Class of Lentigines with its parent images10
Symptoms
Actinic lentigines appear as light brown to dark brown spots or reticulated patches on sun- exposed areas like rearward hands, forearms, upper box, and face. They may be solitary or multiple and frequently act seborrheic keratosis or simplex lentigos, causing ornamental enterprises due to their association with aging. Histologically, they show hyperpigmentation of the rudimentary subcaste( hypermelaninosis), with some studies also reporting increased melanocyte figures( hypermelanocytosis). The epidermal structure is frequently disorganized, with broadened rete crests and elongated protrusions into the dermis. Although their strong link to UV exposure is well known, the molecular mechanisms behind their conformation are still being studied, with recent exploration suggesting a part for keratinocyte growth factors and other factors.
Causes
Periorbital hyperpigmentation( POH), generally appertained to as dark circles, is also known as periorbital melanosis or periocular hyperpigmentation and is particularly current in Asians. Studies show that 50 of Indian women witness minor to severe dark circles, particularly on upper eyelid, with inflexibility adding with age( 11). The most common type of POH is the indigenous/ inheritable type, counting for 51.5 of cases, followed by post inflammatory hyperpigmentation at 22.5, although its exact etiology remains unclear. Some experimenters describe POH as acquired idiopathic patterned facial saturation or idiopathic cutaneous hyperchromia at the orbital region 12, both of which affect from genetically increased pigmentary exertion. Sun exposure has been linked as a crucial factor in exacerbating POH. Other contributing factors include vascular abnormalities, indigenous factors, post inflammatory saturation, and shadow goods [12]. Some studies suggest that POH may also be an extension of pigmentary discrimination lines on the face( 11).
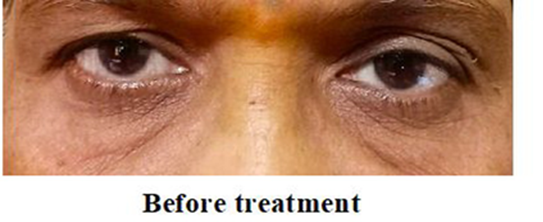
Figure 3. image of periorbital hyperpigmentation before the treatment 11,12
Symptoms
POH presents as dark brown, bluish, or purplish abrasion around the upper and lower eyelids, giving a tired or aged appearance. It may appear bilateral and symmetrical, with variations in intensity depending on skin type, genetics, and environmental exposure. In some cases, vascular traffic may contribute to a sanguine or grandiloquent tinge, while pigmentary causes affect in brownish abrasion. POH is frequently progressive, worsening with aging, stress, sleep privation, and sun exposure. Though not dangerous, it can beget significant ornamental and cerebral torture in affected individualities.
UV-Induced Skin Damage The skin is the first line of defense against environmental factors, including UV radiation. However, exposure to UV ray causes significant damage, ranging from mild sunburn to serious conditions like skin cancer. Sunburn is the most immediate effect of excessive UV exposure, leading to redness, swelling, and pain. Studies show that a large portion of the population, particularly young adults, frequently experience sunburn, which significantly increases the risk of melanoma. UVA rays penetrate deeper into the skin, causing tanning, while UVB rays affect the surface, leading to burns and long-term cellular damage.
UVB exposure also triggers inflammation by activating proteins such as VEGF, TRPA1, and TRPV1. These proteins stimulate inflammatory pathways, increasing redness, pain, and swelling. This inflammatory response is a hallmark of sunburn and can contribute to chronic skin damage over time. The MAPK pathway further amplifies this process, leading to the activation of inflammatory genes. Since repeated sunburns heighten the risk of skin cancer, taking preventive measures is crucial. Using photoprotective sunscreen, wearing UV protected clothing, and less sun exposure can help reduce UV-induced skin damage and lower the risk of long-term health issues. Protecting the skin is essential for maintaining overall skin health.
Symptoms
UV- convinced saturation diseases manifest as dark spots, uneven skin tone, and patient pigmented patches on sun- exposed areas similar as the face, hands, shoulders, and on hands . individualities may also witness skin roughness, fine lines, blankness, greenishness, and increased perceptivity to sun. In more severe cases, dragged UV damage can lead to freckling, solar lentigines, and worsening of being saturation diseases. Over time, repeated UV exposure contributes to unseasonable aging and an increased threat of skin malice, making photoprotection essential in managing these conditions.13
Hyperpigmentation creams aim to lighten dark spots, balance skin tone, and restore skin radiance. These plant-based ingredients are scientifically and traditionally known to target excess melanin, inflammation, and oxidative damage — the primary causes of hyperpigmentation.
1. Turmeric (Curcuma longa)14
Active compound: Curcumin
Role in cream:
Formulation Use: Ideal in creams as an extract or essential oil; pairs well with soothing agents like aloe or chamomile to reduce staining.
2. Licorice Root (Glycyrrhiza glabra):-15
Active compound: Glabridin
Role in cream:
Formulation Use: Works best as an extract or hydrosol; ideal for daily use creams and sensitive skin formulations.
3. Aloe Vera (Aloe barbadensis)16
Active compound: Aloin
Role in cream:
Formulation Use: Commonly used as a gel base or extract to enhance skin absorption and moisture retention.
4. Manjistha (Rubia cordifolia)
Role in cream:
Formulation Use: Added as a powdered herb or extract; excellent for both topical and internal skin health synergy.
5. Neem (Azadirachta indica)17
Role in cream:
Formulation Use: Used in leaf extract or oil form; especially beneficial in anti-acne and dark spot treatments.
6. Sandalwood (Santalum album)18,19
Role in cream:
Formulation Use: Sandalwood oil or powder works well in calming night creams or masks for brightening.
7. Saffron (Crocus sativus)19
Active compound: Crocin, Safranal
Role in cream:
Formulation Use: A luxurious and potent addition; best infused in milk or oil before being added to cream bases.
8. Gotu Kola (Centella asiatica)
Active compound: Asiaticoside
Role in cream:
Formulation Use: Found in serums or creams targeting sensitive, scarred, or mature skin.
9. Green Tea (Camellia sinensis)20
Active compound: EGCG (Epigallocatechin gallate)
Role in cream:
Formulation Use: Works well as an extract or infusion; suitable for lightweight, antioxidant-rich creams.
10. Bakuchi (Psoralea corylifolia)
Active compound: Bakuchiol
Role in cream:
Formulation Use: Used in oil or powdered form; great for night creams or anti-aging pigmentation blends.
Its anti-inflammatory nature reduces redness and irritation, which are common triggers for post-inflammatory hyperpigmentation (PIH).
Skin pigmentation disorders are a common concern, especially in regions like India, where sun exposure and genetic factors play a significant role. While conventional treatments like hydroquinone and laser therapy can be effective, they often come with side effects, making natural alternatives an appealing option.
Herbal ingredients such as turmeric, aloe vera, licorice, manjistha, neem, and sandalwood have shown promising results in reducing hyperpigmentation, soothing inflammation, and improving overall skin health. Other natural components like alum, honey, and vitamin E also contribute to skin brightening and repair. These remedies offer a holistic, gentle approach to managing pigmentation without the risks associated with synthetic chemicals. Although herbal formulations hold great potential, more clinical research is needed to validate their long-term safety and efficacy. By integrating traditional knowledge with modern dermatological studies, we can develop safe, effective, and accessible treatments for hyperpigmentation, offering a natural path to healthy, radiant skin.
REFERENCES






Sanket Wankhede*, Sakshi Yadav, Vansh Wagh, Pradyna Yadav, Shreya Yadav, Srushti Phadtare
 10.5281/zenodo.15333304
10.5281/zenodo.15333304