
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dr. K.V. Subba Reddy Institute of Pharmacy, Dupadu, Kurnool-518218, Andhra Pradesh, India.
Tegoprazan is a novel, potent, and highly selective potassium-competitive acid blocker that inhibits gastric and secretion with rapid onset of action and prolonged control of gastric acidity. In patients with gastroesophageal reflux disease (GERD)whose symptoms improve with acid-suppression therapy, on-demand treatment could constitute maintenance therapy. Potassium-competitive acid blockers and proton pump inhibitors/sodium bicarbonate can rapidly increase intragastric pH. A novel and varied class of medications known as potassium-competitive acid blockers (P-CABs), like tegoprazan, can totally block the potassium-binding site of gastric H+/K+ ATPase, potentially getting around the restrictions of proton-pump inhibitors (PPIs). This mechanism allows for consistent acid suppression across a wide pH range and minimizes variability due to CYP2C19 polymorphisms or food intake. Clinical trials have demonstrated tegoprazan’s efficacy in managing gastroesophageal reflux disease (GERD), peptic ulcers, and Helicobacter pylori infection. It achieves rapid symptoms relief and high healing rates, with a favorable safety profile and minimal adverse effects. Pharmacokinetic reveal a peak plasma concentration within 1-2hours and a half-life of approximately 7-10hours, supporting once-daily dosing. Pharmacodynamic data confirm sustained intragastric pH elevation, even during night time periods. This review consolidates current evidence on tegoprazan’s pharmacology, clinical applications, safety, and formulation characteristics, highlighting its potential as a next-generation acid suppressant for diverse patient populations. Recent phase 3 clinical trials, including the TRIUMPH program, have demonstrated that tegoprazan provides statistically superior oesophageal healing compared achieving higher complete healing rates at both four and eight weeks across all grades of erosive esophagitis, including severe forms.
Laryngopharyngeal reflux disease (LPRD)is defined as several symptoms and signs caused by the retrograde flow of gastroduodenal contents into the laryngopharynx, oropharynx, and nasopharynx.[1]LPRD symptoms include hoarseness, throat clearing, sore throat, a globus sensation, chronic cough, dysphagia, and postnasal drip, and the endo laryngeal signs of LPRD include erythema, oedema, and inter arytenoid hypertrophy.[2] Gastro-oesophageal reflux disease (GERD)is a common gastrointestinal disorder resulting from reflux of gastric acid into the oesophagus. The objectives of GERD treatment are symptom relief, EE repair, and avoiding complications and recurrences that have a direct impact on patients quality of life. Proton pump inhibitors (PPI)have been the first line treatment for GERD. They are indicated for initial treatment and relapse.[3] First, they have a slow onset of action without completely suppressing acid production, leading to night time acid breakthrough. Second, cytochrome P450 CYP2C19 genetic polymorphism affects PPI effectiveness. Third, they are unstable in acidic conditions. However, the majority of these studies were retrospective.[4],[5] Tegoprazan, a potent and highly selective P-CAB, exhibits a rapid onset of action within 1h and a sustained holding of intragastric pH above 4 after single or multiple administration.[6],[7] Tegoprazan 50mg or 100mg shows non-inferior efficacy to esomeprazole 40mg in EE patients after 8 weeks of treatment.[8] Furthermore, tegoprazan 50mg and 100mg are non-inferior to lansoprazole 30mg for the treatment of patients with gastric ulcer and superior to placebo for the treatment of non-erosive reflux disease.[9], [10] PPIs have been an essential component of H. pylori eradication regimens.[11]
Gastric acid inhibition is crucial for increasing the H. pylori eradication rate by stabilising acid-labile antibiotics in the stomach and increasing the sensitivity of H. pylori to antibiotics.[12] Currently, PPIs-based triple therapy, which consists of a PPI, Amoxicillin, and clarithromycin, is the most popular. Eradication regimen worldwide.[11], [13] Accordingly, PPIs are limited because the absorption and onset of their antisecretory effects may be delayed. To overcome these limitations, an immediate-release formulation without an enteric coating containing PPI and sodium bicarbonate was developed. Sodium bicarbonate protects uncoated PPIs from degradation by gastric acid, enabling its rapid release and absorption and improving Its onset of action.[14], [15]
Molecular Formula:C20H19F2N3O3(fig 1)
Molecular Weight:387.4g/mol
IUPAC Name:7-[[(4S)-5,7-difluoro-3,4-dihydro-2H-chromen-4-yl] oxy]-N, N,2-trimethyl-3-H-benzimidazole-5-carboxamide
SMILES:CC1=NC2=C(N1) C=C(C=C20[C@H]3CCOC4=C3C(=CC(=C4C) F) F) C(=O) N(C)C
InChl Key: CLIQCDHNPDMGSL-HNNXBMFYSA-N
CAS Number:942195-55-3
Drug Bank ID:DB16690
CHEMBL ID: CHEMBL4297583
Brand Image: K-CAB® s(Tegoprazan)
Formulation:50mg tablets
Appearance: Oval, film-coated tablet with embossed markings
Indication: GERD, peptic ulcers, H. pylori eradication
Core Features:
*Benzimidazole ring
*Difluoro chroman moiety
*Formamide side chain [16]
MECHANISM OF ACTION:
Compared to conventional proton pump inhibitors (PPIs), tegoprazan, a new drug used to treat gastrointestinal diseases caused by acid reflux, has drawn attention due to its unique mode of action. Tegoprazan belongs to the class of drugs known as P-CABS. P-CABs like tegoprazan function differently from PPIs which permanently block the stomach lining’s hydrogen-potassium ATPase enzyme. Through a reversible process.
The main way that tegoprazan works is by competitively blocking the potassium-binding site of the gastric proton pump, sometimes referred to as the H+/K+ ATPase.By blocking this site on the proton pump, preventing the ion exchange necessary for acid secretion.[18]
This competitive inhibition occurs rapidly, giving it a faster onset of action than PPIs, which require multiple doses to reach peak effectiveness. Its reversible binding allows normal acid secretion to resume once the drug is cleared, reducing the risk of rebound hyperacidity seen with PPIs. Clinical trials indicate that a single daily dose effectively controls acid for 24hours, making it a convenient option for long-term management of acid-related disorders. The drug effectively. Inhibits both meal-stimulated and nocturnal acid production, Providing quick relief from symptoms.(fig 2)
Gastric Acid Secretion Pathways:
Gastric acid secretion is regulated by neural, hormonal, and paracrine pathways that activate the gastric H+/K+ ATPase enzyme in parietal cells. The process begins when food-related stimuli trigger the vagus nerve, causing acetylcholine to be released.[19].This attaches to parietal cells, muscarinic M3 receptors, raising intracellular calcium and triggering the proton pump. Additionally, histamine binds to parietal cells,H2 receptors, activating adenylated cyclase and raising cyclic AMP levels, which enhances proton pump activity and increases acid secretion. By engaging with cholecystokinin B (CCK-B) receptors on parietal and ECL cells, the hormone gastrin, which is generated by G cells in response to protein digestion and gastric distension, further increases the generation of acid. Strong acid production for digestion is ensured by the combined actions of histamine, acetylcholine, and gastrin.
To preserve mucosal integrity, inhibitory systems balance acid secretion. By preventing the release of histamine and gastrin, somatostatin, which is secreted by D cells in reaction to increased acidity, reduces the formation of acid. By lowering cyclic AMP levels in parietal cells and encouraging the release of mucus and bicarbonate, prostaglandins like PGE2 also control acid secretion and shield the stomach lining from too much acidity.
THERAPEUC USES OF TEGOPRAZAN:
Tegoprazan is highly effective in treating GERD, including both non-erosive and erosive forms. It providing fast symptom relief and promotes mucosal healing.[17]
Used to treat gastric and duodenal ulcers by reducing acid secretion and allowing ulcerated tissue to heal.
Tegoprazan is being studied as part of combination regimens for H. pylori eradication,often alongside antibiotics. Its acid suppression enhances antibiotic efficacy.[8],[16]
Approved in South Korea for treating erosive esophagitis, with clinical trials showing strong healing rates and symptoms control.[20]
Though still under investigation, tegoprazan shows promise in managing dyspeptic symptoms linked to acid imbalance.
Its ability to suppress nocturnal acid secretion makes it useful for patients with night time GERD symptoms.[18]
5.SIDE EFFECTS:
Nausea, diarrhoea, dyspepsia, abdominal pain. Nasopharyngitis, upper respiratory tract infection, chest discomfort, indigestion, altered taste sensation [18]
Constipation, abdominal distension, vomiting, headache, dizziness, hepatic enzyme elevations, flatulence, chest discomfort, fatigue, myalgia, tendonitis, insomnia, ear pain [18],[21]
Hepatotoxicity (much lower risk vs PPIs, based on real-world post -market data),
cyanocobalamin (Vitamin B12) deficiency on long-term use, allergic reaction: rash, itching, swelling, severe dizziness, difficulty breathing, anal incontinence, toxic skin
CONTRAINDICATIONS:
Patients with known allergy to tegoprazan or any of its excipients should not take the drug
Though tegoprazan is not a PPI, caution is advised in patients allergic to substituted benzimidazoles, due to structural similarities.
Tegoprazan should not be used with Atazanavir, Nelfinavir, or Rilpivirine, as it can significantly reduce their absorption and efficacy due to pH-dependent solubility.
While data is limited, caution or avoidance is recommended in patients with a significant liver or kidney dysfunction, especially in the absence of safety data.
Safety and efficacy have not been established in children and adolescents, so use is contraindicated in these groups.[22]
NURSING CONSIDERATIONS FOR TEGOPRAZAN:
Assessment:
Administration:
Monitoring:
Patient Education:
Safety Precautions:
PATIENT EDUCATION:
Understanding the Medication:
How to Take it:
What to watch for:
Lifestyle Tips:
Special Populations:
Medication Safety:
PHARMACOKINETICS
Absorption
Rapidly absorbed (Tmax: 0.5–1.5 h)[23] with dose-proportional plasma levels.Food and CYP2C19 genotype do not significantly affect absorption.Acid-stable and lipophilic, allowing high membrane permeability.Formulations: IR for rapid onset; DR or IR+DR for prolonged pH control.May alter absorption of pH-dependent drugs (e.g., dabigatran, iron salts, atazanavir).
Distribution
Moderate tissue distribution; preferential accumulation in gastric parietal cells.[24]
Physicochemical properties: MW ~ 387 g/mol, log P ~ 2.3, pKa ~ 6.8, BCS Class II.Likely moderate plasma protein binding.
Metabolism
Primarily metabolized by CYP3A4; minor role for CYP2C19.Major metabolite (M1) inactive; undergoes hydroxylation and glucuronidation.
Half-life: ~7–10 h; clearance mainly hepatic (75%).CYP3A4 inhibitors ↑ exposure (up to 3×)[25]; inducers ↓ exposure (~30%).
Elimination
Excreted mainly via feces (50–60%) and urine (~30%) as metabolites.
Negligible unchanged drug excreted.Terminal half-life: 7–10 h, supporting once-daily dosing.[26]
PHARMACODYNAMICS
Mechanism: Reversible potassium-competitive inhibition of gastric H?/K?-ATPase.
Onset: Within 1 hour; Duration: up to 24 hours.[23]
Selectivity: Highly specific to gastric proton pumps; minimal off-target effects.
pH Stability: Acid-stable; no need for enteric coating.
Clinical effects: Rapid, sustained acid suppression; effective for GERD, erosive esophagitis, and H. pylori eradication.
Reversibility & Tolerance: Reversible binding with minimal tolerance during long-term use.
DRUG-DISEASE INTERACTIONS:
Liver Impairment:
Renal Impairment:
Infections (e.g., Clostridium difficile):
Osteoporosis:
Vitamin B12 Deficiency:
PHARMACEUTICAL INTERACTIONS:
Clarithromycin:
Amoxicillin:
CYP3A4 Modulators:
STRUCTURAL INTERACTIONS WITH PROTON PUMPS:
Tegoprazan’s effectiveness is due to its structural interactions with the H?/K?-ATPase enzyme. Unlike PPIs, which require activation in an acidic environment and irreversibly modify cysteine residues on the proton pump, tegoprazan binds directly and reversibly to the enzyme’s potassium-binding site. This non-covalent interaction prevents the conformational changes necessary for ion exchange, halting acid secretion.
Its pyrimidine-based core enhances high-affinity binding, allowing consistent inhibition under varying gastric pH conditions. This eliminates the delays associated with PPI activation, making tegoprazan a more reliable choice for rapid acid suppression. Its reversible nature allows for flexible dosing and reduces concerns about long-term desensitization of the proton pump.
Crystallographic studies show tegoprazan’s binding mode differs from PPIs, as it does not require active transport into acidic canaliculi. This avoids protonation-dependent activation, which can lead to variability in PPI efficacy. Its structural stability ensures prolonged acid suppression, even after plasma concentrations decline, benefiting patients needing continuous acid control, such as those with GERD or Zollinger-Ellison syndrome.[19]
METHODOLOGY:
Study Population:
Study Design:
This was a multi?centre, randomised, double?blind, actively controlled, phase 3 study designed to assess the non?inferiority of tegoprazan 25 mg to lansoprazole 15 mg as maintenance therapy in Korean patients with healed EE[31]. The study protocol was reviewed and approved by the Institutional Review Boards of 33 institutes. This study was performed in accordance with the Declaration of Helsinki and the International Congress on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use for Good Clinical Practice guidelines. Written informed consent was obtained from all subjects prior to any study?related procedure. This study was registered at ClinicalTrials.gov (identifier number: NCT04022096; healed erosive oesophagitis).(fig 3)
Study protocol:
Randomisation, treatment and follow?up:
During the screening period, endoscopy was performed to evaluate the presence and severity of EE based on the Los Angeles Classification System. Following 4 or 8 weeks of treatment with either PPIs (esomeprazole, lansoprazole, dexlansoprazole, pantoprazole or rabeprazole) or tegoprazan, endoscopy confirmed that EE was healed. Patients with endoscopically confirmed healed EE were randomised to receive tegoprazan 25 mg or lansoprazole 15 mg at a 1:1 ratio using an interactive web response system of the central registration system. Patients received tegoprazan 25 mg or lansoprazole 15 mg once daily 30 minutes before breakfast.[32] The treatment was completed after 24 weeks
Participant Flow:
Patients 18–75 (up to 85 in some studies) years old, with EE confirmed by endoscopy; H. pylori-positive, IBS, or IBD patients generally excluded.
Calculated for >90% power to test non-inferiority with pre-specified healing rates and margins; ~100–130 subjects per treatment arm, accounting for dropouts.[8]
Excluded for protocol violations, withdrawal of consent, use of contraindicated drugs, loss to follow-up, or adverse events.
Outcome parameters used to assess efficacy
The primary efficacy endpoint was the endoscopic remission rate following 24 weeks of maintenance therapy. The secondary efficacy endpoint was endoscopic remission rate following 12 weeks of maintenance therapy. Additional efficacy endpoints included evaluation of the proportion of patients without symptomatic heartburn and acid reflux, days without symptoms at 4, 12 and 24 weeks, and baseline?adjusted gastro?oesophageal reflux disease health?related quality of life (GERD?HRQL) scores at 4, 12 and 24 weeks. The GERD?HRQL scale has 11 items focusing on heartburn symptoms, dysphagia, effects of medications and health condition of patients. Each item was scored from 0 to 5, with a higher score indicating a poorer quality of life[31].
Adverse Events and Safety:
Gastrointestinal: diarrhea, nausea, abdominal pain, distention, dry mouth, eructation;Nervous system: headache
Discontinuation due to AE, serious TEAEs <1% for both tegoprazan and comparators.[32]
Statistical analysis:
Hypothesis testing was based on the primary efficacy endpoint—the endoscopic remission rate at week 24. The sample size (318 subjects; 159 per group) was calculated assuming remission rates of 88.4% for tegoprazan and 83.2% for lansoprazole, with a non-inferiority margin of −10%, 90% power, and a 0.025 significance level, accounting for a 30% dropout rate.
Efficacy was analyzed using the Per-Protocol Set (PPS) as primary and the Full Analysis Set (FAS) as secondary; safety was assessed using the Safety Analysis Set (SAS).
Non-inferiority of tegoprazan was established if the lower bound of the 95% CI for the treatment difference exceeded −10%. Statistical analyses were conducted using SAS® version 9.4, with continuous data summarized by mean, SD, median, min, and max, and categorical data by frequency and percentage. All tests used a two-sided 5% significance level, unless otherwise stated.[31]
Data Collection Tools
Standardized endoscopic assessment (LA grading for EE, ulcer healing for GU).
Used to record daily symptoms, rescue medication, and adverse events.
Central review committees validated endoscopic findings; study monitors ensured protocol compliance.
Baseline Clinical Characteristics:
No significantly changes in vital signs or ECG findings during treatment
REFERENCES
Tables:
Table 1: Types Of Side Effects
|
Category |
Description |
Examples |
|
Common |
Occur in >10% of patients |
Nausea, headache, fatigue |
|
Less Common |
Occur in 1-10% |
Rash, dizziness, dry mouth |
|
Rare |
Occur in <1% |
Anaphylaxis, liver toxicity |
|
Serious |
Life threatening or requiring intervention |
Pulmonary embolism, renal failure |
Table 2:
Table 3:
Figures:
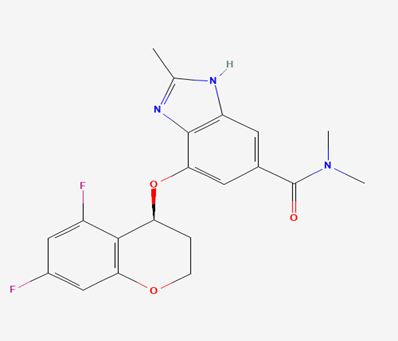
Figure 1: Chemical structure of tegoprazan
Figure 2: Mechanism of action
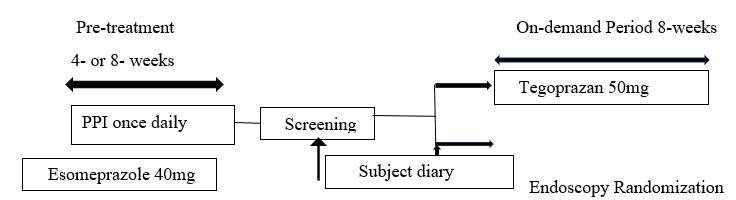
Figure 3: Study design. Patients with GERD who experienced symptom improvement after completing at least 4 or 8- week PPI therapy
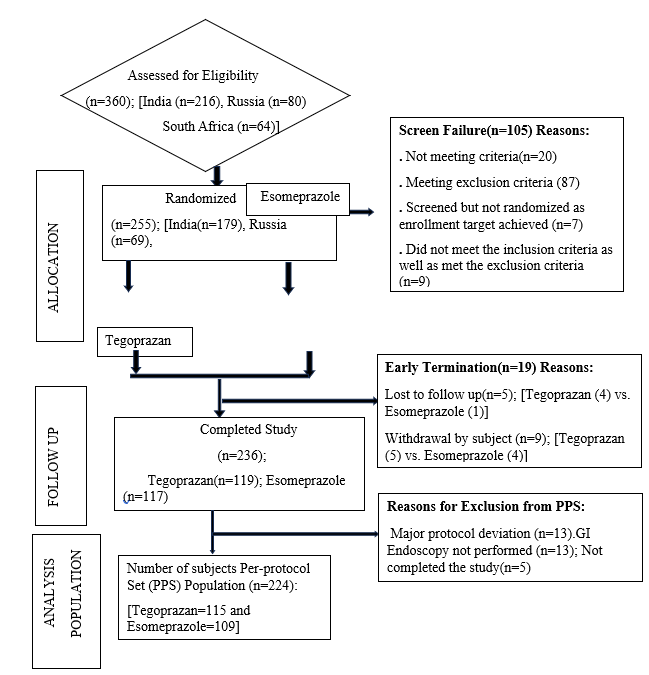
Figure 4: Consort diagram displaying the flow of participants through the study

Dr. R. Jona Methusala, Thouday Keerthi*, Tegoprazan: A Next-Generation P-CAB Redefining Acid Suppression, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 4709-4723 https://doi.org/10.5281/zenodo.17757232
 10.5281/zenodo.17757232
10.5281/zenodo.17757232