
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Women’s College of Pharmacy, Peth Vadgaon, India.
Pharmacogenomics (PGx) the study of how an individual’s genomic variation affects drug response promises to revolutionize personalized therapy by optimizing efficacy and minimizing adverse effects. Recent data indicate that a striking majority of individuals carry at least one clinically actionable pharmacogenomic variant: in a large cohort study, nearly 80?% of a general patient population could benefit from PGx testing during their lifetime (Visscher et al., 2023). In specific populations, including Indian cohorts, prevalence of actionable genotypes remains high: a Central Indian study reported that 86?% of subjects harbored at least one actionable PGx variant, with 46.2?% and 74.2?% potentially benefitting from CYP2D6- and CYP2C19-guided dose adjustments respectively (Patel et al., 2025). Recent genomic analyses among Indians identified 76 known and 52 predicted deleterious variants associated with non-insulin antidiabetic drugs (NIADs), including a relative excess of alleles linked to decreased response to metformin compared to global populations (Sivadas et al., 2024). These findings underscore the vast, untapped potential of PGx in routine clinical care. Despite this, implementation remains limited globally. Systematic cost effectiveness analyses of PGx-guided therapy for drugs with clinical guidelines (e.g., from Clinical Pharmacogenetics Implementation Consortium?(CPIC)) show that 71?% of reviewed studies found PGx testing cost-effective or cost-saving (Morris et al., 2022). Pre emptive “panel testing” (rather than reactive single-gene assays) has emerged as attractive: more than 95?% of individuals harbor actionable variants across multiple genes, and panel-based testing may optimize prescribing across a lifetime (Meyer et al., 2025). In real-world settings, PGx-guided therapy was associated with reduced hospitalizations and emergency visits (PMed study, 2025). However, widespread adoption faces challenges: limited population specific data (especially in LMICs), cost, lack of guidelines tailored to regional genetic diversity, insufficient clinician training, and infrastructural and ethical bottlenecks (Kulkarni et al., 2025; Sivadas et al., 2024; IJCRT-2024). Advances in sequencing, bioinformatics, and integration with electronic health records (EHRs) combined with development of region specific PGx allele databases present a pathway forward. This review provides a detailed account of genetic variation and drug response data, clinical evidence, economic analyses, challenges, and future perspectives arguing for prioritized PGx implementation, especially in genetically diverse populations like India.
The term “pharmacogenomics” (PGx) refers to the study of how genome?wide genetic variations influence an individual’s response to medications. While often used interchangeably with “pharmacogenetics,” the latter historically focused on single gene–drug interactions, whereas pharmacogenomics encompasses a broader, genome?wide scope including multiple genes (e.g., metabolizing enzymes, transporters, receptors), structural variants, copy number variations (CNVs), and complex gene–gene or gene–environment interactions (Dovepress, 2022; Meyer et al., 2025).
The concept of genetically influenced drug response traces back to early observations of variable drug metabolism and idiosyncratic toxicity; however, PGx gained impetus after the advent of large?scale genomic sequencing and the completion of the human genome project. Enhanced sequencing technologies, bioinformatics, and pharmacogenomic databases (e.g., PharmGKB, CPIC) have enabled identification of clinically relevant variants across populations.
PGx holds particular significance in ethnically diverse countries such as India, where genetic architecture differs substantially from populations of European descent. Implementation of PGx-guided therapy promises to improve drug safety and efficacy, reduce adverse drug reactions (ADRs), decrease trial-and-error prescribing, and promote rational, individualized therapy. Recent large-scale genomic analyses and population-based studies have begun to quantify the potential reach and benefit of PGx in diverse populations (Patel et al., 2025; Sivadas et al., 2024).
This review provides an evidence?based, data-driven evaluation of pharmacogenomic variation, testing methodologies, clinical applications, real-world impact, economic analyses, challenges especially in the Indian context and future directions toward integrating PGx into standard clinical practice.
2. GENETIC VARIATIONS AND DRUG RESPONSE: EVIDENCE & POPULATION DATA
2.1. Prevalence of Actionable PGx Variants in Populations
A fundamental question for clinical relevance of PGx is: how many people carry variants that alter drug response. Evidence suggests that the vast majority estimated 90–95?% of individuals carry at least one actionable pharmacogene variant. (Haidar et al., 2022; Meyer et later 2025)
In a life time?impact study of a general patient population, nearly 80?% could benefit from PGx testing over their lifetimes (Visscher et al., 2023) The authors recommend conducting PGx testing ideally before age 50, although many individuals still benefit even into older age.
Region?specific data reinforce this. A recent Central Indian cohort study (2025) demonstrated 86?% of individuals carried at least one actionable PGx genotype; 46.2?% and 74.2?% of individuals would benefit respectively from CYP2D6- and CYP2C19-guided dosing changes (Patel et al., 2025). Another genomic survey in Indian subjects estimated that each Indian individual harbors on average ~8 medically actionable PGx variants (Kulkarni et al., 2025).
For non-insulin antidiabetic drugs (NIADs), a large analysis of 1,029 Indian whole genomes identified 76 known and 52 predicted deleterious PGx variants associated with 44 NIADs. Notably, Indians and South Asians carried a significant excess of alleles associated with decreased metformin response compared with global populations, suggesting population-specific reduced efficacy (Sivadas et al., 2024)
These studies underscore that PGx variation is both widespread and in genetically diverse populations like India may differ markedly from global or European-centric data, reinforcing the need for population?specific PGx resources.
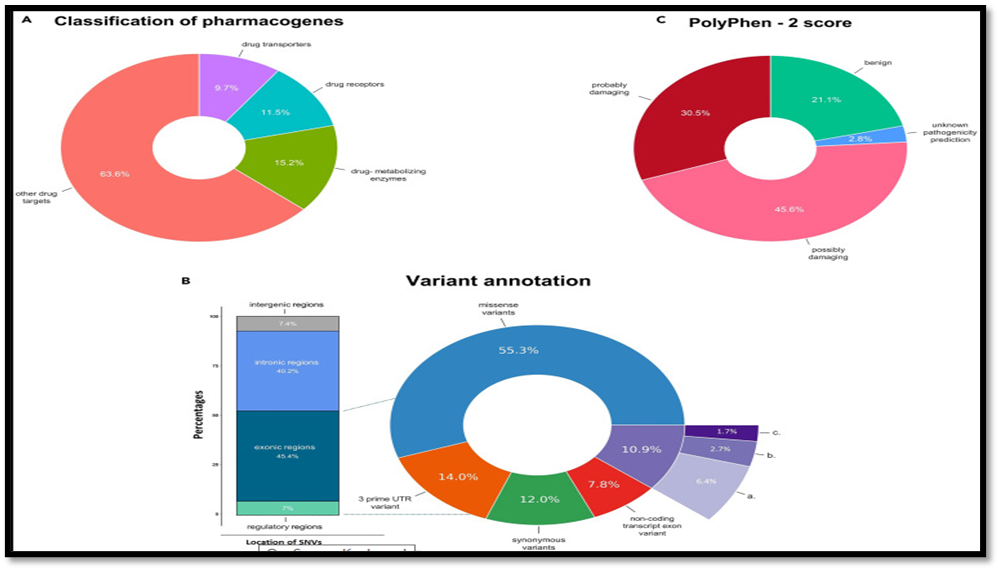
Fig no.1: Comparative distribution of major pharmacogenomic alleles across global populations, emphasizing frequency variation.
2.2. Genetic Variation Types: Beyond Simple SNPs
While single nucleotide polymorphisms (SNPs) account for much of the known actionable variation, PGx variation also includes structural variants, copy number variants (CNVs), and rare variants. For example, CYP2D6 key drug-metabolizing enzyme often exhibits copy-number variation, gene duplications or deletions, leading to ultra-rapid or poor metabolizer phenotypes (Meyer et al., 2025; Patel et al., 2025)
Moreover, germline variants in drug target genes (not only metabolizing enzymes) are relevant. Computational analysis of >60,000 human exomes revealed that ~80?% of patients harbor functional variants in at least one drug?target gene; for oncological drugs, the probability of germline variation impacting efficacy was ~44?% suggesting that pharmacogenomic considerations extend beyond metabolism to drug targets themselves (Schärfe et al., 2017).
2.3. Drug Classes and Genes of High PGx Relevance
Population-specific reviews have proposed a “core set” of pharmacogenes for pre?emptive PGx testing. Analysis of essential medicines (WHO list), neonatal drugs, and over-the-counter (OTC) drugs revealed 24 “prime genes” relevant to 57 drugs. In adults, 18 genes affect 44 drugs; in pediatrics, 18 genes impact 18 drugs. Over-the-counter drugs such as ibuprofen and omeprazole were identified as having actionable PGx variants (e.g., via CYP2C9 or CYP2C19 metabolism) underscoring PGx relevance even in common everyday medications (Kulkarni et al., 2025) Core genes frequently proposed for routine PGx panels in India include CYP2C19, CYP2C9, CYP2D6, TPMT, NUDT15, CYP3A4, CYP3A5, VKORC1, and CYP4F2 covering drugs from NSAIDs to antiplatelets, anticoagulants, immunosuppressants and more (Kulkarni et al., 2025).
In the context of type?2 diabetes therapy, the Indian variant landscape suggests particular caution: for many non?insulin antidiabetic drugs, PGx alleles associated with reduced response are overrepresented which could partly explain suboptimal glycemic control among Indian patients (Sivadas et al., 2024)
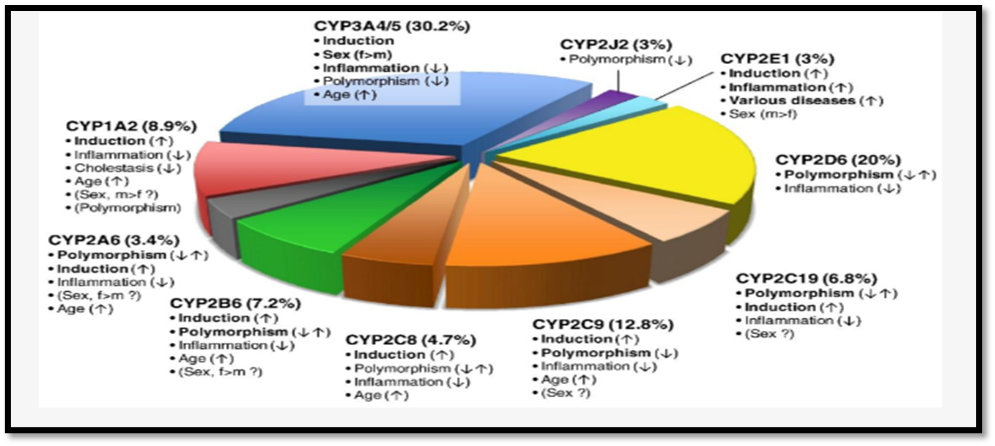
Fig no 2: Influence of CYP450 genetic polymorphisms on drug metabolism and clinical outcomes. Poor metabolizers accumulate drugs, risking toxicity, whereas ultra-rapid metabolizers may have sub-therapeutic effects.
3. PHARMACOGENOMIC TECHNOLOGIES
Advances in molecular biology and genomics underpin the feasibility of widespread PGx testing.
Recent real-world implementation studies demonstrate feasibility: in a Singapore outpatient clinic, pre-emptive PGx panel testing achieved a turnaround time of 2–7 business days (median ~5), and 21.2?% of patients receiving at least one actionable PGx recommendation leading to changes in prescriptions, dose adjustments, or increased monitoring (IMPT study, 2025).
Thus, with current technologies and workflows, PGx testing is technically feasible the key challenge lies in clinical implementation, guideline integration, and infrastructural readiness.
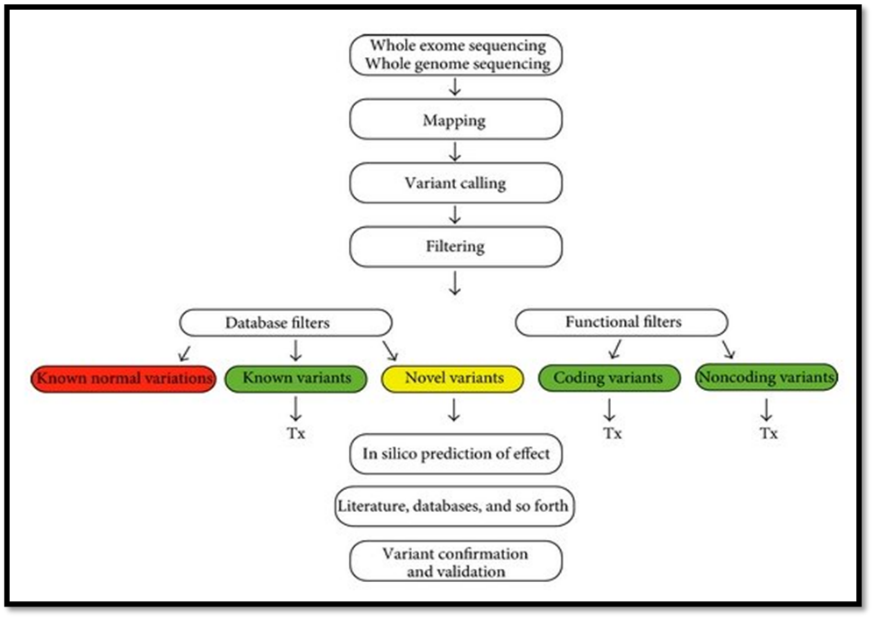
Fig no. 3: Workflow of pharmacogenomic-guided drug therapy showing the process from patient sampling, genotyping/sequencing, variant interpretation, clinical decision making, and therapeutic outcome monitoring
4. CLINICAL APPLICATIONS AND REAL-WORLD EVIDENCE
4.1. Scope of PGx-Relevant Drug Use
A large register-based study of 1,425,000 patients plus a university hospital cohort (n = 2,178) found that over a 2-year period, 60.4?% of patients received at least one pharmacogenetically actionable drug most commonly ibuprofen (25?%) and codeine (19.4?%) (Clinical Pharmacology & Therapeutics, 2024). Within the genotyped subset (n = 930), 98.8?% had at least one actionable genotype, and 23.3?% had at least one actionable gene?drug pair. A cost?benefit model suggested a saving of €17.49 per patient over 2 years (excluding cost of testing) when pre?emptive PGx panel testing was employed (CPT, 2024).
These data highlight that PGx-relevant prescribing is common, and pre-emptive panel testing could lead to meaningful cost savings and reduced ADR burden.
4.2. Impact on Adverse Drug Reactions (ADRs) and Safety
Serious ADRs remain a significant burden on healthcare systems worldwide. A 2024 systematic review identified over 254 RCTs / post-hoc studies and 207 meta-analyses linking genomic variants with drug-induced adverse effects (ADEs), including serious toxicity. While many gene–drug–ADE associations exist, only a subset has sufficient evidence to guide clinical decisions; nonetheless, the review underscores the potential of PGx to mitigate drug toxicity (International Institute of Anticancer Research, 2024).
In a U.S. rural population study, pharmacogenomic single-nucleotide variants were projected to substantially reduce ADR risk and associated healthcare costs; ADRs in the U.S. are estimated to cause over 100,000 fatalities annually and more than USD?136?billion in costs (Williams et al., 2023). Such data underline the public health value of PGx implementation.
In psychiatry, a large-scale real-world study involving 15,000 patients demonstrated that PGx testing (including CYP2D6 CNV analysis and detection of phenoconversion) uncovered novel actionable findings potentially guiding safer and more effective mental health medication prescribing (Molecular Psychiatry, 2024).
4.3. Real-World Implementation: Outcomes & Health Utilization
A prospective observational cohort from mixed outpatient settings (cardiology, internal medicine, primary care) used multigene PGx panel testing (genes: CYP2C9, CYP2D6, CYP2C19, CYP3A4, CYP3A5, VKORC1). On average, ~2 prescribing recommendations per patient were generated; 46?% of the 381 recommendations were followed, leading to a significant decrease in hospitalizations and emergency visits translating into healthcare cost savings (PMed?study, 2025).
These findings show that PGx-guided prescribing can deliver tangible clinical and economic benefits particularly when integrated into real-world care settings with decision support.
4.4. Disease-specific Example: Diabetes
In type 2 diabetes a major public health issue in India variable drug response to non-insulin antidiabetic drugs (NIADs) has been widely observed. The Indian genomic survey (n=1,029) identified numerous PGx variants associated with altered drug response, including a significant excess of alleles linked to poor metformin response compared with global populations (Sivadas et al., 2024).
These data suggest that standard dosing or drug choices may be suboptimal in a substantial fraction of Indian patients; PGx-guided personalization could improve glycemic control, reduce trial-and-error therapy, and mitigate long-term complications.
4.5. Broad Clinical Relevance: Why PGx Matters
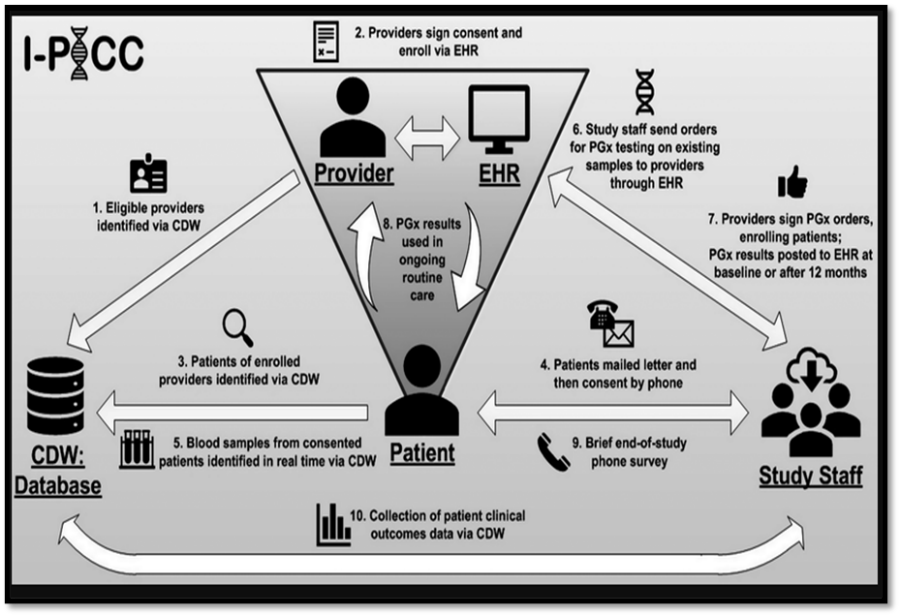
Fig no: 4. Integration of pharmacogenomics into clinical workflow, linking genetic testing, laboratory interpretation, clinician decision-support, and optimized therapy outcomes.
5. Economic and Cost?Effectiveness Evidence
Adoption of PGx-guided therapy often depends on whether it is economically justifiable. A 2022 systematic review of 108 studies on PGx-guided treatments (with CPIC?recommended drugs) found:
In the real?world hospital cohort (CPT 2024), pre?emptive PGx-guided therapy in patients receiving actionable drugs resulted in healthcare cost savings (estimated ~€17.49 per patient over 2 years), even without factoring in testing costs (Clinical Pharmacol Ther, 2024).
Moreover, implementation of PGx-guided prescribing was linked with fewer hospitalizations and emergency department visits in cohort studies indicating potentially large downstream savings, improved patient safety, and resource utilization (PMed 2025).
These economic data reinforce that PGx is not only scientifically useful but can be an economically sound strategy especially when applied pre-emptively in high?risk or chronically medicated populations.
6. REGULATORY, IMPLEMENTATION, ETHICAL, AND PRACTICAL CHALLENGES
Despite strong scientific and economic rationale, PGx implementation remains limited particularly in low- and middle-income countries like India. Key challenges include:
6.1. Lack of Population?Specific Data and Representation
Many PGx databases and guidelines are derived from European or North American populations. Frequency and functional impact of variants often differ in non?European populations. For instance, the Indian genomic survey revealed distinct PGx variant distributions, especially for antidiabetic drugs (Sivadas et al., 2024) and for essential / OTC medications (Kulkarni et al., 2025).
The lack of comprehensive allele-frequency data (e.g., minor allele frequency, MAF) for many drugs in Indian-specific databases remains a barrier (Kulkarni et al., 2025).
Thus, extrapolating PGx data from other populations may lead to inaccurate predictions; robust population-specific studies are essential for clinical validity in ethnically diverse settings.
6.2. Infrastructure and Healthcare Integration
Even where PGx data exist, integration into healthcare systems requires infrastructure: genetics labs, sequencing / genotyping facilities, bioinformatics support, electronic health records (EHRs), clinical decision support (CDS), and trained clinicians. Many settings especially rural or resource-limited lack such infrastructure (IJCRT?2024).
Moreover, clinicians often lack confidence or training in interpreting PGx reports; surveys report low genomic literacy and hesitation to use PGx information without clear institutional guidelines (IJCRT?2024; Dovepress, 2022).
Regulatory frameworks and standardized guidelines for PGx use in many countries are still nascent or absent; this complicates clinical adoption, reimbursement, and integration into prescribing practice (IJCRT?2024; Pharmacology & Clinical Research 2024).
6.3. Cost and Economic Barriers
Although sequencing costs have fallen, PGx testing (especially pre-emptive panel testing) remains expensive particularly in low?resource settings (India and other LMICs). Without insurance coverage or public health policies supporting testing, many patients may not access PGx (IJPS review 2025; Pharmacology & Clinical Research 2024)
Cost-effectiveness analyses often depend on long-term follow-up, high-risk populations, or high medication usage; for sporadic or single drug use, benefit may be modest (Morris et al., 2022).
6.4. Complexity of Genetic Variation and Interpretation
Pharmacogenomic variation is often polygenic; drug response can be influenced by multiple genes, gene–gene interactions, structural variants, rare variants, and regulatory regions not just common SNPs. This complicates interpretation, especially when functional data are lacking (PowerTech Journal review, 2024).
Moreover, many PGx associations are derived from observational studies or retrospective analyses; randomized controlled trials (RCTs) demonstrating improved clinical outcomes (efficacy or reduction in ADRs) remain limited (Systematic review on ADE variants, 2024)
6.5. Ethical, Social, Data?Privacy Issues
Genetic testing raises concerns around consent, data privacy, data sharing, potential misuse (e.g., genetic discrimination), especially in countries lacking robust data protection laws. Without appropriate governance, PGx implementation could exacerbate inequities rather than mitigate them (IJPS review, 2025; Pharmacology & Clinical Research 2024)
Finally, pediatric PGx presents additional challenges: small sample sizes, rare ADRs, lack of standardized phenotype definitions, ethical issues with consent in minors leading to a dearth of robust evidence in children (Pediatrics & Child Health review, 2023)
7. FUTURE PERSPECTIVES
Given the high burden of actionable PGx variants, growing evidence of clinical and economic benefit, and advances in sequencing and bioinformatics, the future of PGx appears promising provided key challenges are addressed. Key future directions include:
Panel testing (covering core pharmacogenes) rather than reactive single-gene assays is increasingly recommended. More than 95?% of individuals harbor actionable variants, and panel testing can guide multiple drug prescriptions over a lifetime (Meyer et al., 2025; Haidar et al., 2022).
For genetically diverse populations (e.g., India, South Asia), there is an urgent need for large-scale genome sequencing, allele-frequency mapping, and functional validation to generate region?specific PGx panels and prescribing guidelines. Studies like Sivadas et al. (2024) and Kulkarni et al. (2025) provide early steps.
Embedding PGx information into EHRs with CDS so that when a clinician prescribes a drug, relevant genotype-based recommendations (drug choice, dose, monitoring) pop up will enhance usability, reduce errors, and encourage uptake (Dovepress, 2022; PMed 2025)
To justify implementation in public health systems (especially in LMICs), more cost–benefit analyses are needed factoring in local disease burden, prevalent drugs, population genetics, and healthcare costs. Evidence to date is promising (Morris et al., 2022; CPT 2024) but under?represented in low-income settings.
PGx can have particular impact in elderly, polypharmacy, chronic diseases (e.g., diabetes, cardiovascular disease, psychiatry), where multiple medications and comorbidities increase risk of ADRs and therapeutic inefficacy. Large real-world cohorts (e.g., PMed 2025, CPT 2024) have started to demonstrate such benefits.
As sequencing becomes widespread, rare variants, CNVs, non-coding variants, regulatory variants, epigenetics, and gene–environment interactions will be uncovered requiring multi?omics approaches, functional studies, and integration into PGx models (PowerTech Review 2024; Schärfe et al., 2017).
For broad adoption, initiatives are needed to raise genomic literacy among clinicians, develop national/regional guidelines, ensure data privacy, equitable access, reimbursement mechanisms, and public awareness especially in LMICs (IJCRT?2024; Dovepress 2022.
8. CONCLUSION
Emerging evidence strongly supports that pharmacogenomics is not a niche or rare?disease tool but a cornerstone for modern, personalized medicine. With more than 80–95?% of individuals carrying at least one actionable PGx variant, and common use of PGx?relevant drugs (NSAIDs, PPIs, antidiabetics, statins, antiplatelets, psychotropics), the potential for population-level impact is vast. Real-world data confirm that PGx-guided therapy can reduce hospitalizations, ADRs, and save costs; economic analyses underline its cost?effectiveness or cost-saving potential, especially when pre-emptive multigene panels are used.
Nevertheless, significant challenges remain especially for countries like India including lack of population-specific data, limited infrastructure, cost and reimbursement barriers, insufficient clinician training, and need for ethical and regulatory frameworks. Addressing these will require coordinated efforts: large-scale genomic sequencing in local populations, building PGx allele databases, integrating PGx into EHR/CDSS, conducting local cost-benefit studies, and establishing national policies to support equitable access.
Given advances in sequencing, bioinformatics, and growing clinical and economic evidence, now is the time for stakeholders researchers, clinicians, policymakers to invest in scalable PGx implementation, particularly in genetically diverse and high-disease-burden regions. If done thoughtfully, pharmacogenomics can realize its promise: safer, more effective, individualized therapy a true cornerstone of precision medicine.
REFERENCES

Shraddha?Lakambare, Tanishka Ubale, Dr. Dhanraj Jadge, Pharmacogenomics: The Future of Personalized Medicine, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 1191-1203. https://doi.org/10.5281/zenodo.17840409
 10.5281/zenodo.17840409
10.5281/zenodo.17840409