
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
S. V. U. College of Pharmaceutical Sciences, Sri Venkateshwara University, Tirupati, Andhra Pradesh, India 517502
Diabetes Mellitus is one of the fastest growing diseases in the world now. Diabetes mellitus is a chronic metabolic disorder characterized by elevated blood glucose levels (hyperglycemia) resulting from defects in insulin secretion/action, decrease in glucose utilization and increase in glucose production. It is a major public health concern globally, contributing significantly to morbidity, mortality and healthcare costs.It is mainly classified into three types Type-1 diabetes, Type -2 diabetes and Gestational Diabetes mellitus. Over 540 million adults live with diabetes worldwide (IDF 2024). Common symptoms include excessive thirst, polyuria, polyphagia, weight loss and fatigue. It is a leading cause of morbidity and mortality worldwide, necessitating the discovery and development of novel antidiabetic agents. To facilitate this, a wide array of screening models has been developed to evaluate potential antidiabetic compounds through various mechanisms. Invitro and in-vivo animal models are essential to understand new therapies and cure. Streptozotocin and Alloxan are diabetogenic agents which causes diabetes. The antidiabetic properties of synthetic or natural substances can be evaluated by in-vitro methods such as glucose uptake, effect on glycosylation, inhibition of alpha-amylase and alpha-glucosidase enzymes.
Diabetes Mellitus (DM), or diabetes is a chronic illness characterized by persistently high blood glucose levels due to inadequate insulin production, or body does not properly use the insulin that is produced. Insulin is a hormone produced by the pancreas that regulates blood glucose levels.The body needs insulin to convert sugar, starch and other foods into energy. Diabetes impairs the body’s ability to regulate blood sugar levels, leading to a range of short-term and long-term complications. The long-term effects of diabetes include damage to blood vessels (leads to heart attack and stroke), problems with eyes, kidneys, feet and nerves [1]. Diabetes mellitus is commonly referred to as a “sugar” and is the most common endocrine disorder. The International Diabetes Federation (IDF) estimates that India has large and growing number of people with diabetes. The IDF estimates that in 2021, there were 77 million adults living with diabetes in India. This number is projected to 156.7 million by 2050.It is a prevalent condition worldwide, affecting millions of people. Various risk factors such as obesity and sedentary lifestyle contribute to its development. Diabetes mellitus is a significant medical condition with rising incidence and fatality rates. Elevated plasma glucose levels caused by insulin deficiency, insulin resistance, or both are signs of diabetes mellitus and result in changes in how proteins, lipids, and carbohydrates are metabolised [2]. The exact cause for diabetes is uncertain. Nevertheless, scientists believe that genes, environmental factors and other pathological conditions cause resistance to insulin action, involves in the development of the diabetes mellitus [3].
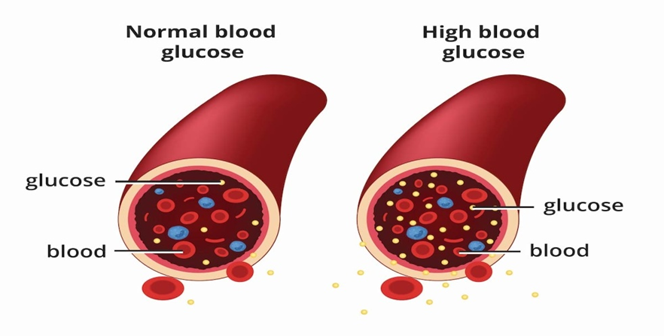
Fig 1: Glucose level in diabetes
TYPES:
Also known as autoimmune diabetes or juvenile -onset diabetes. It is a condition in which the body does not manufacture any insulin.This type of diabetes caused by autoimmune destruction of insulin beta-cells in the pancreas. 5-10 % of diabetescases are type 1 diabetes.
Symptoms: Sudden onset- weight loss, frequent urination, thirst, fatigue.
Also known as adult-onset diabetes. In which the body does not make enough or does not utilise the insulin that is released properly, and is most prevalent kind of condition and accounts for 90-95 % of all case of diabetes [2].
Symptoms: Gradual onset- may be mild or unnoticed for years.
This type of diabetes occurs during pregnancy and usually resolves after child birth. GDM is a carbohydrate intolerance of variable severity develops in the second trimester or in the third trimester. Increases the mother’s risk of type 2 diabetes later; baby may have high birth weight or low blood sugar at birth.
Type 1 diabetes often referred to as juvenile diabetes, is insulin dependent and know to affect only 5% of diabetic population. Type 2 diabetes, which is non-insulin dependent, usually develops in adults over the age of 40 [4, 5].
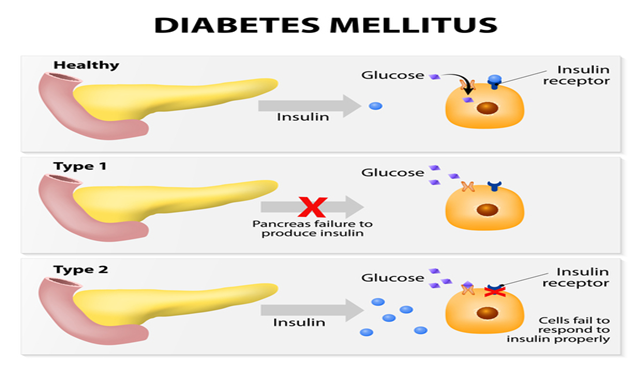
Fig 2: Types of diabetes
EPIDEMIOLOGY:
There has been a sharp increase in diabetes prevalence in the past several decades. The number of people diagnosed with diabetes has risen dramatically since 1980, with low- and middle-income countries. WHO data shows that the number of people living with diabetes has risen dramatically from 200 million in 1990 to 830 million in 2022. According to the International Diabetes Federation the global prevalence is expected to continue rising with projections estimating that 1 in 9 adults (20-79 years) will have diabetes by 2025. It is higher in developed countries than in developing countries.There were an estimated 9.50 million people living with type 1 diabetes in 2025. The countries with the largest number of people with diabetes are, and will be in the year 2025, India, China, and the US [6, 7].
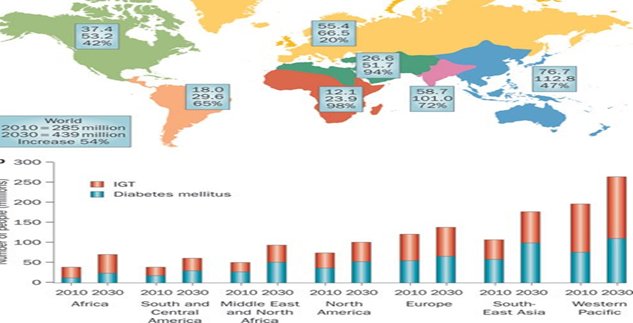
Fig 3: Diabetes level past to future
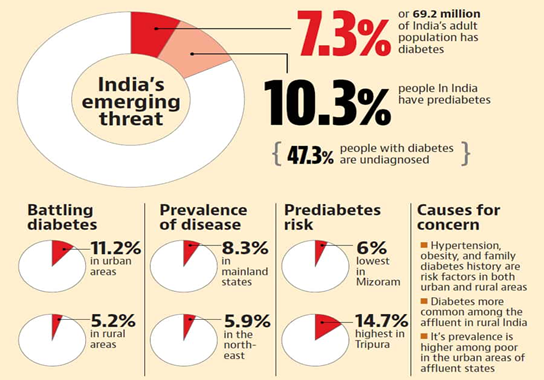
Fig 4: Diabetes cases in India (News, July 5 2023)
PATHOPHYSIOLOGY:
Diabetes mellitus has a severe negative impact on social, psychological, and physical health as well as quality of life. The majority of diabetic problems are caused by oxidative stress, such as increased ROS generation or compromised antioxidant changes in antioxidant enzymes, and decreased glutathione metabolism. Free radical production contributes to the pathophysiology of several diseases, including diabetes mellitus. Through a series of pathological alterations, increased advanced glycation product (AGE) synthesis and accumulation is also connected to diabetes squeal as retinopathy, neuropathy, and renal dysfunction [5].
Pathophysiology of Type 1 DM:
Pathophysiology of Type 2 DM:
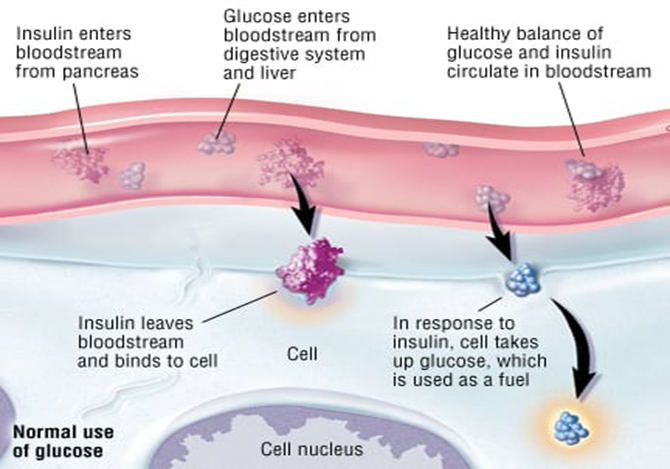
Fig 5: Pathophysiology of diabetes
CAUSES:
Mainly causes are morbidity and mortality, and obesity and weight gain. In type 2 diabetes, the deterioration of pancreatic cell function prominently progress over time. Age, obesity, insufficient energy intake, alcohol consumption, smoking, and are all independent contributors to this disease [9].
SYMPTOMS:
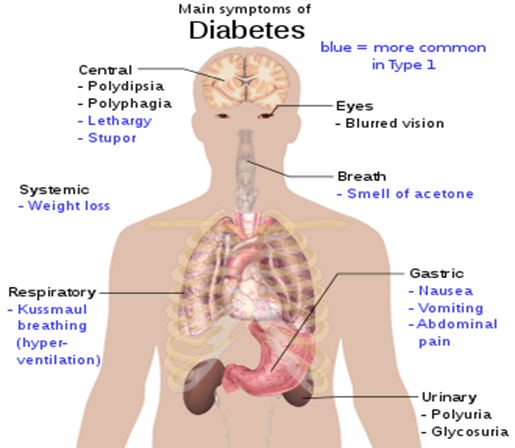
Fig 6: Diabetes symptoms
CLINICAL MANIFESTATIONS:
DIAGNOSIS:
Diabetes is typically diagnosed through several clinical tests that assess bloog glucose levels:
This blood test, which does not require not eating for a period of time (fasting), shows your average blood sugar level for the past 2 to 3 months. It measures the percentage of blood sugar attached to haemoglobin, the oxygen carrying protein in red blood cells [10].
A blood sample will be taken after you have not eaten anything the night before. A fasting blood sugar level less than 100mg/dL is normal.
For this test, you fast overnight. Then the fast blood sugar level is measured.
TREATMENT:
The diabetes mellitus is reduced by using ofsome medicinal plants and oral hypoglycemic drugs such as sulfonylureas, biguanides, acarbose and guar gum etc. New drugs for treatment of NIDDM like Troglitazone, Thiazolidinediones groups and insulin is reviving by the repaglinide and benzoic acid derivatives at food intake time in diabetes type 2 cases.The two different Incretins-based therapy modalities designed for the management of diabetes are incretins mimetic and incretins effect amplifiers [11].
Herbal medicine such as plants also used in the diabetic treatment and now-a-days herbal products are ruling the world and also WHO approved 21,000 plants are listed as medicine, 2500 species are from India and in Indian species 150 species are most costly and sell by India. India is a world’s botanical garden and also known as world’s largest producer of the herbal plants [12, 13].
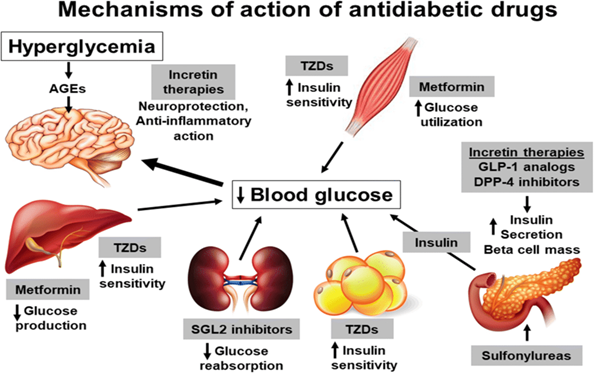
Fig7: Mechanism of action of anti-diabetic drugs
SCREENING METHODS OF ANTI-DIABETIC ACTIVITY:
A. INVIVO SCREENING MODELS
Chemically induced diabetes:
The three types of chemical agents that induce diabetes are those that directly harm β-cells, temporarily limit insulin secretion and synthesis, and reduce insulin’s metabolic effectiveness in the target tissue.This is based on using of diabetogenic agents.
Diabetes is brought on by STZ in practically all animals. STZ has the ability to cause diabetes either with a single injection or several low-dose injections. The most used medication for causing diabetes in rats is STZ.
Ex:1. The stem bark of Berberis aristata DC (family: Berberidaceae) extract in STZ-induced diabetic Albino Wister Rats and proved that these plants used as anti-diabetic drug [14].
Alloxan also known as mesoxalylurea and pyrimidinetetrone, itcomes under urea derivatives and unstable in water at neutral pH, and pH3 stable state. Alloxan produce reactive oxygen species in dialuric acid which produces superoxide radicals, hydrogen peroxide, hydroxyl radicals are responsible for death of beta cell and ensure state of insulin - dependent alloxan diabetes [15].
Ex: Anti-diabetic effect of the ethanolic extract of carica papaya leaves in alloxan-induced diabetic ratsto investigate the treatment for diabetes and proved that may be replaced by the glibenclamide in treatment of diabetes which does not cause any side effect [16].
Surgical induced diabetes:
This method totally depends on pancreatectomy in animals. This is used for type 1&2 diabetes induction.
Mainly used partial pancreatectomized animals, ex: dog, primate, pig, and rat. In high dose of STZ or alloxan may cause to higher toxicity other than diabetes, so to avoid that condition researchers have done partial pancreatectomy in dogs with low doses of STZ [17].
Genetically induced diabetics models
These methods conduct on genetic mutation transmitted from the generation to generation.
Hormone induced diabetics:
Diabetes caused by growth hormone in an unharmed adult cats and canines.Growth hormone increases glucose production by gluconeogenesis and glycogenolysis from liver and kidney. Repeated growth hormone injections results in a severely diabetic conditions with all associated symptoms, such as ketonemia and ketonuria [18].
Insulin deficiency due to insulin antibodies:
Guinea pig serum can induce insulin antibody that are used to produce insulin deficiency animal model of diabetes. Every month, guinea pigs receive subcutaneous injections of bovine insulin [1mg], which are then punctured with a heart needletwo weeks later to induce bleeding. From collected blood serum is separate out and injected intravenously to the rats,which causes a dose-dependent increase in blood sugar.
Virus induced diabetes:
A viral infection plus a B-cell-specific autoimmune may cause type-1 diabetes. Similar to a human insulin-dependent diabetic, the d-variant of the encephalamycarditis virus [emc-d] selectively infects and kills the cells in male ICR Swiss mice
B. IN VITRO SCREENING MODELS:
1.Insulin secretagogue activity:
This mainly promotes insulin secretion from pancreatic β-cells. Plants extract or distinct organic substances that are potentiating the several in-vitro models, including isolated islets, perfuse pancreas, and different B-cell lines, can be utilised to study the glucose-stimulated insulin release by pancreatic B-cells. For instance, a modelof perfuse rat pancreas [19].
2. Insulin sensitizing activity:
Magnify the glucose uptake by target tissue by promoting the cell surface expression of GLUT transporters. The major target of the insulin is liver, adipose tissue and skeletal muscle and using of insulin mimetic and insulin sensitizing properties of the compounds to test or screen these organ parts [20].
3. Alpha glucosidase and alpha amylase inhibitory activity:
Alpha glucosidase and alpha amylase are the intestinal enzymes and very strong role in carbohydrate digestion. These activities are inhibition to reduce the post prandial glucose levels in blood.
Ex: In-vitro anti-diabetic activity of methanolic extract of Psidium guajava leaves. This assay shows the inhibition of these enzymes increase and proved this plant have anti diabetic activity in vitro studies [21].
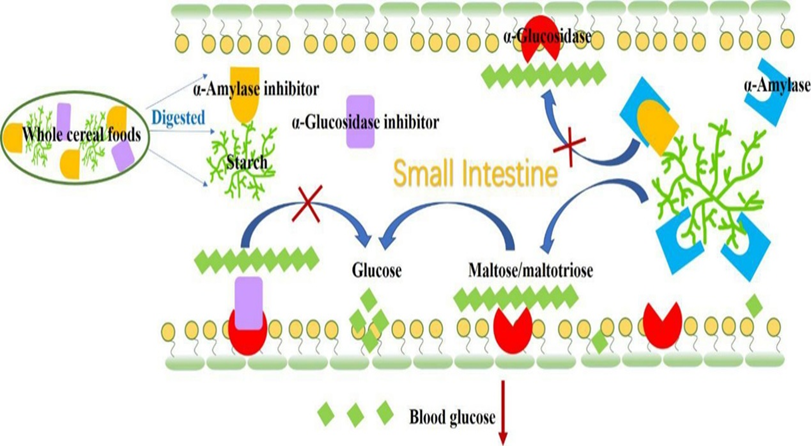
Fig 8: Alpha- amalyse and glucosidase mechanism
4. In-vitro anti-hyperglycemic activity screening by starch-iodine colour assay:
Diagrammatic illustration of the starch-iodine colour assay’s in vitro anti-hyperglycemic effect. This test is based on the small amount of iodine test -starch modification. Test solution concentrations are made, then incubated in alpha amylase-containing sodium phosphate buffer (pH 6.9;sodium chloride) for 10mins at 37? each reaction well receives a 1% soluble starch solution, which is then incubates at 37? for 15 mins. Iodine reagents are used after adding 1M hydrochloric acid to halt the action of alpha amylase. In a micro plate reader, the colour change is visible, and the absorbance at 660 nm is accurate with control, the same process is repeated [21].
5. Glucose diffusion assay:
In this case glucose diffusion is main characteristic. Since glucose is a large molecule, its diffusion across a membrane is difficult. Hence, it diffuses across membranes through facilitated diffusion, down the concentration gradient.The carrier protein at the membrane binds to the glucose and alters its shape such that it can easily transported.
Ex: Using of H. beccarii by dialysis models. The experiment starts with loading of 1ml of extract (500µg/ml) and 1ml of glucose solution (20mm in 0.15 M NaCl) into dialysis bag (12000 MW, Hi-Media laboratory). The dialysis bag sealed with both ends and placed in a 200 ml beaker containing 45 ml of 0.15 M NaCl. The control bag was loaded with 1 ml of 0.15 M NaCl, 20 mm glucose, and 1 ml distilled water. The quantity of glucose in the external solution was measured. The beaker was placed in orbital shaker at room temperature (20±2°C). All tests were carried out in triplicate, and the concentrations of glucose were estimated using the O-Toluidine method [22].
6. Goldthioglucose obese diabetic model:
Goldthioglucose (GTG) is a diabetogenic compound; it causes obesity induced Type -2 diabetes. The intraperitoneal administration of GTG in experimental animal causes the obesity, hyperinsulinemia, hyperglycemia, insulin resistance for a period of 16- 20 weeks. The GTG is travels into the cells and causes necrotic lesions, which is responsible for the development of hyperphagia and obesity. It also increases body lipid, hepatic lipogenesis and triglyceride secretion, increased adipose tissue lipogenesis and decreases glucose metabolism [23].
7. Glucose uptake assays by adipocytes cell line:
Adipose tissue is a link between obesity and Type 2 diabetes, and develops intracellular lipid concentrations and insulin resistance. Insulin resistance either at the adipocytes or skeletal muscle levels contribute to hyperglycemia. This Pathways related to insulin resistance may be studied in cell lines of adipocytes such as 3T3-L1 cells and rat L6 muscle engineered to over-express GLUT4 [24].
8. Non-enzymatic glycosylation on haemoglobin inhibition assay:
Glucose (2%), haemoglobin (0.06%), and Gentamycin (0.02%) solutions were prepared in phosphate buffer 0.01 M, pH 7.4. 1 ml each of the above solutions was mixed and 1ml of the methanol extract of varying concentrations was added to it, respectively. The reaction mixture was incubated in dark at room temperature for 72hrs and then the degree of glycosylation of haemoglobin was measured calorimetrically at 520nm. Metformin was used as a standard drug for the assay and percentage inhibition was calculated by using the formula: %inhibition = Absorbance Sample – Absorbance Control × 100 Absorbance Sample
where, Abs control is the absorbance of the control reaction (containing all reagents except the test sample) and Abs sample is the absorbance of the test sample [25].
9. Glucose Uptake by Yeast Cells:
Yeast suspension was prepared by repeated washing (by centrifugation 3,000×g; 5 min) in distilled water until the supernatant fluids were clear. A 10% (v/v) suspension was prepared with the supernatant fluid. 1mL of the glucose solution (5, 10, and 25 mM) was added to various concentrations of methanol extract (250, 500, 750, and 1000 µg) and incubated for 10 min at 37 °C. Reaction was started by adding 100 μl of yeast suspension, vortexes and further incubated at 37 °C for 60 min. After 60 min, the reaction mixture was centrifuged (2,500×g, 5 min) and the glucose content was estimated in the supernatant. Metronidazole was taken as a standard drug. The percentage increase in glucose uptake by yeast cells was calculated using the following formula:
%inhibition = Absorbance Sample – Absorbance Control × 100 Absorbance Sample.
where, Abs control is the absorbance of the control reaction (containing all reagents except the test sample) and Abs sample is the absorbance of the test sample [25].
CONCLUSION:
Diabetes mellitus remains a global health challenge with rising prevalence. Early diagnosis, lifestyle modification, and appropriate pharmacological treatment are crucial to preventing complications. The former is more prevalent among children and latter is among adults.
A number of potential therapies for DM are recently being investigated. It is widely reported that oral delivery is the convenient administration route for diabetes. The management of Type 1 DM is usually injectable insulin delivery in contrast to Type 2 in which the major drugs are administered orally.
The antidiabetic activity properties evaluated by several methods such as Chemical (STZ, Alloxan-induced rats), Surgical, Genetic, Hormone induced, insulin deficiency due to insulin antibodies, virus induced diabetes and in vitro methods such as insulin secretagogue and insulin sensitizing activities and also alpha-glucosidase and alpha- amylase enzyme inhibition activities.
REFERENCES



Dr. Girish. C, Mahitha. M , Muniraja Lakshmi. K, A Comprehensive Review of Diabetes Mellitus with Insights into Current Screening Approaches, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 2437-2448. https://doi.org/10.5281/zenodo.16028753
 10.5281/zenodo.16028753
10.5281/zenodo.16028753