Department of Pharmacy Practice, Srinivas College of Pharmacy, Valachil, Post Farangipete, Mangalore-574143
Regular medication reconciliation is a valuable tool for improving patient medication safety by reducing potential medication errors. By systematically comparing a patient’s medication orders to all of the medications that the patient has been taking, healthcare providers can ensure accuracy and prevent harmful discrepancies. The Objective of the study was to identify the factors associated with medication discrepancies and understand their impact on patient safety. It was a prospective observational study on medication reconciliation was conducted over 6 months in a tertiary care hospital. Medication discrepancies were identified by reviewing medical records. The study included all patients aged 18 years and above, aiming to capture a broad and representative patient population. The study included 225 patients (mean age 57.82 years; 132 men, 123 women). A total of 633 discrepancies and 784 comorbidities were identified during admission. The majority of patients (47.84%) had two comorbid conditions, followed by those with three comorbidities (22.74%). Most patients (63.52%) were prescribed 1-5 medications based on their past medication history. Factors associated with unintentional discrepancies included age, past medication history, and comorbidities. In conclusion the findings reveal a significant prevalence of medication discrepancies, particularly among elderly patients with multiple comorbidities and those on polypharmacy. Addressing these discrepancies is crucial for improving patient outcomes, as unintentional medication discrepancies can lead to adverse drug events and compromised patient safety. The study underscores the importance of thorough medication reconciliation processes to mitigate risks and enhance the overall quality of healthcare delivery.
The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) defines medication reconciliation as "the process of comparing a patient's medication orders to all the medications the patient has been taking.1. High rates of medication errors brought on by inadvertent medication inconsistencies continue to be a problem in spite of multidisciplinary collaborations for patient care 2. Up to 50–70% of patients may experience medication errors as a result of these inadvertent inconsistencies during care transitions3. Routine medication reconciliation helps reduce medication errors and maintain or improve patient medication safety4. To be effective, medication reconciliation requires cooperation, task reallocation among healthcare professionals, and a robust implementation strategy to optimally reduce adverse health consequences associated with medication use5. Accordingly, efficient medication reconciliation can be completed by pharmacists, physicians or nurses6. More specifically, pharmacists are among key members of the team for medication reconciliation service and this also has an opportunity for reconciliation intervention and recommendation7. Various characteristics are highlighted to predict harmful discrepancies8. Although data on the effectiveness of these various options are limited, some of the programs have success fully reduced the number and severity of discrepancies using an interdisciplinary process9. To contribute to the growing literature on medication discrepancies and the reconciliation process, this study aimed to describe the frequency of discrepancies in admission medications, the medication classes involved, and the factors associated with these discrepancies.10. And elderly inpatients assigned to a discharge planning and education intervention program that included medication reconciliation and counseling, in addition to a follow-up even after discharge.
MATERIALS AND METHODS
Study Design: A prospective, observational study was performed on medication reconciliation in inpatient of various department of the Hospital. The study was completed in the period of 6 months.
Sample Size: 255 [9]
Study Criteria:
Inclusion criteria: Patient admitted in the hospital aged >18 years, of any sex and who is already havingany comorbid condition and was using any drug prior to the admission.
Exclusion Criteria: Patients of vulnerable population, unconscious, who are not willing to participate, those who are not able to provide history within 24 hours are excluded from the study.
Source Of Data Collection:
Information Physician, Patient and Medical Records. The BPMH for each patient includes all information regarding pre-admission medication along with the dose and frequency for each drug, vitamins, herbal medication or non-prescription drugs or any drug or food allergies.
Statistical Analysis: Statistical analysis involves collecting and scrutinizing every data sample in a set of items from which samples can be drawn and a suitable statistical test was applied to analyze the, data. The collected data were analyzed using Microsoft Excel.
RESULT:
Patient demographics:
Out of the 600 patients included in the study, 42.5% (255 patients) had discrepancies in their prescriptions. The average age of the patients was 58.6 years, with 51.76?ing male. Notably, 55.29% of the patients were aged above 60, emphasizing the vulnerability of geriatric individuals for developing chronic diseases. This finding has significant implications for healthcare, highlighting the need for tailored care and interventions for older patients. Detailed demographic information of the subjects can be found in Table 1, highlighting the importance of these findings.
Table 1: Demographics of Subjects
|
Age (yrs.) |
Male (n=132) |
Female (n= 123) |
Total (n=255) |
|||
|
n |
% |
n |
% |
n |
% |
|
|
18-39 |
21 |
15.90 |
15 |
12.19 |
36 |
14.11 |
|
40-59 |
36 |
27.27 |
42 |
34.14 |
78 |
30.58 |
|
60 &above |
75 |
56.81 |
66 |
53.65 |
141 |
55.29 |
Number of Co-Morbidities
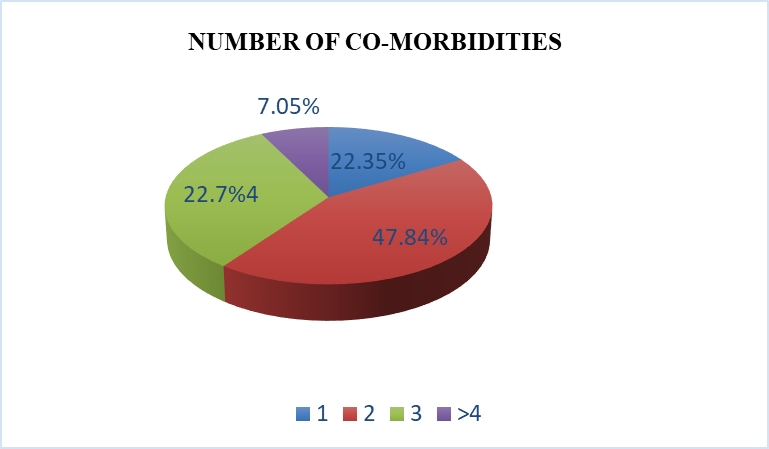
The study explores the relationship between comorbid conditions and medication discrepancies. Evidence suggests that as the number of comorbid conditions increases, the number of prescribed medications also rises, potentially leading to intentional or unintentional medication discrepancies on charts. In this study, 784 comorbidities were identified. The majority of patients (47.84%) had two comorbid conditions, followed by those with three comorbidities (22.74%). A detailed breakdown of the quantity of comorbidities can be found in Table 2. This analysis provides valuable insights into the association between comorbidities and medication discrepancies,
Table 2: Number of Co-Morbidities
|
Number of co-morbidities |
No. of co-morbidities per subject(n=255) |
Percentage (%) |
|
1 |
57 |
22.35 |
|
2 |
122 |
47.84 |
|
3 |
58 |
22.74 |
|
>4 |
18 |
7.05 |
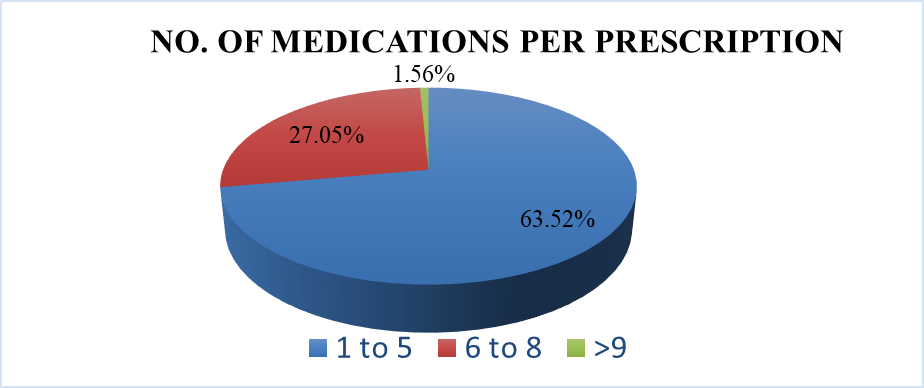
Number of Past Medications Per Prescription
Effective medication reconciliation relies on obtaining a patient's past medication history. The presence of polypharmacy is a key factor in the occurrence of medication discrepancies. This study delves into the examination of the quantity of medications used. Among the 255 patients in the study, a total of 1007 drugs were administered. Table 3 illustrates the distribution of participants based on their past medication history. The majority, 162 patients (63.52%), were prescribed 1-5 medications, followed by 6-8 medications for 35.29% of patients, and 1.56% of patients received 9 or more medications. These findings will be valuable for assessing the association of past medication history (Table 11) with medication discrepancies.
Table 3: No. of Past Medications Per Prescription
|
No. of medications per prescription |
No. of prescription (n=255) |
Percentage (%) |
|
1-5 |
162 |
63.52 |
|
6-8 |
90 |
35.29 |
|
>9 |
4 |
1.56 |
Association between Medication Discrepancies and Study Characteristics
In analyzing the patient data, several significant distinctions emerged between the two groups. First and foremost, the age distribution within these groups displayed a notable contrast. The "unintentional" group, comprising 124 individuals, exhibited 28 patients aged 18-39, 61 in the 40-59 age bracket, and 35 individuals aged 60 and above. In contrast, the "intentional" group, consisting of 131 patients, featured only 8 individuals aged 18 39, 17 in the 40-59 age range, but a substantial 106 patients aged 60 and above.
The statistical analysis underscored the significance of this difference, as the p-value for the age group comparison was less than 0.00001, indicating a highly significant variance in age distribution between the two groups. Additionally, an investigation into the past medication history of these patients revealed another noteworthy distinction. Within the "Unintentional" group, 67 patients had a history of 1-5 past medications, while 56 individuals had taken 6-8 past medications, and 1 patient had more than 9 past medications. Conversely, in the "Intentional" group, 95 patients had a history of 1-5 past medications, 34 individuals had taken 6-8 past medications, and 3 patients had consumed more than 9 past medications. The statistical analysis again emphasized the significance of this difference, with a p-value for the past medication comparison of less than 0.00001, signifying a highly meaningful distinction in past medication profiles between the two groups. Furthermore, an evaluation of the number of co-morbidities among the patients revealed a substantial difference between the "unintentional" and "intentional" groups. In the "unintentional" group, 25 individuals had one co-morbidity, 39 had two co-morbidities, and 45 had three co-morbidities, and 15 had more than four co-morbidities. Conversely, in the "No" group, 32 patient had one co-morbidity, 83 had two co-morbidities, 13 had three co-morbidities, and 3 individuals had more than four co-morbidities. Once again, the statistical analysis highlighted the significance of this distinction, as the p-value for the co-morbidity comparison was less than 0.00001, indicating a highly meaningful difference in the number of co-morbidities between the two groups. These findings shed light on the patient demographics and medical histories, underscoring the importance of these factors in the context of the study.
Table 3: Association Between the Medication Discrepancies And Study Characteristics
|
Characteristics |
Descriptions |
Discrepamcies |
P-value |
|
|
Unintentional n=124 |
Intentional n=131 |
|||
|
Age Group |
18-39 |
28 |
8 |
< 0> |
|
40-59 |
61 |
17 |
||
|
60 &above |
35 |
106 |
||
|
Past Medication |
1-5 Past Medications |
67 |
95 |
< 0> |
|
6-8 Past Medications |
56 |
34 |
||
|
>9 Past Medications |
1 |
3 |
||
|
co-morbidities |
1 |
25 |
32 |
< 0> |
|
2 |
39 |
83 |
||
|
3 |
45 |
13 |
||
|
>4 |
15 |
3 |
||
DISCUSSION
The current study, based on a study involving 600 patients, showed a slightly higher percentage of men suggesting a greater presence of male patients. Additionally, majority of the patients were aged above 60 years, further emphasizing the importance of addressing the healthcare needs of older individuals. In contrast, Meda V.S et al result, based on a study with 106 participants, revealed that around 42% of the subjects were men, while 58% were women. It also highlighted that the majority of these individuals were aged above 60 years, accounting for 63% of the sample. Results from the present study, with its larger sample size and focus on prescription accuracy, provides a more detailed and actionable understanding of patient demographics and healthcare quality. These findings shows the necessity of reconciling healthcare for older patients and the critical need to ensure precise medication administration to enhance patient care and safety1. The present study analyzed a total of 784 comorbidities, most patients had two comorbidities followed closely by those with three. This suggests that many patients have multiple health issues simultaneously, which can complicate their medical care. Mattia Del tos et al.'s study echoes this pattern, finding that a high percentage of patients (77.8%) had two or more comorbidities when admitted to the hospital. Together, these findings emphasize the importance of considering these multiple health conditions when providing care, as they can impact treatment decisions and patient outcomes11.
It was found that most prescriptions, contained between 1 to 5 past medications. A smaller number, had 6 to 8 past medications, and very few, had 9 or more past medications. This shows that how many medications patients were taking when they were admitted, and it's crucial for understanding medication discrepancies. Mattia Del tos et al.'s study, they examined medications in their patient group and found a total of 1565 medicines. Out of these, 856 were medications that patients were already taking at home, and 709 were new medications prescribed during their hospital stay11.
CONCLUSION
In conclusion, this comprehensive study on medication reconciliation and discrepancies in hospitalized patients highlights critical aspects of patient care. The findings reveal a significant prevalence of medication discrepancies, especially among elderly patients with multiple comorbidities and those on polypharmacy, posing substantial risks to patient safety. This research underscores the importance of robust medication reconciliation processes in preventing adverse events and improving patient outcomes. Future efforts should focus on targeted interventions and quality improvement initiatives to enhance patient safety further.
ACKNOWLEDGEMENTS:
Authors would like to extend deepest gratitude to Srinivas College of Pharmacy and would like to extend our thanks and appreciation to the study participants for smooth completion.
Conflicts of Interest: The authors declare that there are no conflicts of interest.
REFERENCES


Satish S., Jush Shah*, A. R. Shabaraya, A Prospective Observational Study on Medication Reconciliation: Factors Contributing to Medication Discrepancies, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 598-603. https://doi.org/10.5281/zenodo.14278952
 10.5281/zenodo.14278952
10.5281/zenodo.14278952
