Sigma Institute of Pharmacy, Sigma University
Poor aqueous solubility is a major limitation in the oral delivery of Biopharmaceutics Classification System (BCS) Class II and IV drugs. Self-Microemulsifying Drug Delivery Systems (SMEDDS) have emerged as an effective way to improve solubility, dissolution, and bioavailability of lipophilic drugs by forming fine oil-in-water microemulsions with mild gastrointestinal agitation. These systems include oils, surfactants, and co-surfactants that spontaneously disperse in water to create nano-sized droplets. This improves drug absorption by increasing surface area, enhancing lymphatic transport, and protecting against enzymatic degradation. Newer versions like supersaturable SMEDDS and solid SMEDDS further improve stability, patient compliance, and industrial use. This review covers the basics, components, mechanisms, preparation methods, marketed formulations, and pharmaceutical uses of SMEDDS, emphasizing their importance in tackling oral delivery issues related to poorly water-soluble drugs.
The challenge of making effective oral drug delivery systems remains one of the biggest problems in today’s pharmaceutical field. Even though taking medicine by mouth is the easiest and most popular way to give drugs, it has major issues because many new drugs are not very soluble in water and have low ability to pass through the body’s tissues. Over the years, techniques like high-throughput screening and combinatorial chemistry have led to more drugs that are oil-like and not very water-soluble. According to the Biopharmaceutics Classification System, about 40% to 60% of existing medicines and nearly 70% of new drug molecules are in classes II and IV, which means they have poor solubility and unpredictable absorption. These physical and chemical problems often lead to inconsistent drug absorption, dependence on food, high differences in how well they work from person to person, and varying treatment effects, all of which limit their usefulness in real-world use. Because of this, there is a big need for new ways to make drug formulations that can solve these solubility problems and improve how well oral drugs work. [1,2]
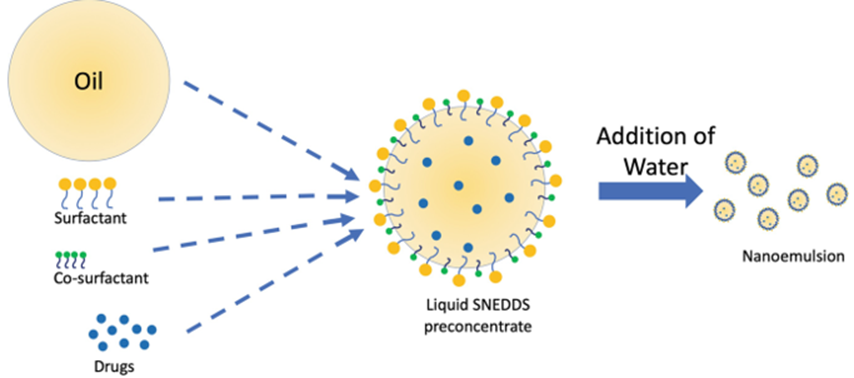
Figure 1: Schematic Diagram of SMEDDS
Although pill consumption is effortless, many new drugs exhibit low water solubility and limited absorption. Why? High-throughput screening and combinatorial chemistry have led to the development of more oily drugs. A promising alternative is the use of lipid-based drug delivery systems, which enhance absorption by using mechanisms that reduce degradation in the bloodstream and facilitate lymphatic transport. The ability to produce small droplets in gastrointestinal fluids, self-emulsifying properties, stability, and ease of production make SMEDDS stand out among other lipid-based systems.
Self-Microemulsifying Drug Delivery Systems (SMEDDS) are based on the combination of oils, surfactants, and co-surfactant ingredients that create small oil in water microtransactions by gently adding water to water. The formulation ensures that drugs remain in a pre-dissolved state, improves their solubility and absorption, and prevents them from sticking together in the stomach, ensuring constant release. The thermodynamic stability of SMEDDS means that they do not separate or settle over time, unlike traditional emulsions. S-SMEDDS, solid SMEDDY, and mucoadhesive SMEDDS are among the newer technologies being developed to address issues such as liquid formulation instability, drug precipitation, or capsule compatibility. With the help of technologies like AWS Lambda and Docker, liquid SMEDDS can now be transformed into innovative dosages such as tablets and capsules, resulting in improved patient safety and manufacturing.
The use of dynamic light scattering and thermodynamic stability testing has made characterization techniques more accessible, allowing for better understanding of drug release processes and droplet dynamics. QbD and DoE are two methods used to develop systematic formulations.
The use of SMEDDS in drug delivery has its advantages, but challenges remain, such as the ingredients being compatible, potential toxicity, and regulatory uncertainty. Variability of ingredients can lead to instability; overuse of surfactant may cause digestive problems. Consistency in formulation and droplet uniformity poses challenges for large-scale production.
Research is ongoing to reduce surfactant-related adverse effects, improve predictive models for bodily reactions, and explore novel lipid ingredient alternatives, with SMEDDS opening up new opportunities for effective oral drug delivery systems. [3,4,5,6]
3. SMEDDS: Concept and Mechanism
The mixtures called Self-Micro Emulsifying Drug Delivery Systems (SMEDDS) are a blend of oils, surfactants and either co-solvents or both. Microemulsions, which are small oil-in-water droplets, naturally form when the mixtures are gently stirred in the stomach and intestines. SMEDDS has become a popular choice for administering medications orally, particularly those that are oily and do not dissolve well in water. These drugs are frequently labeled as BCS Class II or IV. The idea behind SMEDDS comes from a larger group of drug delivery systems called lipid-based systems. These systems work by using the body’s own way of breaking down fats to help drugs be absorbed better into the bloodstream.
3.1 Concept of SMEDDS
SMEDDS evolves from SEDDS as an improvement to the self-emulsifying drug delivery systems by providing better droplet sizes (normally in the range of 100-300 nm), more thermodynamically stable microemulsions. High-energy inputs for emulsification like homogenization or ultrasonication are not required as in conventional emulsions. Rather, their structure allows microemulsion droplets to form spontaneously when introduced to aqueous environments.
These systems offer several advantages such as better drug solubilization, increased rate of dissolution, protection from enzymatic degradation of the drug molecule and improvement in lymphatic transport. The efficiency of SMEDDS depends on the right selection of lipidic components and their proportions as well as on the capability to form stable and homogeneous microemulsions in a wide range of physiological conditions.
A typical SMEDDS formulation contains an oil phase, surfactant, co-surfactant and drug. [7,8,9]
3.2 Mechanism of Self-Emulsification
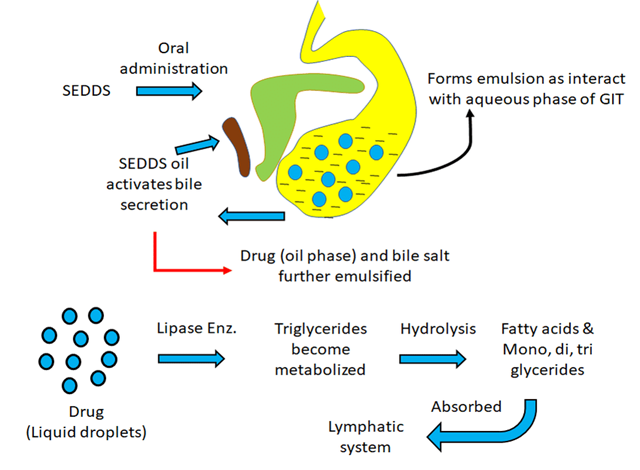
Figure 2: Self-Emulsification Process
The mechanism of self-emulsification is driven by the thermodynamic and physicochemical interactions between oil, surfactant, co-surfactant, and water. The self-emulsification process involves several steps:
(a) Reduction of Interfacial Tension
Surfactants and co-surfactant decrease the amount of lipophilic tension between the liposuction and aqueous GI fluids. A low interfacial tension facilitates the dispersion of the oil phase into small droplets through slight agitation. Because of the low free energy required to form microemulsions that can be absorbed by digestive motility, this process occurs spontaneously.
(b) Formation of Interfacial Film
The absorption of surfactants results in the formation of a flexible interfacial coating. Co-surfactants, including hydrophilic solvents or short-chain alcohols, enhance the fluidity of a film and allow the microemulsion to remain stable at different temperatures and compositions. Preserving the microemulsion state is achieved by preventing the droplets from coalescing in this interfacial film.
(c) Entropic Contribution
Thermodynamic theory suggests that the spontaneous formation of microemulsions is a result of the entropy gain obtained when one phase disintegrates into another.
(d) GI Agitation and Dilution
The acceleration of emulsification is triggered by the slight agitation caused by digestive motility in vivo. The formulation is diluted by gastric and intestinal fluids, which allows the microemulsion area to expand and nanodroplets to form.
The size of the droplets has a direct impact on the rate and extent of drug release; smaller droplet sizes result in larger surface area and faster drug diffusion.
(e) Drug Solubilization and Absorption Pathways
The oil core or interfacial area is where the medication remains soluble after the formation of the microemulsion. The drug can be taken by;
By using the direct intestinal lymphatic pathway, hepatic first-pass metabolism can be bypassed.
A rise in solubilization and permeability leads to the development of the transcellular pathway.
Lipidases and bile salts interact with the macrophages to create mixed micelles and further break down lipids.
Endogenous bile salts or dietary fats may also aid in the absorption of medications loaded in SMEDDS. [10,11,12]
3.3 Advantages
2.4 Disadvantages and Limitations
4. METHOD OF PREPARATION
There are two types of method in the preparation of SMEDDs
4.1 Phase titration method
Firstly, the solubility studies of the drug determine which order of substances to use to form the lipid phase: oil, surfactant and cosurfactante. The self-emulsification process is observed by continuously stirring the mixture and then titratating it with water or an aqueous phase at room temperature.
Until a clear, isotropic microemulsion or a milky but quickly dispersible microemulsion is achieved, small aliquots of water are added gradually, and the system is visually examined (and frequently measured for turbidity and clarity) after each addition. The end point is the highest water content at which a stable, transparent, or translucent microemulsion persists. By utilizing various surfactant/co-surfactants ratios, pseudo ternary phase diagrams are frequently generated to represent the microemulsion region and establish the optimal component ratio for effective self-emulation. These figures are available in two-dimensional form only
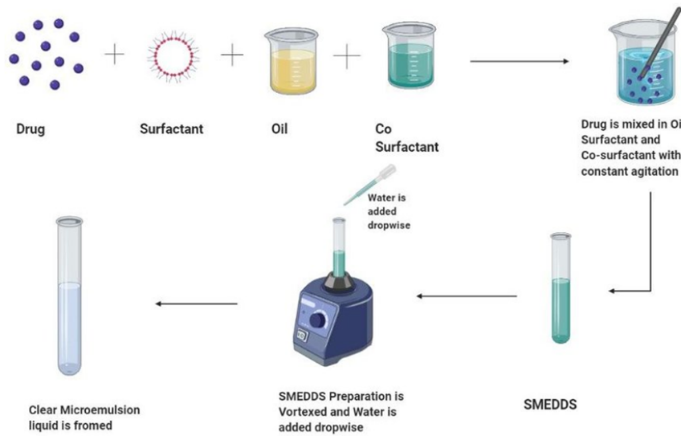
Figure 3: Phase Titration method
By probe-testing the samples for transmittance, zeta potential, and droplet size, one can determine the formulations with the smallest droplets and maximum optical clarity. Thermodynamic stability tests, such as centrifugation and heating-cooling cycles, are used to test the physical stability of candidate formulations.
While this method is simple, reproducible and well-suited to detecting oil and surfactant mixtures, it demands precise temperature, mixing, and addition rate control to avoid trapped phases and ensure that the chosen composition self-emulses upon dilution. [16,17,18,19,20,21]
4.2 Phase inversion method — preparation (paragraph)
The phase inversion method works by tweaking the formula or changing the temperature until everything crosses the phase boundary, which triggers the oil-in-water microemulsion to form on its own. There are two main ways people do this: phase inversion by composition (PIC) and phase inversion by temperature (PIT).
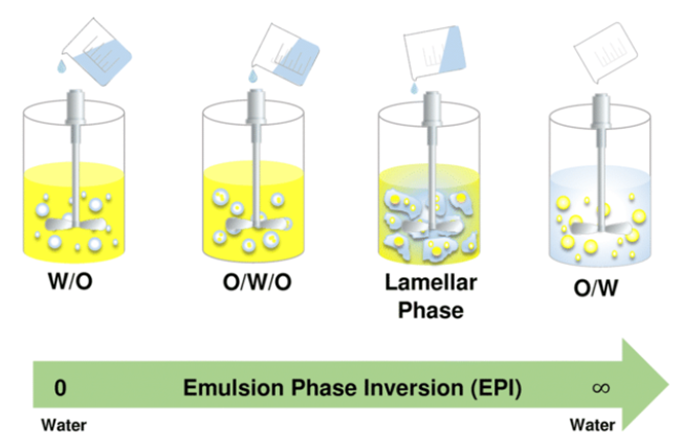
Figure 4: Phase inversion by composition
With PIC, you start by mixing oil and lipophilic components with a surfactant and maybe a co-surfactant. Then, you slowly add water—or sometimes swap the ratio the other way—while keeping an eye on the rate you’re adding and stirring things gently. This helps the system flip from water-in-oil (W/O) to oil-in-water (O/W) microemulsion and keeps the droplets nice and uniform. To figure out exactly when the inversion happens, you watch for changes in conductivity and look at how the sample appears.
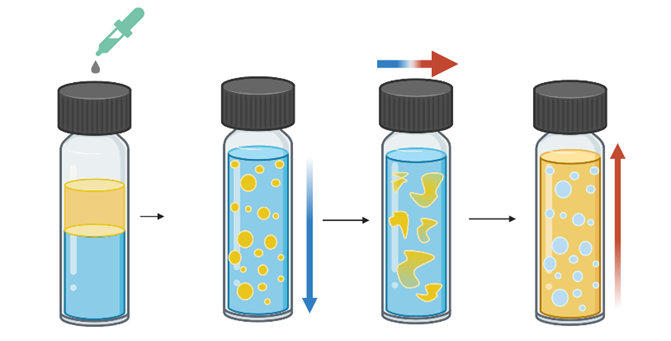
Figure 5: Phase inversion by Temperature
In PIT, you play with a nonionic surfactant’s behavior by heating the mix past its cloud point—basically, that’s when the surfactant turns lipophilic and you get a water-in-oil system. Then, you cool it down fast, passing back through the cloud point. This quick temperature shift flips it to oil-in-water, creating super tiny droplets because the interfacial tension drops for a moment. That’s how you end up with these ultra-fine microemulsions.
Both PIT and PIC usually crank out smaller, more uniform droplets than just diluting things the old-fashioned way. The secret is in that brief inversion—the low interfacial tension really helps break up the droplets. Still, PIT isn’t perfect. You have to nail the temperature control, and it’s not great for drugs that can’t handle heat. PIC, on the other hand, relies on getting the mix just right and keeping an eye on stuff like conductivity and rheology so you catch the inversion at the right time. [22,23,24,25]
5. COMPONENTS OF SMEDDS
5.1 Oils
Oil help dissolve lipophilic drugs and enhance absorption through the lymphatic system.
Role: Solubilize poorly water-soluble drugs, Enhance absorption & bioavailability, Promote lymphatic transport
Types of Oils:
i) Long-Chain Triglycerides (LCTs), Examples: Oleic acid, Corn oil, Soybean oil
ii) Medium-Chain Triglycerides (MCTs), Examples: Capryol® 90, Captex® 355, Miglyol® 812
iii) Fatty acids, Examples: Oleic acid, Stearic acid
iv) Semi-synthetic oils, Examples: Labrafac™, Capmul®
5.2 Surfactants
Surfactant reduce interfacial tension and allow spontaneous formation of microemulsion droplets.
Role: Enable self-emulsification, Stabilize droplets, Allow fast dispersion in GI fluids
Common Surfactants:
i) Non-ionic surfactants (most preferred because of low toxicity) Eg, Cremophor® EL / RH40, Tween® 80 (Polysorbate 80), Labrasol®
ii) Ionic surfactants (rarely used due to irritation) Eg, Sodium dodecyl sulfate (SDS)
5.3 Co-surfactants
These help further reduce interfacial tension and increase the flexibility of the interfacial film.
Role: Improve micro-emulsification efficiency, Increase drug loading, Aid solubilization of surfactant and oil mixture
Common Co-surfactants / Co-solvents:
5.4 Drug:
Usually poorly soluble BCS Class II or IV compounds. Eg. Nifedipine, Griseofulvin, Ibuprofen etc.
Examples: Fenofibrate, Cyclosporine, Ritonavir, Curcumin[26,27,28,29,30]
6. Marketed Formulation [31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41]
|
Product Name |
API |
Company |
Type |
Indication |
|
Neoral® |
Cyclosporine A |
Novartis |
SMEDDS |
Immunosuppressant |
|
Sandimmune Neoral® |
Cyclosporine A |
Novartis |
SMEDDS |
Immunosuppressant |
|
Norvir® |
Ritonavir |
AbbVie |
SNEDDS |
HIV |
|
Fortovase® |
Saquinavir |
Roche |
SEDDS |
HIV |
|
Kaletra®/Aluvia® |
Lopinavir + Ritonavir |
AbbVie |
SEDDS/ SNEDDS |
HIV |
|
Lipirex® |
Fenofibrate |
— |
SMEDDS |
Hyperlipidaemia |
|
Targretin® |
Bexarotene |
Eisai Pharma |
SEDDS |
CTCL |
|
Agenerase® |
Amprenavir |
GSK |
SEDDS |
HIV |
7. APPLICATIONS OF S-SMEDDS
8. CONCLUSION
Self-Microemulsifying Drug Delivery Systems is one of the most potential and auspicious solution for augmenting oral delivery of poorly water-soluble drugs. Its ability to form nano-sized microemulsion, enhancing drug solubilization capacity, reducing absorption variability and promoting lymphatic transport has added advantage in modern product development. The key factor that plays a major role in successful self-emulsification and stability is the selection of oil(s), surfactant(s) and co-surfactant(s). Despite several issues like high surfactant contents, formulation constraints, drug precipitation problems during dilution and regulatory aspects exist in exploiting full benefits of SMEDDS technology; it is still growing fast with other options like solid-SMEDDSs, supersaturable systems for bringing out immediate release profile, mucoadhesive forms for site specific therapy; hybrid polymer–lipid based forms etc. Introduction of novel technologies/characterization techniques will support researchers further to probe into complete insights of utilized as well as unutilized latent capability toward refining/improvising patient tolerant easy fabrication oral dosage forms.
REFERENCES

Mihir Rathod, Bhoomika Malete, Priyanka Patil, Self-Micro Emulsifying Drug Delivery Systems (SMEDDS): A Comprehensive Review of Formulation, Mechanisms, and Applications, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3187-3197. https://doi.org/10.5281/zenodo.18709680
 10.5281/zenodo.18709680
10.5281/zenodo.18709680
