NRI College of Pharmacy, Pothavarapadu, Agiripalli Mandal
Substernal chest pain, pressure, or discomfort lasting longer than 30 to 60 seconds is a sign of angina pectoris. It usually gets better with rest and gets worse with physical activity and emotional stress. Angina is now a predictor of major adverse cardiac events, Additionally, angina should be treated because it is a serious morbidity that lowers quality of life. Pharmacologic treatments for angina in the United States include beta-blockers, nitrates, and calcium channel blockers. More sophisticated and efficient treatments are required because a considerable percentage of patients still experience recurrent or ongoing angina after revascularization, despite the fact that it has been demonstrated to alleviate angina and is advised for certain high-risk individuals. Improved external counter pulsation and stem cell therapy are two options for treating refractory angina that is not responsive to standard pharmaceutical treatments or revascularization techniques. Angina remains a major contributor to morbidity. In addition to improving survival and addressing the risk factors for atherosclerotic disease, therapy should focus on preventing or lessening angina and enhancing patient’s capacity for physical activity.
The term "angina pectoris" comes from the Latin word "ANGERE," which means to strangle.[1] Chest pain or discomfort brought on by myocardial ischemia is the hallmark of the clinical syndrome known as angina pectoris. It is a condition in which heart muscle receives an insufficient supply of oxygen-rich blood. Angina is a symptom of acute coronary syndrome and can be further categorized into [2]
STANDARDIZED DEFINITION:
Recurrent substernal chest pain, or angina pectoris, is brought on by coronary artery spasm or atherosclerosis, which impairs the heart's ability to pump blood and oxygen to a particular area. [7]
EPIDEMOLOGICAL STUDIES:
In western nations, there were between 30,000 and 40,000 cases of chronic stable angina per million. For both men and women, the prevalence rises with age. For women and men aged 45–64, the estimated prevalence is 4–7% and 5–7%, respectively. Similarly, for men and women aged 65–84, the estimated prevalence is 14–15% and 10–12%, respectively. [8]
PROGNOSIS:
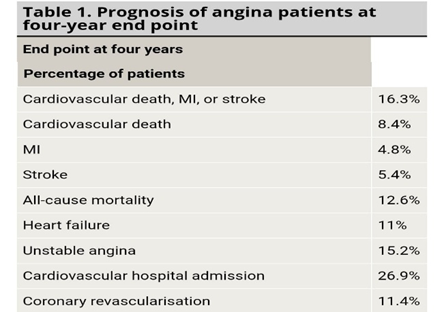
ETHIOLOGY:
Chest pain can be caused by ischemic heart disease, non-ischemic heart disease, or non-cardiac causes. Non-cardiac causes include conditions of the lungs, musculoskeletal disorders, anxiety/panic episodes, and gastro-oesophageal reflux disease. Pericardial disease is one of the non-ischemic cardiac causes. Heart muscle and coronary blood vessel receptors are activated when there is enough oxygen present. The causes of chest pain include: [10]
Other symptoms:
Additional signs of this condition may include: [11]
PATHOPHYSIOLOGY:
Ischemic at the fundamental level elevates anaerobic glycolysis. This results in increased potassium and lactate levels in the venous return of the hydrogen-affected myocardium. The affected area experiences hypokinesia or akinesia as a result of calcium ions conflict with hydrogen ions.[10]
Myocardial ischemia occurs when the heart's oxygen demand is not met by coronary blood flow. As myocardial cells transition from aerobic to anaerobic metabolism, their mechanical, metabolic, and electrical capabilities gradually deteriorate. The myocardium and vessels' biologic and mechanical stimulating of the sensory afferent nerve endings in the coronary arteries is the cause.
Angina's primary chemical mediator can be adenosine. Adenosine is generated when ATP is broken down during ischemia and diffuses into the extracellular space, causing artery dilatation and anginal pain. The main way that adenosine causes angina is by stimulating the A1 receptors in cardiac afferent nerve endings. [12]
The myocardial oxygen demand rises in response to an increase in heart rate and myocardial contractile state. Elevations in both preload (ventricular end-diastolic volume) and afterload (aortic pressure) raise myocardial wall tension and O2 demand.1. Coronary flow reserve, or CFR, is the capacity of the coronary arteries to raise blood flow in response to elevated cardiac metabolic demand. In healthy person, the maximal coronary blood flow after full dilation of the coronary arteries is roughly 4-6times. CFR depends on small large coronary artery resistance, extravascular resistance and blood composition.[13] The most common cause is atherosclerotic plaque formation, which results in fixed coronary artery obstruction. This restricts blood flow during increased myocardial demand. [14]
CLASSIFICATION:
METHODOLOGY
Calcium channel blockers:
Strong first-line antihypertensive medications are calcium channel blockers (CCBs), which include dihydropyridine (DHP) and non-dihydropyridine. 2. They are common medications for patients with peripheral vascular disorders and angina (variant, unstable). [16,17]
STATINS:
In patients with CAD efforts made to lower the LDL level (e.g. with a statin).
Guidelines from the Adult Treatment Panel III (ATP III) are as follows:
The objective for high-risk patients is to have a blood LDL cholesterol level of less than 100 mg/dL. A treatment objective for very high-risk patients is an LDL cholesterol level of less than 70 mg/dL. The suggested LDL cholesterol level in individuals at moderate risk is less than 130 mg/dL; however, a therapeutic threshold of 100 mg/dL is also an alternative. When someone has high triglyceride levels (>200 mg/dL), their non-HDL cholesterol level is a secondary aim of treatment; the objective for them is to have a non-HDL cholesterol level that is 30 mg/dL higher than the target LDL cholesterol level.
Individuals with low HDL levels and established CAD are at significant risk of recurrent events.
The following is the currently recognized management approach:
The main goal of treatment for all individuals with low HDL cholesterol levels is to raise LDL cholesterol levels to the ATP III guidelines using medication, diet, and exercise as necessary. The focus switches to other issues once the targeted LDL level goal is reached.[18]
REVASCULARIZATION:
When the symptoms of hemodynamically severe coronary stenosis do not improve with optimal medical therapy, myocardial revascularization is recommended. Since PCI can relieve the burden of polypharmacy for patients with angina and obstructive CAD, patient preferences should be taken into consideration when determining the degree of antianginal medication. More than one in five patients experience persistent or recurrent angina after PCI, and microvascular dysfunction may be a contributing factor.
Patients with complicated coronary artery disease (CAD), such as those who have had prior coronary artery bypass grafting (CABG) or chronic complete occlusions (CTOs), The success of CTO PCI has significantly increased over the past ten years because to significant advancements in technique, training, and technologies. Angina patients previously considered "unsuitable for intervention" frequently had incomplete revascularization with lesions that can now be treated by skilled operators. [19]
DIAGNOSIS:
It produces the images of the heart to check the heart and its blood vessels for damage or disease. It is invaluable in evaluating many cardiac and great vessel abnormalities. It may be due to evaluate CAD by severe techniques, which gives direct visualization of coronary stenosis blood flow Myocardial viability and cardiac anatomy and function evaluation are among the indications for cardiac MRI. In patients with known or suspected CAD, cardiac MRI, more especially stress perfusion MRI and quantitative myocardial blood flow measurement, may also be recommended for diagnostic and risk assessment.
Creates images of the chest to know the any lung related issues.
Checks for elevated protein levels in the heart, cholesterol levels, and other signs of the inflammation.
It uses the soundwaves to create the image of the heart to see how well the heart is working.[20]
DOSAGE REGIMEN: [21]
Bisoprolol: 1.25-10mg
Isosorbide mononitrate: 30-120mg one time a day (controlled release)
Ramipril: 2.5-10mg daily
Atorvastatin: 10-80mg daily
Rosuvastatin: 5-40mg daily
SIDEEFFECTS:
In general, "adverse effects to angina pectoris" refers to problems, deteriorating circumstances, or negative consequences that could arise from severe, poorly managed, or untreated angina pectoris.[21]
Fatigue, blurred vision, cold hands
Constipation, ankle swelling, flushing
Headaches, dizziness, flushing
Cough, renal impairment, hyperkalaemia
Adjunctive non pharmacological interventions
Myalgia, headache, cramps
CONCLUSION:
These medications widen coronary arteries and lessen myocardial muscle contraction. Myocardial oxygenation rises when the arterioles dilate, and the ischemic myocardial oxygen demand falls when systemic arterial blood pressure falls.
Nifedipine: Nifedipine lowers blood pressure by lessening the effect of high ambient dilatation on smooth muscle tone. Hot flashes, headaches, dizziness, and hypotension are among the side effects; occasionally, the patient stops taking the medicine because of the dizziness and hot flashes.
Verapamil: This medication has anti-arrhythmic effects by lowering the atrial sinus node's automatic power and extending the atrial node's impasse transmission time, which lowers heart rate. 1. Beta-blockers should always be taken carefully, even though this medication lowers heart rate.
Diltiazem: This medication is the most effective at controlling pain because it combines the qualities of both medications. Due to its impairment of myocardial contractility, it is contraindicated in congestive heart failure or should be taken with caution. It is recommended that these medications be taken four to six hours apart.
REFERENCES

Shaek Nasibunnisha, Tripurari Sudeepthi, Ramakuri Gnaneswari, Shaik Shakeera, Mudhigonda Likhitha, Recognizing and Managing the Angina Pectoris, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1353-1359. https://doi.org/10.5281/zenodo.17107067
 10.5281/zenodo.17107067
10.5281/zenodo.17107067
