1,2,3,4 Dr. Shivajirao Kadam College of Pharmacy, Kasabe Digraj, Sangli, Maharashtra, India.416305
5 Shri. Ambabai Talim Sanstha’s, Diploma In Pharmacy College, Miraj, Maharashtra, India.416410
The treatment of a variety of ocular disorders affecting the anterior and posterior regions of the eye as well as the ocular surface still relies heavily on corticosteroids. They possess strong anti-inflammatory, anti-edematous, and anti-angiogenic qualities that contribute to their therapeutic effects. Ophthalmic corticosteroids such as loteprednol etabonate, triamcinolone acetonide, fluocinolone acetonide, dexamethasone, prednisolone, and prednisolone acetate are frequently used. The ocular efficacy and potency of these agents vary because of their inherent pharmacological and medicinal properties. Corticosteroid delivery in ophthalmology can be optimized using a range of administration methods and regimens. For conditions that only affect the ocular surface and anterior portion, topical treatment is still the recommended method. Conversely, to better treat posterior segment diseases, periocular, intravitreal, and suprachoroidal injections are used. But there are hazards associated with corticosteroid medication. Notable local side effects linked to topical and systemic corticosteroid use include cataract development and elevated intraocular pressure. Invasive delivery techniques, like intracameral, subconjunctival, and intravitreal injections, can lower the frequency of dose and greatly increase ocular absorption, but they may also raise the risk of problems from steroids. The therapeutic uses of corticosteroids in ophthalmology are critically examined in this review, with particular attention paid to drug delivery principles, delivery routes, new implantable steroid systems, what influences side effects, and developing methods for safer and more efficient ocular corticosteroid therapy.
The pharmacological effects, therapeutic indications, methods of administration, innovative drug delivery systems, adverse effect profiles, and future prospects of corticosteroids in ophthalmology are all covered in detail in this study. Optimizing the use of corticosteroids has grown more and more important for ophthalmologists, pharmacists, pharmaceutical scientists, and other healthcare professionals as the prevalence of eye illnesses rises worldwide. Synthetic versions of natural glucocorticoids, corticosteroids work to reduce inflammation through a variety of processes. Pro-inflammatory gene expression is suppressed, anti-inflammatory protein synthesis is increased, cytokine production is inhibited, leukocyte infiltration is prevented, vascular permeability is decreased, and cellular membranes are stabilised. Their main mechanism of action is the glucocorticoid receptor pathway, which involves both transactivation and transrepression mechanisms that alter nuclear-level gene transcription. Corticosteroids are commonly used in clinical settings to treat eye disorders of the anterior and posterior segments. In the anterior segment, they are recommended for disorders such corneal transplant rejection, ocular surface damage, scleritis, episcleritis, dry eye syndrome, anterior uveitis, postoperative inflammation, and allergic conjunctivitis. In order to treat vision-threatening conditions related to posterior segment disorders, such as diabetic macular oedema (DME), age-related macular degeneration (AMD), diabetic retinopathy (DR), non-infectious posterior uveitis, macular oedema secondary to retinal vein occlusion, and postoperative cystoid macular oedema, corticosteroids are necessary.[1, 2] Prednisolone/prednisolone acetate, triamcinolone acetonide, loteprednol etabonate, difluprednate, fluocinolone acetonide, fluorometholone, and dexamethasone are among the commonly used ocular corticosteroids. Pharmaceutical versions of these drugs include eye drops (solutions, suspensions, and emulsions), ointments, gels, and long-acting implants. Whether topical, systemic, periocular (subconjunctival, sub-Tenon's, retrobulbar) or intraocular (intravitreal), the choice of formulation and administration method is contingent upon the targeted ocular tissues, the degree of inflammation, the drug's pharmacokinetics, and the intended balance between local and systemic effects. Corticosteroid treatments are now far more accurate, long-lasting, and safe thanks to recent developments in ocular drug delivery technologies. In situ-forming gels, punctal plugs, liposomes, nanoparticles, microparticles, and intravitreal implants are examples of innovative systems that have enhanced treatment results. Biodegradable implants (like the dexamethasone intravitreal implant) and non-biodegradable devices (like the fluocinolone acetonide insert) are examples of sustained-release systems that provide extended medication release over a period of weeks to months. Patients' adherence to treatment is improved and frequent dosing is lessened because to these advances. Long-term use of corticosteroids is associated with substantial limits, despite the fact that they offer major therapeutic advantages in ophthalmic therapy. Serious ocular side effects, including elevated intraocular pressure (IOP), steroid-induced glaucoma, posterior subcapsular cataracts, increased susceptibility to eye infections, and delayed wound healing, can result from prolonged treatment. A patient's sensitivity, the dosage, the length of treatment, and the particular corticosteroid molecule all affect the frequency and intensity of these adverse effects. [3, 4] Pharmaceutical research is now placing more and more emphasis on creating safer, site-specific, and sustained-release delivery systems in order to maximise therapeutic benefits and reduce side effects. This study explores the clinical pharmacology of ophthalmic corticosteroids, assesses the difficulties presented by ocular barriers to drug penetration, and critically looks at existing approved drug delivery modalities. Furthermore, it investigates new approaches to enhance the corticosteroid therapy's efficacy-to-toxicity balance. Promising developments that will help develop the next generation of ocular therapies include gene therapy, microneedle-based delivery, stimuli-responsive formulations, and bioengineered implants. To accomplish these objectives and guarantee the safe and efficient use of corticosteroids in ophthalmology, pharmacologists, formulation scientists, and clinicians must work together in a multidisciplinary manner, as shown in Figure 3. [5, 6]

Figure 1 Various ocular surface, anterior and posterior eye diseases that can be treated with corticosteroids
Corticosteroids: structure and physicochemical properties
Every corticosteroid has the same core sterane structure, which is made up of four fused rings of 21 carbon atoms. This backbone can be structurally altered to produce derivatives with different biological potencies and unique physicochemical characteristics. Their therapeutic effectiveness in ocular applications is largely determined by important properties such solubility, formulation types, and the log partition coefficient (log P). A hydroxyl group at the C17 α-position, a C4–C5 double bond, a ketone group at C3, and an oxygen-containing functional group at C11 are the structural characteristics associated with the anti-inflammatory effect of the majority of corticosteroids. By lowering degradation, the addition of a C1–C2 double bond, as in prednisolone, increases metabolic stability. The anti-inflammatory effectiveness of triamcinolone is increased by fluorination at the C9 site. Fluticasone furoate and mometasone furoate are examples of strong corticosteroids that have a furoate ester added at the C17 α-position, which also boosts the glucocorticoid receptor binding affinity. Prednisolone acetate, a prodrug created by replacing the C21 hydroxyl group in prednisolone with an acetate group, has improved corneal penetration and increased lipophilicity in comparison to its parent molecule and phosphate salt. The addition of an acetonide group at locations C16 and C17 also makes molecules like triamcinolone acetonide and fluocinolone acetonide more lipophilic. Because corticosteroids are often poorly soluble in water, they are made with a variety of administration methods other than simple solutions. Solutions, suspensions, emulsions, gels, ointments, and implants are among the commercially available forms of ophthalmic corticosteroid medications. With 0.5% w/v carboxymethyl cellulose, the solubility trend in phosphate-buffered saline is as follows: prednisolone (0.243 mg/mL) > dexamethasone (0.16 mg/mL) > fluocinolone acetonide (0.05 mg/mL) > triamcinolone acetonide (0.021 mg/mL). Because of the acetonide group, fluocinolone acetonide is notably less soluble than dexamethasone, by just around 4%. Water solubility is greatly increased by adding a phosphate group at C21, which permits the production of sodium ions. [7, 8] Corticosteroids are categorised as either water-soluble or poorly water-soluble based on their solubility. Examples that dissolve in water include prednisolone sodium phosphate and dexamethasone sodium phosphate, both of which are commonly prepared as eye drop solutions. Prednisolone, prednisolone acetate, triamcinolone acetonide, and fluocinolone acetonide, on the other hand, are poorly soluble corticosteroids that are typically administered as emulsions or suspensions. Because of the hydroxyl groups at positions X17 and R21, dexamethasone is thought to be rather water soluble. A proven treatment for a number of inflammatory disorders of the eyes is the intravitreal injection of triamcinolone acetonide. Bristol Myers Squibb's injectable triamcinolone acetonide, Kenalog®-40, has been used extensively off-label in ophthalmology but is not authorised for intraocular usage. Its formulation contains benzyl alcohol, a preservative that has been associated with a small number of clinically relevant instances (~1%) of sterile endophthalmitis. This is probably because of its ability to irritate the eyes. The European Union does not advise its intraocular usage as a result. These issues were addressed by the development and approval of preservative-free formulations for intravitreal injection, such as Triesence® and Trivaris®, which offer safer substitutes for intraocular delivery. [9, 10]
Solubility and Classification of Corticosteroids
A basic physicochemical characteristic of corticosteroids, solubility has a major impact on their formulation design, mode of administration, pharmacokinetics, and therapeutic efficacy in ophthalmology. Due in significant part to structural elements such the existence of polar functional groups, halogen atoms, and ester modifications, these drugs' water solubility varies greatly. [11] At room temperature, the water solubility of commonly used ophthalmic corticosteroids decreases in the following order:
This broad range of solubility demonstrates how fluocinolone acetonide has very poor water solubility (about 4% of that of dexamethasone). Because of the hydrophobic acetonide group, which reduces the compound's polarity and affinity for aquatic environments, the solubility is largely reduced. Commonly used chemical changes, such as phosphate esterification at the C21 hydroxyl position, are used to overcome these solubility restrictions. Water-soluble corticosteroid derivatives such as dexamethasone sodium phosphate and prednisolone sodium phosphate are produced by this method; these are usually prepared as clear ophthalmic solutions and easily separate into ionic forms in water. Because of their immediate onset of action and rapid corneal penetration, these formulations are perfect for treating acute inflammatory diseases.[12] Based on solubility characteristics, corticosteroids used in ophthalmology can be broadly classified into two categories:
1. Water-Soluble Corticosteroids
Examples include:
Since they are mainly made as aqueous eye drops, they are convenient for frequent usage. However, their brief residence durations on the ocular surface are frequently caused by quick precorneal clearance, which limits their therapeutic duration. [13]
2. Poorly Water-Soluble Corticosteroids
Examples include:
The most common ways to administer these corticosteroids are as ointments, emulsions, or suspensions. Because of its reduced solubility, the medicine is better retained at the ocular surface and its therapeutic action is prolonged. Crucially, their solubility profile also makes them perfect for formulations with prolonged release. [14]
Sustained-Release Applications
Poorly water-soluble corticosteroids are widely used in long-acting injectable or implantable delivery systems for chronic ocular diseases. Examples include:
These sophisticated methods reduce the frequency of injections and enhance patient adherence by utilising the corticosteroid's inherent low solubility to provide slow, controlled diffusion. However, during development, formulation issues must be resolved, including possible drug crystallisation, dosage uniformity, and long-term stability. [15, 16]
Pharmacological Role of Corticosteroids in Ocular Inflammation
Serious side effects, such as vision impairment and irreversible vision loss, can result from untreated ocular inflammation. Increased local blood flow and immune response activation triggered by different pro-inflammatory mediators are common characteristics of this syndrome. Pain, swelling, itching, and redness are typical clinical signs.
For more than 50 years, corticosteroids have been a cornerstone in the treatment of ocular inflammation. The systemic infusion of adrenocorticotrophic hormone (ACTH), which shown notable efficacy in treating uveitis, marked the beginning of their use. Since then, corticosteroids have been used extensively because of their strong immunosuppressive and anti-inflammatory effects. They target important inflammatory pathways and mediate their therapeutic effects through a variety of mechanisms. Corticosteroids reduce pro-inflammatory mediators, suppress cytokine and matrix metalloproteinase activity, and prevent the formation of eicosanoids. [17] Corticosteroids act via two principal mechanisms: genomic and non-genomic pathways.
Genomic Mechanism
In the genomic pathway, corticosteroids enter target cells and bind with high affinity to cytosolic glucocorticoid receptors (GRs). The resulting corticosteroid-GR complex trans locates into the nucleus, where it modulates gene transcription. [18] This results in:
Non-Genomic Mechanism
The non-genomic effects of corticosteroids occur more rapidly and are independent of gene transcription. These include:
Anti-Angiogenic Effects
Apart from their anti-inflammatory capabilities, corticosteroids also have anti-angiogenic qualities, which are especially advantageous in retinal conditions including diabetic macular oedema (DME) and age-related macular degeneration (AMD). Through downregulating VEGF expression, they prevent pathological neovascularisation and aid in stabilising the blood-retinal barrier. Fluocinolone acetonide, for instance, has shown in animal models that it can suppress angiogenesis that is triggered by VEGF and tumour necrosis factor-alpha (TNF-α). [19]
Ocular Administration Routes and Pharmacokinetics
The choice of administration route for corticosteroids in ophthalmology is largely dictated by the target site within the eye. While topical application is preferred for anterior segment conditions due to its ease and reduced systemic effects, treating posterior segment diseases often necessitates alternative delivery approaches to achieve sufficient intraocular concentrations. [20]
Topical Administration
Topical distribution, mostly in the form of eye drops, is a patient-friendly, non-invasive technique that offers high local drug concentrations with little systemic absorption. Its efficacy is mostly limited to disorders of the anterior segment, though, because anatomical constraints make it difficult to achieve therapeutic levels in the posterior section. The cornea, which serves as the primary barrier, prefers medications with the ideal ratio of hydrophobicity to lipophilicity. When it comes to corneal permeability, lipophilic corticosteroids like prednisolone acetate and dexamethasone alcohol are superior to their hydrophilic counterparts, such as sodium phosphate salts. Cyclodextrins are one formulation technique that has been used to improve the solubility and corneal penetration of poorly soluble medications, such as dexamethasone. Improved penetration, however, may also raise dangers like increased intraocular pressure (IOP) and the reactivation of ocular diseases, especially the herpes simplex virus. In experimental models, new methods for delivering medications to the posterior segment, like topical nanocarrier systems loaded with beclomethasone dipropionate, have showed promise (see Table 1) [21, 22]
Systemic Administration
Oral or intravenous corticosteroid administration is usually used for severe inflammatory disorders or posterior segment diseases when topical treatments are insufficient. The blood-aqueous and blood-retinal barriers, on the other hand, severely limit the drug's ability to enter ocular tissues, requiring larger systemic dosages and raising the possibility of systemic adverse effects like immunosuppression, cataracts, and glaucoma. For example, systemic prednisolone treatment only produces roughly half of the aqueous humour concentration that topical application achieves. Comparing intramuscular methylprednisolone versus particular injections, the former results in significantly lower ocular drug levels. Notwithstanding these disadvantages, systemic corticosteroids continue to be essential for treating diseases such as severe uveitis, corneal graft rejection, and ocular illness associated with IgG4 (see Table 1) [23, 24]
Subconjunctival Injection
Through subconjunctival injection, corticosteroids are administered beneath the conjunctiva, allowing the medication to spread over the sclera and avoid the conjunctival epithelium. This approach permits bigger injected volumes than other periocular channels and enables higher local drug concentrations than systemic delivery. With lipophilic corticosteroids like triamcinolone acetonide, it works exceptionally well for prolonged drug release. However, when it comes to treating superficial ocular irritation, subconjunctival distribution is typically less successful than eye drops, and systemic absorption or reflux may cause some medication loss. The dangers associated with this method include ocular discomfort, globe perforation, retinal detachment, and granuloma formation, despite the fact that it is usually well tolerated. Notwithstanding these reservations, subconjunctival injections are nevertheless a useful method for producing corticosteroid action in ocular tissues for an extended period of time (see Table 1). [25]
Table 1 Corticosteroid implants and suspensions approved for intravitreal injection
|
Corticosteroid member
|
Dosage form |
Route of administration |
Clinical uses |
Main advantages |
Major (> 10%) adverse effects |
Duration of Therapy |
References |
|
Fluocinolone acetonide |
Retisert® (0.59 mg) |
Implanted surgically into the posterior segment of the eye |
Chronic non-infectious uveitis |
Much longer therapy than Ozurdex® |
Elevation of IOP Cataract Ocular |
Up to 30 months |
20 |
|
Fluocinolone acetonide |
Iluvien® (0.19 mg) |
Intravitreal implant |
Diabetic macular edema |
Does not require sutures |
Cataract (82%) Myodesopsia (21%) |
Up to 36 months |
12 |
|
Triamcinolone acetonide |
Triesence® 40 mg/ml |
Intravitreal injection (25-100μl per single injection) |
Ocular inflammatory condition |
Simple needle injection |
Elevated IOP |
Intravitreal injection every 3-4 weeks |
11 |
|
Dexamethasone |
Ozurdex® (0.7 mg) |
Intravitreal implant |
Macular edema |
Long-acting device with less repeated intravitreal injections |
Elevated IOP (25%) |
Up to 6 months |
9 |
Retrobulbar Injection
A medicine is injected into the intraconal space, which is behind the globe and inside the muscle cone made up of the rectus muscles, in a procedure known as retrobulbar administration. This method minimises systemic exposure while providing direct access to the posterior part of the eye, allowing for high drug concentrations in the retina and surrounding tissues. The retrobulbar route is frequently used in clinical practice to provide anaesthetics during eye procedures since it may administer relatively high amounts. Compared to systemic methods, retrobulbar injection provides clear pharmacokinetic benefits for corticosteroid administration, resulting in noticeably greater retinal drug levels. Preclinical research has shown that, in contrast to systemic intramuscular delivery, which is unable to sustain detectable intraocular drug levels over the same time period, corticosteroids delivered by retrobulbar injection remain detectable in retinal tissues for several days. These results highlight the improved ocular penetration and long-lasting therapeutic impact of retrobulbar injection. But even when the surgery works, there are risks involved. The main worry is that the injection needle may cause damage to the optic nerve, particularly if it is inserted too deeply. To reduce difficulties and guarantee patient safety, precise anatomical knowledge and cautious technique are therefore crucial (see Table 3 for summarised data). [26, 27]
Sub-Tenon Injection
A medication is injected into the possible gap between Tenon's capsule and the sclera during a sub-Tenon injection. In addition to giving corticosteroids to treat posterior segment inflammatory disorders such macular oedema and non-infectious uveitis, this method is frequently utilised to deliver local anaesthesia during ocular procedures. Triamcinolone acetonide, the corticosteroid most commonly used in this manner, has shown good therapeutic results with a low rate of side effects, including a lower risk of elevating intraocular pressure (IOP) than alternative delivery modalities. Retinal oedema can be efficiently reduced by both intravitreal and sub-Tenon injections; however, intravitreal delivery typically results in a higher morphological improvement. [28] Sub-Tenon injection is still a good substitute, nevertheless, particularly for patients who don't respond to or are incapable of handling intravitreal anti-VEGF treatments. Sub-Tenon administration appears to have a better safety profile with fewer serious side effects while lowering VEGF expression and retinal thickness. This makes it a crucial modality for the individualised treatment of retinal disorders (summarised comparisons are shown in Table 3). [29, 30]
Intraocular Injection
Corticosteroids can be delivered directly into the eyes, avoiding the ocular barriers that frequently reduce the efficacy of topical or systemic administration. Although there are inherent hazards associated with the injection process as well as the pharmacologic effects of corticosteroids, this method is quite effective for treating localised eye disorders. Increased susceptibility to ocular infections, delayed wound healing, cataract development, and high intraocular pressure (IOP) is all possible side effects of corticosteroids. Pain, unintentional globe damage, retinal detachment, bleeding, and different forms of endophthalmitis are some of the procedural dangers connected to injections.
A number of methods, including injections into the anterior chamber, vitreous cavity, or suprachoroidal area, can be used to provide intraocular corticosteroids. [31, 32] Table 3 summarises the advantages, disadvantages, and hazards of these routes.
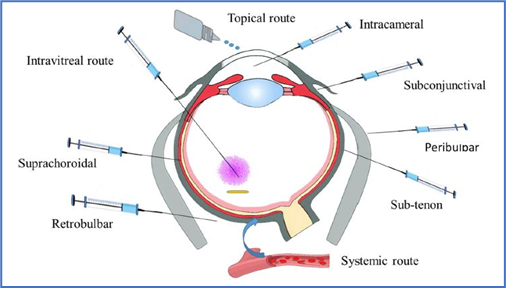
Figure 2 Routes of administration for ocular delivery of corticosteroids
Suprachoroidal Route
An inventive method of delivering medications straight to the back of the eye, the suprachoroidal space (SCS), minimises exposure to anterior structures like the cornea and lens, and targets the choroid and retina. Common negative effects associated with corticosteroid use, including as cataract development and increased intraocular pressure, are lessened by this tailored distribution. Up to 200 microlitres is the maximum injection volume that the SCS can handle; going over this could result in issues like oedema or choroidal separation. A substantial decrease in systemic absorption and anterior segment exposure results from the drug's localisation within the suprachoroidal compartment. A well-known illustration of this strategy is a suspension of triamcinolone acetonide that is intended for suprachoroidal injection and is authorised in a number of nations to treat macular oedema linked to uveitis. [33] According to animal research, there is a lesser chance of negative consequences from corticosteroid use since there are higher drug concentrations in the posterior ocular tissues and less in the anterior chamber. Serious side effects, like elevated intraocular pressure or systemic reactions, are uncommon, and only mild ocular pain has been recorded in human clinical studies, indicating good tolerance. In order to enable minimally invasive suprachoroidal injections, current research is investigating microneedle technology. Retinal detachment and haemorrhage are among the consequences that these microneedles have avoided, and the injection site usually seals in an hour or so. [34, 35]
Retrobulbar Route of Drug Administration
By injecting medicine into the muscle cone behind the eyeball—an anatomical region bounded by the rectus muscles and their intramuscular septa—the retrobulbar route is used. Drugs are mostly delivered to the posterior portion of the eye using this technique, which limits systemic exposure while producing high local drug concentrations. It is also frequently used to give anaesthesia during eye procedures; the usual injection volume is up to 5 millilitres. Retrobulbar injections have been shown to be effective in sustaining long-term medication levels in ocular tissues in animal investigations. In contrast to systemic treatment, which did not result in detectable ocular levels, corticosteroids given to monkeys via the retrobulbar route remained detectable in retinal tissues for up to nine days after injection. According to these results, the enhanced penetration and extended retention provided. [36]
Table 2 Relative anti-inflammatory properties of certain ocular corticosteroids
|
Corticosteroid agent |
Relative anti-inflammatory potency |
|
Hydrocortisone |
1 |
|
Prednisolone/prednisone |
4 |
|
Methyl prednisone |
5 |
|
Triamcinolone |
5 |
|
Fluocinolone acetonide |
25 |
|
Betamethasone |
25 |
|
Dexamethasone sodium phosphate |
25 |
Intravitreal Route of Drug Delivery
Conditions of the posterior eye, including posterior uveitis and macular oedema, are frequently treated with intravitreal injections. This method avoids physiological barriers such as the blood-ocular barrier by administering drugs directly into the vitreous humour. This minimises systemic negative effects and enables effective drug concentrations with lower dosages. The creation of controlled-release systems, which maintain therapeutic medication levels for months or even years, has enhanced this approach even more. A limited injection volume (usually up to 100 microliters) and the comparatively brief half-life of medications in the vitreous humour are two drawbacks of the intravitreal method. As a result, in order to maintain appropriate therapy levels, patients frequently need several injections, raising the possibility of problems. [37] One important topic of current study is to increase the duration of a drug's occupancy in the vitreous. Properties including molecular weight, water solubility, and lipophilicity affect how quickly medications are cleared from the vitreous. Medication that has a larger molecular weight or is less soluble in water tends to stay in the vitreous cavity longer. For instance, when given as a suspension, triamcinolone acetonide shows longer retention because of its poor solubility, while water-soluble corticosteroids, such as dexamethasone sodium phosphate, are eliminated more rapidly. Additionally, because to binding interactions with melanin, medication retention may be prolonged in pigmented eyes. [38, 39]
Table 3 Lipid-based systems for ocular delivery of selected corticosteroids and their effects on ocular pharmacokinetics
|
Lipid-based delivery System |
Loaded Corticosteroids |
Ocular Pharmacokinetics |
References |
|
Cubosomes |
Beclomethasone dipropionate |
Cubosomes increased the Papp by 3.8-fold compared with the control suspension. The precorneal residence time and the AUC increased by 8.5- and 5.5-fold, respectively, compared with the control sodium fluorescein solution. The ocular bioavailability of the loaded drug was 5.52 compared with the suspension form. |
[20,21] |
|
Cubosomes |
Dexamethasone |
Cubosomes increased the Papp and the AUC by 4.5- and 1.8-fold compared with suspension eye drops. |
[21,22] |
|
Ethoniosomes |
Prednisolone acetate |
Ethoniosomes enhanced the ocular bioavailability (AUC) by 1.54-fold compared with the commercial suspension eye drops. |
[25,27] |
|
Liposomes |
Dexamethasone hemisuccinate |
Liposomes showed 2.3-time reduction in the pro inflammatory cytokine interleukin 6 (IL-6) concentration compared with the free dexamethasone hemisuccinate solution. |
[29,30] |
|
Liposomes |
Prednisolone acetate |
Liposomes increased the AUC compared with control solution. Also, they markedly reduced the inflammatory signs of uveitis compared with the solution dosage form, indicating enhanced ocular bioavailability. |
[32,33] |
|
Niosomes |
Prednisolone sodium phosphate |
Niosomal in situ gel increased AUC and Papp, value by 1.75- and 2.82-fold, respectively, compared with the control pure drug solution. |
[34,35] |
|
Niosomal in situ gel |
Prednisolone sodium phosphate |
The Tmax increased from 1 h for solution to 2 h for the niosomal in situ gel. |
[36,37] |
Ocular Side Effects of Corticosteroids
Adverse Effects of Corticosteroids on the Eye
The cornea, lens, optic nerve, and surrounding tissues are only a few of the ocular components that corticosteroids might negatively affect, despite their substantial therapeutic benefits. Increased intraocular pressure (IOP) and cataract development are the two most common consequences. Whether administered topically, systemically, intravitreally, or implant-based, these side effects may occur.
Corticosteroid-Induced Elevation of Intraocular Pressure (IOP)
IOP elevation is one of the most dangerous side effects of corticosteroid therapy, and if left untreated, it can result in steroid-induced glaucoma and damage to the optic nerve. Topical eye drops are not the only administration route that might cause this adverse response. People who have a personal or familial history of primary open-angle glaucoma are particularly vulnerable to elevated intraocular pressure caused by corticosteroids. Headaches, ocular pain, and vision abnormalities are possible symptoms.
There are a number of theories as to why corticosteroids cause an increase in intraocular pressure.[40, 41] These include decreased enzyme activity within the meshwork, increased water retention, accumulation of glycosaminoglycan’s, and malfunction of the trabecular meshwork, all of which hinder the outflow of aqueous humour (Fig. 3). Factors Influencing Corticosteroid-Related IOP Increase
Corticosteroid-Induced Cataract Formation
Corticosteroid use is also associated with the serious side effect of cataract development. The greatest risk factor is still ageing, but corticosteroids also play a role by accelerating oxidative stress and encouraging protein aggregation in the lens. These procedures cause lens opacification by decreasing the solubility of lens proteins. By blocking the sodium-potassium pump, promoting protein cross-linking, and creating steroid-protein adducts that change lens structure, corticosteroids may interfere with lens metabolism in a number of ways. By interfering with protein structure and function, these chemical interactions between corticosteroid molecules and lens proteins promote the development of cataracts. Corticosteroids can cause lens opacities that resemble human cataracts, according to experimental research conducted on animal models. Long-term usage of corticosteroids, even those with low intraocular penetration, can result in cataract development. [43, 44]
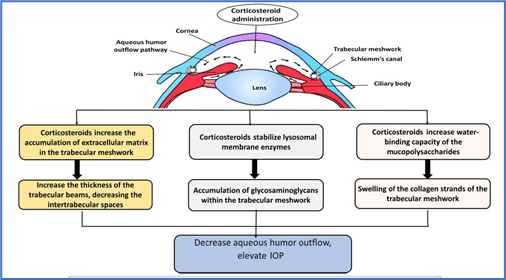
Figure 3 Graphical illustrations of proposed mechanisms of corticosteroid-induced elevation of intraocular pressure
Preventing and Reducing Ocular Side Effects of Corticosteroids
To minimize complications associated with corticosteroid use in the eye, several preventive measures are recommended:
FUTURE PERSPECTIVES
Corticosteroids are still essential for treating a variety of eye conditions. Innovative medication delivery systems that increase therapeutic advantages while lowering negative effects are the main focus of current research. There are several new formulations being developed, such as biodegradable implants, emulsions, gels, ointments, and punctual plugs. New methods such as iontophoresis, which increases medication penetration by using modest electrical currents, have a lot of promise. For instance, clinical trials have shown that the EyeGate II Delivery System is safe and efficient at administering dexamethasone. Tear duct inserts, such Dextenza®, offer a continuous delivery of corticosteroids with the option to be removed if side effects occur. In order to minimise adverse effects, the goal of retrometabolic medication design is to produce corticosteroids that are only momentarily active before quickly deactivating. With its strong anti-inflammatory properties and decreased incidence of cataracts and elevated intraocular pressure, loteprednol elaborate is a prime example of this strategy and is appropriate for long-term use. Researchers are also looking into conjugating corticosteroids with hydrophilic molecules to reduce side effects and restrict tissue penetration without sacrificing effectiveness.
CONFLICT OF INTEREST
The authors report neither conflict of interest nor financial interest.
REFERENCES


Sarthak Khandekar, Mrunal Karande, Afrin Sayyad, Vaishnavi Parit, Raju Rathod, Ophthalmic Corticosteroids: Innovations in Delivery Systems and Future Therapeutic Outlook, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 5619-5634. https://doi.org/10.5281/zenodo.15766448
 10.5281/zenodo.15766448
10.5281/zenodo.15766448
