Rabies virus infection often begins with flu-like symptoms and nonspecific neurological signs. Once clinical symptoms develop, the disease is almost always fatal, with treatment limited to palliative care focused on easing the patient’s suffering. In regions with poor healthcare access, many patients die at home. Healthcare providers must understand the correct postexposure prophylaxis (PEP) schedule and vaccine administration methods relevant to their area, as well as general global rabies prevention strategies. Rabies and related Lyssaviruses are found worldwide and can infect dogs, cats, livestock, and wild animals. Transmission typically occurs through bites or contact of infected saliva with broken skin or mucous membranes. However, human rabies is preventable through proper pre- and post-exposure care. PEP involves immediate and thorough wound cleansing and administration of rabies vaccines. If the individual was not previously vaccinated, human rabies immune globulin (HRIG) is also applied to the wound. Early and appropriate intervention is highly effective in preventing disease progression. The most cost-effective strategy to prevent rabies in humans is the One Health approach, which promotes coordination between environmental, veterinary, and human health sectors. Mass vaccination of dogs—the main source of transmission—remains the most critical intervention in eliminating dog-mediated human rabies.
Keywords
Rabies, lyssaviruses, postexposure prophylaxis, dog vaccine, prophylaxis
Introduction
×
Rabies is a highly fatal zoonotic disease that causes acute inflammation of the central nervous system in warm-blooded animals, including humans. It is caused by the rabies virus (RABV), a neurotropic virus belonging to the genus Lyssavirus, family Rhabdoviridae [1]. The disease is primarily transmitted to humans through the bite or scratch of an infected animal, most commonly domestic dogs.
Despite being preventable through vaccination, rabies continues to be a major public health concern, particularly in Asia and Africa, where over 95% of human deaths occur due to limited access to timely medical care and post-exposure prophylaxis (PEP) [2]. According to the World Health Organization (WHO), rabies causes an estimated 59,000 human deaths annually, with India alone contributing to nearly 20,000 of these deaths, often due to stray dog bites [3].
The clinical presentation of rabies includes fever, hydrophobia, confusion, paralysis, and coma, progressing rapidly to death once neurological symptoms appear. At this stage, no effective treatment is available, and the disease is almost invariably fatal [4].
Historically, rabies has been recognized for millennia, with references dating backto ancient Mesopotamian texts and Greek literature. The first scientific breakthrough came in the 19th century when Louis Pasteur developed the first rabies vaccine, a milestone in virology and immunization [5].
The global strategy to eliminate human deaths from dog-mediated rabies by 2030, known as “Zero by 30”, is spearheaded by WHO, OIE, FAO, and GARC. This initiative focuses on dog vaccination, human awareness, and improved access to PEP [6].
OBJECTIVES OF RABIES
1. Prevent Human Rabies Deaths:
Provide universal access to life-saving post-exposure prophylaxis (PEP).
Ensure availability of safe and effective vaccines and rabies immunoglobulin.
Reduce the time between exposure and treatment, especially in rural areas [7].
2. Eliminate Canine Rabies as a Public Health Threat:
Conduct mass dog vaccination campaigns, aiming for 70% coverage.
Control the stray dog population through humane means.
Break the transmission cycle between dogs and humans [8].
3. Increase Public Awareness and Education:
The dangers of rabies- Animal bite prevention
The importance of timely PEP
Target high-risk groups such as children and rural communities [9].
4. Strengthen Surveillance and Diagnostic Capacity:
Improve early detection and laboratory diagnosis of suspected rabies cases.
Establish reliable reporting and data-sharing systems.
Monitor the effectiveness of control strategies and adapt as needed [10].
5. Promote One Health Collaboration:
Encourage collaboration between human health, veterinary, and wildlife sectors.
Integrate rabies control with other zoonotic disease programs.
Foster international and regional cooperation [11].
ETIOLOGY OF RABIES
Rabies is caused by the rabies virus (RABV), a member of the Lyssavirus genus within the family Rhabdoviridae [12]. The virus is enveloped, bullet-shaped, and contains a non-segmented, single-stranded, negative-sense RNA genome. It is one of the oldest known zoonotic viruses, capable of infecting all warm-blooded mammals, including humans.
The primary reservoir for the rabies virus differs across geographical regions. In Asia and Africa, domestic dogs are the main source of human rabies infections [13]. In the Americas, wildlife species such as bats, raccoons, skunks, and foxes are important reservoirs [14]. The virus is transmitted mainly through saliva, introduced via the bite or scratch of an infected animal.
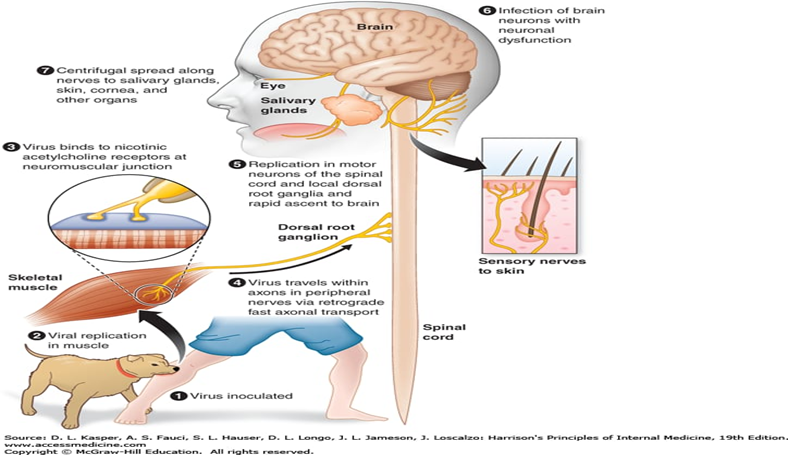
Once introduced into the host, the virus initially replicates in striated muscle tissue at the site of entry. It then enters the peripheral nervous system by binding to nicotinic acetylcholine receptors at the neuromuscular junction and travels retrogradely along motor neurons to reach the central nervous system [15].
There are at least 16 recognized species in the Lyssavirus genus. While Rabies lyssavirus (classic rabies virus) is the most common and well-known, other lyssaviruses such as Duvenhage virus, European bat lyssavirus types 1 and 2, and Australian bat lyssavirus have also been isolated from animals and have caused rare human infections [16].
The virus is neurotropic, and its ability to evade the immune response until it reaches the central nervous system is a key factor in its pathogenesis. Understanding the etiological agent, including its molecular biology and evolution, is essential for improving diagnosis, treatment, and vaccine development strategies.
CLINICAL FEATURES OF RABIES
Rabies has a well-defined but variable clinical course. The disease is almost universally fatal once symptoms appear, with neurological signs being the hallmark of infection. The incubation period typically ranges from 1 to 3 months, but it can be as short as a few days or as long as several years, depending on factors like the site of the bite, viral load, and host immunity [17].
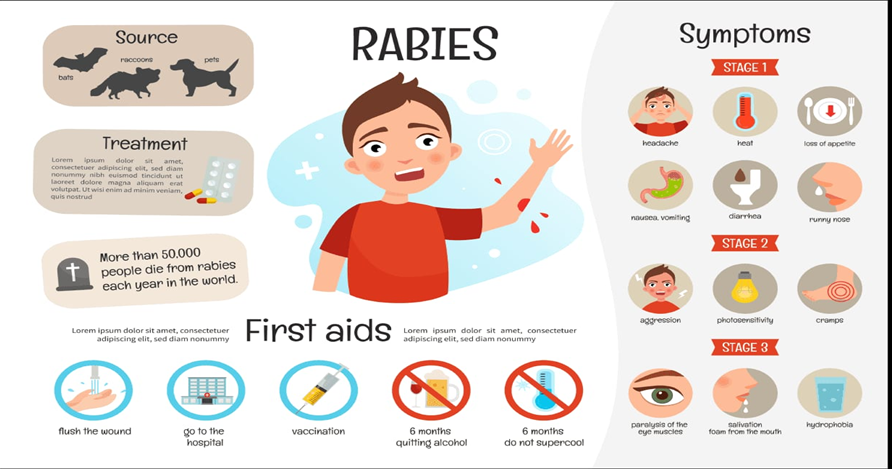
1. Prodromal Phase: This phase lasts 2–10 days and is often nonspecific. Patients may experience:
Fever
Malaise
Headache
Fatigue
Pain, tingling, or itching at the bite site (a key diagnostic clue) [18]
2. Acute Neurologic Phase: Rabies presents in two main clinical forms:
a) Furious Rabies (80% of human cases)
Anxiety and agitation
Hallucinations and hyperactivity
Hydrophobia (fear and painful spasms when attempting to drink water)
Paralytic rabies is harder to diagnose and often misdiagnosed, leading to delays in appropriate care [20].
3. Coma and Death: Following neurological decline, patients typically enter a coma and die within 7–10 days, usually due to cardiorespiratory failure [21]. Supportive care may prolong survival slightly, but once symptoms appear, there is no effective treatment.
The clinical manifestations reflect the neurotropic nature of the virus, which targets and disrupts various regions of the central nervous system, especially the brainstem and limbic system [22].
DIAGNOSIS OF RABIES
Diagnosing rabies is challenging, especially in the early stages, due to nonspecific symptoms and the rapid progression of the disease. Once clinical symptoms appear, rabies is almost always fatal. Thus, early and accurate diagnosis is critical for both epidemiological surveillance and public health interventions.
1. Clinical Diagnosis- Rabies should be suspected in any patient presenting with:
Acute encephalitis or myelitis
History of an animal bite or unexplained neurologic symptoms
Classic signs such as hydrophobia, aerophobia, and altered behavior [ 23]
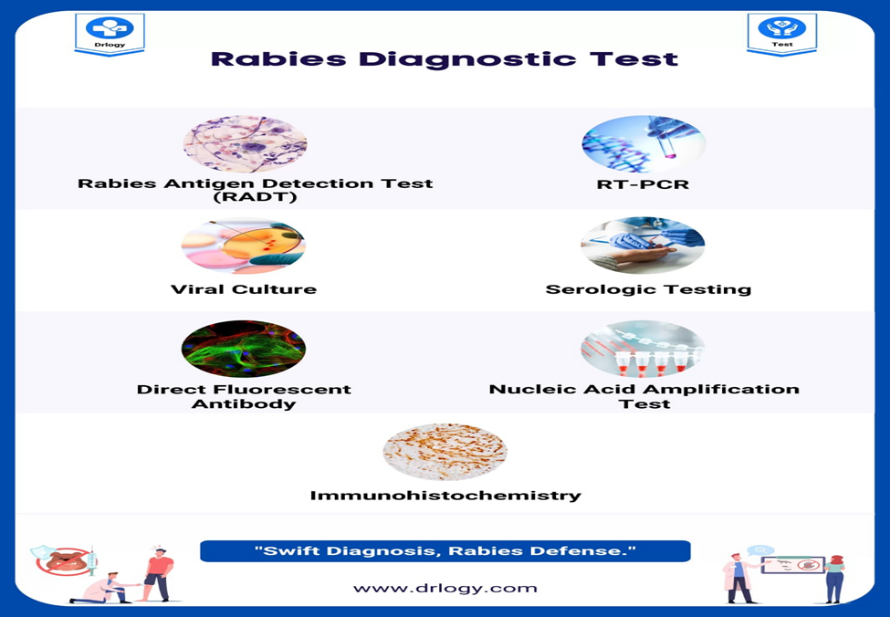
2. Antemortem Diagnosis- Several laboratory techniques are used, usually in combination, to confirm rabies in live patients:
a) Saliva:
Detection of rabies virus RNA by RT-PCR.
Non-invasive and commonly used, but requires strict handling [24].
b) Skin Biopsy (Nuchal Region):
Detection of viral antigen in hair follicles using Direct Fluorescent Antibody (DFA) test or immunohistochemistry.
Considered reliable and widely used [25].
c) Cerebrospinal Fluid (CSF):
May show mild pleocytosis or elevated protein.
RT-PCR or antibody detection can support diagnosis [26].
d) Serum and CSF:
Detection of rabies virus-neutralizing antibodies (RVNA) via Rapid Fluorescent Focus Inhibition Test (RFFIT) or ELISA [27].
3. Postmortem Diagnosis: After death, brain tissue is the preferred specimen:
DFA test on brain impression smears (gold standard).
Virus isolation in cell culture or laboratory animals (less commonly used due to ethical issues) [28].
4. Emerging Techniques: Newer molecular and point-of-care diagnostics are being developed:
Real-time RT-PCR and loop-mediated isothermal amplification (LAMP)
Lateral flow rapid diagnostic kits (in evaluation phase)
While these have high sensitivity and specificity, their availability is limited in endemic regions due to cost and infrastructure constraints [29].
TREATMENT OF RABIES
1. Overview : Rabies is almost invariably fatal once clinical symptoms appear. Therefore, early intervention before symptom onset is the only effective way to prevent death. Once a patient becomes symptomatic, supportive care is the only available option, and recovery is exceedingly rare.
The cornerstone of rabies treatment is post-exposure prophylaxis (PEP), which is nearly 100% effective if administered promptly and properly.
2. Post-Exposure Prophylaxis (PEP): PEP involves three key components:
a) Wound Washing:
Immediate and thorough cleaning of the wound with soap and water for at least 15 minutes is crucial.
This step significantly reduces viral load at the site of entry [30].
b) Rabies Vaccine:
Given on days 0, 3, 7, and 14 (Essen regimen).
Intramuscular or intradermal administration depending on national guidelines [31].
c) Rabies Immunoglobulin (RIG):
Human RIG (HRIG) or Equine RIG (ERIG) is infiltrated around the wound for Category III exposures.
It provides passive immunity during the window before active antibodies develop [32].
PEP is effective even days after exposure, but delays reduce efficacy.
3. Pre-Exposure Prophylaxis (PrEP): Recommended for high-risk groups such as veterinarians, laboratory workers, and travelers to endemic areas. Involves two or three doses of rabies vaccine administered before exposure [33].
4. Treatment After Symptom Onset: Once clinical rabies symptoms appear, there is no established curative treatment. The following have been attempted with limited success:
Milwaukee Protocol: First reported survival in 2004 using a combination of induced coma and antiviral drugs [34]. However, subsequent attempts have largely failed, and this protocol remains experimental and controversial [35].
Supportive Care: Includes mechanical ventilation, sedation, hydration, and seizure control.Aimed at keeping the patient comfortable and prolonging survival
5. Novel and Experimental Approaches: Use of monoclonal antibodies (e.g., rabies-neutralizing monoclonal antibodies) is under clinical evaluation. RNA-based vaccines and vector-based delivery are being developed but are not yet widely available [36].
PREVENTION OF RABIES
Rabies is 100% preventable, yet it continues to cause tens of thousands of deaths annually. Effective prevention relies on a One Health approach, integrating animal control, public education, and access to vaccines and immunoglobulins. The World Health Organization (WHO), in collaboration with international agencies, promotes the “Zero by 30” initiative to eliminate dog-mediated human rabies deaths by 2030.
1. Prevention in Humans
a) Post-Exposure Prophylaxis (PEP): PEP is the most effective life-saving intervention and consists of:
Wound cleansing: Immediate washing of bite wounds with soap and water for at least 15 minutes reduces viral load [37].
Rabies vaccination: Given intramuscularly or intradermally on days 0, 3, 7, and 14 (Essen regimen).
Rabies immunoglobulin (RIG): For Category III exposures, HRIG or ERIG is infiltrated around the wound to provide passive immunity [38].
PEP is nearly 100% effective if given promptly and correctly.
b) Pre-Exposure Prophylaxis (PrEP): Recommended for:
Laboratory workers
Veterinarians
Travelers to high-risk regions
Children in rabies-endemic areas
Regimens include two or three doses of the rabies vaccine before exposure. It reduces the number of PEP doses required and eliminates the need for RIG [39].
2. Animal Rabies Control
a) Mass Dog Vaccination:
Dogs are the main source of human rabies (up to 99% of cases).
Vaccinating at least 70% of the dog population is essential to interrupt transmission [40].
b) Dog Population Management: Sterilization, registration, and humane culling (where necessary) reduce the stray dog population and improve vaccination coverage [41].
3. Public Awareness and Education- Community-based education programs help:
Improve reporting and treatment-seeking behavior
Promote safe interaction with animals
Dispel myths and fears around rabies and vaccination
4. International Collaboration: Zero by 30: The global strategic plan launched by WHO, FAO, OIE, and GARC includes three core objectives:
Effective use of vaccines and biologics
Education and awareness
Strong surveillance and inter-sectoral collaboration [42]
5. Wildlife Rabies Control: Oral rabies vaccines (ORV) for foxes, raccoons, and other wildlife have helped eliminate rabies in parts of Europe and North America. Bait vaccines are distributed in wildlife habitats [43].
RECENT OUTCOMES
Zero to 30: Eradicating Dog-Transmitted Human Rabies
Delivering proper healthcare to people exposed to rabies is challenged by obstacles at the patient, provider, and system levels. To protect communities vulnerable to rabies, multiple strategies must be adopted. The United Against Rabies coalition proposed several such strategies in 2017 under the WHO framework, aiming to eliminate dog-mediated human rabies by the year 2030.
A comprehensive strategy for eradicating human rabies requires collaboration from governments, increased awareness among healthcare workers and the public, availability of both pre- and post-exposure prophylaxis, and a unified One Health approach. This includes coordination between environmental, medical, and veterinary sectors, especially focusing on widespread vaccination of dogs and other rabies-transmitting animals, to meet the WHO target of zero human deaths from dog-transmitted rabies by 2030.
Strategic actions include:
Effective use of tools and technology: This involves expanding knowledge about PEP, promoting mass dog vaccinations, and ensuring timely and efficient use of PEP.
Innovation and impact monitoring: This includes forming and implementing policies and guidelines to prevent rabies-related deaths, maintaining access to relevant technologies and data, and continuously evaluating progress toward elimination goals.
Sustained support and funding: Efficient use of financial and other resources is essential, along with routine monitoring and transparent reporting to stakeholders on the outcomes of global anti-rabies initiatives.
A 2021 study by Changalucha et al highlighted persistent challenges in rabies-endemic countries but also emphasized promising developments in technical capabilities, institutional support, and financial investments. The success of rabies control efforts in regions like North America, Europe, Japan, and parts of the Americas proves that elimination is achievable.[44]
REFERENCES
Rupprecht CE, Hanlon CA, Hemachudha T. Rabies re-examined. Lancet Infect Dis. 2002;2(6):327–43.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9(4):e0003709.
World Health Organization. Rabies [Internet]. Geneva: World Health Organization; 2023 Jun
Warrell MJ, Warrell DA. Rabies and other lyssavirus diseases. Lancet. 2004 Mar 20;363(9413):959-69. doi:10.1016/S0140-6736(04)15792-9. Erratum in: Lancet. 2004 Dec 11;364(9451):2096. PMID:15043965.
Pasteur L. Method for preventing rabies by attenuated virus inoculations. Ann Inst Pasteur. 1885.
World Health Organization, Food and Agriculture Organization of the United Nations, World Organisation for Animal Health, Global Alliance for Rabies Control. Zero by 30: global strategic plan to end human deaths from dog-mediated rabies by 2030. Geneva: World Health Organization; 2018.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015 Apr;9(4):e0003709. doi:10.1371/journal.pntd.0003709.
Cleaveland S, Kaare M, Tiringa P, Mlengeya T, Barrat J. A dog rabies vaccination campaign in rural Africa: impact on the incidence of dog rabies and human dog-bite injuries. Vaccine. 2003 May 16;21(17-18):1965-73. doi:10.1016/S0264-410X(02)00778-8.
Dzikwi AA, Ibrahim AS, Umoh JU. Knowledge, attitude and practice about rabies among children receiving formal and informal education in Samaru, Zaria, Nigeria. Glob J Health Sci. 2012 Jul;4(5):132-9. doi:10.5539/gjhs.v4n5p132.
Fooks AR, Banyard AC, Horton DL, Johnson N, McElhinney LM, Jackson AC. Current status of rabies and prospects for elimination. Lancet. 2014 Oct 4;384(9951):1389-99. doi:10.1016/S0140-6736(13)62707-5. PMID:24828901.
Taylor LH, Nel LH. Global epidemiology of canine rabies: past, present, and future prospects. Vet Med (Auckl). 2015;6:361-71. doi:10.2147/VMRR.S51147.
Fooks AR, Banyard AC, Horton DL, Johnson N, McElhinney LM, Jackson AC. Current status of rabies and prospects for elimination. Lancet. 2014;384(9951):1389-99.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al; Global Alliance for Rabies Control Partners for Rabies Prevention. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9(4):e0003709.
Rupprecht CE, Hanlon CA, Hemachudha T. Rabies re-examined. Lancet Infect Dis. 2002;2(6):327-43.
Jackson AC. Rabies: scientific basis of the disease and its management. 3rd ed. London: Academic Press; 2013.
Banyard AC, Evans JS, Luo TR, Fooks AR. Lyssaviruses and bats: emergence and zoonotic threat. Viruses. 2014;6(8):2974-90.
Warrell MJ, Warrell DA. Rabies and other lyssavirus diseases. Lancet. 2004;363(9413):959-69.
Hemachudha T, Laothamatas J, Rupprecht CE. Human rabies: a disease of complex neuropathogenetic mechanisms and diagnostic challenges. Lancet Neurol. 2002;1(2):101-9.
Jackson AC. Rabies: scientific basis of the disease and its management. 3rd ed. London: Academic Press; 2013.
Gadre G, Satishchandra P, Mahadevan A, Suja MS, Madhusudana SN, Sundaram C, Shankar SK. Rabies viral encephalitis: clinical determinants in diagnosis with special reference to paralytic form. J Neurol Neurosurg Psychiatry. 2010;81(7):812-20.
Rupprecht CE, Hanlon CA, Hemachudha T. Rabies re-examined. Lancet Infect Dis. 2002;2(6):327-43
Dacheux L, Reynes JM, Buchy P, Sivuth O, Diop BM, Rousset D, Rathat C, Jolly N, Dufourcq JB, Nareth C, Diop S, Iehlé C, Rajerison R, Sadorge C, Bourhy H. A reliable diagnosis of human rabies based on analysis of skin biopsy specimens. Clin Infect Dis. 2008;47(11):1410-7.
Warrell MJ, Warrell DA. Rabies and other lyssavirus diseases. Lancet. 2004;363(9413):959-69.
Wacharapluesadee S, Hemachudha T. Ante- and post-mortem diagnosis of rabies using nucleic acid-amplification tests. Expert Rev Mol Diagn. 2010;10(2):207-18.
Dacheux L, Reynes JM, Buchy P, Sivuth O, Diop BM, Rousset D, Rathat C, Jolly N, Dufourcq JB, Nareth C, Diop S, Iehlé C, Rajerison R, Sadorge C, Bourhy H. A reliable diagnosis of human rabies based on analysis of skin biopsy specimens. Clin Infect Dis. 2008;47(11):1410-7.
Hemachudha T, Laothamatas J, Rupprecht CE. Human rabies: a disease of complex neuropathogenetic mechanisms and diagnostic challenges. Lancet Neurol. 2002;1(2):101-9.
Smith JS, Yager PA, Baer GM. A rapid fluorescent focus inhibition test (RFFIT) for determining rabies virus-neutralizing antibody. In: Laboratory techniques in rabies. 4th ed. Geneva: World Health Organization; 1996. p. 181-92.
World Health Organization. Laboratory techniques in rabies. 4th ed. Geneva: World Health Organization; 1996.
Nadin-Davis SA, Fehlner-Gardiner C. Diagnostic tools and surveillance systems for the detection of rabies virus. Trop Med Infect Dis. 2017;2(4):53.
World Health Organization. Rabies vaccines: WHO position paper, April 2018 – Recommendations. Vaccine. 2018;36(37):5500-3.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al; Global Alliance for Rabies Control Partners for Rabies Prevention. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9(4):e0003709.
Wilde H, Khawplod P, Khamoltham T, Hemachudha T, Tepsumethanon V, Lumlerdacha B, Mitmoonpitak C, Sitprija V. Rabies control in South and Southeast Asia. Vaccine. 2005;23(17-18):2284-9.
Manning SE, Rupprecht CE, Fishbein D, Hanlon CA, Lumlertdacha B, Guerra M, Meltzer MI, Dhankhar P, Vaidya SA, Jenkins SR, Sun B, Hull HF; Advisory Committee on Immunization Practices, Centers for Disease Control and Prevention (CDC). Human rabies prevention—United States, 2008: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2008;57(RR-3):1-28.
Willoughby RE Jr, Tieves KS, Hoffman GM, Ghanayem NS, Amlie-Lefond CM, Schwabe MJ, Chusid MJ, Rupprecht CE. Survival after treatment of rabies with induction of coma. N Engl J Med. 2005;352(24):2508-14.
Jackson AC. Current and future approaches to the therapy of human rabies. Antiviral Res. 2013;99(1):61-7.
World Health Organization. WHO expert consultation on rabies: third report. WHO Tech Rep Ser. 2018;(1012):1-195.
World Health Organization. WHO expert consultation on rabies: third report. WHO Tech Rep Ser. 2018;(1012):1-195.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al; Global Alliance for Rabies Control Partners for Rabies Prevention. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9(4):e0003709.
Manning SE, Rupprecht CE, Fishbein D, Hanlon CA, Lumlertdacha B, Guerra M, Meltzer MI, Dhankhar P, Vaidya SA, Jenkins SR, Sun B, Hull HF. Human rabies prevention—United States, 2008. MMWR Recomm Rep. 2008;57(RR-3):1-28.
Cleaveland S, Kaare M, Knobel D, Laurenson MK. Canine vaccination—providing broader benefits for disease control. Vet Microbiol. 2006;117(1):43-50.
World Society for the Protection of Animals. Methods for the control of dog populations: a guide for policymakers. London: World Society for the Protection of Animals; 2007.
World Health Organization, Food and Agriculture Organization of the United Nations, World Organisation for Animal Health, Global Alliance for Rabies Control. Zero by 30: the global strategic plan to end human deaths from dog-mediated rabies by 2030. Geneva: World Health Organization; 2018.
Blanton JD, Niezgoda M, Hanlon CA, Swope CB, Suckow J, Saidy B, Nelson K, Chipman RB, Slate D. Evaluation of oral rabies vaccination: protection against rabies in wild caught raccoons (Procyon lotor). J Wildl Dis. 2018;54(3):520-7.
Changalucha J, Hampson K, Jaswant G, Lankester F, Yoder J. Human rabies: prospects for elimination. CABI Rev. 2021;16:039.
Reference
Rupprecht CE, Hanlon CA, Hemachudha T. Rabies re-examined. Lancet Infect Dis. 2002;2(6):327–43.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9(4):e0003709.
World Health Organization. Rabies [Internet]. Geneva: World Health Organization; 2023 Jun
Warrell MJ, Warrell DA. Rabies and other lyssavirus diseases. Lancet. 2004 Mar 20;363(9413):959-69. doi:10.1016/S0140-6736(04)15792-9. Erratum in: Lancet. 2004 Dec 11;364(9451):2096. PMID:15043965.
Pasteur L. Method for preventing rabies by attenuated virus inoculations. Ann Inst Pasteur. 1885.
World Health Organization, Food and Agriculture Organization of the United Nations, World Organisation for Animal Health, Global Alliance for Rabies Control. Zero by 30: global strategic plan to end human deaths from dog-mediated rabies by 2030. Geneva: World Health Organization; 2018.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015 Apr;9(4):e0003709. doi:10.1371/journal.pntd.0003709.
Cleaveland S, Kaare M, Tiringa P, Mlengeya T, Barrat J. A dog rabies vaccination campaign in rural Africa: impact on the incidence of dog rabies and human dog-bite injuries. Vaccine. 2003 May 16;21(17-18):1965-73. doi:10.1016/S0264-410X(02)00778-8.
Dzikwi AA, Ibrahim AS, Umoh JU. Knowledge, attitude and practice about rabies among children receiving formal and informal education in Samaru, Zaria, Nigeria. Glob J Health Sci. 2012 Jul;4(5):132-9. doi:10.5539/gjhs.v4n5p132.
Fooks AR, Banyard AC, Horton DL, Johnson N, McElhinney LM, Jackson AC. Current status of rabies and prospects for elimination. Lancet. 2014 Oct 4;384(9951):1389-99. doi:10.1016/S0140-6736(13)62707-5. PMID:24828901.
Taylor LH, Nel LH. Global epidemiology of canine rabies: past, present, and future prospects. Vet Med (Auckl). 2015;6:361-71. doi:10.2147/VMRR.S51147.
Fooks AR, Banyard AC, Horton DL, Johnson N, McElhinney LM, Jackson AC. Current status of rabies and prospects for elimination. Lancet. 2014;384(9951):1389-99.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al; Global Alliance for Rabies Control Partners for Rabies Prevention. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9(4):e0003709.
Rupprecht CE, Hanlon CA, Hemachudha T. Rabies re-examined. Lancet Infect Dis. 2002;2(6):327-43.
Jackson AC. Rabies: scientific basis of the disease and its management. 3rd ed. London: Academic Press; 2013.
Banyard AC, Evans JS, Luo TR, Fooks AR. Lyssaviruses and bats: emergence and zoonotic threat. Viruses. 2014;6(8):2974-90.
Warrell MJ, Warrell DA. Rabies and other lyssavirus diseases. Lancet. 2004;363(9413):959-69.
Hemachudha T, Laothamatas J, Rupprecht CE. Human rabies: a disease of complex neuropathogenetic mechanisms and diagnostic challenges. Lancet Neurol. 2002;1(2):101-9.
Jackson AC. Rabies: scientific basis of the disease and its management. 3rd ed. London: Academic Press; 2013.
Gadre G, Satishchandra P, Mahadevan A, Suja MS, Madhusudana SN, Sundaram C, Shankar SK. Rabies viral encephalitis: clinical determinants in diagnosis with special reference to paralytic form. J Neurol Neurosurg Psychiatry. 2010;81(7):812-20.
Rupprecht CE, Hanlon CA, Hemachudha T. Rabies re-examined. Lancet Infect Dis. 2002;2(6):327-43
Dacheux L, Reynes JM, Buchy P, Sivuth O, Diop BM, Rousset D, Rathat C, Jolly N, Dufourcq JB, Nareth C, Diop S, Iehlé C, Rajerison R, Sadorge C, Bourhy H. A reliable diagnosis of human rabies based on analysis of skin biopsy specimens. Clin Infect Dis. 2008;47(11):1410-7.
Warrell MJ, Warrell DA. Rabies and other lyssavirus diseases. Lancet. 2004;363(9413):959-69.
Wacharapluesadee S, Hemachudha T. Ante- and post-mortem diagnosis of rabies using nucleic acid-amplification tests. Expert Rev Mol Diagn. 2010;10(2):207-18.
Dacheux L, Reynes JM, Buchy P, Sivuth O, Diop BM, Rousset D, Rathat C, Jolly N, Dufourcq JB, Nareth C, Diop S, Iehlé C, Rajerison R, Sadorge C, Bourhy H. A reliable diagnosis of human rabies based on analysis of skin biopsy specimens. Clin Infect Dis. 2008;47(11):1410-7.
Hemachudha T, Laothamatas J, Rupprecht CE. Human rabies: a disease of complex neuropathogenetic mechanisms and diagnostic challenges. Lancet Neurol. 2002;1(2):101-9.
Smith JS, Yager PA, Baer GM. A rapid fluorescent focus inhibition test (RFFIT) for determining rabies virus-neutralizing antibody. In: Laboratory techniques in rabies. 4th ed. Geneva: World Health Organization; 1996. p. 181-92.
World Health Organization. Laboratory techniques in rabies. 4th ed. Geneva: World Health Organization; 1996.
Nadin-Davis SA, Fehlner-Gardiner C. Diagnostic tools and surveillance systems for the detection of rabies virus. Trop Med Infect Dis. 2017;2(4):53.
World Health Organization. Rabies vaccines: WHO position paper, April 2018 – Recommendations. Vaccine. 2018;36(37):5500-3.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al; Global Alliance for Rabies Control Partners for Rabies Prevention. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9(4):e0003709.
Wilde H, Khawplod P, Khamoltham T, Hemachudha T, Tepsumethanon V, Lumlerdacha B, Mitmoonpitak C, Sitprija V. Rabies control in South and Southeast Asia. Vaccine. 2005;23(17-18):2284-9.
Manning SE, Rupprecht CE, Fishbein D, Hanlon CA, Lumlertdacha B, Guerra M, Meltzer MI, Dhankhar P, Vaidya SA, Jenkins SR, Sun B, Hull HF; Advisory Committee on Immunization Practices, Centers for Disease Control and Prevention (CDC). Human rabies prevention—United States, 2008: recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 2008;57(RR-3):1-28.
Willoughby RE Jr, Tieves KS, Hoffman GM, Ghanayem NS, Amlie-Lefond CM, Schwabe MJ, Chusid MJ, Rupprecht CE. Survival after treatment of rabies with induction of coma. N Engl J Med. 2005;352(24):2508-14.
Jackson AC. Current and future approaches to the therapy of human rabies. Antiviral Res. 2013;99(1):61-7.
World Health Organization. WHO expert consultation on rabies: third report. WHO Tech Rep Ser. 2018;(1012):1-195.
World Health Organization. WHO expert consultation on rabies: third report. WHO Tech Rep Ser. 2018;(1012):1-195.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, Barrat J, Blanton JD, Briggs DJ, Cleaveland S, Costa P, Freuling CM, Hiby E, Knopf L, Leanes F, Meslin FX, Metlin A, Miranda ME, Müller T, Nel LH, et al; Global Alliance for Rabies Control Partners for Rabies Prevention. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015;9(4):e0003709.
Manning SE, Rupprecht CE, Fishbein D, Hanlon CA, Lumlertdacha B, Guerra M, Meltzer MI, Dhankhar P, Vaidya SA, Jenkins SR, Sun B, Hull HF. Human rabies prevention—United States, 2008. MMWR Recomm Rep. 2008;57(RR-3):1-28.
Cleaveland S, Kaare M, Knobel D, Laurenson MK. Canine vaccination—providing broader benefits for disease control. Vet Microbiol. 2006;117(1):43-50.
World Society for the Protection of Animals. Methods for the control of dog populations: a guide for policymakers. London: World Society for the Protection of Animals; 2007.
World Health Organization, Food and Agriculture Organization of the United Nations, World Organisation for Animal Health, Global Alliance for Rabies Control. Zero by 30: the global strategic plan to end human deaths from dog-mediated rabies by 2030. Geneva: World Health Organization; 2018.
Blanton JD, Niezgoda M, Hanlon CA, Swope CB, Suckow J, Saidy B, Nelson K, Chipman RB, Slate D. Evaluation of oral rabies vaccination: protection against rabies in wild caught raccoons (Procyon lotor). J Wildl Dis. 2018;54(3):520-7.
Changalucha J, Hampson K, Jaswant G, Lankester F, Yoder J. Human rabies: prospects for elimination. CABI Rev. 2021;16:039.
Rushali Darade
Corresponding author
Genba Sopanrao Moze College ( Department of Pharmacy)
Genba Sopanrao Moze College ( Department of Pharmacy)
Tushar Shelke
Co-author
Genba Sopanrao Moze College ( Department of Pharmacy)
Rushali Darade, Payal Dodamani, Akshata Patil, Tushar Shelke, The Fundamental Aspect of Rabies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 3315-3325. https://doi.org/10.5281/zenodo.17223189





 10.5281/zenodo.17223189
10.5281/zenodo.17223189