
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Sagar Institute of Research and Technology – Pharmacy, Sanjeev Agrawal Global Educational University Bhopal.
In addition to acting as a barrier and thermos-regulator, the skin also stops the body's interior organs from losing too much water. By adjusting the skin's barrier qualities, many medication delivery systems have been created. One possible therapeutic use for chemical enhancers that work on the stratum corneum's lipids and keratinized structures, as well as its partitioning and solubility effects, is to increase skin penetration. One promising new technique that might improve the amount of medications absorbed through the skin is penetration augmentation. It would also be easy to deliver medications with a short biological half-life. Eliminating degradation in the liver, having fewer side effects, and increasing bioavailability are three of the numerous benefits of this route over others. The outermost layer of the skin acts as a protective barrier, preventing the loss of physiologically necessary chemicals and providing resistance to penetration. This is the part of the percutaneous medication absorption process that is most time-consuming. Based on a scan of the appropriate scientific literature, this article of review summarizes recent developments in the study of permeation enhancers.
Developing a brand-new medication takes an enormous amount of time and money. It is easier and yields better results to reorganize the modules and find new routes to get the medicine into the bloodstream. To ensure that each patient receives their medication in the most optimal way possible, it becomes more complex to construct the dosage form so that it delivers the exact quantity of medicine to the exact location at the exact time. Slow medication release from the dosage form increases the likelihood that the medicine is going to be poorly absorbed therefore will not reach the bloodstream. Adverse side effects and a shorter-than-desired duration of action could occur if the medicine is released through the recommended dosage type too rapidly. The creation of new non-traditional drug delivery systems (NTDDSs) that can transport the medicine via the skin's pores and maintain therapeutically relevant concentrations for a long time is the answer to this issue [1]. Compared to traditional dosing systems, TDDSs have the potential to provide many benefits, such as higher effectiveness, less side effects, easier administration, more patient adherence, and minimal metabolism in the first pass. The transdermal medication delivery technique allows for more regulated and effective therapy by gradually releasing the medication into the bloodstream through the skin, avoiding the "peak & valley" that occurs naturally with oral or injectable dose forms. Concerning the skin's protective properties, the TDDSs' primary drawbacks are mostly related. The layer that is outermost of the multilaminate tissue known as skin acts as a significant barrier to the penetration of drugs. The stratum corneum (SC), a structure unique to the skin that consists of matrices rich in lipid with incorporated corneocytes in the most superficial layers (15 µm) and acts as a shield, greatly limits the quantity of drug that can be absorbed over an appropriate area of skin throughout the period of dosing. Additionally, the transdermal penetration is impacted by the drug's physicochemical characteristics, which include its molecular weight, log partition coefficient (log P), degree of ionization, and melting point. There are drugs that lack the necessary physicochemical qualities to penetrate living skin, even when transdermal delivery would be physiologically helpful. To improve transdermal medication distribution over the skin, researchers have come up with a number of tactics and procedures based on these parameters. A lot of people are interested in strategies like changing SC and similar procedures because of all the benefits they provide. Substances that momentarily increase the skin's permeability are known as permeability enhancers, and they help drugs absorb through the skin more effectively. Their applications include facilitating the transfer of ionizable like timolol maleate as well as impermeable like heparin, drugs, maintaining blood drug levels, increasing the dosage of less active drugs (like oxymorphane), delivering peptides and hormones with large molecular weights, and reducing the delay in response from transdermal drug delivery systems [2].
The Skin Anatomy.
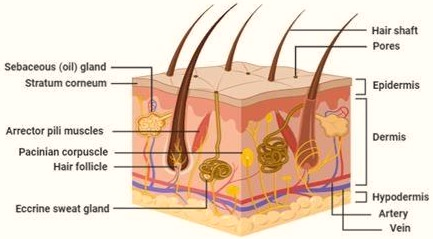
One potential obstacle to transdermal medication administration is the skin. Conversely, its capacity to restore itself and provide protection might make it highly esteemed. An adult's skin prevents water loss and shields us from unwanted environmental stimuli. It covers approximately two m2 of the body [3]. In Figure 1, we can see a simplified skin diagram.
Epidermal Layer
Layers of the epidermis include the outermost stratum corneum, the middle stratum germinativum, the outer stratum spinosum, and the innermost stratum granulosum. An inter-cellular lipid region separates the layers of keratinized corneocytes that make up SC, which is around 15 µm thick [4]. See Figure 2 for a simplified depiction of the skin. Ceramides, free fatty acids, neutral lipids, and triglycerides make up the inter-cellular lipid domain. Essential for desquamation include the remainder of the elements, which include phospholipids, glycosphingolipids, as well cholesterol. The arrangement of the corneocytes in the lipid-protein matrix resembles a brick wall. The lipid-protein matrix is like mortar while the corneocytes are like bricks. Corneo-desmosomes attach the thickly overlapping corneocytes to one another, and an intricate intercellular lipid matrix holds them all in place. An important permeability barrier for hydrophilic molecules with molecular masses larger than 200-350 Da, they're essential in maintaining the firmness along with impermeability of undamaged skin [5].
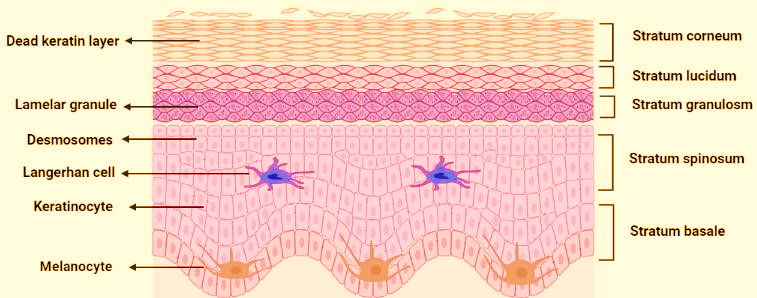
Figure 2. Schematic representation of the epidermis layer.
Dermal Layer
With a thickness ranging from 0.1 to 0.5 cm, the dermis is a deposit that attracts water. Blood arteries, lymphatic and nerve endings, pilosebaceous units, sweat glands, and a network of elastin and collagen fibers embedded in a mucopolysaccharide matrix make up the dermis. Elastic tissue allows movement and support is provided by collagen fibers in connective tissue. Substance transport is unaffected by the dermis (but it could be a major obstacle for more hydrophobic medications). Dermal blood vessels remove chemicals from the skin as they go through the epidermal layers, maintaining the concentration gradient that allows substances to penetrate the skin. A "shunt" route promoting a small number of permeants is also initiated in the dermal area by hair follicles, sebaceous glands, and sweat glands.
Hypodermal Layer
The skin's deepest layer, the hypodermis, also the subcutaneous layer. Insulation and shock absorption are two of its primary functions. Comprising several cell types, the hypodermis includes connective tissue, cells made up of fat, fibroblasts, vessels of blood, macrophages, and fatty tissues [6].
The Process involved in Permeation.
Various drug compounds have the ability to pass the epidermal barrier and reach the bloodstream via various pathways. According to Figure 3, these pathways may go intracellularly, intercellularly, or transfollicularly. Diffusion may take place via the intracellular pathway. Nonetheless, the intercellular gaps were the primary pathways for diffusion in the experimental research. This is because this route contains moistened keratin, a protein cell membrane, an interconnected covalent lipid a single-layer, and free lipids between cells. The several partitioning-diffusion steps across the hydrophilic as well lipophilic domains of this route prevent the majority of medicines from passing through the SC. As an example, when medications follow the intracellular route, those with a high lipophilicity will not be able to cross the hydrophilic domains.
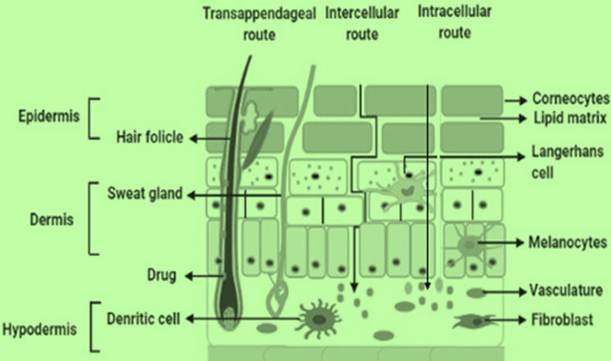
Figure 3. Schematic representation of the permeation process through the skin
On the other hand, because of their likelihood, they will be able to cross the lipophilic domains. It is more probable that hydrophilic medications will traverse the SC via the gaps in the lipids around the corneocytes. Around the corneocytes, the intercellular route is present and continually travels through the lipid matrix via the SC layer. From first application until achieving a favorable steady state, the intercellular route does not alter the penetration direction. Hence, it is thought of as the best route for tiny molecules [7]. The penetration rate and the amount of time needed to reach a steady state are unaffected by this. Molecules moved along this pathway by a process of successive diffusion and partitioning between the intercellular lipid polar head groups and the length of the alkyl chain. Since the combined surface area of the sweat glands and hair follicles is only about 0.1%, it is not thought of as a significant pathway for drug penetration [8]. In addition, the transfollicular route may participate in the rapid drug diffusion in the first hours before reaching a steady-state concentration. However, it is possible that medications with a large molecular weight really must be transported by this route. So far, many methods have been used to improve the transport of drugs across the skin. These methods include electrically-driven procedures, horny layer alteration or removal, vesicles or their counterparts, and drug-vehicle interaction. Methods for determining how drugs and vehicles interact are further subdivided into categories such ion pair, eutectic mixtures, and drug and prodrug selection. There are many types of vesicles, and subtypes such as liposomes, niosomes, transfero-somes etc. are known. Alcohol, surfactants, terpenes, sulfoxides, etc. are among the chemical enhancers, that may be used to modify the horny layer. Conversely, microneedle methods are used to remove the horny layer. Finally, there are electrically-driven methods such as photomechanical wave, iontophoresis, electroporation, and ultrasound. The next sections provide in-depth analyses of the various methods.
Interaction of Drug with its Vehicle
One of the first ways to improve skin absorption was via the interaction between drugs and vehicles. As an example, there are four main ways in which drugs and vehicles interact: chemical potential, ion pairing, eutectic systems, and prodrug selection [9]. The overarching goal of this approach is to improve drug-vehicle interaction and skin permeability by altering the SC in a way that does not impact skin layers outside of the SC.
Important Properties of Permeation Enhancers [10]:
It should not lead to the loss of bodily fluids as well as endogenous elements due to single-directional flow, and the skin should promptly regain its protective barrier capabilities once these substances are wiped out.
It would be ideal if no penetration enhancer had all the aforementioned characteristics. Minimizing the allergic reaction is the primary objective. On the other hand, additives often include chemicals that display most of these characteristics. Clinical trials and laboratory testing have shown their efficacy.
Methods of Improving permeation:
Three primary methodologies exist for enhancing penetration [11, 12].
Chemical Methodologies:
The mechanisms of these penetration enhancers can be categorized into three primary pathways [13]. These include:
1.Disrupting the meticulously organized architecture of the stratum corneum.
2.Engagement with proteins located within the intercellular environment.
3.Enhanced drug partitioning within the stratum corneum facilitated by the use of a co-enhancer (i.e., solvent).
The enhancers function by influencing one of these three routes. One can attain this through two distinct mechanisms: inducing a conformational alteration in skin-associated proteins or facilitating the expansion of the fluid. The fatty acid enhancers, for instance, increase the lipophilicity of the stratum corneum. The function of these enhancers is to facilitate the solubility of the drug within the stratum corneum, thereby promoting its diffusion into the outermost layer of the skin. The equation presented below delineates the factors that influence the degree of penetration of drug across the stratum corneum for flux steady-state. The given formula establishes a connection between steady flux, dm/dt, as well the mass m of the substance passing, per unit of skin surface area: dm/dt = D Co K /h
Here: Co represents the steady-state concentration of the medication in the donor fluid, K denotes the partition coefficient for the solute existing between the membrane's surface and the bathing solution, D signifies the diffusion coefficient, and h indicates the overall thickness of the protective membrane. A multitude of enhancers for permeation has been identified and employed over the decades to serve humanity, with several of the most prevalent examples presented below:
Alcohols: Various processes, including the extraction of lipids and proteins and the thickening of the stratum corneum, might cause alcohols to promote skin permeation. This, in turn, can improve the drug's dissolution into its formulation or its partitioning into the recipient's skin [14]. Here are a few options
Propylene glycol (PG): Drugs like Heparin NaHCl, verapamil HCl, as well ketoprofens are all facilitated by PG. It blocks the efflux of ketoprofen at elevated concentrations. The efficacy of cyclosporine A as well methotrexate is also improved when PG is added with azones. PG binds to SC keratin and takes up residence at the bonding sites for hydrogen. The diffusion of drugs intracellular, is enhanced when PG is coupled with azones, which allows large quantities of glycols to pass through the tissue. As the number of carbon atoms in an n-alcohol chain increases (as much as until 6), so does the drug flow. These alcohols enhance absorption by facilitating the extraction of SC lipids. A terpene-rich solution was prepared in PG-water system of co-solvents, which increased the 5-FU(fluorouracil) flow. The highest flow was achieved by medicines with an 80% PG concentration, and this was correlated with the action of terpenes. Additionally, PG enhances the drug's partitioning. The flow was found to be ten times higher when PG was combined with 5% oleic acid.
Short chain glycerides: Glyceryl mono-caprylate and other short-chain glycerides improve papaverine's partitioning capacity. It has also been shown that short-chain glycerides, such as TCP, are effective permeability enhancers. When combined with ethyl alcohol, it forms an exceptional hydrophobic system that enhances tegafurin absorption.
Amines and Amides:
Urea facilitates transdermal medication permeation by:
An ester groups with long alkyl chains along with a parent moiety, polar in nature, make up cyclic urea category of enhancers for permeation. Thus, the lipid disruption approach as well the existing hydrophilic activity interact to produce an enhanced state. Plus, they break down naturally. In addition, dimethyl acetamide, dimethyl formamide are more examples.
Cyclodextrines:
It has been reported that Cyclodextrines are biocompatible. They form complexes with lipophilic medicines to improve their solubility, particularly in water. The formation of an inclusion complex between piroxicam and β-cyclodextrine increases the flow over the non-hairy skin of rodents (mice) three times. Clonazepam and methyl-β- cyclodextrine were complexed to enhance the carbopol hydrogel's release profile via the cellulose nitrate membrane. The concentration of critical micelles of cyclodextrines may be enhanced by complexing them with enhancers, which are ammonium salts, quaternary in nature. Consequently, the boosters' harmfulness is reduced. The findings of the absorption experiments with alprostadil (AP) from the β-cyclodextrine complex as well the CME-β-CD complex were recorded. A hairless mouse was used as a comparison. As an enhancer of permeability, HPE-101 ( i.e. 1-[2-(decylthio) ethyl] azacyclopentan-2 one) was used. There was ten times less flux in the previous one. Hence, the conclusion was drawn that the biological availability of the medication is improved when CME-β-CD forms a compound with HPE-101. It can be typical to see a decrease in flux quantity at elevated levels of cyclodextrines. from this Lofts & Masson came to the conclusion that there could be a link between the impact of penetration into the skin of the medicine with cyclodextrine concentration. Cyclodextrine creates a compound with free drug at greater doses, reducing flow.
Fatty acids (FAs):
Enhancers of absorption may be found in fatty acids and their ester derivatives. When it comes to enhancers, unsaturated FAs are superior than saturated ones. The greatest significant promoter of permeability is palmitoeic acid. The results showed that hydrocortisone penetration across shaved skin of mice increased by a factor of 640. To display their enhancing action, unsaturated FAs must remain in their unrestrained original state.
Pyrrolidones:
It is well-known that pyrrolidones and their derivatives show great promise as trans-cutaneous enhancers of absorption. The most popular pyrrolidone that is known to increase skin penetration is N-methyl-2-pyrrolidone, or NMP. The anti-inflammatory medicine ibuprofen, for instance, had its flow increased by a factor of sixteen, while the flurbiprofen, by a factor of three, via a numb skin surface. Researchers Kim & Chien looked at how NMP affected the SC absorption of zidovudine along with other anti-HIV medications. Their experiments were conducted on shaved skins of mice maintained at 37°C. Research shows that a co-solvent of 1% NMP in ethanol to tricaprylin (TCP) in a volume/volume ratio of 50:50 had no influence on permeability. Numerous enhancing agents which were developed utilizing 2-pyrrolidone. A tiny alkyl group plus a dodecyl group were present at the 1stand third position of the pyrrolidone ring, correspondingly. Research found that the enhancing feature was positively affected by an alkyl group connected at the first position, even if it was short in length. Indomethacin penetration through the SC is significantly enhanced in 60% by weight of ethanolic solution containing 1-propyl and 1-butyl-3-dodecyl-2-pyrrolidone.
Sulfoxides:
Dimethyl sulfoxide: or A chemical that increases drug penetration is DMSO. Because it forms hydrogen bonds within its own cell instead of bonding with water, it functions as an aprotic solvent. Pharmaceutical engineering makes extensive use of it. It is also known as a "Universal Solvent" because of its remarkable ability to dissolve any substance. Both its color and its odor are completely gone. However, it is not without its drawbacks. When used in a system, DMSO causes effects that depend on the concentration. A co-solvent concentration of 60% or higher is necessary for improved enhancement efficiency. The issue is that DMSO might harm the stratum corneum layer and induce erythema at very high doses. Reddening, stinging, as well burning are common side effects of using dimethyl sulfoxide (DMSO) as an enhancer of penetration that denatures skin proteins. You may also get DMAC and DMF as aprotic solvents. While Southwell and Barry showed that caffeine's flow rose twelvefold when applied to DMF-treated human skin, they also discovered that DMF caused permanent destruction of the skin [15].
Surface active agents:
Cationic surfactants: Because of their absorption at interaction faces of two solvents, surface active agents enhance permeability. The penetrating power of cationic surfactants is higher compared to anionic ones. Consequently, they cause more skin injury.
Anionic surfactants: By removing the water-soluble intermediaries, anionic surfactants alter the stratum corneum's barrier properties. An excellent example of a substance that may alter the SC, thus enhance permeation is sodium lauryl sulphate.
Non-ionic surfactants: To emulsify sebum, surfactants that are not ionic have perforations punched into them. Because of this shift in the partitioning capability, permeation is enhanced. The reason these chemicals improve permeability is that the medicine may divide itself among the many enhancer types.
Biochemical Methodologies [16]:
Prodrug creation using bioconversion:
To get the best possible partition coefficient for penetrating the epidermal barrier, prodrugs are useful. Once the prodrug has been absorbed and diffused to the living tissues, enzymes transform it into drug's active state. Using this strategy, several steroids are being created. The ability to penetrate of 5-fluorouracil was increased by a factor of 25 by the formation of N-acyl derivatives. The 6-mercapto-purine molecule's permeability was enhanced by the addition of the S6-acyl-oxy-methyl with 9-di-alkyl-amino-methyl pro-moieties, resulting in a 240-fold increase in its permeability. Nalbuphine, buprenorphine, β-blockers, as well as other anti-inflammatory non-steroidal medicines have their skin permeability increased by the use of prodrugs.
Drugs that impair skin absorption when used together:
Interfering with homeostasis biological membrane, acting as barrier, by changing any or each processes of lamellar membrane coming together which may include production, assembling, release, processing, or stimulation is one assertive strategy suggested for promoting penetration through the skin of an individual. For a limited time, a synthesis inhibitor may prevent the production of cholesterol, ceramide, as well fatty materials. These days, this technique is being used more and more to improve the permeability of medications that normally have low permeability over skin of normal texture. The in vivo absorption of lidocaine hydrochloride is doubled, and the octanol/water partition coefficient is increased by 50 times, when fluvastatin is used.
Physical Methodologies [17]:
Iontophoresis:
The process occurs when the drug moves along the gradient of concentration in the layer of skin, either via migration,dissemination, or electro-osmosis. The majority of the fluid as well the counter ions move via the identical route during electro-osmosis. This fluid's mobility in the absence of the gradient of concentration forms the basis of iontophoresis. The skin has a small negative charge and produces counter ions from cations when circumstances are normal. To facilitate its penetration, a medication with a negative charge is placed between the cathode and the skin's surface. The ion is driven in the direction of anode across skin cells by the cell's electromotive force. If the medicine is positively charged, then the polarities of the electrodes should be reversed. The medicine reaches its destination after penetrating the skin and continuing on via the recipient's system of circulation. Skin permeability is increased by iontophoresis because it changes the SC's barrier function [18].
Sonophoresis:
The process of increasing skin permeability by the application of ultrasonic waves is known as sonophoresis. Several investigations have shown that when the skin is subjected to ultrasound, a variety of events occur.
Although the increased permeability from therapeutic sonophoresis is relatively temporary, it is nonetheless a powerful tool for transdermal improvement. When ultrasound is applied to the skin, it causes a rise in the ambient temperature. This causes the skin to become more permeable, allowing the medication to enter the bloodstream. Zars, lnc., USA has taken a similar strategy. They came up with a compact heater that can maintain a certain temperature for a set amount of time. An oxidation process takes on inside the heat source.
Stratum Corneum Exfoliation:
To quickly penetrate meidcated dosage employed for treating pimples, bruises, skin imperfections, including excessive pigmentation, doctors use a variety of methods that include exfoliating the outermost layer of the skin i.e. SC. One method that falls under the umbrella of superficial skin rejuvenation is microdermabrasion. Eroding the skin with sharp, tiny metal grains is the process that makes micro-channels on the skin's outermost layer. Microchannels develop in the dermis as a result of this. According to research, this method may increase angiogenesis penetration by a factor of 100.
Stratum Corneum Moistening:
The water percentage in stratum corneum is around 15–20%. As the amount of water increases, the swelling of the SC is supposed to cause its permeability to rise, according to the postulated process. No experimental experiments have yet made use of this approach. A daily and cost-effective way to do this would be to apply the occlusion principle, which would prevent water from evaporating off the skin. A variety of emulsions, including creams and lotions as well oils, waxy substances, including paraffins, might be used for this purpose. Among these, oil-based materials as well plastic films are perhaps more operative [19].
Some Natural Permeation Enhancers:
Natural permeation enhancers are substances that are present in nature, primarily within plants. These include fatty acids, polysaccharides, terpenes, and many. These also include ceramides, sterols, urea, fatty acids like oleic acids etc., which are naturally occurring compounds in the stratum corneum of human skin. Oils extracted from plants are the primary source of fatty acids, whereas the oils that are essential are mostly composed of terpenes and terpenoids [20]. In addition to their anti-inflammatory as well as antioxidant qualities, plant oils have the ability to regenerate and restore the protective layer of the skin. They serve as both active chemicals and molecules that help other substances, such as pharmaceuticals, penetrate the body, making them useful components of pharmaceutical & cosmetic goods. For application over the skin, they are regarded as safe and harmless. over the skin, the impact of oils extracted from plants, have been shown to vary somewhat. Olive oil compromises the viability of certain elements of SC, but sunflower seed oil helps to strengthen the skin's hydro-lipidic layer. It has been proposed that these characteristics are dependent on the ratio of oleic to linoleic acid in plant oils, since only the former increases SC permeability, which makes it easier for the medicinal to cross the skin [21, 22]. The composition of the oil fraction that is un-saponifiable, which includes substances like phospholipids, flavonoids, phyto-sterols, squalene, and triterpene alcohols, is also important because it may have an impact on the epidermis' barrier qualities [21]. In order for establishing safety of various penetration enhancers, it requires an understanding of how these natural penetration enhancers work once applied over skin surface. The most important element in attaining better permeation is probably the consideration of the dis-organizing impact on fractions of lamellar lipids by certain natural derivatives like urea. Because of their molecular makeup, which includes both polar as well as nonpolar groups, terpene compounds are known to be the most adaptable natural permeation enhancers. Terpenes can facilitate the penetration of hydrophilic as well as lipophilic pharmaceutical active agents [23]. Furthermore, the muco-adhesive qualities of hyaluronic acid (HA) enables regulated release of medications over time improving its rate of absorption. Modern medical treatments are certainly moving in towards the idea of using natural compounds with characteristics that make it easier for pharmaceutical active agents to pass through the SC.
Benefits of Permeation enhancers [24]:
Here are some benefits that we get from permeability enhancers:
Restrictions related to Permeation enhancers [25]:
CONCLUSION
It is necessary to inject several current medications, which is not only uncomfortable but also potentially dangerous. Consequently, the transdermal medication delivery system—which involves delivering drugs via the skin—has become more popular in recent years. The Stratum Corneum acts as a barrier to prevent drugs from entering the bloodstream. Because of how challenging it is to pass through the SC, permeation enhancers are necessary for this. There is a lot of room for growth in this new area. Researchers in this area have shown that absorption enhancers may make it easier and faster for drugs to be absorbed via the skin. The main issue with permeation enhancers is that they may irritate the skin and cause unsightly spots.
The primary goal is to develop absorption augmentation technologies that cause little or no skin discomfort. The fact that this enhanced augmentation often results in toxicity limits their clinical applicability. A permeability enhancer may help get the right amount of medicine into the skin for therapeutic purposes. Synthesizing a penetration enhancer by studying its interaction and creating a structural activity connection is one way to get chemicals that completely satisfy the ideal criteria. Aiming to create structures with lowest toxicity and optimum features, contemporary discovery and modelling tools may accomplish this.
Conflict Of Interest:
The authors have no conflicts of interest regarding this investigation.
ACKNOWLEDGMENTS:
The authors would like to thank Sanjeev agrawal global educational university Bhopal for their kind support during Permeation enhancers in Novel Drug Delivery System and all other lab studies.
REFERENCES



Vivekanand Rai*, Dr. Swati Kharee, Dr. Jitendra Banweer, Permeation Enhancers in Novel Drug Delivery System, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 165-177 https://doi.org/10.5281/zenodo.17035524
 10.5281/zenodo.17035524
10.5281/zenodo.17035524