The Oxford College Of Pharmacy, Hongasandra, Bengaluru 560068
Non-insulin-dependent diabetes is already globally on the rise, with its prevalence steadily increasing, notably in developing countries like India. These are attributed to lifestyle changes — particularly physical inactivity and unhealthy eating, which are risk factors that can be modified. Available evidence indicates that increased physical activity reduces the risk of T2D. Equally important is the consumption environment that could help people engage in more healthy behaviour by making it easier for them to do so and this includes another rapid shift in nutrition: the consumption of diets high in refined grains, fat, sugar, sweetened beverages and low in fruits and vegetables. A multisectoral approach for promoting healthy diets and increasing physical activity is needed to stem the tides of the diabetes epidemic; however, such reforms require strong political will— if preventive measures are to be effective, they must also be sustainable as well as scalable. Diabetes is assumed to affect about 530 million adults when taking a global perspective, with a prevalence of 10.5 percent globally among adults aged between 20 to 79 years. Type 2 diabetes constitutes about 98 percent of global diabetics; this figure varies greatly between nations. According to an analysis of the National Health Interview Survey data (2016 and 2017), the average percentage rate was 8.5 for diagnosed type 2 diabetes among U.S adult populations. Other nationally representative databases like the Centre for Disease Control and Prevention Diabetes Surveillance System in revealed that in 2022, the overall estimated diagnosed diabetes prevalence was about 11.3 percent of adults (37.3 million people were out of these, there were previously known cases which numbered millions, leaving an estimated few undiagnosed cases-of whom approximately have type 2 diabetes). This has led to speculation regarding a potentially large increase in diabetic numbers due to numbers in childhood obesity being on the rise. Global data seem to support this worry as rates of the worldwide occurrence of type 2 diabetes among teenagers and young adults (15-39 years) increased from 117 to 183 per 100,000 population between 1990 and 2019.
The most prevalent metabolic illness is diabetes, which is mostly brought on by the body's organs developing insulin resistance or producing less insulin than usual. People with insulin-resistant diabetes are more feasible who are over 40, have a high diet of processed or junk food, and be old. Compared to women, men are more likely to have type 2 diabetes. The following are important risk factors: dyslipidemia (high cholesterol), excessive alcohol use, tobacco use, sedentary lifestyle, and poor sleep quality1. Diabetes is mostly a lifestyle disease, however many individuals with unhealthy habits—such as inadequate sleep, high levels of stress, and a poor diet heavy in processed foods, fast food, and fats and carbohydrates—are more susceptible The risk of obesity and dyslipidemia is associated with monounsaturated fatty acids (MUFA). For people over 40 as well as young persons, obesity poses a serious risk for diabetes. Age is regarded as a passive risk factor because it is linked to the development of insulin resistance in the body's organs and a slow reduction in the amount of insulin produced by pancreatic cells2.
AGE
Degenerative and lifestyle-related disorders present a major challenge to the senior population. Even while metabolic disorders—such as T2DM and cardiovascular diseases (CVD)—are among the most common ailments affecting adults in the nation, they are directly linked to aging. Age-related changes in body fat, especially visceral fat, decreased insulin sensitivity, and decreased muscle mass all contribute to insulin resistance in the elderly3. Among older persons, metabolic and cardiovascular disorders are frequently associated with central obscenest and insulin rejection. The disease mechanism of mature-onset diabetes mellitus is attributed to decreased insulin sensitivity brought on by age and changes in beta-cell functional mass, or the inadequate restoration of it in response to elevated insulin resistance. An increased susceptibility to apoptosis and a reduced ability for beta-cell proliferation are associated with aging. According to recent study, Glucose intolerance in the elderly may potentially be influenced by age-related reductions in mitochondrial function. Cognitive impairments, cancers, vitamin D deficiency, ischemic heart disease, and other metabolic diseases are often linked to aging. Globally, 537 million persons between the ages of 20 and 79 are thought to have diabetes mellitus at this time4. Globally, this numerical is expected to increase to 643 million by 2030 and might reach 783 million by 2045.Two significant nationally representative surveys have been used in India to study the evolution of diabetes mellitus:
GENDER DIFFERENCES / SEX
Over the last three decades, a significant elevation in mature-onset diabetes mellitus prevalence has been observed, with striking sex and regional differences. These disparities can be assigned to complex interactions between ethnicity, culture, lifestyle, gene-environment interactions, socioeconomic factors, and social roles. Notably, sex differences play a pivotal role in the prevalence, incidence, and severity of various diseases, yet women were excluded from most clinical trials until the early 1990s. Interestingly, diabetes-related hospitalization and mortality rates are higher among men than women6. The largest populations affected by diabetes are Hispanics, followed by non-Hispanic blacks and non-Hispanic Asians. Youth-onset T2DM is rapidly increasing, with a 2:1 female predominance, whereas male youths are more likely to develop prediabetes than female youths. T2DM is often diagnosed at a lower age and body mass index in men. The pandemic increase in T2DM and its associated complications can be attributed to a combination of genetic effects, epigenetic mechanisms, nutritional factors, and sedentary lifestyle, affecting both genders7.
EPIDEMIOLOGY
Research has shown that the prevalence of type 2 diabetes mellitus, also known as non-insulin dependent diabetes mellitus (NIDDM), varies significantly across different geographic regions and ethnic groups. In India, the first reliable data on diabetes prevalence was obtained from a multicentric study conducted by the Indian Council of Medical Research (ICMR)8. The study found that 2.3% of the urban population and 1.5% of the rural population had diabetes. Notably, people living in rural areas tend to have a lower risk of developing T2DM compared to those in urban areas, likely due to differences in lifestyle. Extensive epidemiological research reveals that obesity and inactive lifestyle are independent risk factors for developing T2DM9. Notably, individuals with the healthiest lifestyle have a 75% lower risk of developing T2DM compared to those with the least healthy lifestyle. According to a National health survey, the average age of T2DM diagnosis is between 29-30 years. While the risk factors for youth-onset and late-onset T2DM are similar, the increasing prevalence of obesity and lifestyle changes have led to a rise in T2DM cases among younger individuals. Multiple epidemiological studies suggest that weight loss and regular physical activity can help prevent or delay the onset of T2DM10. According to the International Diabetes Federation (IDF), approximately 1 in 11 adults (415 million) worldwide suffered from diabetes mellitus in 2015, with a projected increase to 642 million by 2040. Notably, over 90% of diabetes cases are diabetes type2. The occurrence of mature-onset diabetes among children and adults is 13.8 per 100,000 youth per year, with a higher incidence among males (16.7 per 100,000/year) compared to females (11.1 per 100,000/year)11. The incidence also increases with age, with enhanced rates among 15-19-year-olds (15.2 per 100,000/year) than 10-14-year-olds (12.4 per 100,000/year). The up-to-date systematic review work estimated that:41,600 recent cases of youth-onset T2DM occurred globally in 202112. Incidence rates vary by country: 397 per 100,000 in India, 734 per 100,000 in China, and 285 per 100,000 in the US. Incidence rates also vary by ethnicity: 37.8 per 100,000/year for black youths, 32.8 for American-Indian youth, 20.9 for Hispanic youth, 11.9 for Asian/Pacific Islander youth, and 4.5 for non-Hispanic white youths13.”
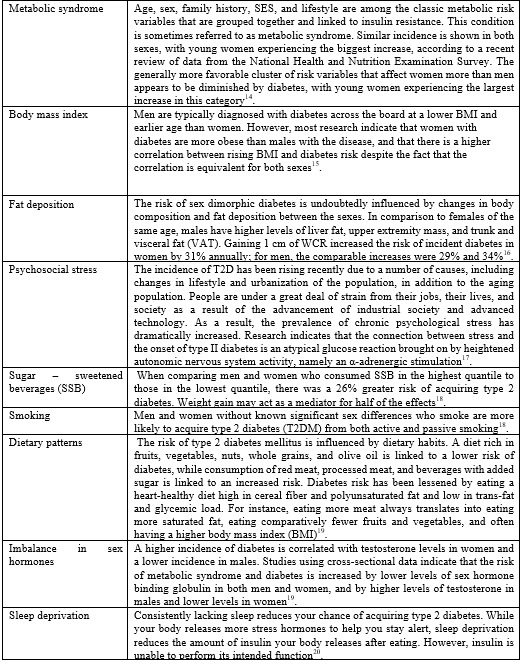
RISK FACTORS
COMORBIDITIES & IT’S COMPLICATIONS:
Diabetes nephropathy:
Chronic consequences, including vascular and non-vascular ones, account for a major portion of the mortality and morbidity linked to diabetes mellitus. The primary factors of end-stage renal disease (ESRD), diabetic nephropathy, commonly known as diabetic kidney disease (DKD), is one of the main microvascular consequences. A slightly elevated urine albumin-to-creatinine ratio (UACR) of 30 to 300 mg/g is indicative of microalbuminuria, the initial stage of diabetic renal disease (DRD). Subsequently, it develops into macroalbuminuria, characterized by UACR levels higher than 300 mg/g, and ultimately results in renal insufficiency, which is described by increasing serum creatinine levels and a decline in estimated glomerular filtration rate (eGFR), ultimately leading to chronic kidney disease (CKD)22. When considering non-diabetics, DKD is a distinct problem in the diabetic population. Its causes are complex and include things like obesity, food, physical activity, smoking, concomitant conditions, diabetes type, and disregard for treatment guidelines. According to studies, 14% of diabetics have fair glycaemic control and 58% of patients have poor glycaemic control23. The use of combined antihyperglycemic medications (oral tablets plus insulin) [adjusted odds ratio (AOR) = 3.77; 95% CI = 1.36-10.44], poor diet adherence (AOR = 1.97; 95% CI = 1.03-3.77), and lack of education (AOR = 2.34; 95% CI = 0.93-5.90) were found to be significant risk factors for inadequate glycaemic control through multivariate logistic analysis. Diabetic nephropathy is present in 32% of cases. Diabetes for five years or longer (AOR = 1.78; 95% CI = 1.05-3.00), age over 50 (AOR = 2.37; 95% CI = 1.15-4.90), hypertension (AOR = 3.22; 95% CI = 1.39-7.47), uncontrolled blood glucose (AOR = 2.67; 95% CI = 1.16-6.16), and low education (AOR = 1.90; 95% CI = 1.16-3.11) are threats for diabetic nephropathy24.
Microvascular complication:
Diabetic Retinopathy:
The most frequent consequence of T2D is diabetic retinopathy, which is defined as damage to the retina's light-sensitive blood vessels. Of the patients in this study, 50% had diabetic retinopathy by the age of 25, usually after a duration of approximately 12 years with the condition. The 35% progressive frequency of peripheral neuropathy, or impairment to the nerves other than the brain, which manifests 12 to 15 years after diagnosis, is as troubling. Changes in the tiny blood vessels at the behind of the eyes are known as retinopathy, and they usually appear after puberty. It is a major cause of visual impairment and blindness in diabetics since it can affect the macula, the peripheral retina, or both. One-fourth of people with type 2 diabetes mellitus and over 10% of the generalized citizens have retinal degeneration25. Significant risk factors for developing retinopathy in people with hyperglycaemia include poor blood sugar regulation, hypertension, and a higher body fat index (BFI). A total of 77 trials from 26 different nations yielded data, which included 99,847 newly diagnosed type 2 diabetic patients. I2 = 97.0% and the pooled prevalence of diabetic retinopathy (DR) was 13.1% (95% CI, 11.1%–15.1%) among these patients. Clinical samples showed a greater prevalence of drug resistance (15.0%, 95% CI = 12.4%–17.8% vs. 11.5%, 95% CI = 8.9%–14.5%; p = 0.05; I2 = 97.0%) than community-based samples. Additionally, the distribution of DR was accelerated in WHO member nations. Africa (19.2%, 95% CI: 14.6%–24.3%; I2 = 76.0%), South-East Asia (15.4%, 95% CI: 10.0%–21.6%; I2 = 79.1%), and Europe (15.0%, 95% CI: 11.2%–19.2%; I2 = 82.0%) are the regions that shared this information. It is significant that a lower incidence of DR among those newly diagnosed with type 2 diabetes was substantially correlated with a higher proportion of female patients. Patients with recently diagnosed glucose intolerance have a increased prevalence of DR has remained unchanged over time26.
Cardiovascular complication:
Heart muscle injury is frequently the first step toward the slow, progressive development of heart failure. cardiac attacks, damaged cardiac valves, or uncontrolled high blood pressure are the usual causes of this injury. The weaker heart muscle has to exert more effort to meet the body's needs as a result, which may wear it out. Diabetes has a significant correlation with an escalated risk of cardiovascular death. The risk of heart related disease is higher among individuals with diabetes, according to the American Diabetes Association and the American Heart Association27. Age, high blood pressure, and high cholesterol are risk factors that become more noticeable after a person has had diabetes for ten years. Diabetes increases the risk of heart failure in Northern Italy by five times when compared to other comorbidities. South Asians in Newcastle also report habitually being physically less active than Europeans, which probably accounts for their higher rates of diabetes and cardiovascular disease. Of those with type 2 diabetes mellitus who were diagnosed, more than half (61.90%) had a family history of the disease, while 38.10% did not. Sixty-nine percent of those with type 2 diabetes were sedentary to lightly physically active28. Of those with a diagnosis, 47.62% were underweight and 52.38% were classed as pre-obesity to obese. 70% of diabetes women and 63.64% of diabetic men in the current study had a large waist circumference. Of the 425 participants, the waist-to-hip ratio (WHR) was higher in 41.25% of the males and 84.16% of the females. To be more precise, 50% of the 22 males with diabetes had a high WHR (>1), compared to 60% of the 138 non-diabetic males with a normal WHR (<1>0.8) was present in 83.26% of non-diabetic females, and 95% of diabetic females had a high WHR (>0.8)29.
Thyroid Dysfunction:
Diabetes mellitus, along with thyroid dysfunction, is the most common chronic endocrine condition, with varying frequency across populations. It is more common in women than in males, rises with age, and is more susceptible to hyper- or hypothyroidism when diabetes is present. Both hyperthyroidism and hypothyroidism can manifest in severe or subclinical stages30. T3, the active thyroid hormone (TH), causes a decrease in TRH and TSH secretion in response to sufficient tissue levels of TH. It also exerts negative feedback at the level of both thyrotrophs in the pituitary and tanycytes in the brain31. Subclinical thyroid disorders (STDs) are defined by low or elevated serum TSH levels, with TH levels at the top and lower ends of their reference range, respectively, in subclinical hyperthyroidism (SHyper) and subclinical hypothyroidism (SHypo). Since 1980, the global prevalence of this condition has nearly doubled, from 4.7% to 8.5% among adults. Insulin and thyroid hormones are inextricably linked in cellular metabolism, thus excess or deficiency in one cause functional derangement in the other32. The physiological and biochemical interactions between insulin, as well as the effects of insulin and iodothyronines on carbohydrate, protein, and lipid metabolism, are documented. Such data show that iodothyronines are insulin antagonists, with high levels being diabetogenic, but the absence of the hormone prevents the development of diabetes.
Excess thyroid hormones accelerate digestive tract absorption while increasing insulin resistance and degradation33. In hypothyroidism, liver glycogen secretion and breakdown diminish, resulting in higher glycogen levels. The gastrointestinal tract's glucose absorption is slowed, as is glucose use in peripheral tissues34. A retrospective analysis was conducted utilizing the Ministry of Health's Primary Care Clinical Database (BDCAP). Type 1 (T1D) and type 2 (T2D) diabetes were assessed using relative risks (OR) and 95% confidence intervals (CI). In a study of 2,596,041 hypothyroid individuals, we identified an OR of 1.77 (1.75-1.80) for T1D and 1.77 (1.76-1.78) for T2D34. This increased risk was seen in both men and women. Hypothyroid individuals over 65 years old had a nearly neutral risk of T1D (0.96 [0.94?0.99]) and T2D (0.99 [0.98?0.99]). Hypothyroid individuals on replacement medication had a higher risk of T1D (1.32 [1.28?1.36]) and T2D (1.23 [1.22?1.24]) than untreated hypothyroid patients. Hyperthyroidism was associated with a higher risk of T1D (1.66 [1.60?1.72]) and T2D (1.71 [1.70?1.73]) among 418,772 individuals. This risk was present in both sexes. Individuals over 65 had a low risk of T1D (0.89 [0.83?0.95]) and a nearly neutral risk of T2D (1.03 [1.02?1.05]). And it has been discovered that in both sexes, people under the age of 65 who have thyroid malfunction are more likely to get diabetes35.
Chronic Kidney Disease:
Chronic kidney disease (CKD), a major consequence of type 2 diabetes (T2D), raises the risk of both cardiovascular disease (CVD) and end-stage kidney disease. Studies were undertaken, and data was gathered. The study comprised 48,011 patients with CKD (mean age ± SD, 73.8 ± 13.1 years; 44?male), with 47.9% having co-existing T2DM36. Patients with T2DM were older (75 ± 10.6 versus 72.7 ± 14.9 years, p < 0>
Diabetic Neuropathy:
Diabetic neuropathy is the most prevalent consequence in both Type 1 and Type 2 DM patients, with more than half having nerve damage at some point in their lives, hence a risk prediction model for diabetic neuropathy was established in industrialized nations. DN affects up to 50% of diabetic people. It includes a number of neuropathic syndromes, the most prevalent of which being distal symmetrical polyneuropathy or "diabetic peripheral neuropathy" (DPN). Poor glycaemic management, as well as macrovascular disease drivers such as hypertension and obesity, are risk factors for DPN. Retrospective follow-up research was undertaken with a total of 808 diabetic patients recruited from January 1, 2005 to December 30, 2021 at two designated referral hospitals in Amhara regional state38. Multi-stage sampling approaches were utilized, and data was gathered from medical records using a checklist by Kobo and converted to STATA version-17 for analysis. The results revealed that the incidence of diabetic neuropathy among DM patients was 21.29% (95% CI; 18.59, 24.25). In multivariate logistic regression, glycaemic control, other comorbidities, physical activity, hypertension, alcohol use, type of therapy, and white and red blood cell counts were all statistically significant. The nomogram was produced, with a discriminating power AUC of 73.2% (95% CI: 69.0%, 77.3%) and a calibration test (P-value = 0.45). It was internally verified using the bootstrapping approach, with discrimination performance of 71.7 (95% CI: 67.2%, 75.9%)39.
Obesity:
Obesity or excessive weight gain is recognized as the most significant risk factor for the development and progression of type 2 diabetes mellitus (DM) across all age groups. It has reached pandemic proportions, making the treatment of obesity essential in the global effort to prevent and manage type 2 DM. Numerous clinical studies have shown that moderate, sustained weight loss can improve blood glucose levels, enhance insulin sensitivity, and reduce the need for diabetic medications. A comprehensive approach involving diet, exercise, and lifestyle changes can effectively reduce obesity, thereby alleviating the harmful effects and severe complications of DM.
The rapid pace of modernization, urbanization, and socio-economic growth has led to improved living standards but also to a more stressful, sedentary lifestyle and unhealthy eating habits in many parts of the world40. Over the past two decades, obesity has become a global pandemic, impacting nearly every organ system and emerging as a significant public health concern as one of the most prevalent non-communicable diseases (NCDs). Data published from 2017 to 2020 indicate that 42.4% of adults have a BMI of 30 kg/m?2; or higher, while 20.9% of youth fall into the same category. Additionally, the age-adjusted prevalence of severe obesity (BMI ? 40 kg/m?2;) is 9.2%. By 2030, it is projected that 14% of men and 20% of women worldwide will develop clinical obesity. Furthermore, 18% of individuals are expected to have a BMI greater than 30 kg/m?2;, 6?MI greater than 35 kg/m?2;, and 2?MI greater than 40 kg/m?2; 41.
Diabetic foot:
Diabetic foot disease is a common and debilitating consequence of diabetes mellitus, encompassing a range of conditions such as infection, ulceration, and gangrene. It is one of the most severe complications of diabetes and the leading cause of hospitalization for diabetic patients. Unfortunately, even after successful wound healing, the recurrence rate of diabetic foot ulcers is alarmingly high. Risk factors for diabetic foot ulcers include peripheral neuropathy, peripheral arterial disease, frequent or minor foot trauma, infection, foot deformities, a history of diabetic foot ulcers or amputations, and Charcot osteoarthropathy42. However, poor wound healing is considered the primary cause of chronic diabetic wounds, and the presence of polymicrobial infections can further exacerbate this issue. Individuals with diabetes and diabetic foot complications face a higher mortality rate compared to those without foot complications. Diabetic foot infections (DFIs) can quickly escalate to life-threatening conditions and are directly responsible for amputations in 25%-50% of diabetic individuals. Each year, approximately 18.6 million people worldwide develop a diabetic foot ulcer, including 1.6 million people in the United States43. These ulcers precede 80% of lower extremity amputations among people with diabetes and are linked to an increased risk of mortality. Studies comparing vitamin D levels in diabetic patients with and without diabetic foot ulcers (DFU) have shown that patients with DFU have lower vitamin D levels. Specifically, vitamin D levels in patients with DFU were found to be 8.90 ng/mL (6.52–10.90), compared to 16.25 ng/mL (13–19.59) in those without DFU. These findings suggest a correlation between lower vitamin D levels and the presence and severity of DFU44.
Diabetic dyslipidaemia:
Triglyceride levels that are raised and low levels of high-density lipoprotein (HDL) cholesterol are indicative of dyslipidaemia linked with type 2 diabetes. These changes frequently occur long before hyperglycaemia becomes a clinically relevant condition. Low HDL cholesterol has been linked to an independent risk factor for both the onset of diabetes and cardiovascular disease, according to recent research. It is possible for atherosclerosis to progress more quickly before diabetes is formally diagnosed, and this is probably due in part to these lipid abnormalities as well as the presence of small, dense LDL particles45. On the other hand, unless nephropathy or inadequate glycaemic control are present, hypertriglyceridemia may be seen in type 1 diabetes, but HDL cholesterol levels usually stay normal or even raised. Additionally, across all lipoprotein classes, patients with diabetes display anomalies in both quality and kinetics. Adipocytokines, hyperglycaemia, and insulin insufficiency or resistance are a few of the variables that may be responsible for the alterations in lipid metabolism observed in diabetic individuals. Apolipoprotein B (apoB) secretion is positively correlated with increased hepatic triglyceride production. Additionally, insulin has less of the typical inhibitory influence on hepatic apoB synthesis and triglyceride release in VLDL, leading to larger and more triglyceride-enriched VLDL particles. Both type 1 and type 2 diabetes have a substantial correlation between triglycerides and coronary heart disease (CHD). When combined with other characteristics of the metabolic syndrome or congestive heart failure, elevated serum triglycerides frequently occur prior to the onset of type 2 diabetes mellitus. High triglyceride levels, once diabetes is established, continue to predict the risk of CHD, frequently without reference to other risk factors. Smoking, obesity, glucose intolerance, hyperuricemia, cholesterol, and triglycerides are all favourably connected with HDL cholesterol and negatively correlated with total triglycerides. The risk associated with hypertriglyceridemia is still substantial even though multivariate analysis may lessen the apparent risk directly related to triglycerides46. Triglyceride levels measured while fasting between 2.6 and 4.5 mmol/L are connected with a twofold increase in the risk of CHD, while values between 4.5 and 9.0 mmol/L are linked to The risk associated with hypertriglyceridemia is still substantial even though multivariate analysis may lessen the apparent risk directly related to triglycerides. A two-fold increase in the risk of CHD is connected with fasting triglyceride levels between 2.6 and 4.5 mmol/L, while a nine-fold increase is linked to levels between 4.5 and 9.0 mmol/L47. At the King Faisal University (KFU) Health Centre in the eastern part of Saudi Arabia, a retrospective cross-sectional investigation was conducted. Data about patients was collected between October 2014 and February 2021. The KFU polyclinic management granted permission for us to access this data from the KFU Health Centre. Prior ethical approval (approval number 2020-10-62) was obtained from the Institutional Review Board of Ethics and Research Committee in the KFU College of Medicine. Gender, age, country, and the results of blood tests, which comprised lipid profiles (triglycerides, HDL, and LDL) and haemoglobin A1c (HbA1c) levels, were among the information gathered on the patients.191 individuals with type 2 diabetes (T2D) were included in the study; 137 (71.7%) of these patients were from Saudi Arabia, while 54 (28.3%) were from other nations. The ages of the patients ranged from 21. 191individuals with type 2 diabetes (T2D) were included in the study; 137 (71.7%) of these patients were from Saudi Arabia, while 54 (28.3%) were from other nations. With a mean age of 56.2±11.8, the patients' ages ranged from 21 to 100 years. 107 of them (56%) were female. With an average of 187.3 mg/dl, cholesterol levels ranged from 102 to 300 mg/dl48.
REFERENCE:






Jenisha K. , Chaithra K. , Chandana N. , Deepthi R. , Dhruva R. , Gagana K. , A Comprehensive Review On Integrating Lifestyle Modifications To Manage Diabetes Mellitus & Its Comorbidities , Int. J. of Pharm. Sci., 2024, Vol 2, Issue 9, 791-803. https://doi.org/10.5281/zenodo.13786067
 10.5281/zenodo.13786067
10.5281/zenodo.13786067
