1Assistant Professor, Department of Pharmacology & Therapeutics, MKCG Medical College & Hospital, Berhampur , Ganjam, Odisha, India
2Student (M. Pharmacy – Pharmaceutical Chemistry), Department of Pharmacy, Jagannath University, State Highway 22, Bahadurgarh–Jhajjar Road, Jhajjar, Haryana, India
3Professor, Department of Pharmacy, Jagannath University, State Highway 22, Bahadurgarh–Jhajjar Road, Jhajjar, Haryana, India
4Professor, Department of Pharmacy, Jagannath University, Bahadurgarh, Haryana, India
5Assistant Professor, Department of Microbiology, Dinabandhu Andrews College, Baishnabghata, South 24 Parganas, Kolkata, West Bengal, India
6Department of Botany, Brahmananda Keshab Chandra College, Baranagar-700108, West Bengal, India
7Research Scholar, Department of Pharmacology, School of Pharmaceutical Education and Research, Jamia Hamdard, New Delhi, India
8Associate Professor, Department of Pharmaceutical Chemistry, Goel Institute of Pharmaceutical Sciences, Lucknow, Uttar Pradesh, India
*9Professor and Head, Department of Pharmacognosy, School of Pharmaceutical Sciences, Vels Institute of Science Technology and Advanced Studies, Old Pallavaram, Chennai – 600117, Tamil Nadu, India
Background: Polycystic Ovary Syndrome (PCOS) is a complex, heterogeneous endocrine disorder affecting women of reproductive age. It is characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology, with substantial metabolic and neuroendocrine involvement. Beyond infertility, PCOS is associated with insulin resistance, chronic inflammation, cardiometabolic risk, and psychological comorbidities. Understanding the integrated mechanisms underlying reproductive dysfunction is critical for targeted infertility management. Objective: To review the endocrine, metabolic, and neuroendocrine mechanisms contributing to infertility in PCOS and to summarize current and emerging therapeutic targets aimed at restoring ovulation and improving long-term health outcomes. Methods: This narrative review synthesizes current evidence from clinical trials, mechanistic studies, and international guidelines focusing on ovarian dysfunction, insulin resistance, neuroendocrine dysregulation, systemic complications, and therapeutic interventions in PCOS-related infertility. Results: PCOS pathophysiology involves disrupted folliculogenesis, theca cell hyperactivity, and altered steroidogenesis leading to hyperandrogenism. Abnormal pulsatile secretion of gonadotropin-releasing hormone (GnRH) contributes to elevated LH/FSH ratios and ovulatory failure. Insulin resistance and compensatory hyperinsulinemia exacerbate androgen excess and impair ovarian function through PI3K/Akt and MAPK signaling pathways. Chronic low-grade inflammation and adipose tissue dysfunction further amplify metabolic disturbances. Therapeutic strategies include ovulation induction (letrozole, clomiphene citrate), gonadotropin therapy, insulin sensitizers (metformin, inositols), lifestyle modification, neuroendocrine modulation (kisspeptin analogs), and emerging agents such as GLP-1 receptor agonists. Integrated, phenotype-driven approaches demonstrate improved reproductive and metabolic outcomes. Conclusion: Infertility in PCOS results from intertwined endocrine, metabolic, and neuroendocrine abnormalities. Effective management requires multi-target strategies that address both reproductive dysfunction and systemic risk factors. Future directions emphasize biomarker-guided therapy, precision medicine approaches, and translational research to optimize individualized infertility care and long-term health.
Polycystic Ovary Syndrome (PCOS) is one of the most common endocrine disorders affecting women of reproductive age. It is a heterogeneous condition characterized by a combination of menstrual irregularity, hyperandrogenism, and polycystic ovarian morphology. Although PCOS has been recognized for decades, its clinical presentation remains variable, reflecting the complex interplay of endocrine, metabolic, and neuroendocrine mechanisms underlying the disorder. The syndrome not only affects reproductive health but also exerts long-term systemic consequences, making it a significant public health concern.
The diagnosis of PCOS has evolved over time. The National Institutes of Health (NIH) criteria, established in 1990, require the presence of both chronic anovulation and clinical and/or biochemical signs of hyperandrogenism, after excluding other etiologies such as congenital adrenal hyperplasia or androgen-secreting tumors (Zawadzki & Dunaif, 1992). In contrast, the Rotterdam criteria, introduced in 2003 by a joint consensus of the European Society of Human Reproduction and Embryology and the American Society for Reproductive Medicine, broadened the definition. According to these criteria, PCOS can be diagnosed when any two of the following three features are present: oligo- or anovulation, hyperandrogenism, and polycystic ovarian morphology on ultrasound (Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group, 2004). This expanded framework acknowledges the heterogeneity of the syndrome but has also contributed to ongoing debates regarding phenotype classification and long-term risk stratification.
Epidemiologically, PCOS affects approximately 6–20% of women of reproductive age worldwide, depending on the diagnostic criteria applied and the population studied (Azziz et al., 2016). The prevalence tends to be higher when the Rotterdam criteria are used, reflecting the inclusion of milder or non-hyperandrogenic phenotypes. Importantly, PCOS is observed across diverse ethnic and geographic populations, although clinical manifestations and metabolic risks may vary. In South Asian women, for instance, there is evidence of a higher propensity toward insulin resistance and metabolic complications at lower body mass indices compared to Western populations (Teede et al., 2018).
Clinically, PCOS is a leading cause of anovulatory infertility. Women commonly present with irregular menstrual cycles, hirsutism, acne, and difficulties in conceiving. Beyond reproductive dysfunction, PCOS is strongly associated with insulin resistance, type 2 diabetes mellitus, dyslipidemia, and increased cardiovascular risk (Azziz et al., 2016; Teede et al., 2018). Psychological comorbidities, including anxiety, depression, and reduced quality of life, further compound the burden of the condition. The syndrome therefore represents not merely a gynecological issue but a systemic disorder with lifelong implications.
Given its multifactorial nature, understanding PCOS requires an integrated perspective. Endocrine disturbances such as excess ovarian androgen production, altered luteinizing hormone secretion, and disrupted folliculogenesis form the classical framework of the disease. However, mounting evidence highlights the pivotal role of metabolic dysfunction, particularly insulin resistance and compensatory hyperinsulinemia, in amplifying androgen excess and impairing ovulation. In parallel, neuroendocrine abnormalities involving altered gonadotropin-releasing hormone pulsatility and hypothalamic–pituitary–ovarian axis dysregulation are increasingly recognized as central contributors to the pathophysiology of infertility in PCOS. Exploring these interconnected pathways is crucial for identifying targeted therapeutic strategies that move beyond symptom management toward mechanism-based infertility treatment.
The aim of this review is to provide a comprehensive overview of the pathophysiological mechanisms underlying PCOS, with particular emphasis on endocrine, metabolic, and neuroendocrine interactions that contribute to infertility. By synthesizing current evidence on systemic complications and emerging therapeutic targets, this review seeks to clarify how integrated, multi-target approaches may improve reproductive outcomes and long-term health in women affected by PCOS.
2. Ovarian and Endocrine Pathophysiology
The ovarian and endocrine disturbances in Polycystic Ovary Syndrome (PCOS) represent the central biological drivers of anovulation and infertility. Although clinical manifestations vary, a consistent feature across phenotypes is disrupted folliculogenesis accompanied by androgen excess and gonadotropin imbalance. These abnormalities arise from intrinsic ovarian dysfunction, altered hypothalamic–pituitary signaling, and metabolic influences that amplify steroidogenic activity.
2.1 Ovarian Folliculogenesis Abnormalities
Normal folliculogenesis involves the coordinated growth of primordial follicles into dominant preovulatory follicles under tightly regulated endocrine control. In PCOS, this process is arrested at the small antral stage, leading to the accumulation of multiple immature follicles visible on ultrasound. Rather than a true increase in cyst formation, the ovary contains numerous arrested follicles that fail to achieve dominance (Franks, 1995).
Excess intraovarian androgens disrupt granulosa cell proliferation and impair aromatase activity, limiting estradiol production and preventing follicular maturation (Azziz et al., 2016). Additionally, increased levels of Anti-Müllerian hormone (AMH) produced by small antral follicles further inhibit follicle sensitivity to follicle-stimulating hormone (FSH), reinforcing developmental arrest (Dewailly et al., 2014).
Table 2.1. Normal vs. PCOS Folliculogenesis
|
Feature |
Normal Ovary |
PCOS Ovary |
|
Follicle recruitment |
Cyclic, regulated |
Excess early recruitment |
|
Dominant follicle selection |
Single dominant follicle |
Arrest at small antral stage |
|
Estradiol production |
Adequate |
Reduced aromatization |
|
Ovulation |
Regular |
Oligo/anovulation |
|
AMH levels |
Physiological range |
Elevated |
2.2 Hyperandrogenism: Sources and Mechanisms
Hyperandrogenism is a defining endocrine feature of PCOS. Androgen excess originates primarily from ovarian theca cells, although adrenal contribution is observed in a subset of women (Rosenfield & Ehrmann, 2016). Elevated luteinizing hormone (LH) stimulates theca cells to produce androstenedione and testosterone through enhanced enzymatic activity in steroidogenic pathways. Hyperinsulinemia further augments androgen production by acting synergistically with LH and by suppressing hepatic sex hormone–binding globulin (SHBG), increasing free androgen levels (Diamanti-Kandarakis & Dunaif, 2012).
The clinical consequences include hirsutism, acne, and follicular arrest. Importantly, androgen excess perpetuates a self-reinforcing cycle, impairing normal follicular development and ovulation.
Table 2.2. Sources of Androgen Excess in PCOS
|
Source |
Mechanism |
Clinical Impact |
|
Ovarian theca cells |
LH-driven steroidogenesis |
Testosterone excess |
|
Adrenal cortex |
Increased DHEAS secretion |
Variable contribution |
|
Hyperinsulinemia |
Amplifies theca response, reduces SHBG |
Increased free androgens |
2.3 Role of Theca Cell Dysfunction
Theca cell hyperactivity is intrinsic to PCOS ovaries. Studies demonstrate that theca cells from affected women exhibit exaggerated androgen production even in vitro, suggesting inherent dysregulation (Nelson et al., 1999). Upregulation of steroidogenic enzymes such as CYP17A1 enhances androgen biosynthesis. This intrinsic ovarian defect appears independent of circulating gonadotropin levels, although LH excess intensifies the response.
2.4 Altered LH/FSH Ratio and Gonadotropin Dysregulation
Neuroendocrine abnormalities contribute significantly to ovarian dysfunction. Women with PCOS commonly exhibit increased LH pulse frequency and amplitude, leading to a disproportionately elevated LH/FSH ratio (Pastor et al., 1998). Elevated LH stimulates androgen production, while relatively low or normal FSH levels fail to adequately support granulosa cell maturation.
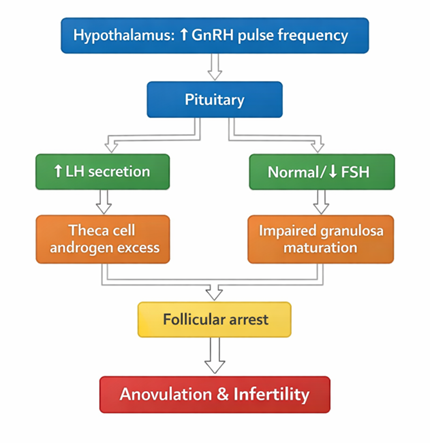
Figure 1. Gonadotropin Dysregulation in PCOS
This altered pulsatility of gonadotropin-releasing hormone favors LH synthesis over FSH, disrupting the hormonal environment required for ovulation (Rosenfield & Ehrmann, 2016).
2.5 Steroidogenesis Pathway Alterations
The ovarian steroidogenic pathway is dysregulated in PCOS, particularly at the level of 17α-hydroxylase/17,20-lyase (CYP17A1). Increased enzymatic activity shifts steroid production toward androgen synthesis rather than estrogen formation (Diamanti-Kandarakis & Dunaif, 2012).
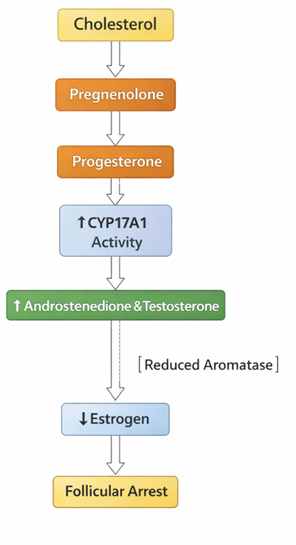
Figure 2. Simplified Steroidogenesis Alteration in PCOS
Reduced aromatase activity in granulosa cells limits conversion of androgens to estradiol, thereby impairing dominant follicle selection.
2.6 Anti-Müllerian Hormone (AMH) Excess
AMH levels are consistently elevated in PCOS and correlate with follicle number. Beyond serving as a biomarker, AMH may actively contribute to pathophysiology by inhibiting FSH sensitivity and modulating GnRH neuronal activity (Dewailly et al., 2014). High AMH levels reinforce follicular arrest and may contribute to abnormal gonadotropin secretion.
2.7 Impact on Ovulatory Dysfunction and Infertility
The combined effects of androgen excess, gonadotropin imbalance, intrinsic theca cell dysfunction, and AMH overproduction culminate in chronic anovulation. Without regular ovulation, progesterone production is insufficient, menstrual cycles become irregular, and fertility is compromised. Persistent anovulation also exposes the endometrium to unopposed estrogen, increasing the risk of hyperplasia over time (Azziz et al., 2016).
Table 2.3. Pathophysiological Mechanisms Leading to Infertility
|
Mechanism |
Direct Effect |
Fertility Outcome |
|
Hyperandrogenism |
Follicular arrest |
Anovulation |
|
Elevated LH |
Excess theca stimulation |
Poor oocyte quality |
|
Low FSH activity |
Inadequate granulosa maturation |
Failed dominant follicle |
|
High AMH |
Reduced FSH sensitivity |
Persistent immature follicles |
|
Insulin synergy |
Amplified androgen production |
Ovulatory dysfunction |
Collectively, ovarian and endocrine abnormalities form the biological foundation of infertility in PCOS. Understanding these mechanisms provides a framework for targeted therapeutic interventions aimed at restoring ovulation and improving reproductive outcomes.
3. Insulin Resistance and Metabolic Dysregulation
Metabolic dysfunction is not merely an associated feature of Polycystic Ovary Syndrome (PCOS); it is a central component of its pathophysiology. Insulin resistance (IR) affects a substantial proportion of women with PCOS, including those who are lean, indicating that it is partly intrinsic to the disorder rather than solely a consequence of obesity (Diamanti-Kandarakis & Dunaif, 2012). The metabolic disturbances seen in PCOS extend beyond glucose intolerance to encompass dyslipidemia, chronic low-grade inflammation, oxidative stress, and adipose tissue dysfunction. These interconnected abnormalities amplify hyperandrogenism and contribute to long-term cardiometabolic risk.
3.1 Mechanisms of Insulin Resistance in PCOS
Insulin resistance in PCOS involves impaired cellular responsiveness to insulin despite normal or elevated circulating insulin levels. At the molecular level, post-receptor defects appear to play a major role. Abnormal serine phosphorylation of the insulin receptor and insulin receptor substrate (IRS) proteins interferes with downstream signaling, particularly within the phosphatidylinositol-3-kinase (PI3K) pathway responsible for glucose transport (Diamanti-Kandarakis & Dunaif, 2012).
In skeletal muscle and adipose tissue, reduced translocation of glucose transporter type 4 (GLUT4) to the cell membrane leads to decreased glucose uptake. Meanwhile, hepatic insulin resistance contributes to excessive gluconeogenesis and impaired suppression of hepatic glucose output. Notably, these abnormalities have been documented in both obese and non-obese women with PCOS, supporting the hypothesis that intrinsic genetic or developmental factors may predispose to metabolic impairment (Dunaif, 1997).
Obesity, particularly central adiposity, further exacerbates insulin resistance by increasing free fatty acid flux and inflammatory cytokine release. However, the persistence of IR in lean women underscores the multifactorial nature of the defect.
3.2 Compensatory Hyperinsulinemia
When peripheral tissues fail to respond adequately to insulin, pancreatic β-cells increase insulin secretion to maintain euglycemia. This compensatory hyperinsulinemia is a hallmark of PCOS. Although initially adaptive, chronic hyperinsulinemia becomes pathogenic. Elevated insulin levels exert direct ovarian effects, stimulating androgen production independently of gonadotropins (Nestler et al., 1998).
Over time, sustained β-cell stress may lead to impaired glucose tolerance and type 2 diabetes mellitus. Epidemiological data indicate that women with PCOS have a significantly higher lifetime risk of developing glucose intolerance compared to age-matched controls (Azziz et al., 2016). Thus, compensatory hyperinsulinemia bridges reproductive dysfunction and long-term metabolic disease.
3.3 Insulin–Androgen Interaction
A critical feature of PCOS is the synergistic interaction between insulin and luteinizing hormone (LH) in the ovarian theca cell. Insulin enhances LH-stimulated androgen synthesis by upregulating steroidogenic enzymes, including CYP17A1 (Diamanti-Kandarakis & Dunaif, 2012). Furthermore, insulin suppresses hepatic production of sex hormone–binding globulin (SHBG), increasing circulating free testosterone concentrations.
This interaction creates a feed-forward cycle: insulin resistance leads to hyperinsulinemia; hyperinsulinemia augments androgen production; androgen excess worsens visceral adiposity and insulin resistance. Experimental studies demonstrate that reducing insulin levels through pharmacologic or lifestyle interventions can lower circulating androgen concentrations and improve ovulatory function (Nestler et al., 1998).
3.4 Adipose Tissue Dysfunction
Adipose tissue in PCOS exhibits functional and structural abnormalities beyond simple fat accumulation. Visceral adiposity is particularly prominent and metabolically active. Adipocytes in women with PCOS display impaired insulin signaling, increased lipolysis, and altered adipokine secretion patterns (Carmina et al., 2019).
Adipokines such as adiponectin, leptin, and resistin are dysregulated. Reduced adiponectin levels, even in lean women with PCOS, contribute to diminished insulin sensitivity and increased inflammatory signaling. Excess free fatty acids released from dysfunctional adipose tissue further impair insulin signaling in muscle and liver, reinforcing systemic insulin resistance.
3.5 Dyslipidemia and Altered Lipid Metabolism
Dyslipidemia is commonly observed in PCOS and is characterized by elevated triglycerides, increased low-density lipoprotein (LDL) cholesterol, and reduced high-density lipoprotein (HDL) cholesterol. These lipid abnormalities are strongly associated with insulin resistance and central obesity (Wild et al., 2010).
Insulin normally suppresses lipolysis and regulates hepatic lipid metabolism. In insulin-resistant states, increased hepatic very-low-density lipoprotein (VLDL) production and reduced HDL formation occur. The resulting atherogenic lipid profile contributes to elevated cardiovascular risk, even in younger women.
3.6 Role of Inflammation and Oxidative Stress
PCOS is associated with chronic low-grade inflammation. Elevated circulating levels of inflammatory mediators such as tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) have been reported (Escobar-Morreale et al., 2011). These cytokines interfere with insulin signaling by promoting serine phosphorylation of IRS proteins, thereby impairing glucose uptake.
Oxidative stress further compounds metabolic dysfunction. Increased reactive oxygen species (ROS) production damages cellular components and disrupts insulin receptor signaling. Oxidative stress also enhances androgen production in ovarian cells, linking metabolic imbalance with reproductive dysfunction.
The interplay between inflammation, oxidative stress, and insulin resistance suggests that PCOS shares mechanistic similarities with metabolic syndrome.
3.7 Molecular Signaling Pathways: PI3K/Akt and MAPK
Insulin exerts its biological effects through two major intracellular pathways:
In PCOS, selective impairment of the PI3K/Akt pathway has been observed, while the MAPK pathway remains relatively intact (Diamanti-Kandarakis & Dunaif, 2012). This selective resistance explains why metabolic actions of insulin are diminished whereas mitogenic and steroidogenic actions persist. Consequently, insulin continues to stimulate ovarian androgen production despite reduced glucose-lowering effectiveness.
This divergence in signaling creates a paradoxical situation: metabolic dysfunction coexists with enhanced androgen synthesis. Understanding these molecular distinctions provides a rationale for targeted therapies that improve insulin sensitivity without stimulating ovarian steroidogenesis.
Insulin resistance and metabolic dysregulation form a pivotal axis in the pathogenesis of PCOS. Through compensatory hyperinsulinemia, altered adipokine secretion, inflammatory activation, and selective signaling pathway defects, metabolic abnormalities amplify androgen excess and impair ovulation. These disturbances not only compromise fertility but also predispose affected women to long-term cardiometabolic disease. Therapeutic strategies that address insulin sensitivity therefore hold dual benefits—improving reproductive outcomes and reducing systemic risk.
4. Neuroendocrine Mechanisms and Hypothalamic–Pituitary–Ovarian Axis Dysfunction
Neuroendocrine dysregulation is a central driver of reproductive dysfunction in Polycystic Ovary Syndrome (PCOS). While ovarian and metabolic factors contribute substantially, abnormalities within the hypothalamic–pituitary–ovarian (HPO) axis shape the hormonal environment that sustains hyperandrogenism and chronic anovulation. Altered pulsatile secretion of gonadotropin-releasing hormone (GnRH), heightened pituitary responsiveness, sympathetic overactivity, stress-axis perturbations, and neurotransmitter imbalance collectively disrupt normal feedback regulation, leading to infertility.
4.1 Abnormal Pulsatile Secretion of Gonadotropin-Releasing Hormone
Under physiological conditions, gonadotropin-releasing hormone (GnRH) is secreted in a pulsatile manner from hypothalamic neurons. The frequency and amplitude of these pulses determine the relative secretion of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) from the pituitary. In PCOS, GnRH pulse frequency is persistently accelerated, favoring LH over FSH synthesis (Pastor et al., 1998).
This rapid pulsatility increases LH secretion, stimulating ovarian theca cells to produce excess androgens. At the same time, relatively inadequate FSH secretion impairs granulosa cell maturation and estradiol production, preventing dominant follicle selection. Studies suggest that androgen excess itself may impair hypothalamic sensitivity to progesterone negative feedback, perpetuating rapid GnRH pulsatility (Rosenfield & Ehrmann, 2016).
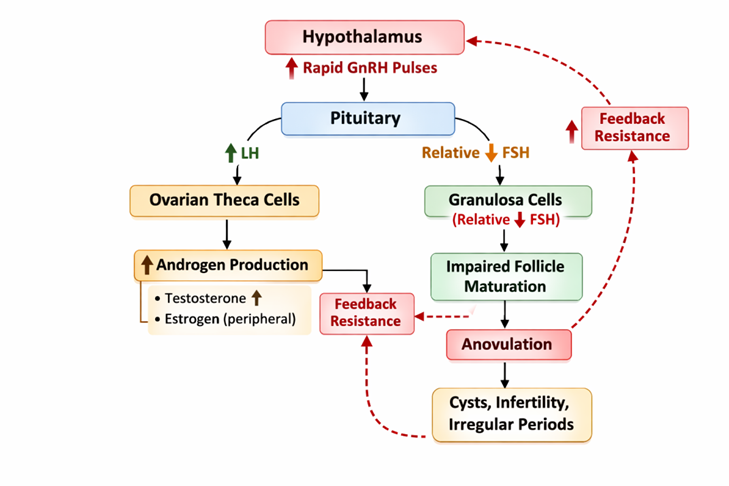
Figure 3. Accelerated GnRH Pulse Frequency in PCOS
This self-reinforcing loop underscores how central neuroendocrine alterations sustain ovarian dysfunction.
4.2 Hypothalamic Dysregulation
Hypothalamic neurons that regulate GnRH activity exhibit altered sensitivity to steroid feedback in PCOS. Normally, progesterone slows GnRH pulse frequency during the luteal phase. In PCOS, this inhibitory effect is blunted, likely due to chronic androgen exposure and altered neurotransmitter signaling (Marshall & Eagleson, 1999).
Additionally, metabolic cues such as insulin and leptin influence hypothalamic function. Insulin resistance and hyperinsulinemia may directly modulate GnRH neuron activity, linking metabolic and neuroendocrine pathways. This integration highlights PCOS as a systemic disorder rather than a purely ovarian condition.
4.3 Pituitary Sensitivity Changes
The pituitary gland in PCOS demonstrates enhanced responsiveness to GnRH stimulation. Even when exposed to similar GnRH concentrations as controls, women with PCOS secrete disproportionately higher LH levels (Pastor et al., 1998). This increased sensitivity contributes to the elevated LH/FSH ratio frequently observed.
Such alterations may arise from changes in GnRH receptor expression or intracellular signaling mechanisms within gonadotroph cells. Elevated LH perpetuates androgen excess, reinforcing the cycle of follicular arrest.
4.4 Sympathetic Nervous System Overactivity
Emerging evidence indicates increased sympathetic nervous system (SNS) activity in PCOS. Ovarian sympathetic innervation appears heightened, potentially stimulating androgen production and follicular arrest (Stener-Victorin et al., 2008). Elevated nerve growth factor (NGF) levels in ovarian tissue further support the role of autonomic dysregulation.
Sympathetic overactivity may also contribute to metabolic disturbances, linking stress responses with insulin resistance and ovarian hyperandrogenism.
4.5 Stress Axis Involvement (HPA Axis)
The hypothalamic–pituitary–adrenal (HPA) axis interacts closely with the reproductive axis. In some women with PCOS, subtle hyperactivity of the HPA axis leads to increased adrenal androgen secretion, including dehydroepiandrosterone sulfate (DHEAS) (Azziz et al., 2016). Chronic stress may amplify cortisol production, which can worsen insulin resistance and alter gonadotropin dynamics.
The interplay between the HPO and HPA axes suggests that chronic stress and psychological burden may exacerbate endocrine imbalance in PCOS.
4.6 Neurotransmitter Imbalance: GABA and Kisspeptin Pathways
Neurotransmitters are key regulators of GnRH neuron activity. Gamma-aminobutyric acid (GABA), typically inhibitory in many brain regions, paradoxically stimulates GnRH neurons. Increased GABAergic tone has been observed in experimental PCOS models, contributing to heightened GnRH pulse frequency (Moore et al., 2015).
Kisspeptin, a potent stimulator of GnRH release, is also implicated. Elevated kisspeptin signaling may sustain LH hypersecretion and androgen excess. These findings highlight neurotransmitter imbalance as a critical neuroendocrine component of PCOS pathogenesis.
Table 4.1. Neuroendocrine Alterations in PCOS
|
Mechanism |
Primary Effect |
Reproductive Consequence |
|
↑ GnRH pulse frequency |
↑ LH secretion |
Androgen excess |
|
Blunted progesterone feedback |
Persistent rapid pulses |
Chronic anovulation |
|
Pituitary hypersensitivity |
Elevated LH/FSH ratio |
Follicular arrest |
|
Sympathetic overactivity |
↑ Ovarian androgen output |
Impaired ovulation |
|
HPA axis activation |
↑ Adrenal androgens |
Hormonal imbalance |
|
GABA/kisspeptin dysregulation |
Sustained GnRH stimulation |
Infertility |
4.7 Feedback Loop Disruption in Infertility
The normal menstrual cycle depends on finely tuned feedback loops between ovarian steroids and the hypothalamus–pituitary unit. In PCOS, androgen excess, insulin resistance, and neurotransmitter imbalance reduce sensitivity to progesterone and estrogen feedback. This disruption prevents cyclical hormonal variation and ovulation. Without ovulation, progesterone production remains insufficient to slow GnRH pulses. The cycle becomes locked in a state of hormonal imbalance, culminating in infertility.
Neuroendocrine dysfunction in PCOS involves accelerated GnRH pulsatility, pituitary hypersensitivity, impaired steroid feedback, autonomic imbalance, and neurotransmitter dysregulation. These central alterations sustain ovarian hyperandrogenism and prevent ovulation. Understanding these interconnected mechanisms offers opportunities for targeted therapeutic strategies aimed at restoring hormonal feedback integrity and improving fertility outcomes.
5. Systemic Complications of PCOS
Although Polycystic Ovary Syndrome (PCOS) is often initially recognized because of menstrual irregularities or hyperandrogenic symptoms, its clinical implications extend far beyond the ovary. PCOS is now understood as a multisystem disorder with reproductive, metabolic, cardiovascular, hepatic, oncologic, and psychological consequences. These systemic complications arise from the combined effects of chronic anovulation, hyperandrogenism, insulin resistance, and low-grade inflammation, and they frequently persist across the lifespan.
5.1 Reproductive Complications
5.1.1 Anovulation and Infertility
Chronic anovulation is a defining feature of PCOS and remains one of the leading causes of infertility worldwide (Azziz et al., 2016). The failure to develop a dominant follicle prevents regular ovulation and adequate luteal progesterone production. As a result, menstrual cycles are irregular, and spontaneous conception becomes difficult.
Even when ovulation occurs, hormonal imbalances—particularly hyperinsulinemia and elevated androgens—may impair oocyte quality and endometrial receptivity. This altered intrauterine environment can reduce implantation success and increase early pregnancy loss.
5.1.2 Recurrent Miscarriage
Women with PCOS have a higher risk of first-trimester miscarriage compared to women without the condition. Insulin resistance, obesity, hyperandrogenemia, and impaired endometrial function are implicated as contributing factors (Palomba et al., 2015). Elevated insulin levels may disrupt trophoblastic development, while chronic inflammation and altered coagulation profiles may further compromise pregnancy maintenance.
5.2 Metabolic Syndrome
Metabolic syndrome is significantly more prevalent in women with PCOS than in age-matched controls. It is characterized by central obesity, hypertension, dyslipidemia, and impaired glucose regulation. Insulin resistance serves as the core pathophysiological link connecting these features (Diamanti-Kandarakis & Dunaif, 2012).
Even in younger women, clustering of metabolic risk factors is common. Central adiposity plays a particularly important role, as visceral fat is metabolically active and contributes to inflammatory cytokine production, worsening insulin resistance.
Table 5.1. Components of Metabolic Syndrome in PCOS
|
Component |
Pathophysiological Basis |
Clinical Consequence |
|
Central obesity |
Visceral adipose dysfunction |
Insulin resistance |
|
Hyperglycemia |
Impaired insulin signaling |
Diabetes risk |
|
Elevated triglycerides |
Hepatic lipid overproduction |
Atherogenesis |
|
Low HDL cholesterol |
Altered lipid metabolism |
Cardiovascular risk |
|
Hypertension |
Endothelial dysfunction |
Vascular complications |
5.3 Type 2 Diabetes Mellitus
Women with PCOS have a markedly increased risk of developing type 2 diabetes mellitus (T2DM). Long-standing insulin resistance and compensatory hyperinsulinemia eventually strain pancreatic β-cell function, leading to impaired glucose tolerance and overt diabetes (Azziz et al., 2016).
Population-based studies indicate that glucose intolerance may appear at an earlier age in women with PCOS compared to the general female population. Screening for glucose abnormalities is therefore recommended, particularly in those with obesity or a family history of diabetes (Teede et al., 2018).
5.4 Cardiovascular Risk Factors
Although overt cardiovascular events are relatively uncommon in young women, surrogate markers of cardiovascular disease are frequently observed in PCOS. These include endothelial dysfunction, increased carotid intima-media thickness, dyslipidemia, and systemic inflammation (Wild et al., 2010).
Insulin resistance, chronic inflammation, oxidative stress, and hyperandrogenism collectively contribute to vascular impairment. Elevated LDL cholesterol and triglyceride levels, combined with reduced HDL cholesterol, create an atherogenic lipid profile. Hypertension is also more prevalent, further increasing long-term cardiovascular risk.
Table 5.2. Cardiovascular Risk Profile in PCOS
|
Risk Factor |
Mechanistic Link |
Long-Term Outcome |
|
Dyslipidemia |
Insulin resistance |
Atherosclerosis |
|
Hypertension |
Endothelial dysfunction |
Stroke risk |
|
Chronic inflammation |
Cytokine activation |
Plaque instability |
|
Hyperandro-genism |
Vascular remodeling |
Increased CV risk |
5.5 Non-Alcoholic Fatty Liver Disease (NAFLD)
Non-alcoholic fatty liver disease (NAFLD) has emerged as a significant hepatic complication in PCOS. Insulin resistance promotes hepatic lipid accumulation by increasing de novo lipogenesis and reducing fatty acid oxidation. Hyperandrogenism may further exacerbate liver fat deposition (Lonardo et al., 2015).
Women with PCOS are more likely to develop hepatic steatosis independent of obesity. In some cases, NAFLD may progress to non-alcoholic steatohepatitis (NASH) and fibrosis, underscoring the importance of metabolic evaluation in affected individuals.
5.6 Endometrial Hyperplasia and Cancer Risk
Chronic anovulation results in prolonged exposure of the endometrium to unopposed estrogen without the counterbalancing effects of progesterone. This hormonal environment promotes endometrial proliferation and increases the risk of hyperplasia and, over time, endometrial carcinoma (Azziz et al., 2016).
Women with prolonged amenorrhea are particularly vulnerable. Regular induction of withdrawal bleeding or ovulation is therefore recommended to mitigate this risk.
Table 5.3. Hormonal Mechanisms Leading to Endometrial Risk
|
Hormonal Imbalance |
Endometrial Effect |
Clinical Risk |
|
Chronic anovulation |
Lack of progesterone |
Continuous proliferation |
|
Unopposed estrogen |
Endometrial thickening |
Hyperplasia |
|
Insulin resistance |
Mitogenic signaling |
Carcinogenic potential |
5.7 Psychological Comorbidities
Psychological complications are increasingly recognized as integral to PCOS. Women with PCOS have higher rates of depression, anxiety, body image dissatisfaction, and reduced quality of life (Cooney et al., 2017). Contributing factors include hormonal imbalance, metabolic disturbances, infertility stress, and cosmetic concerns such as hirsutism and acne.
Hyperandrogenism and insulin resistance may also influence neurotransmitter systems, potentially contributing to mood dysregulation. The bidirectional relationship between psychological stress and endocrine imbalance may further exacerbate symptoms.
Table 5.4: Multisystem Complications of PCOS Summary
|
System Affected |
Major Complication |
Underlying Driver |
|
Reproductive |
Anovulation, miscarriage |
Hormonal imbalance |
|
Metabolic |
Metabolic syndrome |
Insulin resistance |
|
Endocrine |
Type 2 diabetes |
β-cell dysfunction |
|
Cardiovascular |
Atherosclerotic risk |
Dyslipidemia, inflammation |
|
Hepatic |
NAFLD |
Lipid accumulation |
|
Oncologic |
Endometrial cancer |
Unopposed estrogen |
|
Psychological |
Depression, anxiety |
Hormonal & psychosocial stress |
PCOS is a systemic disorder with far-reaching health implications that extend well beyond reproductive dysfunction. Chronic anovulation, insulin resistance, androgen excess, and inflammation collectively contribute to metabolic syndrome, diabetes, cardiovascular risk, hepatic steatosis, endometrial pathology, and psychological burden. Recognizing these multisystem complications is essential for comprehensive management strategies that address both short-term fertility concerns and long-term health outcomes.
6. Molecular and Genetic Contributors
The complexity of Polycystic Ovary Syndrome (PCOS) reflects the interaction of genetic susceptibility, epigenetic regulation, inflammatory signaling, mitochondrial dynamics, and environmental influences. Rather than being caused by a single mutation, PCOS is now regarded as a polygenic and multifactorial disorder in which inherited variants interact with metabolic and intrauterine factors to shape endocrine and reproductive phenotypes. Understanding these molecular contributors provides insight into disease heterogeneity and opens possibilities for precision-based therapeutic strategies.
6.1 Genetic Susceptibility Loci
Family clustering and twin studies support a heritable component in PCOS. Genome-wide association studies (GWAS) have identified multiple susceptibility loci linked to reproductive hormone regulation, insulin signaling, and ovarian function (Goodarzi et al., 2011). Variants near genes such as LHCGR, FSHR, DENND1A, and THADA have been associated with increased PCOS risk.
Alterations in the luteinizing hormone/ choriogonadotropin receptor (LHCGR) gene may enhance ovarian responsiveness to LH, promoting androgen overproduction. Similarly, variants in DENND1A appear to increase expression of a theca cell–specific isoform that augments steroidogenesis (Rosenfield & Ehrmann, 2016). Importantly, genetic variants often differ across ethnic populations, suggesting that ancestry influences phenotypic presentation.
Table 6.1. Selected Genetic Loci Associated with PCOS
|
Gene/ Locus |
Biological Role |
Potential Contribution to PCOS |
|
LHCGR |
LH receptor signaling |
Enhanced androgen production |
|
FSHR |
Follicle-stimulating hormone receptor |
Impaired folliculogenesis |
|
DENND1A |
Theca cell function |
Increased steroidogenesis |
|
THADA |
Energy metabolism regulation |
Metabolic susceptibility |
|
INSR |
Insulin receptor signaling |
Insulin resistance |
Despite these discoveries, identified loci account for only a portion of heritability, suggesting involvement of additional rare variants and gene–environment interactions.
6.2 Epigenetic Modifications
Epigenetic mechanisms—such as DNA methylation, histone modification, and chromatin remodeling—modulate gene expression without altering DNA sequence. Emerging evidence indicates altered methylation patterns in ovarian and metabolic tissues of women with PCOS (Xu et al., 2011).
Prenatal androgen exposure has been proposed as a developmental origin factor. Animal models demonstrate that excess androgens during fetal life can reprogram hypothalamic and ovarian gene expression, predisposing offspring to PCOS-like features in adulthood. Epigenetic changes may therefore bridge environmental exposures with inherited susceptibility.
Epigenetic dysregulation may affect genes involved in insulin signaling, steroidogenesis, and inflammation, thereby contributing to phenotypic variability.
6.3 MicroRNAs in PCOS
MicroRNAs (miRNAs) are small non-coding RNAs that regulate gene expression post-transcriptionally. Several circulating and ovarian-specific miRNAs are dysregulated in PCOS, influencing insulin sensitivity, granulosa cell proliferation, and androgen synthesis (Chen et al., 2013).
For example, altered expression of miR-93 and miR-21 has been linked to impaired insulin signaling and inflammatory pathways. In ovarian tissue, dysregulated miRNAs may disrupt follicular maturation and steroidogenic enzyme expression. Because circulating miRNAs are detectable in serum, they are being explored as potential diagnostic biomarkers.
Table 6.2. Functional Impact of miRNAs in PCOS
|
miRNA |
Target Pathway |
Biological Effect |
|
miR-93 |
Insulin signaling |
Reduced GLUT4 expression |
|
miR-21 |
Inflammatory pathways |
Cytokine modulation |
|
miR-132 |
Steroidogenesis |
Altered androgen synthesis |
|
miR-320 |
Granulosa cell function |
Impaired follicle maturation |
6.4 Inflammatory Cytokines (TNF-α, IL-6)
Chronic low-grade inflammation is a recognized feature of PCOS. Elevated circulating levels of tumor necrosis factor-α (TNF-α) and interleukin-6 (IL-6) have been reported independent of obesity (Escobar-Morreale et al., 2011).
TNF-α impairs insulin receptor signaling by promoting serine phosphorylation of insulin receptor substrates, worsening insulin resistance. IL-6 contributes to hepatic lipid synthesis and systemic inflammation. Both cytokines may stimulate ovarian androgen production, reinforcing endocrine imbalance.
Inflammation thus acts as both a consequence and a driver of metabolic and reproductive dysfunction in PCOS.
6.5 Mitochondrial Dysfunction
Mitochondria regulate cellular energy production and reactive oxygen species (ROS) balance. In PCOS, evidence suggests altered mitochondrial DNA copy number and impaired oxidative phosphorylation in ovarian and metabolic tissues (Victor et al., 2009).
Mitochondrial dysfunction can increase ROS generation, contributing to oxidative stress and insulin resistance. In oocytes, impaired mitochondrial activity may reduce developmental competence, affecting fertility outcomes. Given the energy-intensive process of follicular maturation, mitochondrial health is particularly critical in ovarian physiology.
6.6 Gut Microbiota Alterations
The gut microbiome has emerged as an important regulator of metabolism and immune function. Women with PCOS exhibit altered gut microbial diversity compared to healthy controls, including increased abundance of pro-inflammatory bacterial species (Lindheim et al., 2017).
Dysbiosis may influence systemic inflammation, insulin resistance, and androgen levels through mechanisms involving short-chain fatty acids, bile acid metabolism, and endotoxin release. Increased intestinal permeability (“leaky gut”) may allow lipopolysaccharide entry into circulation, triggering inflammatory cascades that exacerbate metabolic dysfunction.
Table 6.3. Molecular Contributors and Their Systemic Effects
|
Molecular Factor |
Primary Target |
Downstream Effect |
|
Genetic variants |
Ovarian & metabolic genes |
Hyperandrogenism, IR |
|
Epigenetic changes |
Gene expression control |
Phenotypic variability |
|
miRNA dysregulation |
Post-transcriptional regulation |
Altered insulin & steroid pathways |
|
TNF-α / IL-6 |
Insulin receptor signaling |
Inflammation, IR |
|
Mitochondrial dysfunction |
Cellular energy metabolism |
Oxidative stress |
|
Gut dysbiosis |
Immune & metabolic pathways |
Systemic inflammation |
Molecular and genetic contributors in PCOS reflect a complex interplay between inherited susceptibility, epigenetic programming, inflammatory signaling, mitochondrial function, and gut microbial balance. Rather than acting independently, these factors converge on shared pathways—insulin resistance, androgen excess, and chronic inflammation—shaping both reproductive and systemic manifestations. Continued exploration of these mechanisms may enable biomarker-guided diagnosis and individualized therapeutic approaches in infertility management.
7. Therapeutic Targets in Infertility Management
Management of infertility in Polycystic Ovary Syndrome (PCOS) focuses on restoring ovulation, correcting hormonal imbalance, improving metabolic function, and addressing neuroendocrine contributors. Because PCOS is heterogeneous, tailoring treatment to individual phenotypes enhances reproductive outcomes and reduces long-term risk. The following sections summarize established and emerging therapeutic targets in infertility management, organized into endocrine, metabolic, neuroendocrine, and novel approaches.
A. Endocrine Targets
1. Ovulation Induction
Induction of ovulation is a primary objective in PCOS-related infertility.
Clomiphene Citrate (CC) Clomiphene citrate is a selective estrogen receptor modulator that blocks estrogen feedback at the hypothalamus, increasing endogenous gonadotropin release and stimulating follicular development (Legro et al., 2014). CC remains a first-line agent due to its oral route, low cost, and decades of clinical experience. However, up to 20–40% of women exhibit clomiphene resistance, which may require alternative strategies.
Letrozole Letrozole, an aromatase inhibitor, reduces estrogen synthesis, leading to increased gonadotropin release and enhanced follicular growth. Randomized trials have demonstrated superior ovulation and live birth rates with letrozole compared to CC in women with PCOS (Legro et al., 2014). Letrozole is now often preferred as a first-line ovulation induction agent.
2. Gonadotropin Therapy
For women who do not respond to oral agents, controlled ovarian stimulation with exogenous gonadotropins (FSH ± LH) can be effective. This approach requires careful monitoring due to the risks of ovarian hyperstimulation syndrome (OHSS) and multiple gestations. Low-dose step-up or step-down protocols aim to minimize complications while maximizing ovulation success (Teede et al., 2018).
3. Anti-Androgen Strategies
Elevated androgens can interfere with folliculogenesis. Anti-androgen therapies—such as spironolactone or finasteride—may be considered in select cases, primarily to improve clinical hyperandrogenic features (e.g., hirsutism) and indirectly support ovulatory function. These agents are generally used alongside ovulation induction, not as primary fertility treatments, due to teratogenic concerns and the need for contraception during administration.
B. Metabolic Targets
1. Insulin Sensitizers
Metformin Metformin improves insulin sensitivity, reduces hepatic glucose output, and may lower circulating androgens by decreasing insulin-mediated ovarian steroidogenesis (Nestler et al., 1998). Although its effect on live birth rates is modest, metformin is particularly useful in women with glucose intolerance, obesity, or severe insulin resistance.
Inositols Myo-inositol and D-chiro-inositol are insulin sensitizers that modulate intracellular insulin signaling pathways. Supplementation has been associated with improved ovulation, reduced androgen levels, and better metabolic profiles in women with PCOS (Nordio & Proietti, 2012). Their favorable safety profile makes them attractive adjuncts to fertility treatment.
2. Lifestyle Interventions
Dietary modification and physical exercise are foundational for metabolic control in PCOS. Even modest weight loss (5–10% of body weight) can restore ovulation, improve insulin sensitivity, and increase spontaneous conception rates (Teede et al., 2018). Tailored nutrition plans—such as low-glycemic-index diets—and regular aerobic plus resistance exercise are recommended.
3. Weight Reduction Strategies
For women with obesity, structured weight management programs or bariatric surgery in select cases can yield dramatic improvements in reproductive and metabolic outcomes. Weight loss reduces insulin resistance and hyperandrogenism, often resuming regular ovulation.
C. Neuroendocrine Targets
1. GnRH Modulation
Modulation of GnRH pulsatility may normalize LH/FSH ratios and improve ovulatory function. Although direct pharmacological modulation of GnRH is limited in clinical practice, research continues on agents that adjust GnRH release patterns to correct gonadotropic imbalance.
2. Kisspeptin Analogs
Kisspeptin is a potent stimulator of GnRH neurons. Research in PCOS models suggests that kisspeptin analogs may restore GnRH pulsatility and normalize LH secretion, offering a potential targeted approach to rectify neuroendocrine disruption (George et al., 2016).
3. Stress Management Interventions
Psychological stress activates the hypothalamic–pituitary–adrenal (HPA) axis and can worsen GnRH pulsatility, insulin resistance, and ovulatory dysfunction. Techniques such as cognitive-behavioral therapy, mindfulness, and stress reduction programs support neuroendocrine balance and may complement medical therapy.
D. Emerging Therapies
1. GLP-1 Receptor Agonists
Glucagon-like peptide-1 (GLP-1) receptor agonists—originally developed for type 2 diabetes—promote weight loss and improve insulin sensitivity. Emerging data suggest that these agents can reduce visceral adiposity and androgen levels, improving ovulation and pregnancy outcomes in women with PCOS and obesity (Wu et al., 2020).
2. Anti-Inflammatory Agents
Given the role of chronic low-grade inflammation in PCOS pathogenesis, anti-inflammatory agents (e.g., omega-3 fatty acids, statins) are under investigation for their potential to improve both metabolic and reproductive parameters. Early studies indicate reductions in inflammatory markers and improved insulin signaling.
3. Personalized Medicine Approaches
Advances in genomics, metabolomics, and reproductive endocrinology are paving the way for personalized therapeutic strategies. Stratifying PCOS phenotypes—based on genetic, metabolic, and hormonal profiles—may allow clinicians to match patients with treatments most likely to yield successful pregnancies with minimal side effects.
Table 7.1 Summary of Therapeutic Targets and Mechanisms
|
Target Category |
Intervention |
Primary Mechanism |
Relevance to Infertility |
|
Endocrine |
Clomiphene citrate |
↑ GnRH & gonadotropins |
Stimulates ovulation |
|
Letrozole |
↓ Estrogen → ↑ FSH |
Enhanced follicle growth |
|
|
Gonadotropins |
Direct ovarian stimulation |
Ovulation induction |
|
|
Anti-androgens |
↓ Androgen action |
Improved folliculogenesis |
|
|
Metabolic |
Metformin |
↑ Insulin sensitivity |
Reduces hyperinsulinemia |
|
Inositols |
Improve insulin signaling |
↑ Ovulation rates |
|
|
Lifestyle |
Weight loss, ↑ activity |
Restores ovulation |
|
|
Neuroendocrine |
Kisspeptin analogs |
↑ GnRH pulsatility |
Corrects LH/FSH imbalance |
|
Stress management |
↓ HPA activation |
Supports hormonal balance |
|
|
Emerging |
GLP-1 agonists |
Weight loss, metabolic improvement |
Potential fertility benefit |
|
Anti-inflammatories |
↓ chronic inflammation |
Metabolic & reproductive improvement |
8. Challenges, Future Directions, and Conclusion
The complexity of Polycystic Ovary Syndrome (PCOS) continues to challenge clinicians and researchers. Despite substantial advances in understanding its endocrine, metabolic, and neuroendocrine underpinnings, important gaps remain in optimizing individualized infertility management and long-term health outcomes.
8.1 Heterogeneity of PCOS Phenotypes
One of the central challenges in PCOS management is its marked phenotypic heterogeneity. Women may present with varying combinations of hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology. Some individuals predominantly exhibit metabolic dysfunction, while others display classic reproductive features with minimal metabolic disturbance. This diversity reflects differences in genetic susceptibility, environmental exposures, adiposity patterns, and neuroendocrine regulation (Azziz et al., 2016).
The Rotterdam criteria broadened diagnostic inclusivity, creating four phenotypic subgroups with differing metabolic and reproductive risks. For instance, women with hyperandrogenic phenotypes tend to have greater insulin resistance and cardiometabolic risk compared with normoandrogenic variants (Teede et al., 2018). This heterogeneity complicates treatment selection and underscores the inadequacy of a “one-size-fits-all” therapeutic model.
8.2 Need for Biomarker-Guided Therapy
Current infertility management largely relies on clinical presentation rather than molecular stratification. There is growing recognition that biomarker-guided approaches may improve treatment precision. Potential biomarkers include:
Emerging omics technologies—genomics, transcriptomics, metabolomics, and microbiome profiling—may help identify distinct PCOS endotypes with specific therapeutic responsiveness. For example, patients with predominant insulin resistance may benefit more from insulin sensitizers or GLP-1 receptor agonists, whereas those with neuroendocrine dysregulation might respond better to therapies targeting GnRH pulsatility or kisspeptin pathways.
However, standardized, validated biomarkers for routine clinical use remain limited, and further longitudinal studies are needed before widespread implementation.
8.3 Integration of Multi-Target Therapeutic Approaches
PCOS pathophysiology involves interconnected endocrine, metabolic, inflammatory, and neuroendocrine pathways. Monotherapy may address only one dimension of dysfunction. Therefore, integrative strategies that simultaneously target multiple axes are increasingly favored.
An example of integrated management may include:
Such multimodal approaches aim not only to induce ovulation but also to optimize metabolic health, reduce miscarriage risk, and improve overall well-being. Future treatment paradigms are likely to combine pharmacological agents with structured lifestyle and behavioral interventions tailored to individual phenotype and risk profile.
8.4 Long-Term Reproductive and Metabolic Outcomes
While short-term ovulation and pregnancy rates are common endpoints in infertility trials, PCOS is a lifelong condition. Women with PCOS face elevated risks of:
Therefore, infertility treatment must not compromise long-term cardiometabolic health. For instance, excessive ovarian stimulation protocols may increase obstetric complications, and certain pharmacotherapies require monitoring for metabolic side effects. Longitudinal cohort studies are necessary to determine whether early metabolic intervention during reproductive years alters future cardiometabolic outcomes.
Moreover, intergenerational implications are gaining attention. Offspring of women with PCOS may have increased risk of metabolic disturbances, suggesting potential epigenetic transmission mechanisms that warrant further exploration.
8.5 Translational Research Perspectives
Bridging basic science discoveries and clinical practice remains a priority. Several translational directions are particularly promising:
Robust randomized controlled trials are required to validate these emerging interventions and to clarify their safety in reproductive populations.
8.6 Concluding Summary of Mechanistic Insights and Infertility Management Strategies
PCOS is a multifactorial disorder characterized by intertwined endocrine, metabolic, and neuroendocrine abnormalities. Hyperandrogenism, insulin resistance, chronic inflammation, and altered GnRH pulsatility collectively impair folliculogenesis and ovulation, resulting in infertility. Systemic complications extend beyond reproduction, affecting cardiometabolic and psychological health.
Effective infertility management requires:
Future advances will likely depend on phenotype stratification, biomarker-guided therapy, and integrative treatment frameworks. By shifting from symptom-based management to mechanism-driven precision care, clinicians may improve both reproductive success and lifelong health outcomes for women with PCOS.
REFERENCES

Pratyush Mishra, Yasmin Suthar, Varun Arora, Pragi Arora, Tanmay Ghosh, Rishin Bhattacharyya, Sadma Parveen, Alka Mishra, Malarkodi Velraj, Pathophysiological Mechanisms and Systemic Complications of Polycystic Ovary Syndrome: Endocrine, Metabolic, and Neuroendocrine Targets in Infertility Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 912-933. https://doi.org/10.5281/zenodo.18871059
 10.5281/zenodo.18871059
10.5281/zenodo.18871059
