
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Satyajeet College of Pharmacy, Mehkar, Maharashtra, India.
The human skin microbiome plays a pivotal role in sustaining cutaneous health through barrier fortification, immunological modulation, and microbial equilibrium. This review consolidates existing insights into the diversity, spatial heterogeneity, and functional dynamics of skin-associated microbes, with particular emphasis on the manner in which intrinsic and extrinsic factors—including age, hygiene practices, ultraviolet radiation exposure, and dietary habits—modulate the microbial landscape. Illustrative case studies from Indian populations and site-specific microbial assessments further elucidate the impact of genetic background, lifestyle variables, and environmental context. Microbial dysbiosis has been implicated in a spectrum of dermatological disorders, including atopic dermatitis, acne vulgaris, psoriasis, and chronic wounds, wherein disturbances in microbial communities contribute to heightened inflammation and compromised epidermal integrity. Emerging therapeutic modalities that incorporate prebiotics, probiotics, postbiotics, and engineered bacterial strains offer compelling alternatives to conventional treatments. Notably, “triple biotic” formulations—which integrate all three biotic components—are garnering increased attention for their synergistic efficacy in restoring cutaneous microbial homeostasis. Despite these advancements, several critical limitations persist. The field currently lacks a sufficient volume of clinical trials to substantiate the long-term safety, therapeutic efficacy, and regulatory viability of engineered or synbiotic skin-based therapies. Furthermore, the absence of standardized methodologies, harmonized clinical endpoints, and comprehensive data-sharing protocols continues to obstruct the successful clinical translation of microbiome-based innovations into standard dermatological practice. By synthesizing foundational microbiome science with emerging clinical and bioengineering developments—including triple biotic strategies and microbial engineering—this review delineates both the therapeutic potential and current constraints of microbiome-directed interventions, and provides a prospective framework for their future application in dermatology.
Recent progress in microbiome research has underscored the significant influence of skin-resident microbial communities on cutaneous health, immune function, and barrier physiology. As understanding of these complex microbial ecosystems has expanded, there has been a growing interest in therapeutic interventions aimed at supporting or reinstating microbial equilibrium—particularly through the application of prebiotics, probiotics, and postbiotics. These approaches, whether employed independently or in combination, present a more targeted and sustainable alternative to conventional skincare strategies, which often rely on broad-spectrum antimicrobials or symptomatic relief. Among these emerging innovations, the integrative concept of combining prebiotics, probiotics, and postbiotics into a cohesive “triple biotic” formulation has gained notable momentum. This multifactorial strategy is designed not only to replenish beneficial microbial taxa and their bioactive metabolites but also to foster a conducive microenvironment that promotes their persistence and functional activity on the skin. Although this field remains in an early developmental phase, accumulating clinical data has begun to substantiate the dermatological benefits of such combinatory interventions. For example, recent clinical trials involving triple biotic products have reported measurable improvements in parameters such as skin hydration, barrier integrity, and microbial diversity. Nonetheless, these outcomes are distributed across varying formulations, microbial strains, and evaluation endpoints, highlighting the necessity for broader validation and mechanistic elucidation. Concurrently, advances in synthetic biology and microbial engineering have facilitated the creation of precision-targeted live biotherapeutics and bioactive microbial systems, capable of reshaping the skin microbiota with unprecedented specificity. These engineered bacterial platforms introduce novel therapeutic avenues for managing chronic inflammatory dermatoses, augmenting skin immune defenses, and delivering therapeutic agents directly at the epidermal surface. This review compiles and examines the current body of evidence regarding triple biotic approaches for enhancing skin health, incorporating findings from in vitro experiments, in vivo animal models, and human clinical studies. Particular focus is placed on the impact of specific microbial combinations on community composition, host immune responses, and dermatological outcomes such as inflammation, hydration, and barrier functionality. By critically analyzing and organizing this multidisciplinary literature, the review seeks to clarify the present state of microbiome-focused dermatological interventions, while identifying key areas that warrant further exploration to unlock their full therapeutic potential.
1.1Definition and composition of the skin microbiome
The skin microbiome denotes the intricate and dynamic consortium of microorganisms that inhabit the human skin, functioning as a crucial interface between the host and the external environment. This microbial community comprises a diverse array of taxa—including bacteria, fungi, viruses, archaea, and mites—that coexist with host epidermal cells. Most of these organisms exhibit commensal (nonharmful) or mutualistic (beneficial) relationships with the host, although certain taxa may become pathogenic under specific environmental or physiological conditions.
Major Microbial Groups
1. Bacteria
Bacteria constitute the most abundant members of the skin microbiome and are predominantly represented by four phyla: Actinobacteria (36–51%), Firmicutes (24–34%), Proteobacteria (11–16%), and Bacteroidetes (6–9%).
These bacterial communities contribute to immune modulation, pathogen competition, and maintenance of the skin barrier.
2. Fungi
Fungal populations are predominantly composed of lipophilic Malassezia species, which preferentially colonize sebaceous zones such as the scalp and facial skin. While these yeasts form part of the normal flora, dysregulated overgrowth is associated with conditions such as seborrheic dermatitis and dandruff.
3. Viruses
The skin virome primarily comprises bacteriophages, which infect bacterial hosts, and eukaryotic viruses such as papillomaviruses and polyomaviruses. These viral elements can influence bacterial community structure and functionality.
4. Mites
Demodex species—most notably D. folliculorum and D. brevis—reside within hair follicles and sebaceous glands. Generally benign, they have been implicated in certain inflammatory dermatoses, such as rosacea.
5. Archaea
Although present in relatively low abundance, archaea have been identified predominantly in sebaceous skin regions. Their precise functional roles remain under investigation.
Spatial and Temporal Variation
The skin microbiome exhibits pronounced site specificity, as each anatomical region presents a unique combination of sebum, moisture, and pH, resulting in distinct microbial assemblages. For instance:
The forehead and upper back are dominated by lipid-metabolizing species.
The antecubital fossa (inner elbow) supports organisms adapted to moist environments.
1.2 Functions and Importance in Skin Health
The skin microbiome is not simply a passive colonizer; it performs active functions essential for homeostasis, defense, and repair.
A. Barrier Protection and Competitive Exclusion
Commensal microbes protect the host by occupying ecological niches, thereby preventing pathogen overgrowth through competitive exclusion. Many skin bacteria produce antimicrobial peptides (AMPs)—for example, Staphylococcus epidermidis secretes phenol?soluble modulins that inhibit Staphylococcus aureus colonization . These AMPs complement host?derived peptides, bolstering the skin’s chemical barrier against invading microbes .
B. Immune Education and Modulation
The microbiome plays a critical role in educating the immune system, particularly innate immunity. Skin commensals continually interact with keratinocytes, Langerhans cells, and other immune cells to calibrate immune responses . Through pattern recognition receptors (e.g., Toll?like receptors), microbes stimulate low?level cytokine production that maintains immune tolerance, preventing unnecessary inflammation while priming defenses against real threats . Stimulate host defenses only when needed.
C. pH Regulation and Acid Mantle Formation
Skin commensals contribute to the formation and maintenance of the acid mantle, a thin, slightly acidic film (pH?4.5–5.5) on the stratum corneum that inhibits pathogen colonization . They generate free fatty acids and other acidic metabolites (e.g., lactic acid) via sebum and sweat metabolism, sustaining an environment hostile to many opportunistic microbes . This acid mantle also optimizes the activity of pH?dependent enzymes crucial for lipid synthesis and barrier repair .
D. Wound Healing and Tissue Repair
Certain commensals enhance wound healing by promoting keratinocyte proliferation and migration. Cutibacterium acnes, for instance, produces short?chain fatty acids that drive epidermal regeneration and modulate local inflammation . Staphylococcus epidermidis can upregulate host AMPs and growth factors that accelerate re?epithelialization, reducing scar formation.
E. Systemic and Neuro?Immune Interactions (Emerging)
Emerging research suggests a skin–brain–microbiome axis, whereby skin microbiota influence, and are influenced by, psychological stress and systemic immune responses . Stress?induced hormonal changes can shift microbial composition, which in turn may affect cutaneous barrier integrity and inflammation, linking psychological states to skin disorders
1.3 Skin Microbiome variation in Indian Families.
Family Structure and Sampling
In India, multi-generational “joint families” coexist under one roof, sharing genetics, diet, lifestyle, and environment, providing a unique natural experiment for skin microbiome studies .A recent investigation sampled axillary sweat from 72 individuals across 15 families (three generations, G1: 65–91 yrs; G2: 41–63 yrs; G3: 13–30 yrs) in two Maharashtrian cities (Pune and Ahmednagar). Rigorous controls (no deodorant, standardized collection) minimized transient contamination.
Taxonomic Composition and Diversity
Across families, the most abundant phyla were Firmicutes (mean ~ 73 %), Proteobacteria (~ 24 %), and Actinobacteria (~ 3 %); dominant genera included Staphylococcus (~ 51 %), Bacillus (~ 16 %), and Pseudomonas (~ 9 %). Overall Shannon α-diversity did not differ significantly by age or sex but showed moderate associations with diet (vegetarian vs. mixed; FDR < 0.1) and location (Pune vs. Ahmednagar; FDR < 0.1).
Influence of Geography, Diet, and Cohabitation
β-Diversity (Bray–Curtis) revealed a highly significant familial signature (PERMANOVA p = 0.001) and a borderline effect of geography (p = 0.07), whereas diet, age, and sex were non-significant. Within-family microbiomes were, on average, more similar than those between families—suggesting that cohabitation (shared environment and behaviors) and/or genetics impart a unique “family microbiome”. A parallel study of Indian patrilineal families also found no clear clustering by age or gender but echoed familial patterns in skin profiles Nature.
1.4 Factor affecting Intrinsic and extrinsic factor.
The skin microbiome is shaped by a complex interplay of intrinsic (host?related) and extrinsic (environmental or behavioral) factors. These determinants modulate microbial diversity, community structure, and functional interactions, thereby influencing skin health and disease propensity.
1.4.1 Intrinsic Factors
5. Ethnicity
1.4.2 Extrinsic Factors
3.Occupation and Environmental Contact
4.Textiles and Occlusion
5. Diet
6.Climate, UV Exposure, and Geography
MATERIAL AND METHOD
Study Design and Sampling
Microbiome Analysis
In Vitro Experiments
Results
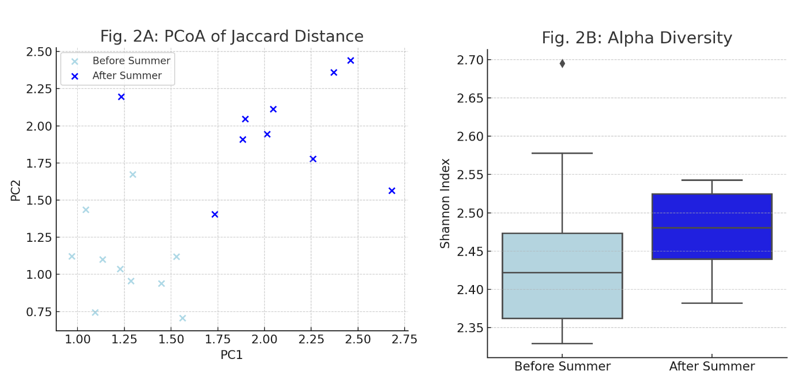
Changes in Skin Microbiome Composition (Fig. 2)
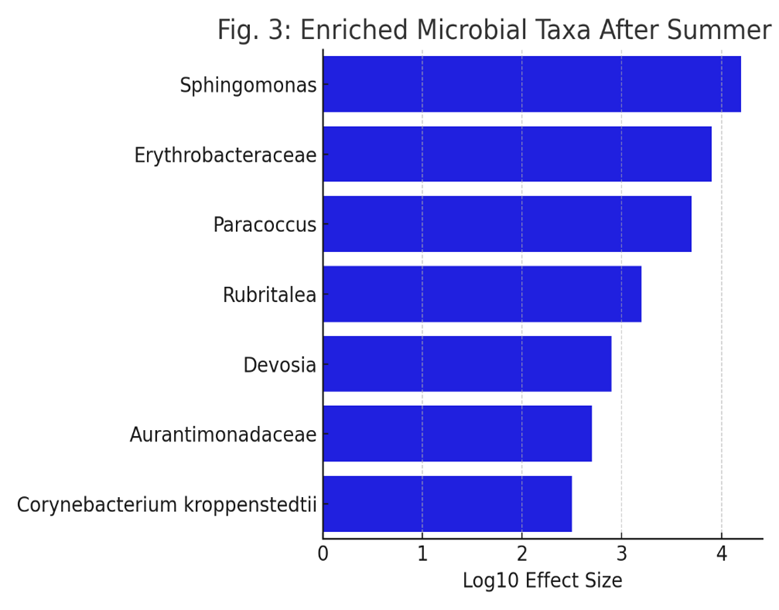
Enrichment of Specific Bacterial Taxa (Fig. 3)
Fig. 3: LEfSe analysis identified specific bacterial taxa that increased in relative abundance after the summer. The figure displays taxa (at family or genus level) present in at least 50% of volunteers, with notable increases in Sphingomonas and Erythrobacteraceae.
Individual Responses in Key Bacterial Families (Fig. 4)
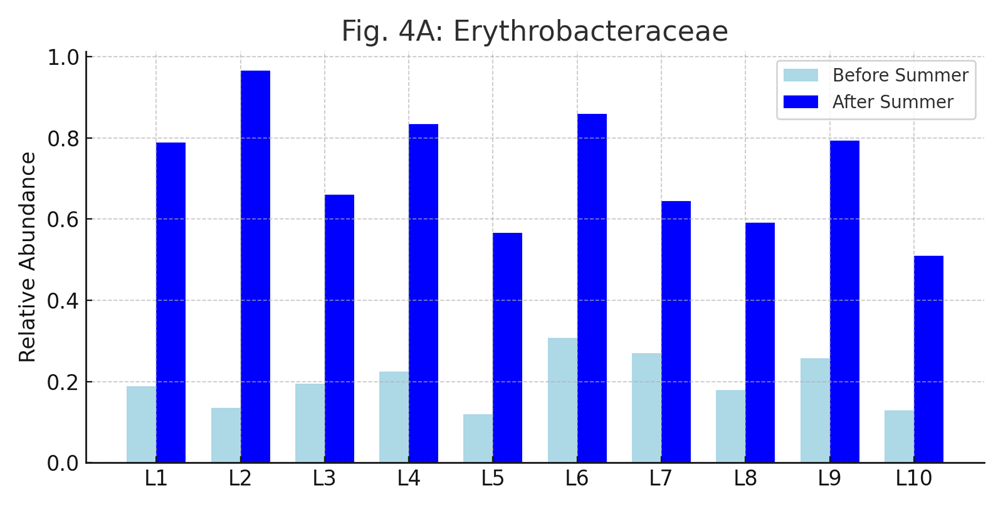
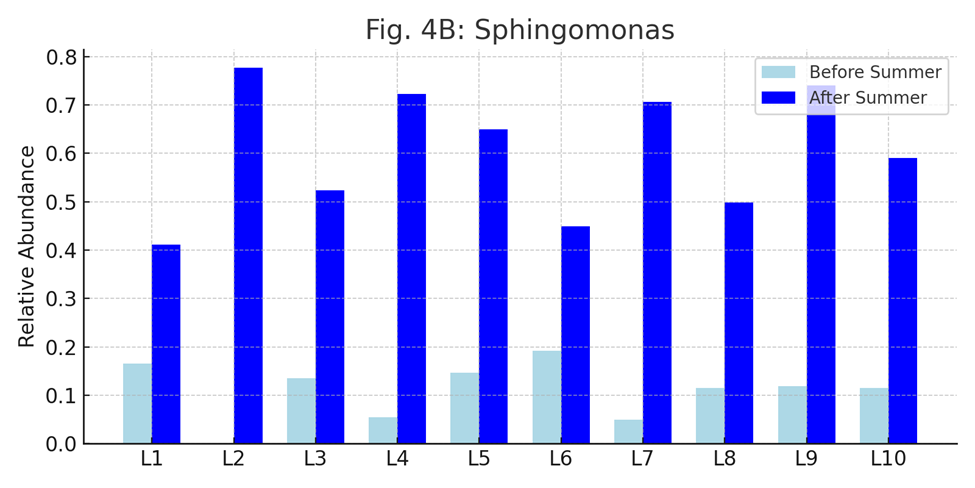
Fig. 4: This figure presents the relative abundances of Erythrobacteraceae (A) and Sphingomonas (B) in each lifeguard before and after the summer. Most participants showed increased levels of these bacteria after prolonged sun exposure.
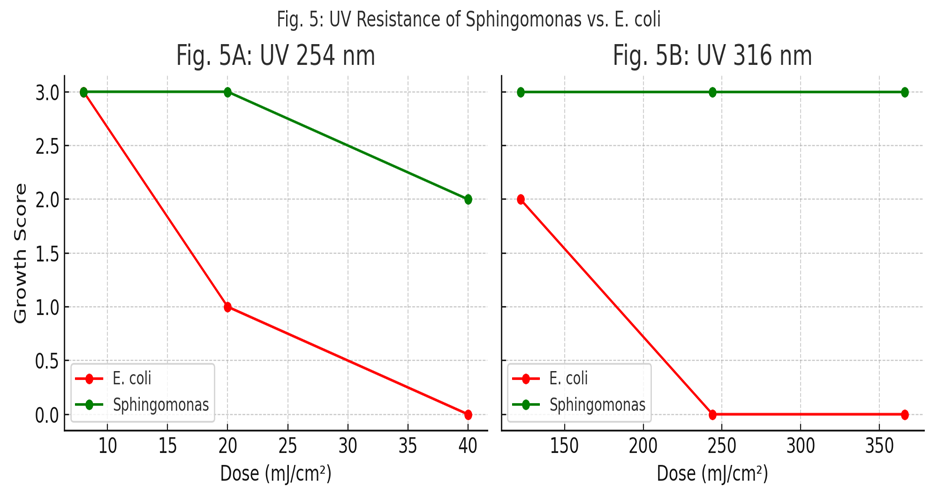
UV Resistance of Sphingomonas (Fig. 5)
DISCUSSION
1.5 Methods of Skin microbiome exploration.
→ are culture-independent, as they analyze microbial communities directly using molecular and computational tools.
1.5.1 Ongoing and Proposed Approaches (Table?1)
|
Step |
Current Methods |
Ongoing/Proposed Improvements |
|
1.Sampling
|
Swabs (dry/moistened), tape-stripping,punch biopsies |
Engineered stabilization kits(eg., OMNIgene*SKIN),3D-printed microprojection arrays for spatially resolved sampling |
|
2.Nucleic Acid Extraction
|
Commercial low-input kits (Qiagen,MoBio), bead-beating Or enzymatic lysis |
Protocols optimized for ultra-low biomass and resilient cutaneous microbes; enhanced host-DNA depletion strategies |
|
3.Sequencing
|
Short-read amplicon( 16S rRNA, ITS) on Illumina; targeted qPCR/RT-qPCR |
Long-read/hybrid platform (Nanopore, PacBio) for full-length marker gene; shotgun metagenomics; metatranscriptomics |
|
4.Bioinformatics Analysis
|
Alpha/beta diversity; taxonomic classification Against SILVA, Greengenes. |
ASV-based denoising (e.g., DADA2) for single-nucleotide Resolution; skin specific reference database; multi-omics integration |
Note: Table1 highlights how each workflow step is being refined to improve sensitivity, resolution, and functional insight in skin microbiome research.
1.5.2 Assessing Reagents and Cross?Contamination (Table?2)
|
Control |
Applied at |
Purpose |
Expected Outcome |
|
Extraction Blank
|
DNA/RNA extraction and library prep |
Reveal DNA from reagents (“kitom”) or plasticware; detect cross-contamination during extraction |
Negligible nucleic acid; minimal amplification; low read counts distinct from true samples |
|
Sampling Negative
|
Collection |
Identify environmental or handling contamination at the point of sampling |
No or minimal DNA; profile matches ambient background rather than skin |
|
PCR No-Template
|
Library preparation |
Detect contaminants introduced during amplification (reagent, aerosols) |
No or minimal amplification product |
|
PCR Positive |
Library preparation |
Verify amplification reagents and thermocycle performance |
Amplicon/library of expected size and yield |
|
Mock Community
|
Extraction Analysis |
Benchmark pipeline sensitivity,specificity, and quantitative accuracy using defined mixtures of cells, DNA, or in silico genomes |
Recovery of expected taxa at correct proportions; metrics of false positive/negative |
|
Technical Replicates
|
Extraction, library, sequencing |
Quantify variability from low_biomass stochastic effects; improve reproducibility |
Consistent profiles across replies; outlier detection |
|
Host Depletion controls |
Extraction/library prep |
Validate efficacy of host- DNA/RNA removal methods |
Enrichment of microbial reads over host reads without introducing bias |
Prevention is the best cure and several best practices can be applied to minimize the impact of reagents combinations and cross – contamination on skin microbiome results when adding one or several of the above – mentioned control.
Best Practice: Sequence all controls alongside samples and apply bioinformatic tools e.g., decontam ( amplicon and shotgun metagenomics),SourceTracker, microDecon ( amplicon data), Recentrifuge ( shotgun metagenomics data),Squeegee ( shotgun metagenomics data with the possibility of application to amplicon data )to identify and remove contaminant signatures.
The comparative overview of the methodological approaches employed in exploring the skin and gut microbiome. Although many techniques overlap due to shared microbiome principles, there are important distinctions due to the anatomical and biological differences between skin and gut environments. The content is synthesized from quality-controlled pipelines used in large-scale studies and adapted to suit both high- and low-biomass microbial communities.
Table 3: Comparative Methodologies for Skin vs. Gut Microbiome Analysis
|
Step |
Skin Microbiome |
Gut Microbiome |
|
Sample Collection |
Sterile swabs or tapes from defined areas (e.g., forehead, forearm). |
Stool collected in sterile containers. |
|
Post-Collection Handling |
Swabs into stabilization buffer or on dry ice. |
Stool mailed ambient or cold, then frozen. |
|
Storage Conditions |
Stored at –80°C. |
Initial –20°C, then –80°C upon lab receipt. |
|
DNA Extraction |
Bead beating + low biomass kits (e.g., QIAamp BiOstic). |
Bead beating + Arrow Stool DNA or PowerSoil kits. |
|
DNA Quantification |
PicoGreen adapted for low DNA yield. |
PicoGreen quantification in 96-well format. |
|
16S rRNA Region |
V3–V4 or V4 hypervariable regions. |
V3–V4 region commonly used. |
|
Library Preparation |
PCR amplification, SequalPrep normalization, AMPure XP, LabChip. |
Similar process with higher yield. |
|
Sequencing Platform |
Illumina MiSeq (2×250 bp). |
MiSeq or NovaSeq for deeper coverage. |
|
Reference Databases |
SILVA v138.1, Greengenes2; ASV via DADA2. |
Same databases and tools (QIIME, Deblur, UPARSE). |
|
Quality Filtering |
DADA2 filtering (error ≤2), chimera removal, low abundance filtering. |
Same parameters with ≥4K reads/sample threshold. |
|
Normalization |
Rarefaction to even depth or VST (CLR, DESeq2). |
Similar, often rarefied to 4K reads. |
|
Batch Effect Mitigation |
Track metadata (e.g., season, storage time); use ComBat, removeBatchEffect. |
Include batch variables in PERMANOVA, multivariate models. |
|
Contamination Controls |
Negative/positive controls; beta diversity & host DNA for swaps. |
Sex typing qPCR; Aitchison distance for same-sex swaps. |
|
Diversity Analysis |
Shannon index (alpha), CLR + Aitchison (beta). |
Same methods applied. |
|
Differential Abundance |
Compositional models (ANCOM, ALDEx2). |
Same statistical tools used. |
|
Multivariate Modeling |
PERMANOVA, MaAsLin2. |
Identical approaches. |
|
Visualization |
Donut plots, heatmaps, PCoA/NMDS. |
Same visualization methods. |
Table 4: Key Differences at a Glance
|
Step |
Skin Microbiome |
Gut Microbiome |
|
Sample Type |
Swabs or adhesive tapes from skin sites |
Stool samples |
|
Storage |
-80°C after collection |
Mailed at -20°C, then -80°C in lab |
|
DNA Extraction |
Low biomass kits (e.g., QIAamp BiOstic) |
High biomass kits (e.g., Arrow Stool DNA kit) |
|
Sequencing Platform |
Illumina MiSeq (2×250?bp) |
NovaSeq or similar high-throughput platforms |
|
Read Filtering |
Higher stringency due to low biomass |
Standard filtering parameters |
|
Contamination Checks |
Negative/positive controls, swaps |
Sex typing, host DNA contamination checks |
|
Taxonomic Resolution |
Genus level common |
Strain-level possible |
|
Applications |
Dermatological studies |
GI health, systemic disease |
2.The Skin Microbiome in Health and Disease
2.1. Role in maintaining skin homeostasis
The skin functions first and foremost as a physical barrier, preventing pathogen ingress and desiccation while simultaneously providing a habitat for commensal microbes that contribute to cutaneous health . Embedded within this barrier are multiple innate immune defenses—notably antimicrobial peptides such as β-defensins, substance P, and cathelicidins—that exhibit broad-spectrum activity against bacteria, viruses, and fungi by disrupting microbial membranes without harming host cells . These peptides can be constitutively expressed or upregulated in response to injury or microbial challenge; for example, cathelicidin levels are abnormally elevated and processed in rosacea, whereas reduced antimicrobial peptide expression in atopic dermatitis predisposes to infection . Beyond peptides, the skin’s cellular innate defenses—including Langerhans cells, natural killer cells, neutrophils, and resident lymphoid populations—continuously survey for and eliminate invading organisms, secrete cytokines that shape adaptive immunity, and help maintain equilibrium between tolerance of commensals and clearance of pathogens . Together, these structural and immunological mechanisms underpin skin homeostasis, orchestrating a balance between barrier integrity, microbial colonization, and immune responsiveness.
2.2. Dysbiosis and its impact on dermatological conditions
Dysbiosis denotes a state in which the normal balance of the skin microbiome—both in species composition and functional capacity—is disrupted, leading to pathological outcomes .
Such microbial imbalance can impair the epidermal barrier, enhancing transepidermal water loss and permitting allergen or pathogen invasion, which fuels cutaneous inflammation.
Furthermore, dysbiosis skews immune education: commensals that ordinarily induce regulatory T?cells diminish, while pro?inflammatory taxa expand, exacerbating disease susceptibility.
Clinical evidence links dysbiosis to worsened disease severity and chronicity across multiple skin disorders, underscoring its central role in dermatological pathophysiology.
"Dysbiosis is an imbalance in microbial composition, often leading to reduced diversity or pathogenic overgrowth. It has been implicated in various skin disorders, including acne, atopic dermatitis, and psoriasis."
One compelling illustration of microbiome-associated dysbiosis is observed in chronic wounds, particularly diabetic foot ulcers, which serve as a model for studying the disruption and restoration of microbial balance during the healing process. Recent research has shown that:
"The microbial landscape of diabetic ulcers evolves during healing. In a study involving 10 diabetic patients treated with a fluorescein-based galenic therapy (Fluorexin), 16S rRNA sequencing revealed significant shifts in bacterial communities within the ulcer bed over 20 days."
Initially, these chronic wounds are dominated by pathogenic species, such as Staphylococcus aureus, which is often associated with inflammation and delayed wound healing. However, as healing progresses:
"There was a reduction in S. aureus and an increase in beneficial genera such as Corynebacterium, Propionibacterium, Streptococcus, and Pseudomonas."
These microbial shifts occurred without the use of topical or systemic antibiotics, highlighting the potential of non-antibiotic antimicrobial and anti-inflammatory approaches to support the healing process. The therapy also led to:
"A reduced prevalence of opportunistic pathogens like Enterococcus, Finegoldia, and Peptoniphilus."
Furthermore, comparison between microbiota at the ulcer bed (intralesional) and the surrounding skin (perilesional) revealed insights into microbial origins and dynamics:
"Comparison between intralesional (ulcer bed) and perilesional (surrounding skin) microbiota showed no major compositional differences at baseline (t0), supporting the hypothesis that ulcer microbiota may arise from the adjacent skin."
However, notable changes in diversity and genus prevalence occurred post-treatment, with significant variation depending on ulcer location:
"Diversity and genus prevalence did change significantly post-treatment, especially depending on ulcer location (e.g., plantar vs. lower leg), with plantar ulcers showing greater homogeneity."
These findings underscore several critical points:
As such, the study provides a compelling case for the therapeutic potential of skin microbiome modulation in wound care, and it reinforces the broader relevance of dysbiosis in the development and resolution of dermatological conditions.
3.Skin Microbiome in Dermatological Conditions
3.1. Eczema and atopic dermatitis
Atopic dermatitis (AD) is characterized by marked dysbiosis, notably a sharp decline in overall bacterial diversity and the overrepresentation of Staphylococcus aureus in lesional skin.
Up to 90?% of AD patients are colonized by S. aureus, compared to ~5?% of healthy individuals, and disease flares correlate with increased S. aureus density.
Strain?level profiling reveals that specific S. aureus lineages carry toxins and proteases (e.g., phenol?soluble modulins, bacteriocins) that directly damage the epidermal barrier and trigger inflammation
Conversely, commensals such as coagulase?negative staphylococci and Cutibacterium spp. normally secrete antimicrobial peptides that limit pathogen overgrowth; their depletion in AD permits pathogenic blooms. Emerging metagenomic studies also implicate shifts in the fungal mycobiome—such as increased Malassezia osloensis—and elevated bacteriophage loads during AD flares, underscoring the multi?kingdom nature of dysbiosis in eczema.
3.2. Acne vulgaris
"Acne is a long-lasting inflammatory skin condition that affects sebaceous glands and hair follicles. Skin rashes, including whiteheads, blackheads, pustules, papules, and cysts on the face, chest, back, and shoulders are the primary clinical symptoms.
The main contributory factors to acne vulgaris are:
Acne is tightly linked to both the abundance and strain diversity of Cutibacterium acnes within the pilosebaceous unit. Acne patients often harbor a higher ratio of acne?associated C. acnes lineages and a lower relative abundance of protective species like C. granulosum. Metagenomic analyses reveal that acneic skin shows enrichment of genes involved in pro?inflammatory metabolite production and biofilm formation, while healthy skin exhibits greater diversity of metabolic pathways that may antagonize C. acnes overgrowth. Cross?talk with Staphylococcus epidermidis is also evident: certain S. epidermidis strains produce antimicrobials that inhibit C. acnes, but in acne, strain?level shifts can turn S. epidermidis into a secondary driver of inflammation via protease secretion.
Probiotic Acne Treatment:
Certain lactic acid bacteria, specifically Streptococcus thermophiles, have been found to enhance ceramide production in the stratum corneum when topically applied as a cream. Ceramides are lipids that play a crucial role in maintaining the skin’s barrier function and hydration levels, and this is particularly beneficial for individuals with acne-prone skin because acne treatments can sometimes lead to dryness and irritation. Additionally, it shows antimicrobial activity against Cutibacterium acnes, a bacterium associated with the development of acne.
3.3 Psoriasis
Psoriasis involves immune dysregulation and microbial imbalance, particularly increased Staphylococcus species and reduced fungal diversity—mainly a dominance of Malassezia restricta and M. globosa. Lesions also show depletion of anti-inflammatory bacteria like Faecalibacterium prausnitzii and enrichment of Streptococcus, promoting Th1/Th17-mediated inflammation. Therapies such as TNF-α and IL-17 inhibitors, and phototherapy, can partially normalize skin (and even gut) microbiota. This suggests that microbial shifts contribute to disease pathology and resolution, reinforcing the relevance of the gut–skin axis in psoriasis management.
Product: Gallinee Soothing Body cream Prebiotic- Alpha-glucan oligosaccharide, inulin promotes beneficial bacteria; suitable for inflammatory skin like psoriasis.
3.4 Other Skin Disorders Linked to Microbiome Imbalance
Rosacea : features increased densities of Demodex folliculorum mites and associated bacteria like Bacillus oleronius, which trigger innate immune activation through proteases and cathelicidin LL?37 upregulation. alongside shifts in S. epidermidis that may produce temperature?dependent virulence factors.
Alterations in the cutaneous and gut microbiome further amplify chronic inflammation;
Hidradenitis Suppurativa (HS): Is marked by decreased alpha diversity and overgrowth of anaerobes such as Porphyromonas and Prevotella in lesional skin, correlating with chronic inflammation in apocrine?rich folds. HS lesions also demonstrate impaired antimicrobial peptide expression and complement dysregulation, compounding microbial invasion and biofilm formation. Broad?spectrum and targeted antibiotics, combined with biologics (adalimumab, secukinumab), offer partial remission, while novel microbiome?targeted approaches remain under investigation.
Vitiligo: In general, the gut microbiota is responsible for the body’s appropriate immunity and defense against harmful microbes. Therefore, alterations that are considered harmful at the intestinal microbiota level may result in infections and autoimmune diseases in a variety of organs outside of the colon, including the skin . A recent study shows that patients with vitiligo have a different microbial composition from healthy people, with a considerably lower Bacteroidetes to Firmicutes ratio. They also differ significantly from healthy people in 23 blood metabolites, and these metabolites are linked to particular microbial indicators. Commensal bacteria are vital components of the skin microbiome and play a crucial role in skin health. Another study highlights that vitiligo-affected skin exhibits a dysbiosis in microbial community diversity, with lesional areas showing reduced taxonomic richness and evenness. Notably, Actinobacterial species are dominant in normal skin, while Firmicutes species dominate in vitiligo lesions, suggesting that these microbial changes could influence the development and severity of vitiligo.
4.The Interplay Between Skin Microbiome and Skincare
4.1. Effects of traditional skincare products on the skin microbiome
Recent clinical studies have revealed the nuanced impact of various skincare formulations on the skin microbiome. In a split-face, randomized, double-blind study, 26 women applied a preservative-containing regimen (CSP) to one cheek and a preservative-free regimen (PFP) to the other for three weeks. High-throughput sequencing and bioinformatics analyses (QIIME2, DADA2, CLR transformation, ANCOMBC2) identified key microbial shifts and correlations with skin quality metrics.
Key Findings:
4.1.1. Ingredient-Level Effects on Microbiota
These insights highlight the need for microbiome-friendly formulations that preserve core communities while selectively targeting pathogens.
4.2. Probiotics, prebiotics, and postbiotics in skincare
4.2.1 Probiotic Lysates as Postbiotics
Topical postbiotics are inactivated microbial preparations—lysates or fermentation broths—rich in peptides, organic acids (e.g. lactic acid), and cell?wall fragments. Unlike live probiotics, they do not require viability, offering enhanced shelf life and safety in formulations .
Lysates of Lactobacillus rhamnosus (LR) have been shown to:
Clinical application of LR lysate in a VHProbi® lotion improved transepidermal water loss (TEWL) and skin hydration over eight weeks in healthy volunteers, demonstrating barrier restoration and soothing effects.
4.2.2 Prebiotics Feeding Resident Microbes
Prebiotics in skincare—typically non?digested oligosaccharides like inulin, arabinogalactan, or galacto?oligosaccharides—serve as fermentable substrates for resident commensals (e.g. Cutibacterium acnes’ benign strains, Staphylococcus epidermidis), promoting their growth over pathogens .
By selectively fueling beneficial microbes, prebiotics:
4.2.3 Synergistic Formulations
Combining probiotic lysates with prebiotic polymers (synbiotic approach) yields synergistic effects: the lysate delivers signaling molecules that modulate keratinocyte gene expression (e.g. upregulation of ceramide synthesis), while prebiotics sustain repopulation of beneficial taxa. Such formulations are typically delivered as:
4.2.4 Skin Brightening and Pigmentation Control
Probiotics and their derivatives have shown promising effects in skin brightening and reducing freckles by modulating pigmentation pathways.
Topical probiotics with these effects include Lactobacillus plantarum, Bifidobacterium longum, and their lysates, now used in whitening serums and anti-freckle creams.
4.2.5 Bioconversion Technologies in Probiotic Skincare
A novel approach utilizes bioconversion via probiotic fermentation to enhance the bioactivity of plant extracts. One example is the Bioconverted Chestnut Shell Extract (BCS) fermented with Lactiplantibacillus plantarum SM4.
* ↑2.6x polyphenols
* ↑5.4x flavonoids
* ↑1.3x antioxidant activity
* ↑1.2x UVA absorption
* ↓ TRP-1/TRP-2 expression (melanin suppression)
Table 4: Functional Summary of Probiotic Mechanisms
|
Function |
Mechanism |
|
Whitening
|
Tyrosinase inhibition, gene downregulation, antioxidant activity |
|
Barrier Support |
Ceramide/lipid production via keratinocyte stimulation |
|
Anti-aging |
Free radical scavenging, increased hydration |
|
Anti-inflammatory |
Suppression of IL-6, TNF-α; restoration of microbiome balance |
4.2.6 Commercial Examples Featuring Probiotic Lysates
Well-known cosmetic products utilizing probiotic technologies:
These real-world examples demonstrate the growing role of probiotic formulations in dermatological and cosmetic applications.
4.2.7 Triple Biotic Technology: A Case Study in Synbiotic Skincare
Triple Biotic Technology combines probiotics, prebiotics, and postbiotics to synergistically enhance skin health by restoring and protecting the skin microbiome. A recent study demonstrated the clinical efficacy of this approach in improving skin barrier function, hydration, and overall skin quality.
The technology includes:
In a double-blind, placebo-controlled clinical trial, a triple biotic serum was applied to the facial skin of 66 female participants over 28 days. Results showed:
A 40% reduction in visible dryness.A 32% improvement in skin hydration (measured via corneometry).Enhanced microbiome diversity and stability (via 16S rRNA sequencing). Furthermore, metagenomic analyses revealed increased abundance of Staphylococcus epidermidis and Cutibacterium granulosum, both known for their roles in barrier integrity and pathogen resistance. The study emphasized the importance of maintaining microbial balance, as dysbiosis was correlated with reduced hydration and barrier dysfunction. This case exemplifies the potential of synbiotic formulations in dermatology, especially when targeting sensitive, dry, or dysbiotic skin conditions. The combination of all three biotic types ensures immediate barrier support, sustained microbial modulation, and long-term skin health benefits.
5.Engineering Bacteria for Dermatological Applications
5.1. Overview of engineered bacteria and bacterial products
Engineered live biotherapeutic products (eLBPs) are genetically modified microbes designed to perform therapeutic functions at the host interface, such as synthesizing antimicrobial peptides or secreting immunomodulatory factors directly on the skin. These platforms often leverage Generally Recognized As Safe (GRAS) strains—like Lactobacillus or Staphylococcus epidermidis—as chassis for therapeutic gene cassettes. Material science innovations embed these bacteria in hydrogels or microneedle arrays to protect them from environmental stressors and enable controlled release on the skin surface.
Microalgal Photosynthetic Patch.
A living patch composed of the microalga Chlamydomonas reinhardtii immobilized on a fibrin scaffold delivers oxygen directly to hypoxic chronic wounds. In a porcine model, this eukaryotic LBP accelerated re?epithelialization and angiogenesis without adverse immune activation .
Yeast-Based Delivery Systems.
Recombinant Saccharomyces cerevisiae particles loaded with curcumin illustrate eukaryotic cell–mediated drug carriers for topical antioxidant therapy, showing sustained release and enhanced skin penetration in ex vivo human skin assays .
5.2. Genetic engineering approaches for skin microbiome modulation
CRISPR-Cas systems, genetic toggle switches, and quorum-sensing circuits have been adapted to skin eLBPs, allowing bacteria to sense disease biomarkers (e.g., inflammatory cytokines) and respond by producing therapeutic molecules only when needed. Directed evolution and promoter engineering optimize expression levels of payload genes (e.g., anti-Staphylococcal bacteriocins) without imposing fitness costs on the chassis. Safety mechanisms—such as kill-switches triggered by environmental cues—prevent uncontrolled bacterial proliferation outside the target site.
Multivalent GM?Lactococcus lactis.
The L.?lactis MG1363 strain was engineered to co?express human FGF?2, IL?4, and CSF?1, combining pro?angiogenic and immunomodulatory signals. In a Phase?II trial for diabetic ulcers, this cocktail enhanced granulation tissue formation and reduced time to wound closure versus placebo .
Quorum?Sensing “Detect?and?Destroy” in S. epidermidis.
The engineered S. epidermis act like biosensor. These engineered strains can detect signaling molecules (called autoinducing peptides) that are naturally produced by S. aureus during quorum sensing (a way bacteria communicate).When these signals are detected, the engineered S. epidermidis responds by releasing antimicrobial peptides. This “detect-and-destroy” approach has shown promise in reducing S.aureus in mouse models of atopic dermatitis.
5.3. Applications in targeted therapy for skin disorders
5.3.1 Atopic dermatitis (eczema): Topical applications of Roseomonas mucosa genetically modified non?Staphylococcus commensals have entered clinical testing were associated with epithelial repair via TNF?mediated lipid signaling in a small open?label study,and Vitreoscilla filiformis extracts improved disease severity in randomized eczema trials . These programs underscore the potential of both whole?cell and extract?based approaches to rebalance dysbiotic skin ecosystems to secrete anti?inflammatory lipids have reduced inflammation and S. aureus colonization in early?phase trials .
5.3.2 Acne vulgaris: Strains engineered to overproduce antimicrobial peptides against Cutibacterium acnes have demonstrated preclinical efficacy in murine models, paving the way for first?in?human studies .
5.3.3 CXCL12?Producing Limosilactobacillus reuteri (ILP100).
Topical ILP100 accelerated wound healing in diabetic?wound pig models through localized CXCL12 release embedded in a hydrogel, promoting keratinocyte migration and neovascularization. This program has advanced to Phase?I trials with a planned 5?year safety follow?up .
5.3.4 Sphingomyelinase?Overexpressing Coagulase?Negative Staphylococci.
Engineered S. carnosus expressing skin?beneficial sphingomyelinase enzymes serves as a testbed before deploying analogous constructs in S. epidermidis, demonstrating increased ceramide production and barrier restoration in reconstructed human epidermis .
5.3.5 Engineered skin bacteria induce antitumor T cell responses against melanoma
Recent advancements in synthetic biology and immunology have paved the way forutilizing engineered skin commensals as therapeutic agents in dermatology. A seminal example of this approach is presented in a study by Chen et al. (2023), wherein Staphylococcus epidermidis—a common human skin bacterium—was genetically engineered to express tumor antigens and used to elicit antigen-specific immune responses against melanoma. This study serves as a groundbreaking case demonstrating the potential of commensal microbes in targeted therapy for skin-related malignancies. In this study, strains of S. epidermidis were engineered to express either full-length or peptide fragments of the ovalbumin (OVA) antigen and melanoma-associated neoantigens. Upon topical colonization of murine skin, these engineered strains induced robust CD8? and CD4? T cell responses specific to the expressed tumor antigens. Remarkably, these T cells were capable of migrating from the skin to tumor sites—including distal and metastatic lesions—where they infiltrated the tumors and exerted cytotoxic effects. The engineered bacteria demonstrated significant antitumor activity in both subcutaneous and metastatic melanoma models, with further enhancement when combined with immune checkpoint inhibitors such as anti-PD-1 therapy. Crucially, this approach avoided the systemic toxicity and inflammation commonly associated with other immunotherapeutic strategies. The therapeutic effect was found to be dependent on bacterial viability and antigen localization, indicating that active colonization and optimized antigen presentation are essential for effective immune priming.
This case study exemplifies the viability of using engineered skin microbiota not just as passive modulators of immunity, but as active participants in precise, site-directed immunotherapy. It opens a novel therapeutic avenue in dermatology—particularly for cutaneous malignancies like melanoma—by leveraging the skin's existing microbial ecosystem to deliver and sustain localized immune activation.
Despite these promising outcomes, several critical challenges remain unresolved. Notably, the clinical translation of such strategies is in its infancy. There is a lack of extensive clinical trials evaluating the long-term safety, stability, and efficacy of engineered commensal bacteria in human populations. Potential issues such as host-microbiome compatibility, immunogenic tolerance, gene transfer risks, and the regulatory complexity of live biotherapeutic products require rigorous investigation.
This innovative approach marks a critical step toward personalized and microbiome-integrated dermatological treatments. However, addressing the outlined research gaps through well-designed clinical trials, biosafety evaluations, and regulatory frameworks is essential before such therapies can become mainstream in dermatological practice.
5.3.6 Psoriasis Using Engineered Bacteria
Psoriasis, a chronic immune-mediated skin disorder, is characterized by hyperproliferation of keratinocytes and inflammation, often requiring long-term topical treatments with limited patient adherence. Recent advances in synthetic biology have enabled the development of engineered bacteria as targeted delivery vehicles for sustained, localized therapy. A notable example is the work of Montgomery et al. (2024), who investigated the use of Bacillus subtilis as a microbiome-based platform for topical drug delivery. By engineering B. subtilis to express green fluorescent protein (GFP) as a model therapeutic, the researchers evaluated its survival, expression capacity, and safety profile on ex vivo pig skin, human skin tissue cultures, and in vivo mouse models. The engineered strain showed persistent colonization and protein production on the skin for up to 5 days, especially when supported by selective pressures such as malate or kanamycin. Moreover, no significant cytotoxic effects were observed in keratinocyte assays or histological analysis of treated mouse skin. Given B. subtilis’ genetic tractability and status as a GRAS (Generally Recognized as Safe) organism, its application in delivering anti-inflammatory or immunomodulatory agents holds significant promise for managing psoriasis. These findings underscore the feasibility of developing next-generation, microbiome-integrated therapeutics aimed at reducing flare-ups, improving skin barrier function, and enhancing adherence in psoriasis care. Further clinical studies are essential to optimize colonization dynamics, regulatory compliance, and therapeutic payload efficacy.
5.4 Research Gap Highlighted Here:
"Engineered Bacteria: Few clinical trials; limited safety and efficacy data."
There is a pressing need for extensive clinical validation of engineered microbes, with long-term safety, efficacy, and host-microbiome interaction studies still underrepresented in dermatological research.
1. Limited Number of Clinical Trials
Despite promising preclinical data, there is a scarcity of clinical trials evaluating engineered bacteria for dermatological applications. Most studies are in early phases, with few progressing to Phase II or III. This limited clinical evidence hinders our understanding of the efficacy and safety of these therapies in diverse patient populations.
Example: A study involving the application of Staphylococcus hominis A9, a beneficial skin bacterium, showed a significant reduction in Staphylococcus aureus levels in eczema patients. While the results were promising, larger and more comprehensive trials are necessary to confirm these findings and assess long-term outcomes.
2. Insufficient Long-Term Safety Data
Long-term safety profiles of engineered bacterial therapies remain underexplored. Potential risks include unintended colonization, horizontal gene transfer, and immune reactions. For instance, while a case report demonstrated no adverse effects 17 months post-treatment with a photosynthetic scaffold for skin regeneration, such long-term follow-ups are rare. Comprehensive studies are needed to assess the persistence and systemic impacts of these therapies over extended periods.
3. Lack of Standardized Efficacy Endpoints
There is a need for standardized biomarkers and clinical endpoints to evaluate the efficacy of engineered bacterial treatments. Current studies often use varied metrics, making it challenging to compare results across trials. Establishing uniform criteria would facilitate more consistent assessments of therapeutic outcomes.
Example: In trials assessing the use of Roseomonas mucosa for atopic dermatitis, improvements were measured using different scales and patient-reported outcomes. The lack of standardized assessment tools makes it difficult to compare efficacy across studies and hinders the development of clear clinical guidelines.
4. Limited Understanding of Host–Microbiome Interactions
The interactions between engineered bacteria and the host's native microbiome are not fully understood. Factors such as colonization dynamics, competition with resident microbes, and immune responses can influence treatment efficacy and safety. Further research is necessary to elucidate these complex interactions and optimize therapeutic strategies.
Example: A study on the application of Staphylococcus epidermidis demonstrated its potential to inhibit S. aureus colonization through the production of antimicrobial peptides. However, the broader implications of introducing engineered strains into the existing skin microbiome ecosystem remain to be fully explored
About the Research Gap
Description
Why It Matters
Future Work to Address This Gap
1. Design and Conduct Rigorous Clinical Trials
2. Develop Standardized Protocols
3. Long-Term Safety Studies
4. Personalization Approaches
5.4.1 Data?sharing and Metadata Gaps Hindering Clinical Validation
Gap?Filling Proposal: Implementing Tier?Based Metadata Standards
1.Bronze: Provides accession IDs and basic MIxS core fields (e.g., sample name, collection date, geographic location) .
2.Silver: Includes recommended MixS checklist fields (e.g., sequencing method, primer sequences) and explicit Data Availability Statements clarifying access conditions .
3.Gold: Publishes raw FASTQ/BCL files alongside full processing scripts in public repositories (e.g., NCBI SRA, ENA) with no login or embargo requirements .
By embedding these tier?based metadata standards into the clinical?trial pipeline, dermatological research can ensure that every study contributes reusable, comparable, and trustworthy data—thereby accelerating the long?term safety and efficacy validation of engineered skin microbiome therapies.
6.The Role of Diet in Maintaining a Healthy Skin Microbiome
Diet plays a pivotal role in shaping the skin microbiome and, by extension, overall skin health. The connection between diet, gut health, and skin health is increasingly recognized through the concept of the "gut-skin axis," which describes how the gut microbiome communicates with the skin via immune, endocrine, and metabolic pathways. Dietary choices can influence inflammation, microbial diversity, and the skin's barrier function, all of which are crucial for maintaining a balanced and resilient skin microbiome.
A well-balanced diet rich in whole foods, antioxidants, fiber, and phytonutrients supports optimal skin health and helps prevent inflammatory skin conditions. Conversely, diets high in sugar, refined carbohydrates, and processed foods can fuel inflammation and disrupt the balance of both gut and skin microbiota, potentially leading to or exacerbating skin disorders such as acne, eczema, and psoriasis.
Nutritional Deficiencies and Excesses: Deficiencies in vitamins, minerals, and fatty acids, as well as excessive intake of unhealthy fats and sugars, can disrupt the skin’s balance and microbiome, manifesting in various skin problems.
Gut Microbiome Modulation: Dietary fibers and prebiotics promote the growth of beneficial gut bacteria, which in turn produce short-chain fatty acids (SCFAs). SCFAs have anti-inflammatory effects and can strengthen the skin barrier.
Direct Impact on Skin Microbiota: Certain nutrients and bioactive compounds can directly influence the composition and function of the skin microbiome, affecting immune responses and barrier integrity.
6.1. Foods that support a balanced skin microbiome
A variety of foods have been identified as particularly beneficial for supporting a healthy skin microbiome:
Benefits: These foods introduce beneficial bacteria (such as Lactobacillus and Bifidobacterium) into the gut, which can help reduce inflammation, improve skin barrier function, and decrease the incidence of skin conditions like acne and eczema.
Benefits: Prebiotics are non-digestible fibers that serve as food for beneficial gut and skin microbes. They help maintain microbial diversity and support the production of SCFAs, which have anti-inflammatory and barrier-strengthening effects.
Benefits: Polyphenols act as antioxidants, reducing oxidative stress and inflammation in the skin. They also modulate the composition of the microbiome, promoting the growth of beneficial bacteria.
Benefits: Omega-3s have strong anti-inflammatory properties and help maintain skin integrity, reduce redness, and support a balanced microbiome.
Avoidance of Processed Foods: Reducing intake of processed foods, excess sugars, and unhealthy fats can minimize inflammation and prevent the proliferation of pathogenic bacteria. A diet emphasizing probiotic and prebiotic foods, polyphenol-rich produce, and omega-3 fatty acids can significantly benefit the skin microbiome, supporting a healthy skin barrier, reducing inflammation, and preventing or alleviating dermatological conditions. Personalized dietary strategies, guided by healthcare professionals, are recommended to address individual needs and optimize skin health through microbiome modulation
7.Bacterial Products as Skincare Solutions
7.1. Antimicrobial peptides from bacteria
Several skin-resident bacterial species naturally produce antimicrobial peptides (AMPs) that enhance host defense and suppress pathogenic colonization. These bacterially-derived AMPs serve critical functions in maintaining microbial balance and protecting against opportunistic infections. Staphylococcus epidermidis, a dominant skin commensal, synthesizes phenol-soluble modulins (PSMs), which exhibit potent bactericidal activity against Staphylococcus aureus, thereby reducing its colonization and inflammatory potential . S. epidermidis also produces epidermin and other lantibiotics that modulate the skin microbiome and immune response. Cutibacterium acnes secretes short-chain fatty acids like propionic acid and CAMP factors, which not only exhibit antimicrobial effects but also contribute to immune modulation and tissue repair . Staphylococcus hominis produces bacteriocins, including sh-lantibiotics, that selectively inhibit S. aureus, making it a potential candidate for microbiome-based therapeutics in atopic dermatitis. Lactobacillus plantarum, often incorporated in probiotic formulations, generates bacteriocin-like peptides that suppress acne-associated C. acnes, reduce inflammation, and promote skin barrier integrity. These natural peptides from commensal microbes act synergistically with host-derived AMPs (e.g., LL-37, β-defensins), reinforcing the skin’s innate barrier against pathogens.
7.2. Bioactive compounds and their dermatological applications
7.2.1 The white?fleshed pitaya (Hylocereus undatus) extract investigated (IBR?Dragon™) is rich in both prebiotic polysaccharides and classic phytochemical antioxidants, which together confer a suite of skin?beneficial activities.
White?fleshed H. undatus contains a high concentration of oligosaccharides—namely raffinose, stachyose, maltopentaose, and maltotriose—that have been shown in vitro to selectively promote the growth of beneficial gut bacteria such as Bifidobacterium and Lactobacillus . When applied topically, these prebiotic sugars similarly foster commensal skin species (Staphylococcus epidermidis, S. hominis) while suppressing pathogens (S. aureus, Cutibacterium acnes) in a competitive coculture model, thereby rebalancing the microbial community toward a healthier state . Clinically, a 1% H. undatus cream increased Faith’s phylogenetic diversity index of facial skin microbiota by 13% versus placebo after 28 days—rising to +22% in volunteers over 45 years—indicating enhanced microbial richness and evenness .
Beyond oligosaccharides, the extract contains a suite of anti?inflammatory and antioxidant compounds, including betacyanin pigments, p?coumaric acid, vanillic acid, and gallic acid . These molecules scavenge reactive oxygen species in the epidermis, mitigating oxidative stress that otherwise drives inflammation and barrier degradation. Indeed, topical application of 1% H. undatus extract reduced clinical red spot counts by 35% at Day 28 (vs. placebo), lowered dermatologist?graded redness by 4%, and delayed histamine?induced microvascular response onset by 32%, demonstrating robust anti?inflammatory effects in vivo .
In streptozotocin?induced diabetic rats, the aqueous extract stimulated collagen synthesis—evidenced by elevated hydroxyproline and DNA content—and improved tissue tensile strength and epithelialization, hallmarks of accelerated wound healing . In human volunteers, transepidermal water loss (TEWL) decreased by 13% with the active formulation, indicating tighter barrier function and improved hydration retention . Mechanistically, phenolic acids like p?coumaric and gallic acid can upregulate keratinocyte filaggrin and ceramide production, further reinforcing stratum corneum integrity and preventing irritant penetration.
The antioxidant fraction also yielded measurable improvements in skin luminosity: ITA (Individual Typological Angle) increased by 11%, and L* (lightness) rose by 3% after 28 days of treatment, reflecting reduced pigmentation heterogeneity and a brighter complexion . In parallel, high?resolution PRIMOS imaging revealed an 11% reduction in wrinkle count and 5–7% decreases in wrinkle volume and length around the crow’s?feet, suggesting that antioxidant?driven protection of dermal collagen and elastin fibers can translate into visible anti?wrinkle effects .
Table 5: Summary of Key Bioactive and Their Actions
|
Compound Class |
Examples |
Dermatological Action |
|
Prebiotic oligosaccharide |
Raffinose, maltotriose,stachyose |
Supports commensal growth; rebalances dysbiosis |
|
Betalains |
Betacyanin pigments |
Potent antioxidant; anti-inflammatory |
|
Phenolic acids |
p-Coumaric, vanillic, gallic acids |
ROS scavenging; stimulates collagen and ceramide |
|
Collagen stimulators |
Hydroxyproline-elevating factors |
Promotes dermal matrix synthesis; accelerates healing |
Collectively, H. undatus extract’s blend of prebiotic sugars and phytochemical antioxidants offers a multifunctional approach: nurturing a resilient, diverse microbiome while directly protecting and rebuilding skin structure, making it a promising cosmeceutical for inflammation?prone, aging, and dysbiotic skin.
7.2.2Case Study – Sugarcane Straw Extract as a Prebiotic:
Carvalho et al. developed a 24?h aerobic in vitro model to screen cosmetic ingredients’ impact on skin microbiota. Their sugarcane straw extract—rich in phenolic acids and flavones—acted as a prebiotic: it preserved overall microbial diversity while shifting species ratios toward S. epidermidis (beneficial) over S. aureus (potentially pathogenic) . This selective modulation suggests its promise as a microbiome?friendly prebiotic in topical formulations.
7.2.3 Case Study – Vitreoscilla filiformis Extract as a Postbiotic Skincare Agent
Vitreoscilla filiformis, a gram-negative bacterium found in thermal spring water, has gained attention as a postbiotic ingredient in dermatology. Its non-viable lysate has been incorporated into various skincare formulations due to its immunomodulatory, anti-inflammatory, and microbiome-balancing properties. Mechanistically, V. filiformis extract stimulates innate immunity through modulation of Toll-like receptors (TLRs) and promotes the production of antimicrobial peptides such as cathelicidins and defensins. This activity supports the host’s defense system and reduces inflammatory cytokine production in skin conditions like atopic dermatitis (AD).
Clinically, topical formulations containing V. filiformis lysate have demonstrated:Reduction in Staphylococcus aureus colonization on eczematous skin. Improvements in barrier function, including increased ceramide synthesis and decreased transepidermal water loss (TEWL).Enhanced skin hydration and significant improvements in SCORAD and EASI scores. As a non-viable postbiotic, it offers several formulation advantages: heat stability, compatibility with diverse delivery systems (creams, emulsions, sprays), and a strong safety profile. Its dual action—targeting both immune modulation and microbial balance—makes it particularly valuable in treating dysbiosis-driven skin disorders. The success of V. filiformis extract illustrates how bacterial derivatives can bridge cosmetic and therapeutic functions, supporting the broader trend of microbiome-conscious skincare.
7.3 Probiotic and Postbiotic Formulations
7.3.1 Overview and Design Principles
1. Probiotic and postbiotic formulations are designed to support the skin barrier, improve hydration, and reduce inflammation.
2. Lactobacillus rhamnosus lysate has been shown in lab studies to strengthen skin structure by increasing proteins that hold skin cells together.
3. A topical application of fermented Lactobacillus helveticus improved skin moisture and reduced water loss in human skin.
4. Vitreoscilla filiformis lysate helps calm inflammation by encouraging anti-inflammatory signals from skin cells.
5. These approaches are directly relevant to earlier discussions on skin microbiome dysbiosis and loss of barrier integrity, offering targeted strategies to restore microbial and epidermal balance.
7.3.2 Delivery Challenges and Encapsulation Strategies
1. Live probiotics are delicate and can be damaged by heat, oxygen, and preservatives used in skincare products.
2. Freeze-drying is commonly used to preserve probiotics in powder form for stability.
3.Protective capsules made from natural gels (like alginate) help keep probiotics alive and effective in cosmetic creams.
4. Postbiotics do not require live cells, making them easier to formulate and more stable for regular use.
7.3.3 Applications and Product Types
1. Postbiotic creams like those containing LactoSporin (from Bacillus coagulans) have been shown to reduce acne lesions and sebum in clinical studies.
2. Lactobacillus plantarum lysate creams reduced acne symptoms in mild to moderate cases.
3. For sensitive skin, probiotic lotion blends (e.g., VHProbi® Mix R) improved skin hydration and reduced irritation over 28 days.
4. In eczema, topical probiotics have helped reduce redness, itching, and skin bacteria like Staphylococcus aureus.
5. A clinical trial by Sathikulpakdee et al. (2022) found that a lotion containing Lactobacillus paracasei supernatant significantly reduced acne lesion counts and redness, performing similarly to benzoyl peroxide but with fewer side effects.
6. In a study by Myles et al. (2020), topical use of Roseomonas mucosa in children with atopic dermatitis led to a 50% reduction in eczema severity and lowered S. aureus colonization, showing long-term skin improvement.
Table: 6 Treatment Modalities Targeting the Skin Microbiome
|
Treatment Modality |
Delivery Method |
Key Components
|
Applications
|
|
Probiotics
|
Topical application |
Live bacteria (Lactobacillus, Bifidobacterium) |
Atopic dermatitis, acne, pigmentation, repigmentation |
|
Prebiotics
|
Oral or topical |
Oligosaccharides (e.g., FOS, GOS) |
Microbial support, suppression of pathogens |
|
Postbiotics |
Topical application |
Lysates, bacteriocins, peptides |
Antioxidant effects, skin barrier support |
7.3.4 Regulatory and Safety Considerations
1. There are no specific regulations for probiotic cosmetics; products must meet general safety standards.
2. Live probiotic ingredients must be proven safe and free of harmful microbes, but postbiotic ingredients are generally easier to approve.
3. Clinical trials report that probiotic and postbiotic skincare is safe and well tolerated, with very few cases of minor irritation.
4. A systematic review by Salem et al. (2018) found that topical probiotics used in cosmetic formulations showed no major adverse effects in human studies, reinforcing their safety.
5. European Union cosmetic regulations require that any ingredient derived from microbial fermentation must meet strict microbial quality criteria to ensure it is non-pathogenic and non-toxic.
7.3.5 Clinical Validation and Future Directions
1. Studies have confirmed that probiotic and postbiotic products can improve hydration, strengthen the barrier, and reduce inflammation.
2. Larger and longer clinical trials are needed to confirm these benefits across broader populations.
3. Future trends include smart delivery systems (like microneedles or responsive hydrogels) and personalized skincare based on individual skin microbiomes.
4. With more scientific support and advanced formulation, probiotic and postbiotic skincare may become key tools in treating common skin concerns.
5. A 2021 study by Knackstedt et al. highlighted the potential of topical probiotics to reduce inflammation and restore microbial balance in chronic skin conditions like psoriasis and rosacea.
6. Innovations such as encapsulated live microbes, pH-responsive vesicles, and postbiotic-enriched creams are being tested in pilot trials, showing early promise for broader dermatologic applications.
7. As discussed in other parts of this review, aligning these microbial strategies with broader trends—such as microbiome-targeted therapies, biomarker-driven personalization, and sustainability in skincare—will help ensure long-term relevance and integration into mainstream dermatology.
8.Clinical Trials and Research in Skin Microbiome Therapies
Over the past three years, the U.S.?Food and Drug Administration has granted its first two approvals for microbiome?based live biotherapeutics—REBYOTA ( RBX2660 ), approved November 30?2022 for prevention of recurrent C.?difficile infection in adults U.S. Food and Drug AdministrationDrugs.com, and VOWST (SER?109), approved April 26?2023 as the first orally administered fecal?microbiota product for the same indication U.S. Food and Drug AdministrationDrugs.com. These landmark approvals underscore how microbiome?based diagnostics and therapeutics are moving rapidly from bench to bedside—and set the stage for analogous efforts in dermatology.
8.1. Advances in microbiome?based dermatology research
The number of registered clinical trials using live biotherapeutic products for skin conditions has grown significantly. Most are in early phases (I/II), targeting conditions like atopic dermatitis, acne, or chronic wounds. These trials use novel endpoints, including microbiome composition, cytokine levels, and lesion imaging, to evaluate both microbial and clinical responses. Compassionate-use studies under FDA Expanded Access protocols have also reported promising outcomes.
8.2. Current clinical trials on engineered bacteria for skin health
Several clinical trials have explored the use of engineered bacteria in treating skin conditions:
Phase 2/3:
9.Ethical and Regulatory Considerations
9.1. Challenges in the regulation of engineered bacteria
The application of engineered bacteria in dermatological therapy presents complex regulatory challenges. These products, often classified as engineered live biotherapeutic products (eLBPs), operate at the intersection of pharmaceuticals, biologics, and devices. As such, current regulatory frameworks are not yet fully equipped to address their unique characteristics—namely, their viability, potential for gene transfer, and interaction with the host microbiome. A significant barrier to clinical translation is the lack of standardized regulatory guidelines. Existing approval pathways for conventional drugs do not readily apply to living microorganisms engineered to deliver therapeutic agents in situ. Issues such as gene stability, microbial persistence, and environmental containment must be considered in regulatory assessments. There is also a need for harmonized potency assays and release criteria, particularly since the therapeutic efficacy of eLBPs can depend on contextual host-microbe interactions.
The manufacturing and quality control of engineered strains pose additional challenges. Ensuring reproducibility, batch consistency, and stability of engineered genetic constructs requires advanced bioprocessing techniques. Approaches such as continuous fermentation, lyophilization, and controlled environmental modulation (e.g., carbon source optimization) are being explored to improve yield and shelf life of eLBPs. Furthermore, defining clinical endpoints and standardized biomarkers for efficacy remains difficult due to the complex and dynamic nature of microbiome-host interactions. Studies such as those involving Staphylococcus hominis A9, Roseomonas mucosa, and Limosilactobacillus reuteri have demonstrated preliminary success, but regulatory bodies require more robust and standardized data to guide approvals. In light of these gaps, there is a pressing need for multidisciplinary collaboration involving microbiologists, dermatologists, regulatory scientists, and bioengineers to develop and validate regulatory frameworks tailored to engineered skin microbiome therapeutics.
9.2. Safety and ethical concerns in microbiome-based treatments
The therapeutic use of microbiome-based products, especially engineered strains, raises a spectrum of safety and ethical concerns. These include risks related to long-term colonization, horizontal gene transfer, and immune modulation. While early-phase trials report minimal adverse effects, comprehensive long-term safety data are scarce. One notable risk is unintended microbiome disruption. The introduction of engineered strains can alter native microbial communities, potentially leading to dysbiosis or resistance emergence. For instance, engineered Staphylococcus epidermidis strains used in melanoma models were effective in eliciting T cell responses but required strict control to avoid uncontrolled colonization or off-target immune effects. Another concern is the potential for immunogenic responses. Although strains like Roseomonas mucosa and Vitreoscilla filiformis have shown therapeutic benefits in atopic dermatitis without major adverse reactions, the variability in host immune responses necessitates personalized approaches and cautious monitoring. Ethically, the transparency of risk communication and informed consent is paramount. Patients should be clearly informed about the live and genetically modified nature of the treatments, including their possible persistence and interaction with host physiology. There is also an ethical imperative to ensure equitable access to microbiome therapies. As these treatments move toward personalization and commercial availability, cost and access disparities could exacerbate existing inequities in dermatological care. Moreover, data sharing and metadata standardization represent crucial ethical considerations. The lack of standardized, machine-readable metadata in microbiome research hampers reproducibility and clinical validation. Implementing structured data standards (e.g., the proposed Bronze/Silver/Gold metadata tiers) and enforcing FAIR principles is essential to build a trustworthy scientific foundation and accelerate safe clinical integration. In conclusion, addressing these safety and ethical challenges through rigorous monitoring, transparent regulation, and inclusive policy development is essential for responsible advancement in microbiome-based dermatology.
10.Future Directions and Challenges
10.1. Personalized microbiome-based skincare
Personalized microbiome-based skincare represents a transformative approach in dermatology that aligns with the principles of precision medicine—customizing treatments based on an individual's unique biological, genetic, and microbial profile. As our understanding of the human skin microbiome deepens, and as sequencing technologies become more accessible, personalized skincare is evolving from a theoretical concept into a tangible, science-driven practice.
The Foundation of Personalization: The Skin Microbiome
Each individual's skin harbors a distinct microbial signature, shaped by genetics, environment, hygiene practices, age, diet, geography, and immune status. This heterogeneity means that even common dermatological conditions, such as eczema, acne, or psoriasis, may have different microbial drivers and immune pathways across individuals. Personalized microbiome-based skincare seeks to:
Microbiome Profiling and AI Platforms
Next-generation sequencing techniques such as 16S rRNA and shotgun metagenomics allow high-resolution mapping of skin microbial communities. AI-powered platforms then analyze these complex datasets to create actionable insights.
These platforms recommend specific probiotic, prebiotic, or postbiotic ingredients designed to restore microbial balance and optimize skin health.
Therapeutic and Cosmetic Applications An increasing number of cosmetic and dermatological products are incorporating microbiome science:
* Microbiome-gentle cleansers
* Serums enriched with Lactobacillus lysates
* Postbiotic-infused facial masks
Brands like *L’Oréal* and *Codex Labs* are leading in funding research on microbial metabolites such as nitric oxide from ammonia-oxidizers, aiming to improve skin barrier function and reduce inflammation. Clinical-stage products, including *AOBiome’s Nitrosomonas eutropha spray*, are currently being tested in acne and eczema.
Synbiotic Formulations
Advanced products combine prebiotics (e.g., inulin) and engineered probiotics to enhance treatment efficacy. This synbiotic approach leverages prebiotics to support the colonization and activity of applied probiotics.
Multi-Omics Integration The integration of metagenomics and metabolomics enables predictive modeling that adjusts formulations in response to microbiome dynamics and host skin responses. These data-driven adjustments promise highly precise treatment personalization.
Engineered Bacteria: Precision Tools for Personalized Treatment
Genetically engineered microbes, or engineered live biotherapeutic products (eLBPs), offer powerful tools for personalized interventions:
Sensing and responding: Some engineered strains incorporate gene circuits that can detect skin inflammation (e.g., cytokines like IL-4 or TNF-α) and respond by producing therapeutic agents such as anti-inflammatory lipids or antimicrobial peptides.
Targeted delivery: These bacteria can be applied specifically to affected skin areas, colonize transiently, and exert localized effects without altering the broader microbiome.
Adjustability: Treatment formulations can be tailored to a patient’s microbiome type (e.g., high C. acnes levels in acne) or even gene expression signatures from skin swabs.
For example, Roseomonas mucosa strains applied topically in early-phase trials reduced eczema severity and S. aureus load specifically in patients whose microbiomes supported the engraftment of these strains. Similarly, strains engineered to inhibit C. acnes have shown promise in acne-prone individuals.
Diagnostics and Biomarkers for Personalization
To enable personalization, reliable microbiome diagnostics are essential. Advances in:
Emerging commercial tests can already provide consumers with microbiome-based skin assessments, though integration with clinical-grade diagnostics remains ongoing.
Personalized Formulations and Delivery Platforms
Microbiome-informed formulations are being developed as:
Challenges and Regulatory Considerations
Despite significant promise, key challenges remain:
* High interindividual variability across age, ethnicity, and skin type
* Limited long-term safety data on live engineered strains
* Lack of regulatory standards for live biotherapeutics
Regulatory frameworks must evolve to address safety, efficacy, and labeling standards for microbiome-based skincare. AI diagnostics and data transparency will be critical in substantiating personalized claims.
Future Prospects With ongoing advances in machine learning, biomarker discovery, and microbiome engineering, personalized microbiome-based skincare is poised to become a mainstay in dermatological care—offering precision prevention and targeted therapy for diverse skin conditions.
10.2. Overcoming hurdles in clinical translation
To advance the clinical application of engineered bacteria in dermatology, several challenges must be addressed:
1.Inter?individual variability: The high diversity of skin microbiomes across age, ethnicity, and body sites complicates patient stratification. Establishing robust microbial and immunological biomarkers will be critical to predict responders versus non?responders in trials
2. Bridging Preclinical and Clinical Research
Translating laboratory findings into clinical practice requires well-designed trials that incorporate standardized endpoints and consider the complexities of human skin microbiota. Collaborative efforts between researchers and clinicians are essential to design studies that accurately reflect clinical scenarios.
Example: The development of Staphylococcus epidermidis-based therapies has shown promise in preclinical models, but translating these findings into human trials necessitates careful consideration of dosing, delivery methods, and patient selection.
3. Establishing Long-Term Monitoring Frameworks
Implementing long-term surveillance systems is crucial to monitor the persistence of engineered bacteria, potential adverse effects, and overall treatment outcomes. Such frameworks would provide valuable data on the durability and safety of these therapies. Long?term safety monitoring: As engineered strains colonize or transiently persist on the skin, post?marketing surveillance must include sequencing?based tracking of horizontal gene transfer and off?target effects on native microbiota. Integrating real?world evidence registries and digital health platforms can facilitate longitudinal safety data collection
Example: Longitudinal studies tracking patients treated with Roseomonas mucosa for atopic dermatitis could offer insights into the long-term colonization patterns and any delayed adverse events.
4. Clarifying Regulatory Pathways
Regulatory guidelines for live biotherapeutic products, including engineered bacteria, need to be clearly defined. This includes establishing safety thresholds, manufacturing standards, and approval processes to ensure patient safety and product efficacy. Regulatory frameworks: Live microbial therapeutics straddle biologics and drug-device categories. Harmonized guidelines—defining potency assays, release criteria, and environmental risk assessments—are urgently needed from agencies such as the FDA and EMA to streamline IND/CTA pathways.
Example: The development of ammonia-oxidizing bacteria-based treatments like B244 highlights the need for regulatory frameworks that address the unique challenges posed by live microbial therapies.
5. Fostering Multidisciplinary Collaborations
6.Manufacturing and formulation: Scaling up production of viable, uniformly engineered strains under GMP conditions remains challenging. Advances in continuous fermentation, automated cell banking, and lyophilization protocols will help ensure lot?to?lot consistency and shelf stability By addressing these research gaps and challenges, the field can move closer to integrating engineered bacterial therapies into standard dermatological practice, offering novel solutions for skin health management.
11.CONCLUSION
11.1. Summary of key findings
The skin microbiome represents a rapidly evolving frontier in dermatology, bridging foundational microbiological science with cutting-edge therapeutic innovation. Through this review, we have analyzed the composition, variation, and functions of the skin microbiome, especially how intrinsic and extrinsic factors—such as age, hygiene, climate, and diet—modulate microbial diversity. Site-specific and familial studies, including data from Indian populations, underscore the nuanced influences of genetics and cohabitation on microbial profiles. We have interpreted the roles of commensal microbes in maintaining skin barrier integrity, immune homeostasis, wound repair, and environmental adaptation. Dysbiosis has been linked to a range of conditions, including atopic dermatitis, acne, psoriasis, and chronic wounds, where microbial imbalance worsens inflammation and impairs healing. Clinical findings and mechanistic studies converge to support the therapeutic promise of microbiome-targeted interventions. Better Tools for Studying the Microbiome-New research techniques—like long-read DNA sequencing and refined contamination controls—allow scientists to more accurately map out skin bacteria, even those present in very small amounts but that play important roles. Triple biotic strategies—integrating prebiotics, probiotics, and postbiotics—emerge as a compelling formulation paradigm. Clinical trials of triple biotic serums show improvements in hydration, microbial diversity, and skin barrier repair, especially in sensitive and dry skin. However, data heterogeneity and lack of standardization in formulation and outcomes remain key limitations. Simultaneously, engineered bacteria and live biotherapeutic products have opened a new era of precision dermatology. These innovations enable targeted antimicrobial peptide production, immune modulation, and even tumor-targeted therapies. Applications span from chronic inflammatory skin disorders to advanced wound healing and melanoma. Despite their promise, long-term safety, host-microbe interaction dynamics, and regulatory clarity remain underexplored. Moving forward, integration of triple biotic approaches with engineered microbial solutions offers a multi-pronged, synergistic pathway to restore skin homeostasis. Realizing this potential will require interdisciplinary collaboration across dermatology, synthetic biology, regulatory science, and patient-centered clinical research. Standardized endpoints, FAIR-compliant data sharing, and safety frameworks will be essential to translate these findings into widely accepted, effective dermatological care. In conclusion, microbiome-based skincare—rooted in ecological, clinical, and technological insights—holds transformative potential for future dermatology. With thoughtful refinement, rigorous validation, and strategic integration, the skin microbiome may transition from passive inhabitant to active therapeutic ally in personalized skin health.
11.2. Recommendations for future research
Further research should explore how engineered or native microbes influence immune function, barrier repair, and skin–brain signaling.
REFERENCES

Minal Chetule*, Atul Pawar, Komal Mule, Dr. Shivshankar Mhaske, The Skin Microbiome: Its role in Health and Disease, including Dysbiosis leading to Dermatological Conditions and Engineered bacteria and Skincare solutions for Dermatological Application, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 5160-5204. https://doi.org/10.5281/zenodo.15561462
 10.5281/zenodo.15561462
10.5281/zenodo.15561462