
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Shree Venkateshwara College of Paramedical Sciences, College of Pharmacy, Erode, Tamilnadu, The Tamilnadu Dr. M.G.R Medical University.
Hypertension remains one of the most common and serious global health problems, contributing significantly to cardiovascular and kidney diseases. Although several classes of antihypertensive drugs are available, many patients struggle with poor adherence and treatment resistance, making long-term blood pressure control difficult. Zilebesiran, a novel small interfering RNA (siRNA) therapy, offers a promising alternative by specifically targeting hepatic angiotensinogen (AGT), a key component of the renin-angiotensin-aldosterone system (RAAS). Using N-acetylgalactosamine (GalNAc) conjugation, zilebesiran achieves targeted delivery to hepatocytes, leading to sustained suppression of AGT production. Clinical studies have shown that a single subcutaneous injection can reduce both systolic and diastolic blood pressure for up to six months, with an encouraging safety profile. This infrequent dosing schedule may overcome adherence issues associated with daily oral medications, positioning zilebesiran as a potential breakthrough in the management of hypertension.
Hypertension, often called the "silent killer," is a major risk factor for cardiovascular and kidney diseases, including strokes, heart disease, and chronic kidney failure. According to the World Health Organization (WHO) fact sheet (2023), an estimated 1.28 billion people worldwide, aged 30 to 79, are affected by hypertension, with nearly two-thirds of them residing in low- and middle-income countries. The likelihood of developing hypertension increases with age, high salt intake, obesity, lack of physical activity, and heavy alcohol consumption. The primary treatment for hypertension involves lifestyle changes and oral medications, such as ACE inhibitors, ARBs, calcium channel blockers, diuretics, and beta-blockers. Despite the wide range of available treatments, only about 21% of patients manage to control their blood pressure effectively. Various factors contribute to poor blood pressure management, such as incorrect dosages and poor adherence to medication. Common reasons for non-adherence include medication side effects like fatigue, dizziness, sexual dysfunction in men, the complexity of dosing regimens, polypharmacy, and strained patient-provider relationships. These challenges highlight the need for new medications that are easier to use, require less frequent dosing, and can be combined with current antihypertensive treatments. A promising new strategy is to target liver-derived angiotensinogen (AGT) to regulate blood pressure by silencing its production. Zilebesiran, an experimental RNA interference drug delivered via injection, binds to the liver’s asialoglycoprotein receptor to lower AGT messenger RNA (mRNA) levels. This results in reduced AGT levels in the bloodstream, helping to lower blood pressure through modulation of the renin-angiotensin-aldosterone system (RAAS). This method offers several potential benefits over traditional treatments. First, modulating RAAS at the liver level may provide better kidney safety. Second, directly targeting AGT could be more effective than inhibiting angiotensin-converting enzymes or angiotensin receptors. Finally, Zilebesiran can be administered via subcutaneous injection every three to six months, potentiallysolving the problem of medication non-adherence often seen with oral treatments. Managing hypertension typically starts with lifestyle changes, such as losing weight, following a diet that’s low in sodium and high in potassium, staying physically active, and either reducing or stopping alcohol intake. These adjustments can help lower blood pressure initially and work in tandem with medications to boost their effectiveness. However, some common side effects from medications can make it challenging for patients to stick with their treatment. For example, calcium channel blockers (CCBs) can cause frequent urination and headaches, diuretics may lead to excessive urination and dizziness, and ACE inhibitors can trigger a dry, irritating cough. These side effects often result in patients stopping their treatment and switching to alternatives.
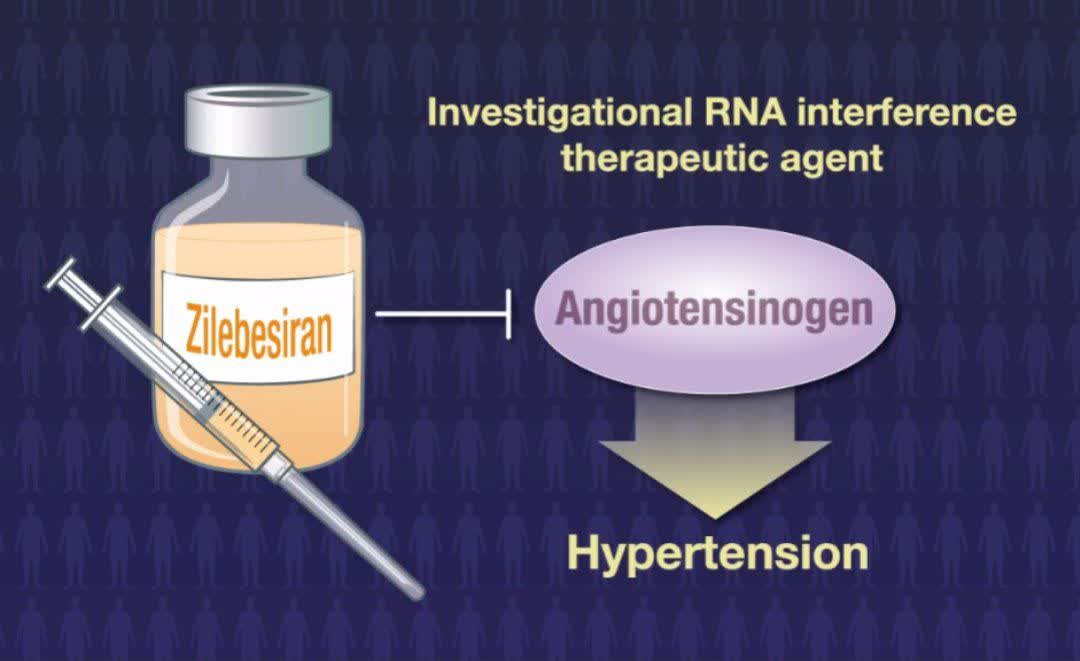
Fig: 1
Table:1
|
AGT |
Angiotensinogen |
|
Ang II |
angiotensin II |
|
ACE |
angiotensin-converting enzyme |
|
BP |
blood pressure |
|
CVD |
cardiovascular disease |
|
GalNAc |
N-acetylgalactosamine |
|
RAS |
renin-angiotensin system |
|
RISC |
RNA-induced silencing complex |
|
RNAi |
RNA interference |
|
SBP |
systolic blood pressure |
|
siRNA |
small-interfering RNA |
Zilebesiran
SiRNA (small interfering RNA) represents a groundbreaking approach in drug development, offering a highly targeted method to regulate protein production. This technology is part of the RNA interference (RNAi) field, which is revolutionizing how we think about gene silencing in medicine. One of the most promising developments in siRNA therapeutics is zilebesiran, a novel treatment that stands out for its potential in managing hypertension. Zilebesiran is a first-of-its-kind siRNA, working by targeting the hepatic asialoglycoprotein receptor. This triggers a series of molecular events that lead to the reduction of angiotensinogen (AGT) messenger RNA. As a result, the liver produces less AGT, which in turn lowers the levels of both angiotensin I and II, key contributors to high blood pressure. The ability of zilebesiran to specifically modulate the synthesis of AGT makes it an exciting new option in the fight against hypertension. The success of siRNA therapies has been marked by significant milestones, with several treatments already approved by the FDA. Drugs like patisiran, givosiran, lumasiran, and inclisiran have demonstrated the power of RNAi in treating various conditions, from rare genetic disorders to cardiovascular diseases. In this evolving landscape, zilebesiran emerges as a strong candidate, offering a subcutaneous treatment that targets the root cause of hypertension by adjusting AGT production. Overall, zilebesiran highlights the immense potential of siRNA technology in transforming therapeutic strategies. It’s a prime example of how precision medicine can directly address the molecular drivers of disease, offering a new, more effective way to manage hypertension and possibly other conditions in the future.
Subcutaneous Administration of Zilebesiran
The subcutaneous (SC) route is one of the methods used for delivering Zilebesiran. The subcutaneous injection route means the drug is administered into the layer of fat and tissue just under the skin, making it easier to self-administer or be given in outpatient settings.
Benefits of SC Administration
The subcutaneous route offers a more convenient method for patients, as it avoids the need for intravenous administration, which can be more invasive and time-consuming.
Zilebesiran is typically administered as a subcutaneous injection at intervals (e.g., every 3 to 6 months) for continuous effect. The sustained action is a significant advantage for patients requiring long-term treatment.
Depending on clinical trials, patients might be able to administer Zilebesiran at home after proper training, which would increase patient convenience and adherence to therapy.
After subcutaneous administration, Zilebesiran is absorbed into the bloodstream, where it exerts its therapeutic effects on liver cells. It is designed for long-lasting suppression of the target gene, which reduces the need for frequent injections.
As with many drugs administered via the subcutaneous route, local reactions such as redness, swelling, or pain at the injection site may occur. There can also be systemic side effects such as fatigue or headaches, though these tend to be mild.
Table:2
|
Title |
Main Findings |
|
Targeting angiotensinogen with Nacetylgalactosamine- conjugated small interfering RNA to reduce blood pressure. |
|
|
|
|
|
|
|
|
|
|
|

Fig:2
Zilebesiran is an experimental RNA-based therapy that targets a specific gene in the liver, called hepatic AGT mRNA, to block the production of the AGT protein. In a Phase 1 clinical trial, which was randomized, double-blind, and placebo-controlled, researchers looked at how zilebesiran affected various factors such as pharmacokinetics, pharmacodynamics, and overall safety. The trial also specifically measured its impact on blood pressure (BP). Patients in the study received either a single subcutaneous dose of zilebesiran (ranging from 10 to 800 mg) or a placebo. Results showed that zilebesiran reduced serum AGT levels in a dose-dependent manner. More importantly, doses of 200 mg or higher resulted in significant reductions in both systolic (over 10 mmHg) and diastolic (over 5 mmHg) blood pressure by week 8, with these effects lasting for up to 24 weeks. This BP reduction was consistent throughout the 24-hour daily cycle. However, when patients were on a high-sodium diet, the BP-lowering effect of zilebesiran was less pronounced. On the other hand, when zilebesiran was taken along with the drug irbesartan, there was a significant additional drop in both systolic (−63 ± 31 mmHg) and diastolic (−3 ± 19 mmHg) blood pressure. These Phase 1 results strongly suggest that targeting liver AGT with RNA interference (RNAi) could be a promising strategy for reducing blood pressure (by 20–25 mmHg). Additionally, zilebesiran doses up to 800 mg were generally well tolerated, with no signs of hypotension, hyperkalemia, or worsening kidney function. The drug demonstrated a long-lasting effect, maintaining its ability to reduce both AGT levels and blood pressure for up to 24 weeks after a single dose. The Phase 2 KARDIA-1 trial (NCT04936035) was a randomized, double-blind, multicenter, placebo-controlled study that evaluated the safety and effectiveness of zilebesiran in people with mild-to-moderate hypertension. The results showed that zilebesiran, when given as a subcutaneous injection either quarterly or every six months, consistently lowered blood pressure and maintained its pharmacodynamic effects over time. Patients receiving 300 mg or 600 mg doses saw significant and sustained blood pressure reductions (on average 10–15 mmHg), with some experiencing reductions of up to 25 mmHg. Remarkably, these effects lasted up to six months after just a single dose. Side effects were generally mild to moderate, with the most common being injection site reactions and occasional cases of hyperkalemia. These findings build on the earlier Phase 1 data and further support zilebesiran's potential as a long-acting therapy for hypertension. Another ongoing trial, the Phase 2 KARDIA-2 study (NCT05103332), is exploring zilebesiran’s role as an add-on therapy for patients whose high blood pressure remains uncontrolled despite being on standard antihypertensive medications. This study is expected to finish by 2025. One of zilebesiran’s most promising features is its infrequent dosing schedule, which could help improve patient adherence compared to daily blood pressure medications. Unlike traditional RAAS blockers, which can show variability in effect depending on daily use, zilebesiran provides a consistent and long-lasting inhibition. Additionally, a growing body of evidence from both clinical and preclinical research supports that GalNAc-siRNA therapies, like zilebesiran, have a strong safety profile and a wide therapeutic window when targeting the liver. The KARDIA-1 Phase 2 trial included 394 patients with mild-to-moderate hypertension, who received subcutaneous injections of zilebesiran at doses of 150 mg, 300 mg, or 600 mg, either quarterly (every 3 months) or biannually (every 6 months). The results showed significant reductions in 24-hour average systolic blood pressure (SBP) across all dosing groups.
At 3 months, the placebo-adjusted SBP reductions were:
These reductions were largely maintained through month 6, ranging from 11.1 mmHg to 14.5 mmHg, indicating durable and sustained blood pressure control. Office blood pressure readings supported these findings, further validating zilebesiran's consistent antihypertensive effect. Achieving this level of sustained control with just two or four injections per year marks a major improvement over traditional treatments that require daily dosing. In terms of safety, zilebesiran was well tolerated. The overall rate of adverse events (AEs) was similar between the zilebesiran and placebo groups. Common AEs included injection site reactions, hyperkalemia, and upper respiratory infections. Serious adverse events (SAEs) occurred in 3.6% of patients receiving zilebesiran, compared to 6.7% in the placebo group, and none of the SAEs were attributed to the drug itself. Zilebesiran’s biannual dosing schedule not only simplifies hypertension treatment but also helps address major limitations of current therapies—particularly poor patient adherence and fluctuating blood pressure control. It may also reduce the risk of RAAS escape, a phenomenon commonly seen with ACE inhibitors and ARBs.
Focus on AGT
AGT is mainly produced by the liver and acts as the only precursor for all angiotensin peptides. Thus, blocking AGT production in the liver may offer an effective approach to treating hypertension by reducing or possibly stopping the formation of the potent vasoconstrictorAng-II.
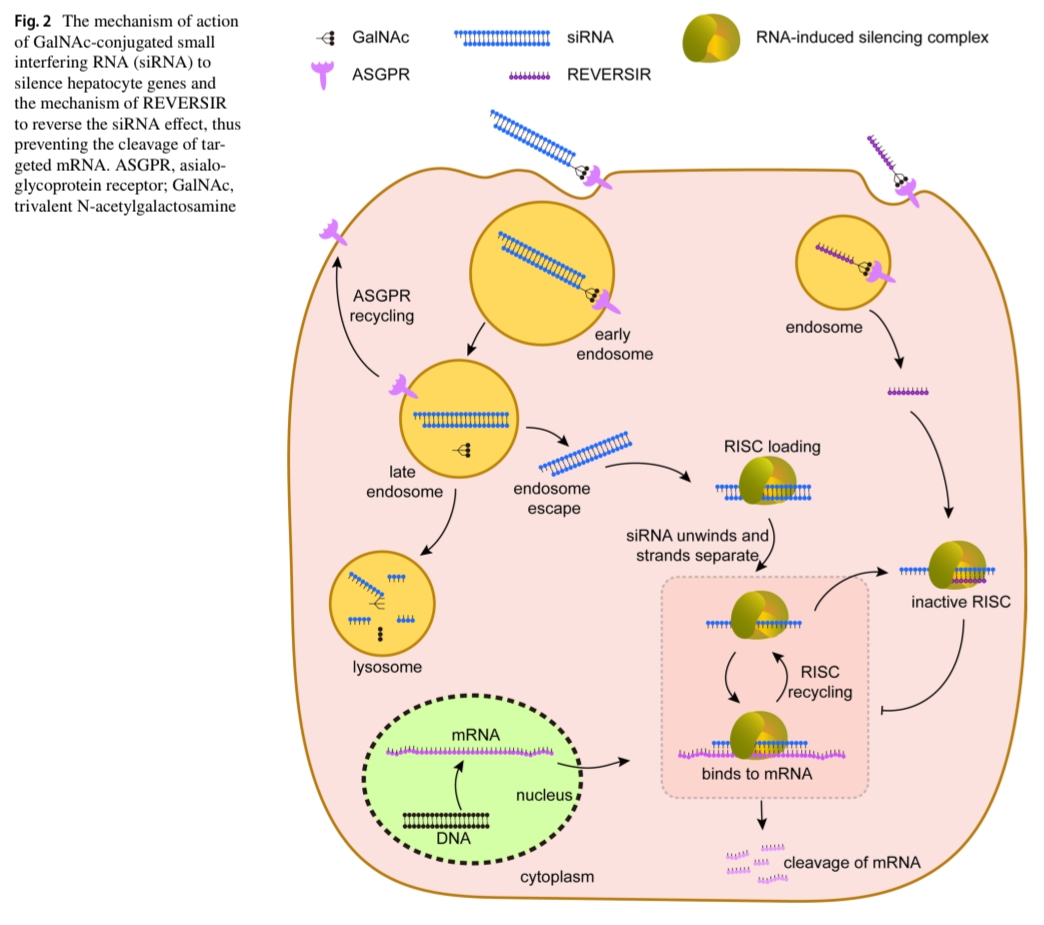
Fig:3
The mechanism of action of GalAc-conjugated small interfering RNA (siRNA) to silence hepatocyte genes and the siRNA effect, thus preventing the cleavage of targeted mRNA . ASGPR, asialogycoprotein receptor;GalNAc, trivalent N-actelgalactosamine.
Mechanism Of Action
Zilebesiran is a novel small interfering RNA (siRNA) therapeutic designed to target hypertension by silencing the gene responsible for producing angiotensinogen (AGT), a key precursor in the renin-angiotensin-aldosterone system (RAAS). The figure illustrates the intracellular mechanism of GalNAc-conjugated siRNA delivery and gene silencing in hepatocytes (liver cells), where AGT is primarily synthesized. The process begins with zilebesiran being chemically conjugated to N-acetylgalactosamine (GalNAc), a sugar molecule that specifically binds to asialoglycoprotein receptors (ASGPR) on the surface of hepatocytes. This targeted delivery system ensures high uptake in the liver while minimizing off-target effects elsewhere in the body. Once the GalNAc-siRNA complex binds to the ASGPR, it is internalized into the cell via receptor-mediated endocytosis, forming an intracellular vesicle called an early endosome. Inside the cell, the ASGPR is quickly recycled back to the cell surface to mediate further uptake. Meanwhile, the endosome matures into a late endosome, and some of the siRNA may be lost to lysosomal degradation. However, a significant portion of the siRNA escapes from the endosomal compartment into the cytoplasm, a crucial step for its gene-silencing action. This step is known as endosomal escape, and it allows the siRNA to access the molecular machinery required for RNA interference. Once in the cytoplasm, the siRNA is incorporated into a protein complex known as the RNA-induced silencing complex (RISC). During this process, the siRNA duplex unwinds, and the passenger strand is discarded, leaving the guide strand attached to the RISC. The guide strand is complementary to the specific target mRNA—in this case, angiotensinogen mRNA (AGT mRNA). The active RISC complex then scans the cytoplasm for matching mRNA sequences. Upon finding its target, the guide strand binds to AGT mRNA, allowing RISC to cleave the mRNA strand. This cleavage prevents translation of the mRNA into protein, effectively silencing gene expression. This degradation of AGT mRNA leads to a reduction in angiotensinogen protein levels, thereby limiting the downstream production of angiotensin I and II. Since angiotensin II is a potent vasoconstrictor and stimulator of aldosterone release, its reduction leads to vasodilation, decreased sodium and water retention, and overall lower blood pressure. Notably, the RISC complex can be recycled multiple times, continuing to degrade newly formed mRNA molecules. This prolonged activity results in sustained gene silencing, allowing zilebesiran to have a long-lasting antihypertensive effect with potentially quarterly or biannual dosing, which is a significant improvement over daily oral antihypertensive medications. The diagram also shows another siRNA-like molecule labeled Reversir, which is likely included for experimental control or to illustrate a reversible mechanism, though it is not directly involved in zilebesiran's function. Importantly, this entire process represents an example of RNA interference (RNAi)—a natural cellular mechanism that has been harnessed for therapeutic purposes. Zilebesiran is one of the first agents to utilize this platform for cardiovascular diseases, demonstrating the potential of gene-silencing therapies to offer precision, potency, and durable clinical effects.
Pharmacokinetics And Pharmacodynamics
Pharmacokinetics
Zilebesiran is designed to work specifically in the liver over a long period. After a subcutaneous injection, the siRNA quickly reaches peak levels in the blood before being efficiently taken up by liver cells. Normally, unmodified siRNA breaks down very fast—in just minutes—because of enzymes called nucleases. But zilebesiran uses special chemical modifications to stay stable longer. Plus, the attached GalNAc molecule helps deliver most of the drug straight to the liver, keeping overall body exposure low. In a phase 1 study, the drug showed dose-proportional pharmacokinetics between 10 and 800 mg, meaning higher doses led to predictably higher levels in the blood and liver without unexpected buildup. What’s more, when two 800 mg doses were given 12 weeks apart in obese patients, the drug’s behavior and effects stayed consistent, suggesting repeat dosing doesn’t change how the body handles it, regardless of body size.
Pharmacodynamics
The key effect of zilebesiran is a strong and lasting reduction in circulating angiotensinogen, which leads to lower blood pressure. In phase 1 trials, doses of 100 mg or more cut angiotensinogen levels by over 90% within weeks, and this suppression lasted from week 3 all the way to week 12 after a single dose. At the highest dose tested (800 mg), this suppression lasted for at least 24 weeks. This long-lasting effect happens because the siRNA stays inside liver cells for a long time, continuously blocking angiotensinogen production. Zilebesiran also affects other parts of the RAAS system. At doses of 200 mg and above, small decreases in plasma renin activity, angiotensin I and II, and aldosterone were seen, showing that the system downstream is also being inhibited. Interestingly, even though plasma renin concentration might increase because angiotensin II’s feedback is lost, the overall production of angiotensin stays low due to angiotensinogen depletion. When it comes to blood pressure, the drop corresponds well with how much angiotensinogen is silenced. Higher doses in the phase 1 study showed bigger reductions in 24-hour ambulatory blood pressure. There was a clear inverse relationship between the dose and systolic blood pressure change—meaning higher doses led to bigger falls in systolic pressure. Patients receiving 200 mg or more saw meaningful decreases by 8 weeks—over 10 mm Hg systolic and 5 mm Hg diastolic on average. These effects began within 2 to 4 weeks and stayed steady at 12 and 24 weeks. For example, 8 patients who got 800 mg experienced an average systolic drop of about 22.5 mm Hg and a diastolic drop of around 10.8 mm Hg at 24 weeks, highlighting the drug’s long-lasting effect. One interesting aspect is how zilebesiran’s effect on blood pressure interacts with salt intake and other RAAS drugs. In a controlled study, a high-salt diet significantly weakened zilebesiran’s blood pressure-lowering effect, while a low-salt diet made it stronger. This fits with what we know about hypertension—high salt expands blood volume and can counteract RAAS suppression. On the other hand, when zilebesiran was combined with an ARB (irbesartan), blood pressure dropped even more than with zilebesiran alone, showing they can work together effectively by blocking the RAAS at different points. These findings suggest that patients taking zilebesiran should keep their salt intake low for the best results, and combining it with other RAAS blockers could safely enhance the blood pressure-lowering effect.
Phase 1 Trials
The first human study of zilebesiran was conducted by Desai and colleagues in a multi-part phase 1 trial. In Part A, 84 patients with mild to moderate high blood pressure (average systolic around 139 mm Hg) were randomly assigned in a 2:1 ratio to receive a single subcutaneous injection of zilebesiran—doses ranged from 10 mg up to 800 mg—or a placebo, with 56 patients receiving the drug and 28 getting placebo. They were followed for 24 weeks. Parts B and E focused on specific conditions: Part B tested the effects of an 800 mg dose under low- versus high-salt diets, while Part E looked at what happened when the 800 mg dose was given alongside the ARB drug irbesartan. The main goals were to assess safety and tolerability, but researchers also tracked how well the drug lowered angiotensinogen levels, its pharmacokinetics, and blood pressure changes. The results were promising. Zilebesiran showed a clear dose-dependent effect, significantly lowering blood pressure at doses of 200 mg and above. By 8 weeks after just one dose of 200 mg or more, 24-hour ambulatory systolic blood pressure dropped by over 10 mm Hg on average, and diastolic pressure fell by more than 5 mm Hg. These reductions lasted throughout the 24-week follow-up, showing the drug’s long-lasting action from a single injection. At the highest dose of 800 mg, average drops in systolic and diastolic pressure were about 22.5 mm Hg and 10.8 mm Hg, respectively, at 6 months. Importantly, the blood pressure lowering effect was steady throughout the day and night, including early morning hours, suggesting good round-the-clock control. The salt study in Part B confirmed that a high-salt diet weakened the drug’s effect—blood pressure returned to baseline despite treatment when salt intake was high—highlighting the importance of lifestyle changes like reducing sodium intake. Part E showed that combining zilebesiran with irbesartan resulted in an even bigger blood pressure drop than zilebesiran alone, indicating that these two drugs can work well together. Overall, these phase 1 results provided solid proof-of-concept that targeting angiotensinogen with siRNA is a safe and effective way to lower blood pressure for several months after just one dose.
Phase 2 Trials
Building on the promising results from phase 1, larger phase 2 studies have been carried out to fine-tune dosing and test how well zilebesiran works in a broader range of patients. One key study, the EKG Anywhere Anytime (KARDIA)-1 trial led by Bakris and colleagues, was a randomized, double-blind, placebo-controlled trial involving 394 adults with mild to moderate hypertension. Patients stopped taking their previous blood pressure medications and were randomly assigned to receive different dosing schedules of subcutaneous zilebesiran or a placebo. The doses tested included 150 mg every six months, 300 mg every six months, 300 mg every three months, and 600 mg every six months. The main goal was to measure the change in average 24-hour systolic blood pressure after three months, using ambulatory blood pressure monitoring. The results of KARDIA-1 clearly showed that zilebesiran significantly lowered blood pressure at all effective dose levels. After three months, patients treated with zilebesiran had strong reductions in their 24-hour systolic BP compared to the placebo group, which actually saw a slight increase in blood pressure. The average reductions compared to placebo were about 14.1 mm Hg for 150 mg every six months, 16.7 mm Hg for the 300 mg doses (pooled across the three- and six-month schedules), and 15.7 mm Hg for 600 mg every six months—all highly significant results. These blood pressure drops are comparable to what you’d expect from a standard blood pressure medication, showing that zilebesiran on its own can effectively lower blood pressure. Importantly, the blood pressure-lowering effect lasted throughout the six-month dosing interval, with blood pressure still reduced at the six-month mark in the treated groups. Most patients receiving zilebesiran reached their target blood pressure during the trial, while those on placebo, who had stopped their prior meds, experienced rising blood pressure. Several other phase 2 trials are currently underway to build on these findings. The KARDIA-2 study is looking at how zilebesiran works when combined with usual blood pressure medications in a larger group of over 600 patients. This trial will help determine whether zilebesiran can add to or even replace some of the conventional drug classes like diuretics, ACE inhibitors, ARBs, or calcium channel blockers. Another trial, KARDIA-3, focuses on patients with uncontrolled hypertension who are at high cardiovascular risk and already taking multiple blood pressure drugs. In this study, zilebesiran is being tested as an add-on to 2–4 existing medications in nearly 400 patients, aiming to improve blood pressure control in those with resistant hypertension. Together, these phase 2 studies will give a clearer picture of how best to use zilebesiran in clinical practice—whether as a stand-alone treatment for patients who can’t control their blood pressure or tolerate standard drugs, or as part of a combination therapy in those with hard-to-treat hypertension.
Table:3
|
Study |
Overview of protocol |
|
KARDIA-1 |
Evaluated zilebesiran monotherapy in people with mild to moderate hypertension. Met primary endpoint. |
|
KARDIA-2 |
Evaluated zilebesiran when added to a standard of care hypertension medication in people with mild to moderate hypertension. Met primary endpoint. |
|
KARDIA-3 |
Designed to evaluated zilebesiran when added to two or more hypertension medications in people with uncontrolled hypertension at high cardiovascular risk. |
Summary

Fig:4
Safety Aspects of Angiotensinogen siRNA
Zilebesiran represents a completely new class of RAS blockers, so it’s crucial to carefully study its side effects before it becomes widely available. Right now, the closest comparison might be inclisiran, which also uses the GalNAc delivery system. However, inclisiran targets a different protein in liver cells — proprotein convertase subtilisin/kexin type 9 — rather than angiotensinogen. Like zilebesiran, a single subcutaneous injection of inclisiran lasts for six months and has been shown to reduce LDL cholesterol by about 50%. So far, the main side effect reported has been injection-site reactions, occurring in 3–5% of trial participants. Importantly, no liver toxicity or immune-related side effects have been observed, suggesting that accumulating siRNA in the liver isn’t inherently harmful. Similarly, the KARDIA-1 study of zilebesiran reported no serious liver problems. The most common mild side effects were temporary low blood pressure (in 4% of patients), elevated potassium levels (6%), and injection-site reactions (6%). It’s well known that too much RAS inhibition can cause issues like hypotension, kidney problems, and hyperkalemia, especially when combining more than one RAS blocker. This is because normal kidney function — particularly the filtration process — depends on some level of RAS activity. Ongoing KARDIA trials with more participants should provide further insights. It’s clear that completely blocking angiotensinogen isn’t ideal. Also, strong RAS inhibition has been linked to thickening of the kidney’s small arteries and arterioles, caused by the growth of immature matrix-producing renin cells and abnormal smooth muscle cell buildup. Recent animal studies show that this effect also occurs with angiotensinogen siRNA treatment, but reassuringly, it’s similar to what’s seen with ACE inhibitors and AT1 receptor blockers. One more concern with angiotensinogen siRNA is its long-lasting effect. While this helps with treatment adherence, it could become problematic if the RAS suddenly needs to activate — like during sepsis or heavy bleeding, when blood pressure must be maintained, or during pregnancy, where the RAS plays a key role in blood flow changes. In animal studies with rats on low-salt diets, angiotensinogen siRNA strongly lowered blood pressure, but giving Ang II or norepinephrine injections could still raise it acutely. When rats were on a high-salt diet plus fludrocortisone, their blood pressure returned to normal over several days. A clever solution to this problem is a method called REVERSIR, which can reverse the gene-silencing effect caused by siRNA. REVERSIR uses synthetic single-stranded oligonucleotides that bind to the siRNA guide strand inside liver cells, blocking its activity and allowing the targeted protein to be produced again. Using REVERSIR on angiotensinogen siRNA-treated rats, researchers observed a dose-dependent return of angiotensinogen levels within a few days, along with blood pressure returning to baseline. Interestingly, even when angiotensinogen increased by only 50%, blood pressure normalized. This was likely because renin levels remained elevated, helping produce enough Ang II to maintain normal pressure. This suggests that even partial restoration of angiotensinogen could help patients quickly raise their blood pressure when needed.
Side effects
CONCLUSION
Zilebesiran is a novel siRNA therapy for hypertension that works by targeting the hepatic asialoglycoprotein receptor to reduce angiotensinogen (AGT) production in the liver, thereby lowering angiotensin I and II levels. It represents a major advancement in RNA interference–based medicine, similar to other FDA-approved siRNA drugs like patisiran and inclisiran. Administered subcutaneously into the fat layer under the skin, it offers a convenient, targeted approach to controlling high blood pressure and exemplifies the potential of precision medicine.
REFERENCES










T Mounika K.*, Dr. K. B. Ilango, Arumugam S., Kanishka Sre S., Srinivasan K., Subashini M., Vishnu Ganesh Kumar B., Dinesh V., Jothika S., Kolandhasamy S., Suriya S., Venkatrama Kishan S. S., Zilebesiran for Hypertension Treatment: An Overview, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 2210-2224 https://doi.org/10.5281/zenodo.17164005
 10.5281/zenodo.17164005
10.5281/zenodo.17164005