
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Shree Warana Vibhag Shikshan Mandal's Tatyasaheb Kore College of Pharmacy, Warananagar,Panhala Kolhapur-416113, Maharashtra, India
Osteonecrosis, also known as avascular necrosis or aseptic necrosis, represents a debilitating condition characterized by cellular death of bone components due to interruption of blood supply. This condition affects approximately 10,000 to 20,000 individuals annually in the United States and poses significant challenges in orthopedic practice. This review synthesizes current understanding of osteonecrosis pathophysiology, risk factors, diagnostic approaches, and treatment modalities to provide clinicians with evidence-based management strategies. We conducted a comprehensive literature review of peer-reviewed articles, clinical trials, and systematic reviews published over the past two decades, focusing on epidemiology, pathogenesis, imaging techniques, and therapeutic interventions. Osteonecrosis results from multifactorial mechanisms including vascular insufficiency, increased intraosseous pressure, and cellular injury. The femoral head remains the most commonly affected site, though multiple joints may be involved. Early diagnosis through MRI enables timely intervention, while treatment strategies range from conservative management and core decompression in early stages to joint arthroplasty in advanced disease. Osteonecrosis represents a complex orthopedic condition requiring multidisciplinary management. Early detection and risk factor modification remain crucial for optimal outcomes. Emerging regenerative therapies show promise but require further validation through rigorous clinical trials.
Osteonecrosis, which is alternatively referred to as avascular necrosis or aseptic necrosis, represents a pathological condition characterized by the death of bone tissue due to inadequate blood supply. The absence of adequate blood circulation initiates a cascade of complications that may result in the deterioration of bone structure, impairment of joint integrity, and a significant decline in functional capacity if not addressed appropriately (1) First described in medical literature over a century ago, osteonecrosis has emerged as an important cause of musculoskeletal morbidity, particularly affecting individuals in their third to fifth decades of life. The femoral head accounts for approximately 80% of all osteonecrosis cases, though the condition may affect other anatomical sites including the humeral head, femoral condyles, tibial plateau, and small bones of the hands and feet (2) The clinical significance of osteonecrosis extends beyond its prevalence. The condition frequently affects young, active individuals during their most productive years, resulting in substantial socioeconomic burden through disability and need for major reconstructive surgery (3). Understanding the underlying mechanisms, identifying at-risk populations, and implementing appropriate management strategies remain critical priorities in orthopedic care. This comprehensive review examines current knowledge regarding osteonecrosis etiology, pathophysiology, clinical presentation, diagnostic modalities, and therapeutic approaches. We additionally discuss emerging technologies and future directions in osteonecrosis management.
Epidemiology :-
Incidence and prevalence :-
Osteonecrosis affects an estimated 10,000 to 20,000 new patients annually in the United States, with approximately 500,000 to 600,000 individuals currently living with the condition. The true incidence may be underestimated due to asymptomatic early-stage disease and diagnostic challenges in resource-limited settings. The condition demonstrates a bimodal age distribution, with traumatic osteonecrosis occurring more frequently in younger patients (20-40 years) and non-traumatic forms showing peak incidence in the fourth and fifth decades (4). Males are affected approximately 2-3 times more frequently than females, though this ratio varies by etiology and geographic location.
Anatomical distribution :-
The femoral head represents the most common site of osteonecrosis, accounting for 75-80% of cases (5). This predilection reflects the unique vascular anatomy of the proximal femur, where blood supply depends primarily on the lateral and medial femoral circumflex arteries. The humeral head ranks as the second most common site (10-15% of cases), followed by the femoral condyles and tibial plateau (6). Bilateral involvement occurs in 50-80% of non-traumatic cases, highlighting the systemic nature of many predisposing conditions.
Geographic and Population variations :-
Epidemiological patterns vary globally, influenced by genetic factors, environmental exposures, and healthcare access. Asian populations demonstrate higher incidence rates compared to Western populations, potentially reflecting genetic susceptibility and cultural practices such as alcohol consumption patterns (7). Certain populations face elevated risk, including patients with sickle cell disease (prevalence 40-50%), systemic lupus erythematosus (5-40%), and organ transplant recipients (5-25%) (8).
3. Etiology and risk factors :-
3.1 Traumatic Osteonecrosis:-
Direct vascular injury represents the most straightforward mechanism of osteonecrosis. Traumatic events disrupting blood flow to bone include:
3.2 Non Traumatic Osteonecrosis :-
Non-traumatic osteonecrosis results from diverse systemic and local factors that compromise bone perfusion through multiple mechanisms:
3.3 Idiopathic Osteonecrosis:-
Approximately 20-30% of osteonecrosis cases lack identifiable risk factors and are classified as idiopathic (23). These may represent unrecognized genetic susceptibilities, subclinical thrombophilia, or multifactorial conditions below diagnostic thresholds. Ongoing research examines genetic polymorphisms affecting bone metabolism, coagulation, and lipid handling as potential contributors (24).
4. Pathophysiology:-
4.1 Vascular Mechanisms:-
The fundamental pathophysiological event in osteonecrosis involves interruption of blood supply to bone tissue. The femoral head's susceptibility reflects its tenuous vascular anatomy, relying primarily on the medial femoral circumflex artery providing 60-80% of perfusion through a limited number of retinacular vessels entering the posterosuperior aspect of the femoral neck.
Vascular compromise occurs through multiple mechanisms:
4.2 Cellular and Molecular Mechanisms:-
Ischemia initiates cellular injury through multiple pathways:-
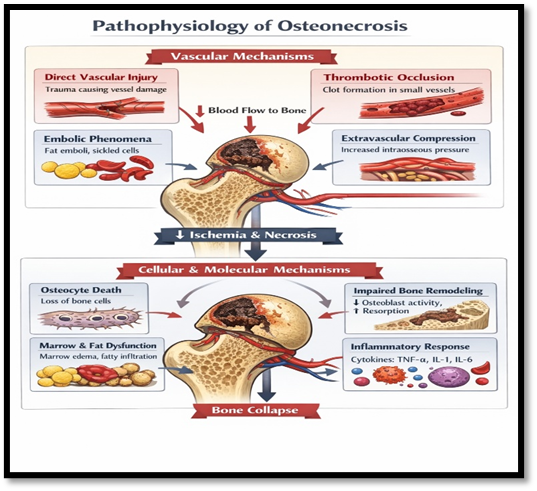
Fig. no. 1. Pathophysiology of Osteonecrosis
4.3 Biomechanical Factors:-
Mechanical stress on weakened bone accelerates disease progression. The femoral head sustains forces of 3-5 times body weight during normal activities, concentrating stress on the anterosuperior subchondral region where osteonecrosis most commonly occurs. As necrotic bone loses structural integrity and undergoes resorption during attempted repair, mechanical failure becomes inevitable without intervention (36). Subchondral fracture represents the critical event transitioning from reversible early-stage disease to irreversible structural collapse (37).
4.4 Stages of Disease Progression:-
Osteonecrosis progresses through predictable stages:-
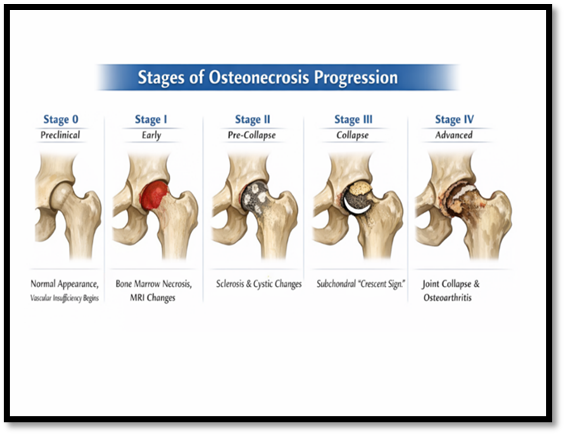
Fig. no.2. Stages of Disease Progression
5. Clinical Presentation
5.1 Symptoms:-
The clinical presentation of osteonecrosis varies with disease stage, anatomical location, and extent of involvement:
Pain:- The cardinal symptom is pain in the affected joint, typically developing insidiously in non-traumatic cases or acutely following trauma. Initially, pain may be intermittent and activity-related, progressing to constant discomfort as disease advances. In femoral head osteonecrosis, pain typically localizes to the groin, though radiation to the buttock, thigh, or knee occurs commonly (41). Pain severity does not always correlate with radiographic stage, with some patients experiencing significant symptoms in early disease while others remain relatively asymptomatic despite advanced structural changes.
Functional Limitation:- Progressive joint dysfunction manifests as decreased range of motion, limping, and difficulty with weight-bearing activities (42). Patients may report difficulty with stairs, prolonged standing, or athletic activities.
Sudden Symptom Onset:- Subchondral collapse may cause acute symptom exacerbation, with sudden intensification of pain and functional impairment marking transition from early to advanced disease.
5.2 Physical Examination:-
Physical examination findings evolve with disease progression:
Early Disease:- Examination may be normal or show only subtle findings. Reduced internal rotation and abduction of the hip may be detected. Pain with extremes of motion, particularly internal rotation and flexion, suggests early involvement (43).
Advanced Disease:- Examination demonstrates restricted range of motion in all planes, pain throughout range of motion, positive impingement signs, antalgic gait, leg length discrepancy (with femoral head collapse), and muscle atrophy from disuse (44)
Hip-Spine Syndrome:- Patients with hip pathology may develop compensatory lumbar spine changes causing overlapping symptoms, complicating diagnosis (45).
5.3 Asymptomatic Disease:-
A significant proportion of early-stage osteonecrosis remains asymptomatic, discovered incidentally on imaging performed for other indications or during screening of high-risk patients (46). The natural history of asymptomatic osteonecrosis remains incompletely understood, with some lesions remaining stable while others progress to symptomatic disease requiring intervention (47).
6. Diagnosis and Imaging
6.1 Plain Radiography:-
Standard anteroposterior and frog-leg lateral radiographs represent the initial imaging modality for suspected osteonecrosis. However, radiographic changes lag behind pathological changes by weeks to months, limiting sensitivity in early disease.
Radiographic Signs:-
Increased density/sclerosis:- Reflects attempted repair with new bone formation around necrotic tissue
Lucent lesions/cysts:- Represent areas of bone resorption
Crescent sign:- Radiolucent subchondral fracture line indicating structural collapse (pathognomonic for Stage III disease)
Flattening/collapse:- Deformity of articular surface
Joint space narrowing:- Secondary osteoarthritic changes in advanced disease
Limitations:- Normal radiographs do not exclude early-stage osteonecrosis. Sensitivity ranges from 40-60% in early disease, increasing to >90% in advanced stages (48).
6.2 Magnetic Resonance Imaging (MRI):-
MRI represents the gold standard for osteonecrosis diagnosis, demonstrating 99% sensitivity and 98% specificity for detecting early disease before radiographic changes appear.
MRI Characteristics:-
Double-line sign:- Pathognomonic finding on T2-weighted images consisting of inner bright line (granulation tissue) and outer dark line (sclerotic bone) (49)
Band-like pattern:- Low signal intensity band on T1-weighted images at interface between necrotic and viable bone.
Bone marrow edema:- High signal on T2-weighted or STIR sequences indicating reactive (50)
Geographic lesion location:- Typically anterosuperior femoral head.
Advantages:-
MRI enables detection 6-12 months before radiographic changes, assessment of lesion size and location for prognostication, bilateral evaluation to detect contralateral involvement, and differentiation from other conditions causing hip pain (51).
Disadvantages:-
Cost, limited availability in some settings, contraindications (metallic implants, pacemakers, claustrophobia), and longer acquisition time compared to other modalities (52).
6.3 Computed Tomography (CT):-
CT demonstrates intermediate sensitivity between radiography and MRI, useful when MRI is contraindicated or unavailable. CT excels at detecting subchondral fracture and quantifying collapse, aiding surgical planning (53).
6.4 Bone Scintigraphy:-
Technetium-99m bone scanning shows increased uptake in osteonecrosis due to reactive bone formation surrounding necrotic tissue. However, sensitivity and specificity are limited compared to MRI, and "cold" lesions may appear in early disease before revascularization begins, potentially leading to false-negative results.
6.5 Laboratory Evaluation:-
No specific laboratory tests diagnose osteonecrosis, but evaluation should identify underlying conditions:
- Complete blood count (hemoglobinopathies)
- Lipid panel (hyperlipidemia)
- Coagulation studies including thrombophilia screening in young patients without obvious risk factors (54).
- Autoimmune markers (ANA, anti-dsDNA) if lupus suspected.
- Hemoglobin electrophoresis in appropriate populations
- HIV testing in at-risk individuals.
7. Classification Systems:- Several classification systems grade osteonecrosis severity, guiding treatment decisions and facilitating research standardization:
7.1 Ficat and Arlet Classification:-
One of the earliest systems, based primarily on radiographic findings:
7.2 Steinberg/University of Pennsylvania Classification:-
Refines Ficat-Arlet system by incorporating lesion size and location:
Stage O-IV: Similar to Ficat-Arlet
Subclassifications (A, B, C): Based on lesion extent (<15%, 15-30%, >30% of femoral head involvement) (55)
7.3 Association Research Circulation Osseous (ARCO) Classification:-
International consensus classification combining multiple imaging modalities:
Incorporates radiographs, MRI, CT findings
Quantifies lesion size and location (56)
Includes both femoral and non-femoral sites
Widely used in contemporary literature and clinical trials.
7.4 Japanese Investigation Committee (JIC) Classification:-
Emphasizes lesion location, recognizing that anterosuperior lesions (weight-bearing surface) carry worse prognosis than medial lesions regardless of size (57)
Prognostic Value: Classification systems help predict disease progression, guide treatment selection, and standardize research reporting. Generally, larger lesions, anterosuperior location, and more advanced stages correlate with higher progression risk and worse outcomes with conservative treatment.
8. Treatment Approaches:-
Treatment selection depends on disease stage, lesion characteristics, patient factors, and symptom severity. Goals include pain relief, preservation of native joint when possible, and maintenance of function.
8.1 Conservative Management:-
Indications:- Early-stage disease (pre-collapse), small lesions in non-weight-bearing regions, or patients with significant comorbidities precluding surgery.
Protected Weight-bearing:- Crutch or walker use reduces mechanical stress on affected joint, theoretically allowing healing. However, effectiveness remains controversial with limited high-quality evidence supporting long-term benefits.
Pain Management:- NSAIDs, acetaminophen, and judicious use of opioids for severe pain (58).
Physical Therapy:- Maintains range of motion and muscle strength while minimizing stress on affected joint (59)
Risk Factor Modification: Cessation of alcohol and tobacco use, corticosteroid minimization when possible, optimization of underlying conditions
Monitoring: Serial imaging to detect progression requiring intervention
Outcomes: Natural history studies demonstrate progression to collapse in 60-85% of conservatively managed symptomatic lesions over 2-5 years, particularly larger lesions in weight-bearing regions (60). Success rates improve with very early detection and small lesions (61).
8.2 Pharmacological Interventions:-
Bisphosphonates: Antiresorptive agents that inhibit osteoclast activity, theoretically preventing collapse during remodeling phase. Multiple small trials and meta-analyses suggest potential benefit in early-stage disease, with some studies showing reduced progression and improved pain (62). Alendronate represents the most studied agent. However, evidence remains limited by small sample sizes and heterogeneous populations. Optimal dosing, duration, and patient selection criteria require further investigation.
Anticoagulants: Enoxaparin and warfarin have been studied based on the hypothesis that some osteonecrosis involves thrombotic mechanisms (63). Limited evidence suggests possible benefit in select early-stage patients, particularly those with underlying coagulopathy (64). Further research needed to define appropriate candidates.
Lipid-Lowering Agents: Statins may theoretically benefit patients with hyperlipidemia-associated osteonecrosis, though clinical evidence is sparse.
Prostacyclin Analogs: Iloprost, a vasodilator and antiplatelet agent, showed promise in small European studies for early-stage disease but has not gained widespread adoption, particularly in North America.
Other Agents: Vitamin D supplementation, hyperbaric oxygen therapy, and pulsed electromagnetic field therapy have been investigated with inconsistent results (65).
8.3 Core Decompression:-
Core decompression represents the most established surgical intervention for early-stage (pre-collapse) osteonecrosis (66).
Technique: The procedure involves drilling one or more channels from the lateral femoral cortex into the necrotic lesion under fluoroscopic guidance. This reduces intraosseous pressure, stimulates vascular ingrowth through the created channels, and initiates a healing response (67).
Variations: Multiple small-diameter channels versus single large-diameter core. Arthroscopic versus open approaches Combined with biological augmentation.
Outcomes: Success rates range from 60-85% in appropriately selected patients (Stage I-II, small-to-medium lesions) (68). Factors predicting success include earlier stage, smaller lesion size, non-weight-bearing location, and pre-collapse status. Benefits include pain relief in 70-80% of patients and reduced progression to collapse compared to natural history (69).
Complications: Include fracture (1-2%), infection (<1%), transient increased pain, and treatment failure requiring additional procedures.
8.4 Advanced Core Decompression with Biological Augmentation:-
Enhancement of core decompression with biological materials aims to improve outcomes:
Bone Grafting:
Autologous cancellous bone:- Harvested from iliac crest, provides osteoconductive scaffold and viable osteoprogenitor cells
Vascularized fibular graft:- Microsurgical transfer of fibular segment with intact blood supply provides both structural support and revascularization. Technically demanding with longer operative time and donor site morbidity, but demonstrates superior outcomes in larger lesions and early collapse (60-80% success preventing progression) (70).
Vascularized iliac crest graft:- Alternative to fibular graft with similar principles
Bone Marrow Aspirate Concentrate(BMAC): Concentrated autologous bone marrow containing mesenchymal stem cells, growth factors, and cytokines. Injected into decompression channels to enhance healing. Early studies suggest improved outcomes compared to decompression alone, though optimal concentration, volume, and technique remain under investigation (71).
Stem Cell Therapy: Direct injection of culture-expanded autologous mesenchymal stem cells (from bone marrow or adipose tissue) aims to regenerate necrotic bone. Multiple small trials demonstrate safety and potential efficacy, but larger randomized controlled trials are needed (72)
Growth Factors and Platelet-Rich Plasma (PRP): Biological adjuncts providing concentrated growth factors to stimulate bone healing. PRP represents an accessible option though evidence for benefit remains mixed.
Tantalum Rod Implantation: Porous tantalum rod inserted into decompression tract provides structural support while allowing bone ingrowth. Some studies suggest improved outcomes versus decompression alone in preventing collapse.
8.5 Osteotomy:-
Rotational or varus/valgus osteotomy repositions the necrotic segment away from the weight-bearing surface while moving healthy bone into functional position (73)
Transtrochanteric Rotational
Osteotomy:- Surgically rotates femoral head to position viable bone under the acetabular weight-bearing surface. Requires precise preoperative planning and technical expertise. Success rates of 60-80% reported in appropriately selected patients (adequate viable bone remaining, pre-collapse or early collapse) (74)
Disadvantages:- Technically demanding, long rehabilitation, altered anatomy complicating future arthroplasty if needed, and limited applicability (requires sufficient healthy bone for rotation).
Current Use: Less commonly performed with improved outcomes from core decompression augmentation and earlier arthroplasty techniques, though remains an option in young patients wishing to preserve native anatomy (75)
8.6 Joint Arthroplasty:-
Arthroplasty represents definitive treatment for advanced osteonecrosis with collapse and secondary osteoarthritis.
Total Hip Arthroplasty (THA): Gold standard for end-stage femoral head osteonecrosis, providing reliable pain relief and functional restoration. Modern implants and techniques demonstrate excellent long-term outcomes with 90-95% 10-year survival rates (76)
Considerations in Osteonecrosis:
Young patient age: Osteonecrosis patients undergo arthroplasty 10-20 years younger than osteoarthritis patients, raising concerns about implant longevity and need for revision (77)
Bilateral disease: Approximately 50-60% require bilateral arthroplasty
Alternative bearing surfaces:- Ceramic-on-ceramic or ceramic-on-polyethylene bearings may improve longevity in young, active patients (78)
Femoral head preservation: Large-diameter metal-on-metal bearings (now largely abandoned due to complications) and modern hard-on-hard bearings aimed to maximize longevity
Hip Resurfacing: Alternative to conventional THA preserving femoral bone stock. Initially popular for young osteonecrosis patients, use has declined due to complications including femoral neck fracture, metal ion release, and pseudotumor formation. Select patients may still benefit, though conventional THA remains preferred.
Outcomes: THA for osteonecrosis demonstrates slightly higher revision rates compared to osteoarthritis (related to younger age and higher activity levels) (79) but provides excellent pain relief and function in >90% of patients (80)
Other Joint Arthroplasty:-
Osteonecrosis affecting other joints follows similar treatment principles:-
Shoulder: Humeral head osteonecrosis may require hemiarthroplasty or total shoulder arthroplasty (81)
Knee: Unicompartmental or total knee arthroplasty for femoral condyle or tibial plateau involvement
Ankle: Talus osteonecrosis may require ankle fusion or total ankle arthroplasty (82)
9. Special Populations:-
9.1 Pediatric Osteonecrosis:-
Osteonecrosis in children presents unique challenges. Legg-Calvé-Perthes disease represents idiopathic femoral head osteonecrosis in children aged 4-8 years, managed differently from adult disease with emphasis on containment and guided growth (83). Secondary osteonecrosis occurs in children receiving corticosteroids for leukemia, organ transplantation, or inflammatory conditions (84). Treatment focuses on risk factor modification, protected weight-bearing, and joint-preserving procedures when possible to delay arthroplasty until skeletal maturity.
9.2 Pregnancy:-
Osteonecrosis rarely occurs during pregnancy or postpartum period, possibly related to hypercoagulability, mechanical factors, or hormonal changes (85). Management emphasizes conservative treatment with protected weight-bearing and pain control using pregnancy-safe medications. Surgical intervention is typically delayed until after delivery when possible.
9.3 Sickle Cell Disease:-
Patients with sickle cell disease demonstrate particularly high osteonecrosis prevalence and unique management considerations including attention to disease-specific complications, optimization of hematological status preoperatively, and awareness of higher perioperative complication rates including infection and thrombosis.
10. Prognosis and Natural History:-
The natural history of untreated osteonecrosis varies with stage, lesion characteristics, and anatomical location:
Early-Stage Disease:- Small, non-weight-bearing lesions may remain stable or heal spontaneously in 10-30% of cases (86). However, most symptomatic lesions (60-85%) progress to collapse without intervention, typically within 2-5 years.
Post-Collapse Disease:- After subchondral fracture, progression to end-stage arthritis occurs in >90% of cases, necessitating arthroplasty (87) (88)
Prognostic Factors:-
Lesion size: Larger lesions carry higher progression risk (89)
Location: Anterosuperior (weight-bearing) location predicts progression
Stage: Later stages demonstrate higher failure rates with joint-preserving treatment
Bilateral involvement: Suggests systemic etiology with potentially worse prognosis
Underlying etiology: Corticosteroid-induced disease may have worse natural history than alcohol-related (90)
Post-Treatment Outcomes:-
Core decompression: 60-85% success in early-stage disease
Vascularized grafting: 60-80% prevent progression in select patients (91)
Arthroplasty: >90% achieve excellent pain relief and function with modern techniques.
11. Future Directions and Emerging Therapies:-
11.1 Regenerative Medicine:-
Stem Cell Therapy: Culture-expanded mesenchymal stem cells, induced pluripotent stem cells, and embryonic stem cells represent promising avenues for bone regeneration (92). Challenges include optimal cell source, delivery method, differentiation protocols, and regulatory considerations.
Tissue Engineering: Scaffold-based approaches combining biomaterials with cells and growth factors aim to regenerate functional bone tissue. Three-dimensional printed scaffolds customized to defect geometry show promise in preclinical studies.
Gene Therapy: Viral vector-mediated delivery of osteogenic genes (BMP-2, VEGF) to enhance bone healing represents an experimental approach requiring extensive safety evaluation (93).
11.2 Advanced Imaging:-
Quantitative MRI:- Techniques including T1 and T2 mapping, diffusion-weighted imaging, and perfusion MRI may enable earlier detection and better characterization of early ischemic changes before frank necrosis (94).
Molecular Imaging:- PET imaging with bone metabolism tracers may identify at-risk bone before structural changes occur.
Pharmacological Prevention:- Identifying high-risk patients (particularly those initiating high-dose corticosteroid therapy) and implementing prophylactic strategies represents an important research priority. Studies examining bisphosphonates, anticoagulation, statins, and other agents for prevention in at-risk populations are ongoing (95)
11.4 Precision Medicine:-
Genetic Risk Stratification: Identifying genetic polymorphisms affecting bone metabolism, coagulation, and lipid handling may enable personalized risk assessment and targeted prevention in susceptible individuals.
Biomarkers: Discovery of serum or imaging biomarkers predicting disease development or progression could transform management by enabling earlier intervention and personalized treatment selection (96)
11.5 Artificial Intelligence
Machine learning algorithms analyzing imaging data, clinical parameters, and treatment outcomes may improve prognostication, treatment selection, and outcome prediction, supporting clinical decision-making.
CONCLUSION
Osteonecrosis represents a complex, multifactorial condition with significant impact on patient quality of life and healthcare systems. Understanding the diverse etiologies, pathophysiological mechanisms, and clinical presentations enables appropriate diagnosis and management. Early detection through judicious use of MRI in symptomatic patients and high-risk populations remains critical, as joint-preserving interventions demonstrate greatest efficacy before irreversible structural collapse occurs.
REFERENCES



Ajit Patil, Pradnya Bhosale, Disha Faratade, Osteonecrosis: A Comprehensive Review of Pathophysiology, Diagnosis, and Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3454-3471. https://doi.org/10.5281/zenodo.18722504
 10.5281/zenodo.18722504
10.5281/zenodo.18722504