
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Vidya Bharti College of Pharmacy Amravati.
Neuromuscular Blocking Agents (NMBAs) are essential in anesthesia for muscle relaxation during surgical procedures. They are classified into non-depolarizing and depolarizing agents, with depolarizing agents activating acetylcholine receptors and non-depolarizing agents blocking them. NMBAs are commonly administered intravenous, intramuscular, or intraosseous, and their dosage depends on patient characteristics. Interprofessional collaboration is crucial for optimal NMBA management.Novel drug delivery systems, such as transdermal patches for Rivastigmine, offer faster onset and non-invasive methods for treating Alzheimer’s. These systems also offer nasal administration, inhalational delivery, intra-articular delivery, mucosal buccal delivery, subcutaneous administration, microdosing, and targeted delivery systems using nanoparticles or liposomes. These systems improve patient comfort, reduce side effects, and speed up drug onset. Applications include nanoparticles for drug solubility and bioavailability, hydrogels for wound healing and tissue engineering, colloidal carriers for targeted therapy, 3D printing for personalized formulations, phytosomes for improved bioavailability, and injectable in situ- gelling systems for sustained.
Background
Neuromuscular blocking agents (NMBAs) are a recent development in anaesthesia that, in addition to their usual effects of narcosis and analgesia, also relax muscles. The purpose of this educational program is to provide healthcare professionals with the knowledge they need to optimize treatment through the use of anesthesia and other therapeutic combinations. It does this by highlighting the indications, mechanism of action, administration methods, adverse effects, contraindications, monitoring, and toxicity of NMBAs. This program helps healthcare professionals better grasp the pharmacological characteristics of NMBAs, which helps them tailor treatment re When a patient has decreased lung compliance, neuromuscular blockade is often utilised in an aesthesia to help with mechanical breathing, optimise surgical circumstances, and make endotracheal intubation easier. Neuromuscular blocking agents (NMBAS) are classified into two categories: nondepolarizing (such as rocuronium, vecuronium, atracurium, cisatracurium, and mivacurium) and depolarising (such as succinylcholine). It is important to carefully consider patient variables, the type of treatment being performed, and the therapeutic indication when choosing the class of NMBAS to use in order to attain blockage of the neuromuscular. Neuromuscular blockers are essential anesthetic medications that help in the care of critically ill patients by allowing muscles to relax during surgery. These medications, which were first introduced in 1942, greatly increase surgical safety and efficacy by enabling surgical access without causing involuntary muscle movement [1].
Depolarizing Agents: Acetylcholine receptors are bound by succinylcholine, which first depolarizes the cell before paralyzing it [2].
Non-Depolarizing Agents: These substances, which include vecuronium and atracurium, prevent acetylcholine from binding and hence impede neuromuscular transmission [2].
Utilizing Clinical Applications
Surgery: Necessary for operations involving the relaxing of muscles [1].
ICU Use: Applied to diseases such as emergency intubation and acute respiratory distress syndrome [3] Modern medications with different onset and duration timings, such as pipecuronium and mivacurium, enhance patient results and safety. This review will cover various routes of administration pharmacology and application of drug delivery systems as well as the reversal of neuromuscular block.
Structure of NMBS:
All quaternary ammonium compounds that are marketed as NMBDs in the UK. N· (CH3)3, a quaternary nitrogen group, is present in acetylcholine (ACh), to which they are structurally similar. The positive nitrogen atoms of NMBDs are drawn to the postsynaptic nicotinic receptor asubunits, just as those of ACh. Pancuronium, atracurium, succinylcholine, and other NMBDs have two quaternary ammonium cations in them. Compared to monoquaternary amines, which only contain one tertiary amine and one permanent quaternary cation, such as rocuronium, tubocurarine, and vecuronium, these bisquaternary amines are more potent. However, the tertiary amine can get protonated and hence positively charged at physiological pH, particularly in acidotic circumstances, which increases the potency of monoquaternary NMBDs. This factor is clinically significant; in acidotic individuals, the effect of such NMBDs is amplified. Acetylcholine, the muscle, and the neurone are the three main elements of the neuromuscular junction shown in Figure 1. Neurones have vesicles that store acetylcholine. Exocytosis, a mechanism that releases acetylcholine into the synapse, occurs when an action potential is formed. To mimic a muscular contraction, acetylcholine attaches to receptors on the muscle cell.gimens to the specific needs of each patient and efficiently control muscle relaxation during surgery. Precise dosage modifications and the reduction of possible adverse effects are made easier with a thorough grasp of NMBAs, which enhances patient safety and effectiveness. In order to improve patient outcomes and care standards, the program emphasises the value of interprofessional collaboration when administering neuromuscular blocking medications. It does this by creating a clear definition of roles and encouraging teamwork. This exercise is an essential tool for medical professionals who want to get better at comprehending and using NMBAs in order to provide more focused, individualised care that enhances patient outcomes.
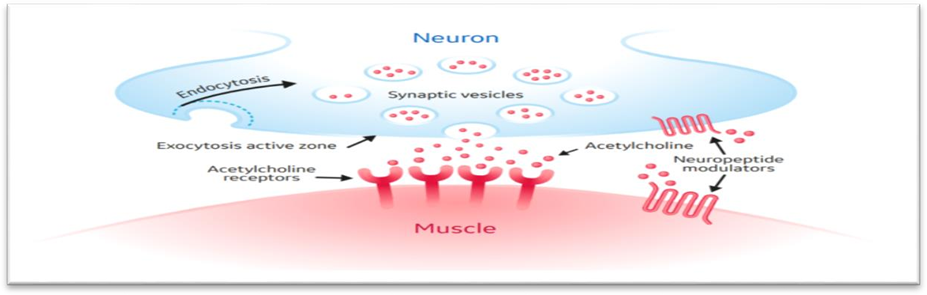
Figure 1: The Principal Elements of The Neuromuscular Connection

Figure2: Neuromuscular Blocking Agent Subtypes
A lipophilic variable-sized bridge structure separates the two quaternary ammonium groups. The bridging structure is a key factor in determining the effectiveness of NMBDs and varies with different series. NMBDs are categorized as either non-depolarizing or depolarizing. [4,5,6]
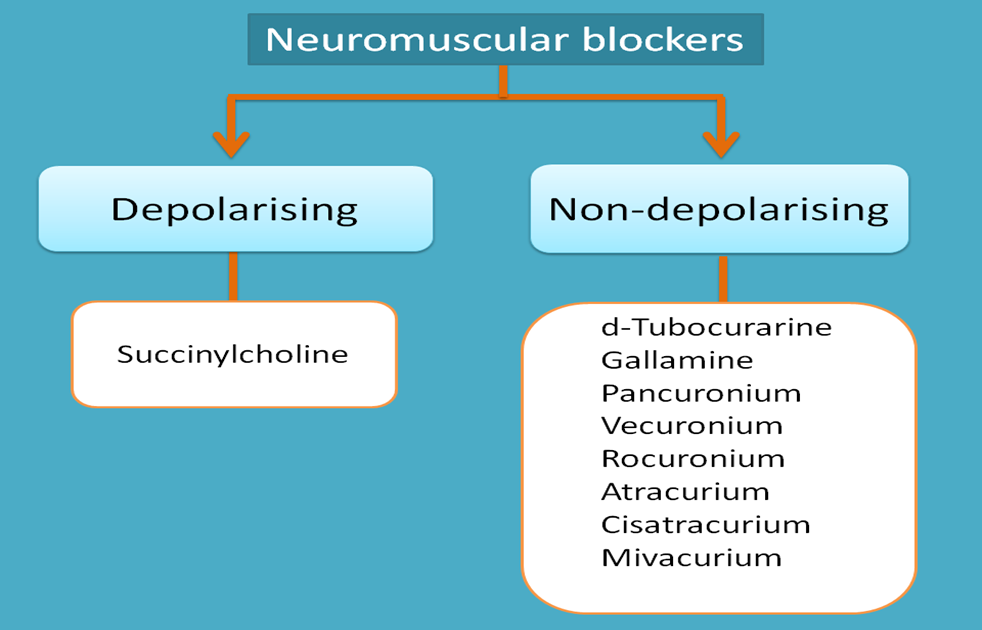
Figure:3 Classification of NMBs
The two main structural groups of non-depolarizing NMBAs are as follows: Aminosteroids Neuromuscular Blockers
Benzylisoquinolinium Neuromuscular Blockers
NMBDs Can Be Categorized as Follows Based on How Long They Last:
•Short-acting (eg, mivacurium, succinylcholine)
•Intermediate-acting (eg, vecuronium, rocuronium, atracurium)
•Long-acting (eg, pancuronium, gallamine, tubocurarine[9]
Mechanism Of Action
One important neurotransmitter in the peripheral nervous system is acetylcholine. Upon deeper examination of the nervous system, we discover that the motor nerve axon splits into terminals known as motor end plates. Although they are encased in muscle fibres, the synaptic cleft keeps them apart from the fibres. An impulse travels down the neurone in response to a stimulation to the nerve. Acetylcholine is released into the neuromuscular junction, also known as the synaptic cleft, when a nerve impulse reaches the end of a motor neurone. There, it binds to receptor sites on the membrane of the muscle cell, depolarising it and causing muscle contraction. iNeuromuscular blocking substances work at the motor end plate by either preventing membrane depolarisation or by vying with acetylcholine for receptor sites.
Depolarizing NMBAs bind to cholinergic receptors on the motor endplate, causing initial depolarization on the endplate membrane but then preventing neuromuscular transmission .
Non-depolarizing NMBAs competitively inhibit the acetylcholine receptor on the motor endplate either by preventing altering the receptor or blocking the ion channels to prevent the creation of an endplate action potential[10]
Depolarizing NMBs Depolarizing medicines act as agonists at Ach receptors. Succinylcholine is the only depolarizing NMBD currently in clinical use. It consists of two Ach molecules connected together by acetate methyl groups. The two quaternary ammonium radicals attach to the two α-subunits of one nicotinic receptor, causing depolarization. When voltage- sensitive sodium channels detect membrane depolarization (due to Ach receptor activation), they first open (Fig. 4A(b)) before closing and becoming inactive (Fig. 4A(c). To restart the sodium channels, the membrane potential must be reset (Fig. 4A(a)). This is a very fast process with Ach

(1 ms), as it is hydrolyzed by acetylcholinesterase (AChE) within the synaptic cleft.However, because succinylcholine is not degraded by AChE, the Ach receptors remain activated for an extended period of time. The sodium receptors on the endplate and in the perijunctional zone remain inactive (Fig. 4A(c)), and junctional transmission is inhibited. The muscle becomes flaccid. Figure 4(A) shows a sketch of the sodium channel. The bars v and t represent the molecule’s gates. Gate v is voltage-dependent, whereas gate t is time dependent. (a) Resting state: v is closed and t is open. (b) Active state: v opens when the surrounding membrane depolarizes, allowing ion flow; t closes shortly thereafter to deactivate the channel. (c) Inactive state: v remains open and t is closed. This condition persists as long as the surrounding membrane is depolarized. When the membrane repolarizes, the channel goes back to its resting condition. (B) Different states of nicotinic acetylcholine receptors.Upper (left to right): resting; resting with agonist bound to recognition sites but channel not yet opened; and active with open channel permitting ion flow.Lower (left to right): desensitized with agonist bound to recognition site. Both are non-conductive. Every conformation is in dynamic equilibrium. (Reproduced with permission from Elsevier, Standaert FG. Neuromuscular physiology and pharmacology. In Miller RD (ed.), Anesthesia, Fourth Edition. New York: Churchill Livingstone, 1994; 731–54. Depolarization block is also called Phase I or accommodation block and is often followed by muscle fasciculation. This is probably the result of the prejunctional effect of succinylcholine, activating Ach receptors on the motor neuron, generating repeated firing and release of neurotransmitter. Recovery from Phase I block occurs as succinylcholine diffuses away from the neuromuscular junction, down a concentration gradient, as plasma concentration declines. Plasma cholinesterase (formerly known as pseudocholinesterase) metabolizes it. Prolonged exposure to succinylcholine at the neuromuscular junction can cause (I) desensitization block or
(ii) Phase II block.
Desensitization Block
Desensitization happens when Ach receptors become insensitive to the channel-opening activities of agonists, including Ach. Receptors are constantly switching between resting and desensitized states, regardless of whether agonists are present (Fig. 1B). Agonists promote or trap receptors in a desensitized state because desensitized receptors have a high affinity for them. Normally, Ach is hydrolyzed so quickly that it has no ability to cause desensitization. Desensitization block may be a safety mechanism that prevents over excitation of the neuromuscular junction.
Phase II Block
Phase II block differs from desensitization block. It happens with several boluses or a protracted succinylcholine infusion.Phase II block, which is characterized by fade of the train-of-four (TOF) twitch response, tetanic fade, and post-tetanic potentiation—all characteristics of competitive block—can occur in patients with atypical plasma cholinesterase after a single dose of the medication. Following the initial depolarization, the membrane potential progressively returns towards the resting state, despite the fact that the neuromuscular junction is still exposed to the drug. Neurotransmission is maintained throughout. Possible explanations for the development of Phase II block include presynaptic block, which reduces Ach synthesis and mobilization; post junctional receptor desensitization; and activation of the sodium-potassium ATPase pump via the postsynaptic membrane repolarizes after its initial depolarization.Inhalation anesthetic medicines hasten the onset of Phase II block. Anticholinesterase medicines can be used to inhibit its activity, although the outcome is unpredictable. Therefore, it is recommended to allow natural recuperation.
Non-depolarizing NMBs
Non-depolarizing NMBDs compete with Ach for binding to the postsynaptic nicotinic receptor. They do not cause conformational changes in the receptor, unlike depolarizing medications. Binding to one or both α-subunits prevents Ach from depolarizing the receptor. Antagonists bind to receptors in a dynamic manner, alternating between association and dissociation. If the concentration of Ach increases, it has a better chance of occupying receptor sites than the antagonist. With antagonist block, the end-plate potential gradually decreases until it falls below the threshold for firing a propagating action potential to cause muscle contraction. Under normal physiological settings, more transmitter molecules than are required generate the end-plate potential, resulting in a larger response than required. At the same time, just a subset of the accessible receptors are utilized to generate the signal. Thus, neuromuscular transmission has a significant margin of safety. Neuromuscular block, defined as a decrease in single twitch height, appears only when 70-80% of receptors are filled by non-depolarizing NMBDs. To achieve totalblock, at least 92% of the receptors must be filled. Non-depolarizing NMBDs, like depolarizing medications, produce desensitization block. They bind firmly to desensitized receptors, trapping them in these states (Fig. 1B). This is an uncompetitive block. When more receptors are desensitized, the margin of safety for transmission is diminished. Many medicines used during anaesthesia increase the number of desensitized receptors [10,11,12,13,14,15].
Routes Of Administration For NMBS
Here are different routes of administration for neuromuscular blockers (NMBs) along with their mechanisms:
1.Intravenous (IV): Most common route for NMBs, administered directly into a vein.
2.Intramuscular (IM): Administered into a muscle, used for some NMBs like succinylcholine.
3.Intraosseous route (IO): Administration directly into bone marrow, used when IV is difficult.
4.Intraperitoneal (IP): Administered into the peritoneal cavity, used in some surgical procedures.
5.Topical: Applied directly to the skin or mucous membranes, used for local anesthesia.
1.Intravenous route (IV)
Intravenous injection is the most common form of administration. Nonetheless, in long-term surgical instances, it can be safely infused intramuscularly or continuously by intravenous infusion[16,17]
Mechanisms of Action:
1.Competitive Blockade: NMBs competitively bind to acetylcholine receptors at the neuromuscular junction, preventing acetylcholine from binding and triggering muscle contraction. Examples: Rocuronium, Vecuronium.
2.Depolarizing Blockade: NMBs depolarize the muscle membrane, causing initial muscle contraction followed by paralysis. Example: Succinylcholine.
3.Non-Depolarizing Blockade: NMBs bind to acetylcholine receptors, preventing depolarization and muscle contraction. Examples: Pancuronium, Pipecuronium.
For example:
•Succinylcholine: Most commonly administered intravenously, but can also be given intramuscularly or via continuous intravenous infusion.
•Rocuronium: Can be administered intravenously for intubation and maintenance.
•Vecuronium: Can be administered intravenously for intubation and intraoperatively.
•Pancuronium: Can be administered intravenously for intubation and intraoperatively.
•Cisatracurium: Can be administered intravenously for intubation and as a maintenance infusion.
•Mivacurium: Can be administered intravenously for intubation and as a maintenance infusion. [23]
Neuromuscular blocking agents (NMBAs) are poorly absorbed when taken orally and are most effective when injected intravenously or intramuscularly.[20] NMBA dosage is determined by the optimal body weight in order to avoid overdosing or chronic paralysis.[21]The Society of Critical Care Medicine Clinical Practice Guidelines for Rapid Sequence Intubation recommends administering in severely unwell adult patients, a neuromuscular blocking drug combined with a sedative-hypnotic induction agent. Improved first- pass intubation success (FPS) and decreased rates of respiratory arrest, cardiovascular collapse, and vomiting/aspiration have been shown in five trials. Prior to administering the NMBA, adequate sedation and analgesia should be established.[22]These dosages are basic suggestions and may need to be adjusted depending on specific patient characteristics and whether they are used in the ICU or during surgery. To ensure correct dosing, clinicians should consult the FDA-approved labeling for each medication and carefully examine the patient’s clinical state. This technique guarantees that medications are administered safely and appropriately, in accordance with best healthcare standards.
•Succinylcholine: 0.6 mg/kg, Maintenance: 0.04 to 0.07 mg/kg
•Atracurium: Initial bolus: 0.4 to 0.5 mg/kg, Maintenance: 0.08 to 0.1 mg/kg
•Cisatracurium: Initial bolus: 0.15 to 0.2 mg/kg, Maintenance: 0.03 mg/kg IV
•Rocuronium: Intubation (RSI): 0.6 to 1.2 mg/kg, Maintenance: 0.01 to 0.012 mg/kg/min
•Vecuronium: Initial bolus: 0.08 to 0.1 mg/kg, Maintenance:0.8 to 1.2 μg/kg/min
2.Intramuscular route (IM)
Neuromuscular blocking drugs (NMBAs) work by inhibiting the action of acetylcholine (Ach) at the neuromuscular junction (NMJ):
Mechanism of action:
Step 1: Absorption IM-administered NMBs are absorbed into the bloodstream through the muscle tissue.The rate of absorption depends on factors like muscle blood flow, dosage, and pH
Step 2: Distribution
Absorbed NMBs are distributed throughout the body via the bloodstream. They cross the blood- brain barrier and reach the neuromuscular junction (NMJ).
Step 3: Binding to Acetylcholine Receptors
NMBs bind to acetylcholine receptors (AChRs) on the postsynaptic membrane at the NMJ.This binding blocks the action of acetylcholine (Ach), the neurotransmitter responsible for muscle contraction.
Step 4: Competitive Blockade (Non-Depolarizing NMBs)
Non-depolarizing NMBs, like succinylcholine, competitively bind to AChRs. They prevent Ach from binding and triggering muscle contraction.
Step 5: Depolarizing Blockade (Depolarizing NMBs)
Depolarizing NMBs, like succinylcholine, depolarize the muscle membrane. This initial depolarization causes muscle contraction, followed by paralysis.
Step 6: Muscle Paralysis
As NMBs block Ach receptors, muscle contraction is prevented, leading to muscle paralysis. This paralysis is reversible, and muscle function returns once the NMB is metabolized or reversed.
Key Factors Influencing IM NMB Action
•Dose: The dose of NMB administered affects the degree of muscle paralysis.
•Muscle Blood Flow: Increased muscle blood flow enhances NMB absorption and efficacy.
•Duration of Action: Different NMBs have varying durations of action, ranging from short (e.g., succinylcholine) to long (e.g., pancuronium).Examples of IM NMBs Succinylcholine: Depolarizing NMB, used for rapid sequence intubation Vecuronium: Non-depolarizing NMB, used for general anaesthesia and surgical procedures.
3.Intraosseous Route (IO)
Intraosseous injection (io) is a technique recommended for both adult and pediatric patients in life- threatening situations where punctures cannot be made more than three times. The patient must be older or have circulatory collapse before vascular access can be achieved, and the infusion of liquids or medications cannot be delayed. Most commonly, it is used for shock patients who require blood, crystalloids, or colloids in cases of allergy, severe burns, obesity, status epilepticus, being imprisoned, dehydrated, having had repeated traumas, altered awareness, etc. It is a simple, accessible, and efficient approach that causes no trouble during insertion.[24] Adults should first consider the proximal humerus if there are distinct anatomical landmarks. According to recent research, we can achieve increased medication absorption, less pain during insertion, and higher infusion rates using this placement. Since fluids and drugs reach the right atrium in about three seconds, we may obtain flows of up to five liters per hour. The sternum, iliac crest, and distal and proximal tibia are the anatomical sites of insertion in adults. [25,26,27,28,29] The intraosseous route is an alternative to intravenous (IV) or intramuscular (IM) administration of neuromuscular blocking agents (NMBAs) in emergency situations:
Fast: It can provide parenteral access in 30–60 seconds. Safe: It has few complications.
Successful: It’s a simple, safe, and successful way to provide parenteral access in emergencies.
4.Transdermal Patch
One medication used to treat Alzheimer’s is rivastigmine, often known as Exelon. It is an acetylcholinesterase inhibitor (AChI) intended to boost central nervous system acetylcholine (Ach) and enhance memory. For the treatment of mild to severe Alzheimer’s disease, it was first approved in 2006, and a higher dose was approved in 2012.[30,31]. The medication comes in two forms: an oral version and a transdermal administration device, or “skin colored” patch, which worries anesthesiologists the most. The patch may remain in place for up to 24 hours, and anesthetic providers may not be aware of its presence because to the pathophysiologic memory loss associated with Alzheimer’s disease. It is widely known how AChI affects neuromuscular blocking (NMB) medications used in anesthesia.[32] In particular, a resistance to nondepolarizing NMBs and sensitivity to depolarizing (succinylcholine) NMBs may arise from the increased Ach that results from the inhibition of acetylcholinesterase. The most urgent safety concern is the possibility of unanticipated patient movement if this drug interaction is originally overlooked. AchI can have a significant impact on the dose, monitoring, and eventual reversal of NMBs.Researchers are exploring new routes of administration for neuromuscular blockers (NMBs), including:
5.Nasal
Administering NMBs intranasally, which can lead to faster onset of action and reduced systemic side effects.Not only is it painless and convenient, but it also doesn’t decrease the bioavailability of medications when inhaled.[33] The nose-brain pathway’s direct delivery to the cerebrospinal fluid shorten the onset time. Low molecular weight, highly lipophilic medications readily penetrate the nasal mucosa.[34,35,36,37] Neither carrier coupling nor therapeutic drug change are necessary.[33] Use 0.25–0.3 ml of concentrated medication per nostril to prevent runoff. One of the drawbacks is that absorption may be compromised in patients with bloody noses or elevated mucus production. Absorption of intranasal medication takes around 3–5 minutes, and respiratory depression is rarely caused by drug levels reached. Sufentanil is an exception, though, as toxic concentrations can rise quickly.[38]
6.Inhalational:
Developing inhalational NMBs that can be administered via inhalation, potentially reducing the risk of respiratory depression.System of pulmonary medication deliveryFor the administration of drugs into the lungs, nebulizers, dry powder inhalers, and metered dose inhalers are utilized.[39] They have more surface area and are nearer the blood flow, among other benefits.[39,40] Systemic toxicity can be prevented by using lower doses. However, the period is shorter and only 10–40% of the medications supplied become available for systemic absorption; nanoparticles have been produced to get around this restriction. The inhalation route has been the persistent target for opioid delivery efforts.[41] When fentanyl is delivered in this way, its bioavailability has been determined to be 20%.[42,43] Iloprost is a more recent prostacyclin analog that is used to treat pulmonary hypertension; however, because of its short half-life, it needs to be taken often.Therefore, an aerosolized controlled release formulation is a viable option to enhance patient compliance.[38,44,45] There are further physiological components to the utilization of colloidal carrier systems in pulmonary DDS.[46] With the use of carriers and better technology, medications for inhaled insulin, asthma, and specific lung infections are also being produced.[47,48]
7.Intra-Articular
The size of the drug molecule has to be 3–5 μ. The residence time of drugs in intra-articular tissues may be prolonged by microspheres that are designed to improve their uptake by the synovium.[49]
8.Mucosal Buccal Delivery
It prevents presystemic removal and the first pass effect in addition to being simple to administer.[50,51] Significantly less toxicity or undesirable side effects occur. This method can be used to deliver medications for breakthrough pains and chronic pain management, such as buprenorphine hydrochloride tablets and fentanyl lozenges, tablets, and films [52]. Sublingual drug administration has a more dramatic beginning, whereas the buccal mucosa has a more gradual onset and is better suited for sustained release preparations due to its vast immobile surface and lesser permeability. [53,54,55]
9.Subcutaneous:
Investigating subcutaneous administration of NMBs, which may provide a more rapid onset of action than intramuscular injection.
10.Microdosing:
Exploring the use of microdoses of NMBs, which may reduce side effects and improve safety.
11.Targeted Delivery:
Developing targeted delivery systems, such as nanoparticles or liposomes, to specifically deliver NMBs to the neuromuscular junction, reducing systemic side effects. Due to partial degradation, conventional DDS may cause medication potencies to decrease before they reach the body’s target tissues. Deploying the active pharmaceutical compound to the specific targeted locations of the body is the aim of any DDS. The last ten years have seen the development of polymeric micelles, microspheres, and other materials that effectively reduce systemic drug toxicity, improve the drugs’ ability to target particular sites, increase absorption rates, and delay the drug’s biochemical breakdown before it reaches the intended site. Liposomes are nanovesicles with a phospholipid bilayer encasing them. They are good drug delivery vehicles since they are nontoxic, biodegradable, and immunegenic. While liposomal medications have made significant strides in the treatment of cancer, anesthetic drug efficiency can also be improved. Early recovery after surgery depends on a multimodal strategy to postoperative pain treatment. The comparatively short duration of action and potential for systemic toxicity of the variety of local anesthetics on the market are two of their main drawbacks.An significant development in the administration of local anesthetic formulations is liposomal bupivacaine.[56] With a delay in peak plasma concentrations, a single dosage can result in a therapeutically active concentration for up to 96 hours.[57] However, before field blocks can be employed in clinical practice, phase 3 trials must be completed.[57] DepoDur, a liposomal version of epidural morphine, offers analgesia for up to two days.[59,60] This was also verified with extended release morphine in a study conducted by Viscusi et al.[60] Additionally, liposomally encapsulated inhaled fentanyl with an intravenous preparation-like start of action is being investigated.[61]
10.Transient Targeted Thromboprophylaxis
Thromboprophylaxis during the initial postoperative phase has consistently been a murky topic. During the postoperative phase, when the patient is immobile, bleeding is a genuine risk, and thrombosis risk is also at its peak. Tissue plasminogen activator (tPA)-coated flow-sensitive nanoparticles that release tPA at the clot site make up the innovative DDS for thromboprophylaxis. [63,64,65,66,67]
11.Electrophoretic: Using electrophoresis to deliver NMBs through the skin, potentially increasing bioavailability and reducing side effects.These new routes of administration aim to improve the safety, efficacy, and patient experience of NMBs. However, further research is needed to overcome the challenges associated with these novel delivery methods.
ADVANTAGES
•Improved patient comfort: Reduced pain and discomfort associated with injections.
•Increased convenience: Easier administration and reduced need for medical professionals.
•Reduced side effects: Targeted delivery and lower doses may minimize systemic side effects.
•Faster onset: Some new routes may lead to faster onset of action.
Applications of Drug Delivery Systems:
•Nanoparticles
•Hydrogels
•Colloidal drug carrier
•3D printing
•Phytosomes
•Injectable in situ-gelling systems
The use of nanoparticles as therapeutic and diagnostic agents, as well as to improve medication delivery, is crucial and urgent for a number of reasons. One of them is that, standard medications available presently for oral or injectable administration are not always made as the ideal formulation for each product. To increase their effectiveness and shield them from unintended breakdown, products comprising proteins or nucleic acids need a more creative kind of carrier system [68] Notably, particle size directly affects the majority of drug delivery modalities’ efficiency (with the exception of intravenous and solution). Drug nanoparticles have increased solubility and, consequently, greater bioavailability, as well as the ability to cross the blood-brain barrier (BBB), enter the pulmonary system, and absorb through cutaneous endothelial cells’ tight connections. These effects are attributed to their tiny size and huge surface area.[69] Another method for delivering chemotherapy drugs is by the use of liposomes and micellar particles. Additionally, because of its hydrophobic core and hydrophilic exterior, micelles are a wonderful way to make medications that are intractable soluble. Higher drug concentrations in tumors can be achieved if the micelle’s surface is further PEGylated, since this will improve the nanocarriers’ capacity to passively carry drugs through the fenestrated vasculature of tumors and inflammatory tissue. Clinical trials are now being conducted on a number of polymeric micelles carrying anticancer medications, including NK012, NK105, NK911, NC-6004, and SP1049C. [70]and one such system, approved for use in treating breast cancer patients, is Genexol-PM (paclitaxel)[71] The absorption, distribution, metabolism, and elimination (ADME) profile of dendrimers—which are highly branched macromolecules with numerous functional groups available for the attachment of drug, targeting, and imaging agents—depends on an assortment of structural elements.[72,73]According to[74] a polyfunctional dendrimer system has been successfully used for methotrexate delivery, imaging, and localization (using fluorescein). By utilizing biocompatible components and surface derivatization with PEGylation, acetylation, glycosylation, and different amino acids, dendrimer-based nanoparticle therapies can enhance the therapeutic index of cytotoxic medications [75]
A hydrogel is a biphasic substance that consists of a mixture of solids that are permeable and porous, and at least 10% of the weight or volume of the interstitial fluid is made up entirely or mostly of water.[76][77] The porous permeable solid in hydrogels is a three- dimensional network of natural or synthetic polymers that is insoluble in water and fluid that has absorbed a significant volume of biological or water-based fluids.[77][78][79][80] Numerous applications, particularly in the biological field, are supported by these qualities. While most hydrogels are artificially made, some are naturally occurring.[81][82] ‘Hydrogel’ was first used in 1894.[83]
•Water sustainability: Hydrogels have become a viable material platform for water disinfection, atmospheric water generation, and solar-powered water purification [84,85,86]
•When they absorb pee, use disposable diapers or sanitary napkins [87]
•Dressings for burns and other difficult-to-heal wounds. Gels for wounds work wonders in creating and preserving a damp atmosphere.
•Hydrogels made of cross-linked polymers (polyethylene oxide, polyAMPS, and polyvinylpyrrolidone) are used in EEG and ECG medical electrodes.
•Quantum dot encapsulation
•Hydrogels that are responsive to the environment (sometimes called “smart gels” or “intelligent gels”). These hydrogels can detect changes in pH, temperature, or metabolite concentration and release their load in response to such changes. [88,89,90]
•Air bubble-repellent (superaerophobicity). Can improve the performance and stability of electrodes for water electrolysis.[91]
•Culturing cells: Hydrogel-coated wells have been used for cell culture.[92]
•Biosensors: Hydrogels that are responsive to specific molecules,[93] such as glucose or antigens, can be used as biosensors, as well as in DDS.[94]
•Cell carrier: Injectable hydrogels can be used to carry drugs or cells for applications in tissue regeneration or 3D bioprinting. [95,96,97]
•Hydrogels with reversible chemistry are required to allow for fluidization during injection/printing followed by self-healing of the original hydrogel structure.[98]
•Scaffolds for tissue engineering. Hydrogels containing human cells can be utilized as scaffolds to heal tissue. They imitate the 3D cellular microenvironment.[99] Materials include polymers produced from nature, agarose, methylcellulose, hyaluronan, and polypeptides similar to elastin.
3.Colloidal drug Carrier
Colloidal drug carriers are nanoscale systems that improve drug delivery by enhancing solubility, stability, and targeting. Applications in drug delivery systems include:
Types of Colloidal Carriers:
1.Liposomes
2.Nanoparticles (polymeric, metallic, ceramic)
3.Micelles
4.Dendrimers
5.Nanoemulsions
6.Nanocapsules
7.Solid Lipid Nanoparticles (SLN)
Applications:
•Cancer therapy (targeted delivery, reduced side effects)
•Infectious diseases (antibiotic delivery, vaccine adjuvants)
•Neurological disorders (blood-brain barrier crossing)
•Ophthalmic diseases (sustained release, targeted delivery)
•Pulmonary diseases (inhalable nanoparticles)
•Cardiovascular diseases (targeted delivery, improved solubility)
•Gene therapy (efficient DNA/RNA delivery)
Challenges and Future Directions:
•Scalability and manufacturing
•Stability and storage
•Toxicity and biocompatibility
•Regulatory approvals
•Clinical translation
Examples
•Doxil (liposomal doxorubicin)
•Ambisome (liposomal amphotericin B)
•Abraxane (nanoparticle albumin-bound paclitaxel)
•Rapamune (nanoparticle-based sirolimus)
•Nano Therm (nanoparticle-based thermal ablation)
4.3D printing
The use of additive manufacturing by scientists working in the pharmaceutical industry has grown. But scientific interest in 3D medication delivery applications increased even more following the FDA’s initial approval of a 3D printed formulation. Many approaches to include medications in a 3D printed formulation are being investigated by research groups worldwide. One such approach is the incorporation of weakly water-soluble drugs in emulsion gels or self- emulsifying systems. Scientists may create formulas using a personalized approach—that is, dose forms made especially for each patient—thanks to 3D printing technology. Furthermore, formulations with different qualities can be achieved based on the benefits of the various approaches used. These could have multi-compartmental designs, drug delivery systems with different release characteristics, numerous medications in a single dosage form, etc.[100,101,102,103,104] Fused Deposition Modelling (FDM) has been the primary focus of study in the past few years. These days, additional printing methods including semi-solid extrusion (SSE), stereolithography (SLA), and selective laser sintering (SLS) are becoming more popular and are being used to pharmaceutical applications.[105][106]
5.Phytosomes
Phytosomes represent a novel approach in drug delivery systems, enhancing the bioavailability and therapeutic efficacy of plant-derived compounds. By complexing standardized plant extracts with phospholipids, phytosomes improve solubility and facilitate cellular absorption, making them a promising alternative to traditional formulations. Enhanced Bioavailability Phytosomes significantly increase the bioavailability of poorly soluble phytoconstituents, such as flavonoids and terpenoids, by forming lipid-compatible complexes[107][108].This technology allows for better absorption and stability, addressing the limitations of conventional herbal formulations[109].
Applications in Cancer Therapy
Phytosomes have shown potential in cancer treatment by enabling targeted drug delivery of bioactive compounds, enhancing their therapeutic effects while minimizing side effects[110].Several phytosomal formulations are currently undergoing clinical trials, indicating their growing relevance in oncology[110].
Versatile Formulation Techniques
The preparation of phytosomes is straightforward, utilizing techniques like FTIR and SEM for characterization [108]. They can be integrated into various drug delivery systems, including liposomes and ethosomes, expanding their application scope[111].While phytosomes offer significant advantages in drug delivery, challenges such as scalability and regulatory hurdles remain, necessitating further research to optimize their use in clinical settings.
Injectable in situ-gelling systems
Injectable in situ gelling systems are revolutionizing drug delivery across various medical fields, offering sustained release and improved patient compliance. These systems transition from a liquid to a gel state upon administration, allowing for localized and prolonged drug action.
Long-Acting Injectable Systems
The development of enzyme-responsive peptoid-peptide hydrogels enables sustained drug release, demonstrated by a model drug, zidovudine, maintaining therapeutic levels for 35 days post-injection [112] This system minimizes initial drug bursts, enhancing therapeutic efficacy and patient adherence.
Ocular Drug Delivery
In situ gelling systems significantly improve ocular drug delivery by prolonging the residence time of drugs on the eye surface, thus enhancing bioavailability and reducing systemic absorption [113][114].These systems utilize innovative polymers to ensure effective drug release while minimizing side effects associated with frequent dosing.
Chemotherapeutic Applications
In situ gelling systems for chemotherapeutic agents allow for targeted delivery with controlled release, improving patient quality of life by reducing the need for frequent administration [115] While these systems present numerous advantages, challenges such as the need for further clinical validation and potential complications from implantation techniques remain critical considerations in their development.
CONCLUSION
Modern anesthesia relies heavily on neuromuscular blocking agents (NMBAs), which effectively relax muscles and make surgical procedures easier. Optimizing patient outcomes requires a thorough understanding of the pharmacological characteristics, mechanisms of action, and optimum dose of both depolarizing and non-depolarizing NMBAs. Health care providers can improve the safety and effectiveness of muscle relaxation techniques during surgery by carefully evaluating the features of the patient and the usage setting. In addition, promoting interprofessional cooperation is essential to provide all-encompassing treatment and raising the bar for general anesthetic practice standards. This training course gives medical staff the skills they need to apply NMBAs successfully, which will eventually improve surgical outcomes and patient care on an individual basis
Abbreviations:
NMBs- Neuromuscular blockers
ACH- Acetylcholine
IO- Intraosseous
IP- Intraperitoneal
FPS- First pass intubation success
DDS- Drug delivery systems
SLN- Solid liquid nanoparticle FDM- Fused Deposition modeling SSE- Semi solid extrusion
SLA- Stereo lithography
FTIR- Fourier transform infrared
SEM- Scanning electron microscopy
REFERENCES


Tanvi Dhapkas*, Vaishnavi Satghode, Dr. Sandeep Atram, Neuromuscular Blocking Agents, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 2520-2542 https://doi.org/10.5281/zenodo.15087055
 10.5281/zenodo.15087055
10.5281/zenodo.15087055