Department Of Pharmaceutics, Krupanidhi College of Pharmacy, Bengaluru.
Periodontitis represents a chronic inflammatory disorder that impacts the tooth-supporting tissues, resulting in gradual deterioration of tissue and bone structures. Local drug administration has emerged as a focal point in treatment approaches to address the limitations associated with systemic therapeutic interventions, including inadequate site-specific drug concentrations and undesirable side effects. In-situ gel formulations demonstrate considerable potential as they maintain a liquid state during application and transform into gel form when exposed to physiological stimuli such as temperature variations, pH modifications, or ionic alterations. This transformation mechanism ensures extended residence time at the treatment site, continuous drug release patterns, and enhanced bioavailability. Through maintaining optimal therapeutic drug concentrations directly within the periodontal pocket, these formulations improve patient adherence and therapeutic outcomes. Multiple natural and synthetic polymeric materials, encompassing pectin, gellan gum, poloxamers, and xyloglucan, have been investigated for gel formulation development. Their biodegradable properties, application convenience, and controlled release characteristics position them as viable alternatives to traditional periodontal treatment modalities. This review emphasizes the pathophysiology of periodontitis, current therapeutic constraints, and the prospective contribution of in-situ gel drug delivery mechanisms in periodontal treatment.
Periodontal conditions constitute a collection of inflammatory pathologies that impact the gingiva, periodontal ligament, alveolar bone, and cementum. These disorders originate from bacterial biofilm deposition, which elicits both immediate microbial harm and host-driven immunological reactions. During initial phases, gingivitis remains confined to gingival structures, however, without intervention, it advances to periodontitis, distinguished by connective tissue deterioration, alveolar bone loss, and ultimate tooth mobility. Pathogenic bacteria including Porphyromonas gingivalis, Actinobacillus actinomycetemcomitans, and Tannerella forsythia serve as primary etiological agents in disease onset. Host-related variables, encompassing heightened inflammatory responses, additionally expedite structural damage. Beyond localized oral manifestations, periodontitis demonstrates systemic correlations with cardiovascular pathology, diabetes mellitus, rheumatoid arthritis, Alzheimer's disease, and specific malignancies. (1, 2) Traditional therapeutic modalities, encompassing systemic antimicrobial therapy and mechanical instrumentation, frequently encounter limitations including inadequate target-site drug penetration, systemic adverse reactions, and patient adherence issues (3). This has prompted investigation into targeted delivery mechanisms. Within this context, in-situ gel formulations have demonstrated considerable potential owing to their capacity for sol-gel transition within periodontal defects, providing extended residence time and sustained drug release. (4, 5)
Pathogenesis:
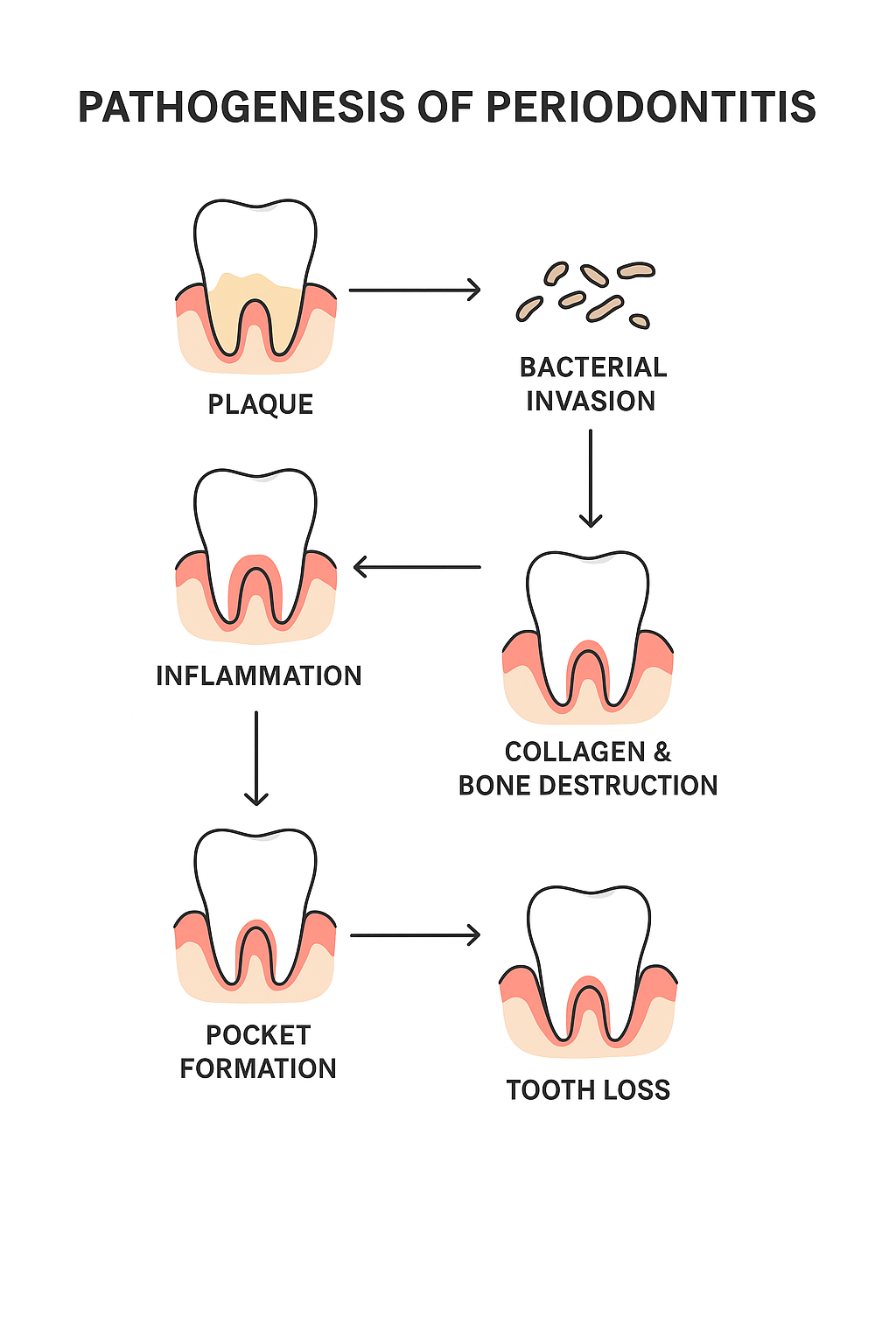
Fig 2: Pathogenesis of Periodontitis
Periodontitis refers to an infectious disease of a chronic character and is the consequence of the cooperation of pathogenic bacteria with a vulnerable host. Although dental plaque biofilm induces the disease, the major factor in tissue loss is excessive immune system response, rather than the microorganisms. The initial phases are gingival inflammation due to deposition of plaque. Without being cured, this advances to the lower periodontal structures, which leads to the destruction of the connective tissue, resorbing of the alveolar bones, and the formation of the periodontal pockets. These pockets develop an environment that prefers to grow anaerobic bacteria which worsens the situation even further. (6) A major determinant in the process of the disease progression is an imbalance of the oral microbiota termed dysbiosis. The red complex of pathogens (Porphyromonas gingivalis, Tannerella forsythia and Treponema denticola) are central to this. These microbes impair microbial homeostasis and excrete virulence factors that destroy periodontal tissues. (7) The host immune system reacts by shedding such inflammatory mediators as interleukin-1-beta (IL-1-beta), tumor necrosis factor-alpha (TNF-alpha), and prostaglandins, which in turn live up collagen lysis and bone resorption (8). Other connective tissue destroying components include the matrix metalloproteinases (MMPs). This forms a loop in which inflammation aids dysbiosis, and dysbiosis causes more inflammation. There are also systemic effects with bacteria and inflammatory mediators reaching the bloodstream, and therefore an association between periodontitis and comorbidities including diabetes, rheumatoid arthritis, and cardiovascular disease. (9, 10)
Periodontitis Classification
Periodontitis has been divided into various categories in order to be able to understand its development and clinically handle it. In 1999, the previous classification categorized the condition into chronic, aggressive, necrotizing periodontitis as well as periodontitis that is associated with systemic diseases. The most common, typically involved in adults, is chronic periodontitis in which the progression of the disease occurs slowly, over time. Its characteristic is attachment loss, gingival recession and resorption of alveolar bone. (11). The aggressive periodontitis is harming younger people and is progressing faster with a genetically predisposed tendency. It can result in premature tooth mobility and loss with little plaque formation. Necrotizing periodontitis is characterized by tissue necrosis, ulceration and pain, and is commonly related to immunosuppression, malnutrition or general disease. Periodontitis associated with systemic diseases is found in patients who have underlying diseases like diabetes, hematologic disorders or genetic disorders that interfere with the host defense. (12, 13)
The modern classification (2017 World Workshop) has provided a staging and grading that helps to more precisely diagnose it:
Stages determine how severe and/or complex to manage disease:
Stage I: Periodontal disease (starting stage)
Stage II: Moderate periodontitis
Stage III: A serious novel complicating with a threat of losing more teeth
Stage IV: advanced disease and threat of full-scale loss of teeth
Extent and distribution reveal whether one has Localized or generalized disease, or in the regions of molar-incisor.
Grades characterise progression and risk factors:
A classification system provides clinicians with greater opportunities to measure the severity of the disease, identify its progression, and formulate an individual treatment plan. (14)
Diagnosis:
Radiographic Evaluation
Horizontal and vertical bone loss, involvement of the furcation, as well as the overall status of alveolar bone, can be diagnosed with the help of intraoral periapical and panoramic radiographs. More detailed three-dimensional assessment is offered with a cone beam computed tomography (CBCT) in complicated cases.
Biomarkers
The research interests where salivary, serum and gingival crevicular fluid (GCF) biomarkers are identified as tools helpful in diagnosis. Cytokines like the interleukin-1 beta, tumor necrosis factor alpha, prostaglandin E- 2 and the matrix metalloproteinases have been described as being typically increased in diseased sites. Systemic inflammatory parameters that have received attention as predictors of disease severity include neutrophil-to-lymphocyte ratios (NLR) or platelet-to-lymphocyte ratios (PLR).
Point of Care Testing (POCT)
More recent technology takes the form of lab-on-a-chip, lateral flow assay, and microfluidics, which provide the ability to identify periodontal biomarkers detection at the point of care. Their objective is to give fast, non-invasive and affordable diagnosis.
Comprehensive Assessment
The diagnosis of this condition is not presented with the help of a single parameter but with the correlation of medical history, the evaluation of risk factors (e.g., diabetes, smoking), clinical data, and radiographic changes. The proposed classification system of 2017 suggests a multidimensional system using staging (severity and complexity) and grading (progression risk) altogether. (15, 16)
Treatment of Periodontitis:
The therapeutic approach to periodontitis centers on infection eradication, inflammation control, and periodontal health restoration. Treatment modalities span from fundamental mechanical debridement to sophisticated regenerative interventions.
Primary Treatment Phase
Patient education and appropriate domestic care constitute the cornerstone of therapeutic intervention, with consistent plaque management through tooth brushing and interproximal cleaning being crucial. Scaling and root planing represents the conventional non-surgical methodology, involving mechanical removal of plaque and calculus deposits from dental surfaces and periodontal pockets. (17, 18)
Supplementary Treatment Approaches
Topical antimicrobial agents, including chlorhexidine gels, minocycline microspheres, or doxycycline chips, are administered directly into periodontal pockets to augment SRP effectiveness. In specific circumstances, systemic antibiotic therapy utilizing metronidazole, tetracycline, or amoxicillin may be considered, although resistance development and adverse effects restrict prolonged application. Host-modulation strategies employing low-dose doxycycline and omega-3 fatty acids have been utilized to diminish destructive inflammatory processes.
Surgical Interventions
Surgical procedures become necessary when non-surgical approaches prove inadequate or in cases of advanced pathology. Resective procedures eliminate pathological tissue and recontour osseous defects. Regenerative approaches, including guided tissue regeneration, osseous grafting, and enamel matrix proteins, facilitate restoration of compromised periodontal structures. Mucogingival procedures address defects such as gingival recession while enhancing esthetic and functional outcomes.
Laser and Photodynamic Treatment Modalities
Laser systems (Er:YAG, diode, Nd:YAG, CO?) and photodynamic therapy can diminish bacterial burden, facilitate healing, and enhance treatment outcomes when utilized as adjunctive measures to conventional therapy.
Implant-Based Treatment
Following tooth loss, dental implants provide a replacement alternative. Nevertheless, peri-implantitis (implant-associated inflammation) presents ongoing challenges, necessitating meticulous planning and maintenance protocols.
Maintenance Protocol
Long-term therapeutic success relies upon supportive periodontal care. Routine recall appointments at 3–6 month intervals enable monitoring of pocket depths, bleeding indices, and osseous levels. Patient adherence to oral hygiene protocols remains essential for preventing disease recurrence. (19, 20)
Risk Factors for Periodontitis:
Periodontitis is a multifactorial disorder that is influenced by microbial components, environmental and systemic factors. It is still essential to understand these contributing factors so that there will be effective prevention and therapeutic management.
Tobacco Consumption
The most important contributing factor that is modifiable is tobacco use Cigarette smoking stimulates immune impairment, reduces gingival blood flow and promotes the establishment of pathogenic bacteria. The tobacco users show deeper pocket, more severe attachment loss, and poor response to therapeutic interventions as compared to non-users. (21, 22, 23)
Diabetes Mellitus
Poorly controlled diabetes increases the chances of periodontitis as well as its severity. Increased glucose levels cause the formation of the advanced glycation end product that leads to the activation of the inflammatory cascade and impairs the tissue repair process. Moreover, periodontitis can worsen glucose control, and there is a mutual relationship between these two pathological conditions.
Cardiovascular Disorders
Periodontitis is related to cardiac diseases through systemic inflammatory responses and spread of bacteria. Inflammatory substances emanating in a periodontium with diseased structures can promote vascular endothelial damage and atherogenesis. (24)
Systemic Inflammatory Response
Periodontitis provokes circulating cytokine and inflammatory mediator, which may complicate the systemic inflammatory burden and increase the risk of chronic disease. (25, 26)
Malignancy
Periodontitis-related recurrent inflammation, bacterial toxins, and disruption of the immune system have been identified with particular cancer development including the oral, gastrointestinal, and lung cancers. (27)
Localised Structural Elements
Condition such as a large matriculation margin, poor contacts, enamel defects, root surface defects, and traumatic occlusion will predispose the attachment to deteriorate should biofilms due to retain there.
Other Influental Factors
Genetic prediscription, psychological stress, hormonal changes (gestation, menopause), malnourishment, immunosuppression also predispose individuals to periodontitis.
IN-SITU GEL:
In-Situ Gel Drug Healthcare Delivery Systems into Periodontitis
Challenges associated with conventional periodontal therapy include the bursting of drugs out of the periodontal pocket, poor retention and systemic effects when orally administered antibiotics are used. In order to reduce these drawbacks, in-situ gelling systems have been developed as drug localized, controlled release systems.
In-Situ-Gel-Principle
In-situ are liquid preparations that when subjected to physiological stimuli (usually temperature, pH, or ionic concentration) it changes to a gel. This transition enables the formulation to spread with ease upon application as a liquid before it is gelated, which promotes prolonged retention and long-lasting clinical drug release at the destination site.
Advantages
In-Situ gel systems have the polymer form a stable gel - characterized by the polymer:
1. Pectin
A naturally occurring polysaccharide, that gels in the presence of the cation calcium. The fact that it is rendered appropriate in controlled release formulation by the property under discussion makes no difference. Applications of pectin-based systems are solvable in water and thus do not require the utilization of organic solvents.
2. Xyloglucan
Xyloglucan can form reversible gels, temperature-dependently, obtained by extraction steps on tamarind seeds. It retains a watery state in low temperatures, but turns into a gel upon heating to therapeutic temperature. This property makes it favorable as the oral and gastrointestinal drug delivery medium.
3. Gellan Gum
This is a polysaccharide coming, once again, by the production of microbes that can form gels at the presence of cationic species such as calcium. It forms strong three dimensional matrices, and is of benefit in the controlled release of oral as well as parenteral formulations.
4. Poloxamers (Pluronics)
These synthetic triblock copolymers have a thermo sensitive controllable gelling behavior They are available in liquid form at room temperature, and when they reach ultra-warm temperature, they gel. The use of formulations that contain poloxamer is widely spread in periodontal therapy due to the excellent flow characteristics and biological acceptance of the material.
5. Additional Polymers
Carbopol, chitosan, and HPMC are commonly added to combination preparations in order to enhance mucoadhesiveness and to increase mechanical stability of gels. (30, 31)
Gelation Mechanisms
Temperature-dependent gelation occurs when formulations transition to gel state at physiological temperature, as observed with poloxamers and xyloglucan compounds (32, 33). pH-responsive systems undergo sol-to-gel transformation following pH variations, exemplified by Carbopol-derived formulations (34). Ionic gelation mechanisms involve gel formation upon exposure to specific cations like calcium, demonstrated in pectin and gellan gum systems.
Clinical Implementation in Periodontal Disease
Upon administration into periodontal spaces, these formulations conform to cavity morphology and establish gel matrices that maintain adherence to dental and gingival tissues. This configuration enables sustained antimicrobial delivery of agents including chlorhexidine, tetracycline, and metronidazole, thereby enhancing localized therapeutic concentrations while minimizing administration frequency requirements.
Current Constraints
Several formulations exhibit potential for rapid initial drug release. Storage stability presents ongoing challenges. Gelation characteristics may fluctuate based on individual patient physiological parameters. Optimization of polymer concentrations and mechanical characteristics requires further refinement.
Emerging Developments
Research initiatives focus on nanoparticle-incorporated in-situ gel systems, combination therapeutic approaches, and stimuli-responsive gel technologies to optimize clinical efficacy. These innovative strategies target both sustained drug delivery and selective antimicrobial activity against drug-resistant bacterial populations and established biofilm structures. (2, 35)
CONCLUSION:
Periodontitis represents a multifaceted inflammatory condition that extends beyond oral cavity implications to encompass broader systemic health consequences. Conventional therapeutic strategies, while demonstrating partial efficacy, face constraints including accelerated pharmaceutical elimination, inadequate target-site drug concentrations, and adherence challenges among patients. In-situ gelification delivery mechanisms offer an encouraging therapeutic option by merging localized administration benefits with sustained-release characteristics. These formulations maintain fluid properties during application and transform into gel matrices upon exposure to physiological triggers, facilitating extended residence within periodontal spaces. The incorporation of polymeric materials including pectin, gellan gum, xyloglucan, and poloxamers enables the creation of biocompatible, biodegradable, and user-acceptable preparations. While preclinical investigations and clinical trials demonstrate their therapeutic potential, obstacles including formulation consistency, initial rapid drug release, and inconsistent gel formation require resolution. Subsequent research endeavors should emphasize innovative methodologies such as nanoparticle-incorporated gels, stimulus-responsive platforms, and multipurpose drug delivery vehicles to optimize therapeutic efficacy.
In summary, in-situ gel systems constitute a notable advancement in periodontitis management, presenting opportunities for enhanced patient compliance, diminished systemic adverse effects, and improved periodontal tissue restoration.
REFERENCES


Nithyasri J.*, Dr. Eswar Gupta Maddi, Review on In-Situ Gel Drug Delivery System for Periodontitis, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 3000-3009 https://doi.org/10.5281/zenodo.16992664
 10.5281/zenodo.16992664
10.5281/zenodo.16992664
