
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Raosaheb Patil Danve College of Pharmacy Badnapur, Jalna.
Buccal route provides direct entry into the systemic circulation (blood) by avoiding the hepatic first-pass effect and degradation in the gastrointestinal tract (GIT), There are various transmucosal routes available but buccal route was found to be the most convenient and easily approachable route for the delivery of therapeutic agents for both local and systemic delivery. Buccal mucosa well positioned to increase the bioavailability of various drugs and bioadhesion. This paper include advantages, limitations, mechanism of buccal absorption, structure of buccal mucosa, theory of buccal mucosa, mucoadhesive polymer, investigated buccal tablets, permeation enhancer, evaluation parameters, commercially available buccal adhesive tablets. Adhesion as a process, simply defined as the “fixing.
Buccal delivery, is drug administration through the mucosal membranes lining the cheeks (buccal mucosa), Adhesion as a process, simply defined as the ‘‘fixing” of two surfaces to each other. There are different conditions of adhesion depending upon the environment in which process occurs. When adhesion occurs biologically it’s normally known as bioadhesion. Bioadhesion may be defined as the condition in which two materials, in which at least one is of a biological nature, held together for long period of time by interfacial forces. Conventional dosage forms for drug delivery through the oral mucosa include chewable tablets, buccal tablets, sublingual tablets and solutions. But a major qty. of the drug in these systems may be unavailable due to swallowing by mistake and a very short residence time, due to masticate, speak or other mouth activity and hence sustained release usually do not within the scope of such formulations1-2.
Amongst the various routes of drug delivery, oral route is the most preferred to patient and clinician alike. Peroral administration of drugs has disadvantages such as first pass metabolism and enzymatic degradation within the GI tract, that prohibit oral administration of certain classes of drugs especially peptides and proteins. Consequently, other absorptive mucosae are considered as potential sites for drug administration. Transmucosal routes of drug delivery offer distinct advantages over peroral administration for systemic drug delivery10.
Buccal mucosa as a site for drug delivery 1, 3.
There are two permeation pathways for passive drug transport across the oral mucosa: Paracellular and transcellular routes. Permeants may traverse these two routes simultaneously, but one route usually is more effective than the other, depending on the physicochemical properties of the diffusant Because the intercellular spaces are less lipophilic in character than the cell membrane, hydrophilic compounds have higher solubility’s in this environment. The cell membrane, however, is highly lipophilic in nature, and hydrophilic solutes have great difficulty permeating the cell membrane because of a low partition coefficient. Therefore, the intercellular spaces pose the major barrier to passive permeation of lipophilic compounds, and the cell membrane acts as the major transport barrier for hydrophilic compounds. Because the oral epithelium is stratified, solute permeation may involve a combination of these two routes. The route that predominates, however, is generally the one that provides the least amount of hindrance to passage. Delivery of drugs within the
Delivery of drugs within the oral mucosal cavity3
It is classified into three categories
1) Sublingual delivery: Is the administration of drug via sublingual mucosa (membrane of the ventral surface of the tongue and floor of the mouth) to systemic circulation. The sublingual mucosa is relatively permeable, giving rapid absorption and acceptable bioavailability of many drugs, and is convenient, accessible, and generally well accepted. The sublingual route is by far the most widely studied of these routes. Sublingual dosage forms are most often one of two designs: those composed of rapidly disintegrating tablets and those consisting of soft gelatin capsules filled with liquid drug. Such systems create a very high drug concentration in the sublingual region before they are systemically absorbed across the mucosa.
2) Buccal delivery: is the administration of drug via buccal mucosa (the lining of cheek) to the systemic circulation. The buccal mucosa is considerably less permeable than sublingual area, and is generally not able to provide rapid absorption and good bioavailability seen with sublingual administration. 3) Local delivery: for the treatment of conditions of oral cavity, principally ulcers, fungal conditions and periodontal disease. These oral mucosal sites differ greatly from one another in terms of anatomy, permeability to an applied drug and their ability to retain a delivery system for a desired length of time. Even though sublingual mucosa is relatively more permeable than buccal mucosa, it is not suitable for a retentive oral transmucosal delivery system. The sublingual region lacks an expanse of smooth and immobile mucosa and is constantly washed by a considerable amount of saliva, making device placement difficult. The preferred site for retentive oral transmucosal delivery systems and for sustainedand controlled-release delivery devices is the buccal mucosa, mainly because of differences in permeability characteristics between the two regions and the buccal mucosa’s expanse of smooth and relatively immobile mucosa.
Overview of Buccal Mucosa[3]
A. Structure: The oral mucosa is anatomically divided into
1) Epithelium: The epithelium consists of approximately 40–50 layers of stratified squamous epithelial cells having thickness 500-800μm. The epithelium of oral mucosa serves as a protective covering for tissues and a barrier to the entry of foreign materials.
2) Basement Membrane and Connective Tissue: The basement membrane (BM) is a continuous layer of extracellular materials and forms a boundary between the basal layer of epithelium and the connective tissues. Connective tissue, along with basement membrane, is not considered to influence the diffusion of most compounds of pharmacological interest although these two regions may limit the movement of some macromolecules and complexes.
B. Buccal Mucosa Environment 2,3: The oral cavity is marked by presence of saliva produced by salivary glands and mucus which is secreted by major and minor salivary glands as part of saliva.
Role of Saliva:
Role of Mucus:
Pathways of Drug Absorption from buccal mucosa 2:
Two major routes are involved: Transcellular (intracellular) and Paracellular (intercellular) . The transcellular route may involve permeation across the apical cell membrane, intracellular space and basolateral membrane either by passive transport (diffusion, PH partition) or by active transport (facilitated and carrier-mediated diffusion, endocytosis). The transcellular permeability of drug is a complex function of various physicochemical properties including size, lipophilicity, hydrogen bond potential, charge and conformation. Transportation through aqueous pores in cell membranes of epithelium is also possible for substances with low molar volume (80 cm3/mol). The second route, available to substances with a wide range of molar volumes, is the intercellular route (paracellular route).within the intercellular space, hydrophobic molecules pass through the lipidic bilayer, while the hydrophilic molecules pass through the narrow aqueous regions adjacent to the polar head groups of the lipids.
Structure and Design of Buccal Dosage Form:2
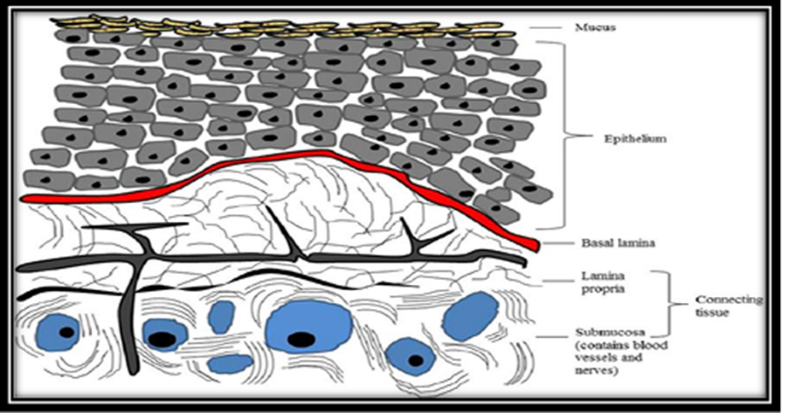
Fig 1. Structure of buccal mucosa
Buccal Dosage form can be of;
1. Matrix type: The buccal patch designed in a matrix configuration containing drug, adhesive, and additives mixed together.
2. Reservoir type: The buccal patch designed in a reservoir system contains a cavity for the drug and additives separate from the adhesive. An impermeable backing is applied to control the direction of drug delivery; to reduce patch deformation and disintegration while in the mouth; and to prevent drug loss
Factors affecting drug delivery via buccal route 3:
Oral cavity is a complex environment for drug delivery as there are many interdependent and independent factors which reduce the absorbable concentration at the site of absorption.
1. Membrane Factors: These involve degree of keratinization, surface area available for absorption, mucus layer of salivary pellicle, intercellular lipids of epithelium, basement membrane and lamina propria. In addition, the absorptive membrane thickness, blood supply/ lymph drainage, cell renewal and enzyme content will all contribute to reducing the rate and amount of drug entering the systemic circulation.
2. Environmental Factors A. Saliva: Thin film of saliva coats lining of buccal mucosa throughout and is called salivary pellicle or film. The thickness of salivary film is 0.07 to 0.10 mm. Thickness, composition and movement of this film affects the rate of buccal absorption.
B. Salivary glands: The minor salivary glands are located in epithelial or deep epithelial region of buccal mucosa. They constantly secrete mucus on surface of buccal mucosa. Although, mucus helps to retain mucoadhesive dosage forms, it is potential barrier to drug penetration.
C. Movement of buccal tissues: Buccal region of oral cavity shows less active movements. The mucoadhesive polymers are to be incorporated to keep dosage form at buccal region for long periods to withstand tissue movements during talking and if possible during eating food or swallowing.
3. Formulation related factors 3:
A. Molecular size: Smaller molecules (75 100 Da) generally exhibit rapid transport across the mucosa, with permeability decreasing as molecular size increases. For hydrophilic macromolecules such as peptides, absorption enhancers have been used to successfully alter the permeability of buccal epithelium, making this route more suitable for delivery of larger molecules.
B. Partition coefficient: partition coefficient is a useful tool to determine the absorption potential of a drug. In general, increasing a drug’s polarity by ionization or hydroxyl, carboxyl, or amino groups, will increase the water solubility of any particular drug and cause a decrease in lipid water partition coefficient. Conversely, decreasing the polarity of a drug (e.g. adding methyl or methylene groups) results in an increased partition coefficient and decreased water solubility.
C. pH: partition coefficient is also affected by pH at the site of drug absorption. With increasing pH, the partition coefficient of acidic drugs decrease while that of basic drugs increase. Partition coefficient is also an important indicator of drug storage in fat deposits. Obese individuals can store large amounts of lipidsoluble drug in fat stores. These drugs are dissolved in lipid and are a reservoir of slow release from these fat deposits.
D. pKa: Ionization of a drug is directly related to both its pKa and pH at the mucosal surface. Only the nonionized form of many weak acids and weak bases exhibit appreciable lipid solubility, and thus the ability to cross lipoidal membranes. As a result, maximal absorption of these compounds has been shown to occur at the pH at which they are unionized, with absorbability diminishing as ionization increases.
Attractiveness of Buccoadhesive drug delivery system4:
Advantages of buccoadhesive drug delivery system: - Drug administration via the buccoadhesive drug delivery offers several advantages such as 1- 6
Limitations of buccoadhesive drug delivery system 1-5:-
There are some limitations of buccal drug delivery system such as-
Methods of preparation of buccal patches [6]
1. Solvent casting:
In this method, all patch excipients including the drug co-dispersed in an organic solvent and coated onto a sheet of release liner. After solvent evaporation a thin layer of protective backing material is laminated onto the sheet of coated release liner to form a laminate that is die-cut to form patches of desired size and geometry.
2. Direct milling:
In this, patches are manufactured without the use of solvents. Drug and excipients are mechanically mixed by direct milling or by kneading, usually without the presence of any liquids. After the mixing process, resultant material is rolled on a release liner until desired thickness is achieved. The backing material is then laminated as previously described. While there are only minor or even no differences in patch performance between patches fabricated by two processes, solvent-free process is preferred because there is no possibility of residual solvents and no associated solvent-related health issues.
3. Solid dispersion extrusion:
In this method immiscible components are extrude with drug and then solid dispersions are prepared Finally the solid dispersions are shaped in to films by means of dies.
4. Semisolid casting:
In semisolid casting method first a solution of water soluble film forming polymer is prepared The resulting solution is added to a solution of acid insoluble polymer (cellulose acetate phthalate, cellulose acetate butyrate), which was prepared in ammonium or sodium hydroxide Then appropriate amount of plasticizer is added so that a gel mass is obtained Finally the gel mass is casted in to films or ribbons using heat controlled drums. Thickness of the film is about 0.015-0.05 inches. The ratio of the acid insoluble forming polymer should be 1:4.
5. Rolling Method:
In rolling method solution or suspension containing drug is rolled on a carrier. The solvent is mainly water and mixture of water and alcohol. The film is dried on rollers and cut in to desired shapes and sizes.
6. Hot melt extrusion:
In hot melt extrusion method, first the drug is mixed with carriers in solid form Then the extruder having heaters melts the mixture Finally the melt is shaped in to films by dies There are certain benefits of hot melt extrusion, Fewer operation units, Better content uniformity, An anhydrous process. Evaluation of buccal patches 9, 10
Evaluation of buccal patches 9, 10
Surface pH :
For the determination of surface pH combined glass electrode are used. The patches are kept in contact with 5 ml of distilled water for 1 hr. The pH can be noted by bringing the electrode near the surface of formulations and allowing it to equilibrate for 1 min.
Weight Uniformity and thickness:
Three samples of each patch (1.5 cm×1.9 cm) are randomly taken and each patch is weighed individually. The data is analyzed for mean weight and 9 standard deviation. Thickness of samples from each patch is measured in tri
Content Uniformity:
Drug content uniformity is determined by dissolving each patch in 10 ml of solvent and filtering it with Whatman filter paper (0.45 μm). The filtrate is evaporated and drug residue dissolved in 100 ml of phosphate buffer (pH 6.8). The 5 ml solution is diluted with phosphate buffer (pH 6.8) up to 20 ml, filtered through a 0.45-μm Whatman filter paper, and absorbance is measured using a UV Spectrophotometer against pH 6.8 phosphate buffer use as blank. The experiments are performed in triplicate, and average values are reported.
Folding Endurance The folding endurance of patches:
It is determined by repeatedly folding one patch at the same place till it break or up to 300 times without breaking. The experiments are performed in triplicate, and average values are reported. plicate and average values are reported.
Percentage moisture loss:
This test is carried out to check the integrity of films at dry condition. Three 1-cm diameter films are cut out, weighed accurately, and kept in desiccators containing fused anhydrous calcium chloride. After 72 hours, the films are removed and weighed. Average percentage moisture loss of three films is found out.
Water absorption capacity test:
Circular Patches, with a surface area of 2.3 cm2 are allowed to swell on the surface of agar plates prepared in simulated saliva (2.38 g Na2HPO4, 0.19 g KH2PO4, and 8 g NaCl per liter of distilled water adjusted with phosphoric acid to pH 6.7), and kept in an incubator maintained at 37°C ± 0.5°C. At various time intervals (0.25, 0.5, 1, 2, 3, and 4 hours), samples are weighed (wet weight) and then left to dry for 7 days in a desiccator over anhydrous calcium chloride at room temperature till constant weight is recorded. Water uptake (%) is calculated using the following equation Water uptake (%) = (Ww – Wf) /Wf × 100 Where, Ww is the wet weight and Wf is the final weight.
Characterization of Drug Release:
Two methods are used to characterize drug release from patches one is simple dissolution using a modified paddle method. Special flasks containing 100 ml of dissolution medium are used. A second method uses a diffusion cell for determining drug release and considered an improvement over dissolution in that only one face of patch is in contact with the medium via a hydrated hydrogel, a situation that more closely mimics the moist surface of buccal cavity.
NEED OF STUDY :-
The development of bacchoadhesive (mucoadhesive) tablets has gained significant attention in modern pharmaceutics because of their unique ability to adhere to the mucosal surfaces of the body and provide controlled or localized drug delivery. Conventional oral dosage forms often face challenges like short gastric residence time, enzymatic degradation, low bioavailability, and frequent dosing, which limit their therapeutic efficacy. To overcome these limitations, bacchoadhesive tablets offer several advantages.
1. Prolonged Residence Time:
By adhering to the mucosal lining of the gastrointestinal tract or other mucosal tissues, bacchoadhesive tablets remain in place for a longer duration, ensuring sustained drug release.
2. Improved Bioavailability:
Drugs that undergo extensive first-pass metabolism or have poor solubility can achieve better absorption and higher bioavailability through buccal or other mucosal routes.
3. Controlled and Sustained Release:
These tablets allow drugs to be released slowly and in a controlled manner, reducing fluctuations in plasma drug levels and enhancing therapeutic efficacy.
4. Patient Compliance:
The reduced frequency of dosing and ease of administration enhance patient convenience and compliance, which is especially beneficial for chronic therapies.
5. Avoidance of First-Pass Metabolism:
Drugs absorbed through mucosal tissues (like buccal or sublingual) directly enter systemic circulation, bypassing hepatic metabolism, which is advantageous for drugs unstable in the liver.
6. Targeted and Localized Action:
For local conditions (such as oral ulcers, gingivitis, or periodontal infections), bacchoadhesive tablets provide site-specific delivery, reducing systemic side effects.
7. Wide Applications:
These systems are useful in delivering a wide range of drugs including peptides, proteins, and drugs with narrow absorption windows, which cannot be efficiently delivered through conventional tablets.
AIM AND OBJECTIVE:-
Aim :- Review On Baccoadhesive Tablet.
OBJECTIVE:-
CONCLUSION
Buccoadhesive tablets represent an innovative approach to drug delivery. By adhering to the buccal mucosa,they by pass hepatic metabolism, provide controlled release, and improve bio availability. With the availability of advanced polymers and modern formulation techniques, these systems are increasingly applied for systemic as well as local therapy. Recent innovations such as nanotechnology and 3D printing further strengthen their future prospects. Thus, buccoadhesive tablets stand as a significant contribution to modern pharmaceutics and patient centered therapy.
Mucoadhesive systems prolongs the residence time of the dosage form at the site of application or absorption and facilitates an intimate contact of the dosage form with the underline absorption surface and thus contributes to improved and/or better therapeutic performance of the drug. It is the developing area whose goal is the development of new devices and more “intelligent” polymers with the great influx of new molecules elucidate from drug research. mucoadhesive systems may play an increasing role in the development of new pharmaceuticals. For safe and effective buccal permeation, absorption enhancer is a crucial component for a prospective future in the area of buccal drug delivery.
SUMARRY :-
Bacchoadhesive tablets represent an advanced drug delivery system designed to improve the therapeutic efficacy and patient compliance of conventional oral dosage forms. These tablets adhere to the mucosal surfaces of the buccal cavity, allowing for prolonged residence time and controlled release of drugs. Unlike traditional tablets, which undergo first-pass metabolism and may show poor bioavailability, bacchoadhesive tablets bypass hepatic metabolism and enable direct absorption into the systemic circulation through the buccal mucosa.
The concept of bioadhesion relies on the interaction between polymeric excipients and the mucin layer covering mucosal tissues. Various natural and synthetic polymers, such as carbopol, chitosan, HPMC, and sodium alginate, are widely used to formulate bacchoadhesive tablets due to their excellent swelling, hydration, and adhesive properties. The choice of polymer and drug release modifiers plays a crucial role in achieving optimum adhesion, drug release kinetics, and patient acceptability.
FUTURE OF SCOPE :-
1. Advanced Drug Delivery
Bacchoadhesive systems can be designed for controlled and sustained drug release, minimizing dosing frequency and enhancing patient adherence. This is especially beneficial for chronic diseases requiring long-term therapy.
2. Targeted Delivery
Future research can explore site-specific drug delivery through bacchoadhesive tablets, ensuring localized action (such as gastrointestinal, buccal, or vaginal delivery), thereby reducing systemic side effects.
3. Integration with Nanotechnology
Incorporating nanocarriers, nanoparticles, or micelles into bacchoadhesive formulations could further enhance absorption, penetration, and bioavailability of poorly soluble drugs.
4. Herbal and Natural Formulations
The use of natural bioadhesive polymers and herbal actives can open new opportunities for safe, biocompatible, and patient-friendly formulations. This aligns with the growing global demand for herbal and green pharmacy.
5. Personalized Medicine
With the advancement of pharmacogenomics, bacchoadhesive tablets can be customized to meet individual patient requirements, enabling precision therapy.
6. Commercial Applications
Development of cost-effective and scalable manufacturing techniques will allow bacchoadhesive tablets to enter the global market, making them competitive alternatives to conventional dosage forms.
7. Combination Therapy
Future formulations may incorporate multiple drugs within a single bacchoadhesive tablet, allowing synergistic effects and improved therapeutic outcomes in complex conditions like diabetes, cardiovascular diseases, or cancer.
8. Regulatory and Clinical Studies
With more clinical evidence and regulatory approvals, bacchoadhesive technology could become a mainstream drug delivery system, widely accepted in hospitals and healthcare setups.
REFERENCES


Suchita Lathi, Shaikh Shahebaj, Baliram Sable, Pawan Hanute, Review on Baccoadhesive Tablet, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 813-824. https://doi.org/10.5281/zenodo.17816849
 10.5281/zenodo.17816849
10.5281/zenodo.17816849