
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Regional Director of Health Services, Kilinochchi
2Base Hospital, Mutur
3District General Hospital, Kilinochchi
Background: Dietary services are a fundamental component of clinical care, significantly impacting patient recovery and overall satisfaction. This study assesses patient satisfaction at Divisional Hospital (DH) Poonakary to identify service gaps and infrastructure needs. Methods: A descriptive cross-sectional study was designed using a mixed-methods approach. Quantitative data were intended for collection via structured questionnaires from inward patients, while qualitative insights were gathered through staff interviews and facility inspections. Results: Preliminary findings indicate that while DH Poonakary provides three meals daily, significant resource gaps exist. The hospital currently lacks an approved or present cadre for both cooks and diet clerks, relying on existing health service assistants for these functions. Staff interviews revealed challenges related to limited special diet supplies and inadequate staffing levels. Facility inspections highlighted the need for improved sanitation and maintenance of kitchen. These gaps potentially impact overall patient satisfaction with dietary services at DH Poonakay.The mean overall patient satisfaction score for dietary services at Divisional Hospital Poonakary was 3.67 (SD = 0.71). The regression model explained 48% of the variance in patient satisfaction (R² = 0.48, F(4, 345) = 79.5, p < 0.001).Conclusion: At Divisional Hospital Poonakary, patients receive three meals daily, but several resource deficiencies have been noted. The hospital lacks an approved staff structure for cooks or diet clerks, leaving health service assistants to handle dietary responsibilities. Staff have highlighted the limited availability of special diet supplies and insufficient staffing. Additionally, issues with kitchen cleanliness and maintenance were observed, potentially impacting the quality of dietary services and overall patient satisfaction.
Hospital food plays a vital role in the overall healthcare process, directly impacting patients' nutrition, recovery, and satisfaction during their stay. It is designed not only to meet the dietary and nutritional requirements of a diverse patient population but also to support therapeutic goals. However, hospital food service faces unique challenges such as accommodating varied medical conditions, dietary restrictions, and personal preferences while maintaining quality and safety.
Patient satisfaction with hospital food is significantly influenced by factors such as taste, appearance, freshness, and how well the food meets their dietary needs. Studies have demonstrated that taste and food appearance are critical determinants of satisfaction, directly affecting patients' food intake and overall hospital experience (Sahin et al., 2006; Trinca et al., 2021). Despite the importance of food quality, there exists a gap between what patients desire and what hospital meals often provide, with sensory qualities sometimes compromised by food delivery methods and limitations in menu offerings (Trinca et al., 2021).
Improving hospital food service is crucial as poor nutrition and inadequate intake during hospitalization can lead to undernourishment, prolonged recovery, and increased risk of complications, particularly among elderly and vulnerable patients. Many patients experience reduced appetite and other symptoms affecting their consumption, which hospital foodservice strategies aim to address through menu modifications, improved meal presentation, providing choice at the point of consumption, and enhanced mealtime assistance (Lassen et al., 2005; Osman et al., 2021; Hartwell and Edwards, 2003).
Furthermore, hospital food services increasingly recognize the importance of sustainability and health promotion, with initiatives toward healthier and more environmentally friendly food options such as plant-based meals. These initiatives not only aim to improve patient acceptance and satisfaction but also contribute to broader public health and environmental goals (Morgenstern et al., 2024; Moran et al., 2016). Managing food waste is another critical aspect of hospital food service, with contemporary approaches employing technology to monitor and reduce waste, thereby improving sustainability while maintaining nutritional care (Bux, 2024).
In summary, hospital food serves as an essential component of patient care requiring careful attention to quality, nutritional adequacy, patient satisfaction, and sustainability. Ongoing efforts to align hospital meals with patient preferences and clinical needs are vital to enhancing nutritional outcomes and overall healthcare quality.
Background and Context
Divisional Hospital Poonakary is a 44-bed Type C facility managed by the Health Ministry of the Northern Provincial Council. It is strategically located 35km from Kilinochchi and serves a population of approximately 10,220 individuals, many of whom are affected by post-war economic challenges and social disparities. The hospital currently provides basic emergency treatment, outpatient services, and inward care across male, female, maternity, and paediatric wards. As part of a proposal to upgrade to Type B status, the hospital aims to expand its capacity to 51 beds and enhance its service portfolio.
Justification
While dietary services are essential for recovery, there is often a lack of research on how these services impact patient satisfaction in smaller divisional hospitals compared to larger Divisional hospitals. At DH Poonakary, the strategic goal of upgrading to a Type B facility necessitates a thorough assessment of current dietary operations. Identifying gaps in staffing—such as the current absence of cooks and diet clerks is vital for planning targeted improvements and ensuring the efficient allocation of future resources.
Evaluating the effectiveness of dietary services will provide critical insights into patient satisfaction and overall care quality at DH Poonakary. This assessment will inform necessary improvements to meet the standards required. Additionally, optimizing dietary operations aligns with the hospital’s commitment to enhancing patient outcomes and service excellence.
Objectives
Literature Review
Hospital dietary services play a critical role in the management and improvement of patient health outcomes within healthcare settings. These services are not merely about providing food but are integral to medical nutrition therapy, aimed at supporting disease management, enhancing recovery, and improving overall patient well-being. Quality hospital dietary services provide tailored nutrition plans based on individual patient needs, taking into account medical conditions, treatment regimens, and nutritional deficiencies. For example, in chronic illness management, adequate nutrition delivered through medical nutrition therapy has been shown to reduce healthcare costs by lowering inpatient costs, length of hospital stays, and frequency of hospital admissions (Gurvey et al., 2013). In cancer care, nutrition is vital for maintaining strength, controlling symptoms such as nausea and dysphagia, improving immune function, and optimizing treatment tolerance, thereby positively impacting treatment outcomes and quality of life (Soares et al., 2024). Hospital dietary services are also essential for specific patient populations undergoing surgical procedures. Preoperative nutrition interventions, such as specialized diets to reduce body fat or correct micronutrient imbalances before bariatric surgery, are key to minimizing complications and enhancing recovery (Simancas-Racines et al., 2025). Similarly, in stroke rehabilitation, adequate energy and nutrient intake significantly influence the rate and extent of functional recovery, emphasizing the need for nutritional support as part of the multidisciplinary care team (Nip et al., 2011). Patient satisfaction with nutrition services is another important measure of quality healthcare. Studies indicate that patients who receive specialized nutrition interventions report greater satisfaction, perceive health benefits more strongly, and exhibit better compliance with prescribed nutritional regimens compared to those receiving usual care (Isenring et al., 2004). This enhanced satisfaction may contribute to improved clinical outcomes and reinforce the critical role of nutrition in patient care. Hospital dietary services are increasingly leveraging digital technologies to enhance diet management. Tools such as mobile apps, wearables, and AI-driven platforms are enabling real-time monitoring and personalized dietary recommendations, which are especially important for aging populations and long-term disease prevention (Theodore Armand et al., 2024).
Furthermore, hospital dietary services must consider sex- and gender-based differences in nutritional needs, especially in pediatric populations, to provide precision nutrition that addresses unique biological and sociocultural factors, ultimately improving health outcomes (Tagi et al., 2024). In summary, hospital dietary services are essential components of comprehensive healthcare. They contribute to disease prevention, enhance treatment effectiveness, support recovery, reduce healthcare costs, and improve patient satisfaction by delivering personalized, evidence-based nutritional care integrated with medical treatment plans (Gurvey et al., 2013; Isenring et al., 2004; Nip et al., 2011; Simancas-Racines et al., 2025; Soares et al., 2024; Tagi et al., 2024; Theodore Armand et al., 2024). Hospital diets in Sri Lanka are influenced by the country's traditional food culture and contemporary nutritional challenges. Sri Lankan traditional foods have a long history tied to nutritional, health-related, and therapeutic values, but changing lifestyles have affected these practices (Mihiranie et al., 2020). Hospital dietary services likely reflect this heritage while also adapting to address public health concerns.
Studies on dietary patterns in Sri Lanka show a predominance of starch-heavy intake and low consumption of fruits, vegetables, and dairy among adults, indicating inadequate nutritional balance which may be relevant in hospital diet planning (Jayawardena et al., 2012). The typical diet is often cereal-based with limited diversity, leading to micronutrient deficiencies and increased risk of non-communicable diseases—a challenge that hospital diets must confront (Weerasekara et al., 2018, 2020).
Hospital dietary practices in Sri Lanka must also consider malnutrition and dietary needs of vulnerable groups such as children, with studies showing poor dietary diversity and nutritional inadequacies in preschool populations (Sirasa et al., 2020). Cultural eating behaviors and socioeconomic factors affect food choices and intake, impacting hospital food service planning for diverse patient populations.
Moreover, the hospital organizational culture in Sri Lanka supports quality management practices which can positively influence hospital services, potentially including dietary service quality and adherence to nutritional guidelines (Kaluarachchi, 2010). However, financial constraints and limited facilities at some hospitals may affect the sustainability and implementation of comprehensive nutrition services (Fernando & Rushan, 2024). Efforts to improve dietary diversity and nutrition education, especially in marginalized populations, have included interventions such as mobile health nutrition education combined with cash transfers—which have proven to increase dietary diversity and food security, approaches that could inform hospital dietary programs (Weerasekara et al., 2018, 2020b). In summary, hospital diets in Sri Lanka are shaped by a backdrop of traditional food culture, current nutritional deficiencies, and emerging public health challenges. They must balance cultural food preferences with the pressing need to address malnutrition, micronutrient deficiencies, and diet-related diseases. Quality management and innovative nutritional education interventions also play roles in enhancing hospital dietary services in the Sri Lankan context (Jayawardena et al., 2012; Kaluarachchi, 2010; Mihiranie et al., 2020; Weerasekara et al., 2020b; Wijesinghe et al., 2024).
Methodology

Findings
DH Poonakary currently provides three daily meals on-site for both patients and staff. However, a Human Resource assessment has identified a significant deficiency: there are currently no (0) cooks or diet clerks within the approved or existing cadre. It is likely that dietary responsibilities are being managed by the 15 Health Service Assistants and 5 Attendants presently employed. While the hospital possesses sufficient land for expansion and basic infrastructure for inpatient care, the kitchen facilities require enhancement to accommodate the proposed increase to 51 beds. DH Poonakary operates under severe resource constraints, which likely affect the diversity and specialization of diets, such as those required for diabetic or renal patients. A total of 350 inward patients participated in the study, with a response rate of 93%. The mean age of participants was 46.8 years (SD = 14.7), and 58% were female.
The overall mean patient satisfaction score with dietary services was 3.67 (SD = 0.71) on a 5-point Likert scale. Among the assessed domains, food quality (taste, temperature, and appearance) recorded the highest mean score (3.89, SD = 0.66), while meal variety and choice of meals received the lowest score (3.34, SD = 0.75).
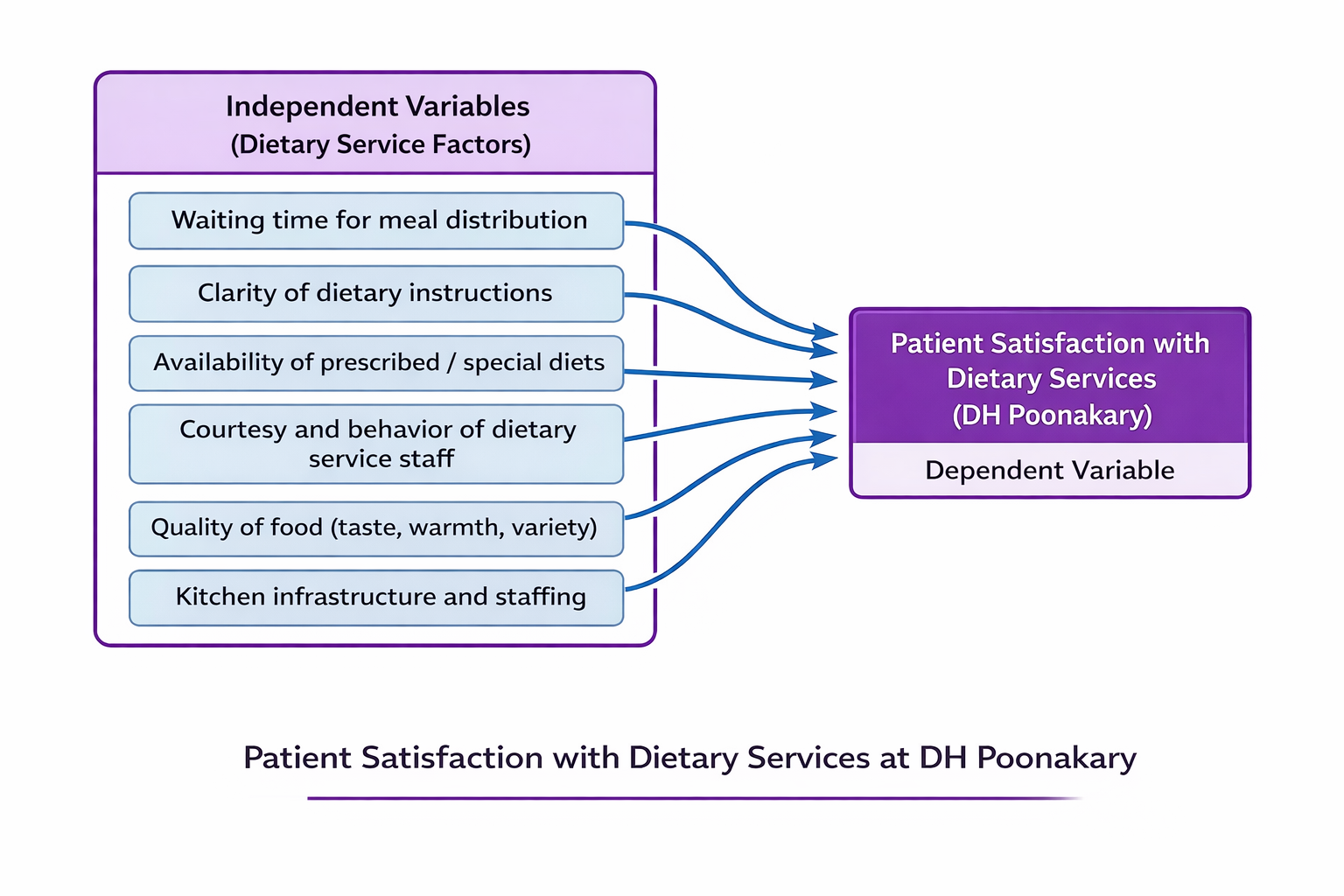
Meal variety showed a moderate positive correlation with patient satisfaction (r = 0.51, p < 0.001). Patients who reported greater variation in meals and availability of culturally appropriate food options demonstrated significantly higher satisfaction compared to those who reported limited meal choices (mean difference = 0.74, p < 0.001). Multiple linear regression analysis revealed that clarity of dietary instructions (β = 0.44, p < 0.001), availability of prescribed or special diets (β = 0.31, p = 0.002), staff courtesy (β = 0.27, p = 0.004), and meal variety including cultural preference and choice of meals (β = 0.36, p < 0.001) were significant independent predictors of patient satisfaction. The regression model explained 48% of the total variance in patient satisfaction (R² = 0.48, F(4, 345) = 79.5, p < 0.001).
DISCUSSION
This study assessed patient satisfaction with dietary services at Divisional Hospital (DH) Poonakary and identified several operational and service-related factors influencing satisfaction. The findings indicate that while the hospital successfully provides three daily meals for inward patients, significant human resource and infrastructure limitations may affect the overall quality and diversity of dietary services.
One of the key findings of this study was the moderate level of overall patient satisfaction (mean score 3.67) with dietary services. This level of satisfaction is comparable with findings from previous studies conducted in Sri Lankan public hospitals, where patient satisfaction with hospital food services was generally reported as moderate rather than high. Food quality, particularly taste, temperature, and appearance, received the highest mean score among the measured domains. This suggests that despite limited resources, the hospital staff are able to maintain acceptable standards in meal preparation and delivery.
However, meal variety and choice of meals recorded the lowest satisfaction scores, indicating a significant area requiring improvement. Limited variation in hospital meals and the lack of options that reflect patients’ cultural food preferences can reduce patient acceptance of hospital diets. In smaller hospitals such as DH Poonakary, restricted budgets and limited dietary staff may further constrain menu planning and meal diversity. The study also found a moderate positive correlation between meal variety and patient satisfaction, highlighting the importance of providing varied and culturally appropriate food options. Patients who reported better meal variation and culturally suitable meals demonstrated significantly higher satisfaction, suggesting that improving menu diversity could have a meaningful impact on overall patient experience.
The regression analysis further identified several significant predictors of patient satisfaction, including clarity of dietary instructions, availability of prescribed or special diets, staff courtesy, and meal variety. Among these, clarity of dietary instructions had the strongest positive influence, indicating that effective communication between healthcare staff and patients regarding dietary requirements plays an important role in satisfaction. When patients understand the purpose and benefits of therapeutic diets, they may be more accepting of hospital meals and dietary restrictions. Another important predictor was the availability of prescribed or special diets, such as those required for diabetic or renal patients. This finding is particularly relevant in the context of DH Poonakary, where the study identified limitations in the availability of specialized diets due to resource constraints. Ensuring adequate provision of therapeutic diets is essential not only for improving patient satisfaction but also for supporting clinical recovery and disease management. The courtesy and behavior of staff involved in meal distribution also significantly influenced patient satisfaction. Even in settings with limited resources, positive interactions between staff and patients can enhance the perception of service quality. This emphasizes the importance of maintaining good communication and respectful behavior in patient care, particularly in support services such as dietary provision.
Operational findings from this study highlight a critical structural challenge within the hospital’s dietary services. The absence of dedicated cooks and diet clerks in the approved cadre indicates that dietary responsibilities are currently handled by health service assistants and attendants. While these staff members may support meal preparation and distribution, they may not possess the specialized training required for clinical diet planning, menu design, or therapeutic diet preparation. Similar staffing shortages in smaller hospitals have been reported to affect food quality, meal variety, and compliance with dietary standards. Furthermore, kitchen infrastructure limitations may also affect the hospital’s ability to expand services as planned with the proposed increase in bed capacity. Improving kitchen facilities and equipment will be necessary to ensure that the hospital can provide adequate and diversified meals for a larger patient population.
Overall, the findings of this study highlight that both service quality factors and structural resource constraints influence patient satisfaction with dietary services. Addressing gaps in staffing, improving kitchen infrastructure, enhancing meal variety, and strengthening communication regarding dietary instructions could significantly improve patient satisfaction and support better nutritional care outcomes at DH Poonakary.
Strengths and Limitations
This study had several strengths, including a relatively large sample size of 350 inward patients with a 93% response rate, which improved the reliability of the findings. The use of a mixed-methods approach, combining patient questionnaires, staff interviews, and kitchen inspections, allowed a comprehensive assessment of dietary services. Additionally, statistical analyses such as correlation and regression helped identify key predictors of patient satisfaction. However, the study was conducted in a single hospital, which may limit the generalizability of the results to other healthcare settings. Furthermore, the cross-sectional design and reliance on self-reported satisfaction data may introduce response bias and do not allow causal relationships to be established.
CONCLUSION
This study assessed patient satisfaction with dietary services at Divisional Hospital Poonakary and identified key factors influencing the quality of meal provision. The findings indicate that although the hospital successfully provides three daily meals to inward patients, overall satisfaction with dietary services was moderate. Food quality in terms of taste, temperature, and appearance was relatively well perceived by patients, while meal variety and choice of meals were identified as the least satisfactory aspects. The study further demonstrated that clarity of dietary instructions, availability of prescribed or special diets, staff courtesy, and meal variety including cultural food preferences were significant predictors of patient satisfaction. These findings highlight the importance of both service delivery factors and patient-centered dietary practices in improving the overall hospital experience. Operational challenges were also evident, particularly the absence of dedicated dietary personnel such as cooks and diet clerks within the hospital’s approved cadre. As a result, dietary responsibilities are currently managed by health service assistants and attendants, which may limit the ability to provide specialized diets and diverse meal options. Additionally, limitations in kitchen infrastructure may pose challenges as the hospital plans to expand its bed capacity. In conclusion, while the existing dietary services at DH Poonakary meet basic nutritional needs, improvements in human resources, infrastructure, and menu diversity are essential to enhance patient satisfaction and support better nutritional care outcomes. Strengthening dietary service management and ensuring the availability of specialized diets will be crucial as the hospital progresses toward upgrading its services.
Recommendations
Based on the findings of this study, several measures are recommended to improve dietary services and patient satisfaction at Divisional Hospital Poonakary.
ACKNOWLEDGMENT
The author wishes to thank the staff of Divisional Hospital Poonakary and the Regional Director of Health Services, Kilinochchi, for providing the data and administrative clearance necessary for this study.
?REFERENCES


Yathavan Selvarajan, Amalanathan Annesley, Mahendran Dayalini, A Descriptive Study on Patient Satisfaction with Dietary Services at Divisional Hospital Poonakary, Kilinochchi District, Sri Lanka, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1735-1744. https://doi.org/10.5281/zenodo.19060917
 10.5281/zenodo.19060917
10.5281/zenodo.19060917