MES College Of Pharmacy Sonai.
Mouth dissolving films (MDFs), also known as oral thin films (OTFs), have emerged as a novel and innovative drug delivery system designed to enhance patient compliance, particularly among pediatric, geriatric, and dysphagic populations. These films disintegrate rapidly upon contact with saliva, eliminating the need for water and allowing for faster onset of action compared to conventional oral dosage forms. A fast-dissolving dosage form that dissolves in the mouth in a matter of seconds without the need for water, mouth dissolving film is mostly utilized for elderly and pediatric patients because of its adaptability and patient compliance. For medications with a high metabolism and low bioavailability, it is a possible dose form. The most common method for producing mouth dissolving film is solvent casting because of its consistency and better physical qualities, although additional methods include rolling, solid dispersion, semisolid casting, hot melt extrusion, and solvent casting. The following parameters, such as chemical and physical properties, are assessed for mouth dissolving film. In addition to providing information on formulation considerations, preparation procedures, and evaluation criteria, the study summarizes data on oral dissolving films as a potentially effective dosage form for administering medications to elderly and pediatric patients.
Mouth Dissolving Films (MDFs) are a novel technology designed for the oral delivery of active substances. In addition to the active ingredients, MDFs contain a variety of excipients, including polymers, and additional additives, including plasticizers, thickening agents, flavors, colors, sweeteners, and surfactants. disintegrants. A common method for systemically distributing a medication to provide a therapeutic or pharmacological effect is the mouth dissolving film (MDF). Because MDF formulations avoid first-pass digestion, their systemic bioavailability is enhanced. It is not necessary to use water because MDFs dissolve rapidly with secretion when placed on the tongue. Consequently, they have a full impact on the drug's bioavailability, which speeds up the onset of the specific action.The oral mucous membrane is more porous and has a large blood supply. One possible location for a rapid, continuous, and regulated medication delivery system is the oral mucous membrane.Available research models suggest that instead of disintegrates we can also use insoluble particles eg. MCC (microcrystalline cellulose), silica as a disintegration enhancer. To beat difficulties related to swallowing of the solid unit dosage form (tablet, capsule.) Oral film technology was invented. The introduction of MDF into the market was closely associated with patient education about appropriate administration, including "do not chew/do not swallow" recommendations.This framework developed in the latter part of the 1970s as an alternative to traditional dose structures, such as rapidly dissolving tablets and containers, for individuals of all ages who had trouble swallowing those forms. A typical oral degradation film is around the size of a postage stamp. The oral dissolving tablet's presence at the commercial center served the following purposes: giving patients advice on how to be organized, along with cautions like "don't bite/don't swallow." In spite of these limitations, gulps and bites were common. Orally decreasing LM, however, freed most people from these tragedies. Because of its ease and versatility, fast-dissolving LMs are the most sophisticated type of oral dosage form. It dissolves in the oral cavity in a matter of minutes, increasing the effectiveness of the active pharmaceutical substances.
When it comes to bedridden, comatose, elderly, and pediatric patients, this kind of technology is quite helpful.
The concept of oral dissolving film:
Limitation of Mouth dissolving film:
The mouth dissolving film can effectively incorporate a variety of API types. The oral fast- dissolving film's texture, solubility, and homogeneity can all be enhanced by micronized API. It is necessary to conceal the taste of the bitter medication in order to stop the API from coming into direct touch with the saliva. API should typically taste good, be stable, able to pass through the oral mucous membrane, and have a low dosage (≤ 40 mg). [3]. The process of loading high doses into the film is called sonication.
Water-soluble polymers are used as film formers because they provide the films with mechanical properties, a nice mouthfeel, and rapid disintegration. To produce films with the required hydrophilicity, flexibility, mouthfeel, and solubility, polymers can be used singly or in combination. As the molecular weight of polymer film bases rises, the rate of polymer disintegration decreases.
Ideal properties of polymer:
1) Polymers that are plain, nontoxic, and inexpressive should be used.
2) It should have no flavour.
3) It should be free of drainable toxins.
4) It should be affordable and simple to obtain.
5) It shouldn't be a major hindrance during the deterioration interaction.
6) It must possess exceptional wetting and spreading qualities.
C. Plasticizer
In general, mechanical properties such as tensile strength and percent elongation are improved by adding plasticizer to the formulations. Plasticizer concentrations typically fall between 0% and 20% w/w. PEG, glycerol, diethyl phthalate, triethyl citrate, tributyl citrate, and so forth are typical examples of plasticizers.
D. Saliva Stimulating Agent
In order to speed up the breakdown and disintegration of the oral film in the mouth, saliva stimulating medications are utilized to increase saliva production. It can be used either alone or in combination, and its range is 2–6%. Saliva-stimulating chemicals that are frequently utilized include tartaric acid, ascorbic acid, lactic acid, malic acid, and citric acid. The most widely used of them is citric acid.
E. Sweetening Agent
Usually, sweeteners are used to mask the bitter taste of certain medications. One can use natural and artificial sweeteners alone or together. Types of sweetener includes natural sweeteners, such as corn syrup solids, xylose, ribose, glucose, mannose, galactose, fructose, dextrose, and sucrose and artificial sweeteners aspartame, cyclamate, and saccharin. Acesulfame K, sucralose, alitame, and neotame
F. Flavouring Agent
Natural and synthetic Flavors, such as methyl salicylate, eucalyptol, thymol, and synthetic vanilla, cinnamon, various fruit flavours, mints like peppermint and menthol, and essential oils, may be used singly or in combination.
G. Surfactant
As a solubilizing, wetting, or dispersion agent, surfactants are employed. To swiftly dissolve the film and liberate the active component, surfactant is utilized. Surfactant can make poorly soluble medications more soluble in quickly dissolving oral films. Poloxamer 407, sodium lauryl sulphate, benzalkonium chloride, benzethonium chloride, tweens, and spans are a few examples.
H. Colouring Agent
When some of the ingredients or drugs in the formulation are present in insoluble or suspension form, FD&C-approved colouring additives or titanium dioxide are added, with concentrations not to exceed 1%w/w.
The methods for manufacturing oral thin films include:
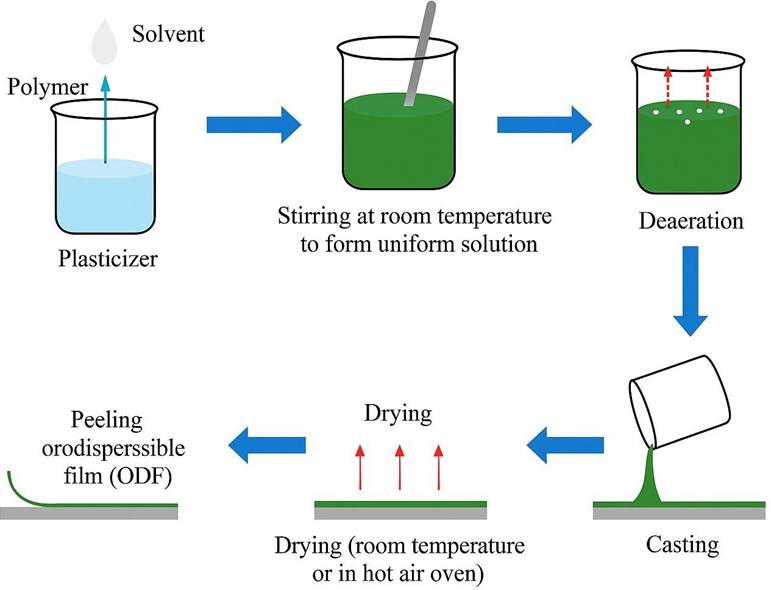
Because of its ease of use, affordability, and capacity to create thin, homogeneous films with accurate drug loading, the solvent casting method is one of the most popular and successful approaches for creating mouth dissolving films (MDFs). In order to create a uniform viscous solution, the film-forming polymer is first dissolved in an appropriate volatile solvent or a mixture of solvents, usually water, ethanol, or hydro-alcoholic combinations, while being continuously stirred. The active pharmaceutical ingredient (API) is then dissolved or dispersed in this polymeric solution, along with other excipients such as plasticizers (e.g., glycerin, polyethylene glycol), sweeteners, flavoring agents, saliva- stimulating agents, and surfactants, depending on the formulation requirements. Once a clear and uniform solution is achieved, it is carefully poured onto a flat, leveled casting surface such as a glass plate or a Teflon-coated surface. The solution is then spread evenly using a casting knife or applicator to ensure a consistent film thickness. After casting, the solvent is allowed to evaporate at controlled room temperature or under mild heating conditions (typically 30–50°C) to avoid degradation of the drug. This results in the formation of a dry, thin film, which is then peeled off, cut into desired sizes, and stored in moisture-proof containers. Critical formulation and process parameters—such as solvent selection, drying time, polymer viscosity, and ambient humidity—must be carefully controlled to ensure film uniformity, mechanical integrity, and drug content uniformity. The solvent casting method is particularly suitable for heat-sensitive drugs and enables precise dose adjustment by modifying the surface area of the film, making it an ideal approach for preparing fast-dissolving oral films. Polymers, plasticizers, and the remaining ingredients of the placebo formulations were dissolved in distilled water and then agitated with a magnetic stirrer to create the aqueous solution. After one hour of stirring and two hours of rest to eliminate air bubbles, 10 milliliters of the solution were transferred onto a glass Petri dish with a surface area of 71.76 cm². At 45 to 50°C, the film solution was dried in a hot air oven. Following drying, the films were sliced into little pieces, each measuring 4 cm2, and removed with the aid of a sharp blade after being stored in a desiccator for 24 hours. Films with air bubbles, cuts, or imperfections were excluded from further study. Selected films were subjected to different evaluation parameters.
3. Addition of API:
The semisolid casting method is an advanced and modified version of the conventional solvent casting technique used for the preparation of mouth dissolving films (MDFs), particularly suitable for formulations requiring higher mechanical strength or incorporating poorly soluble drugs. In this method, a solution of water-soluble film-forming polymer—such as The first step is to prepare sodium alginate, polyvinyl alcohol (PVA), or hydroxypropyl methylcellulose (HPMC) in an appropriate solvent. A separate gel mass or semisolid solution is formed by dissolving or dispersing the active pharmaceutical ingredient (API) and other excipients such as plasticizers, surfactants, sweeteners, and flavouring agents into a gel-forming agent like gelatine or carrageenan. This semisolid mass is then mixed with the polymeric solution under continuous stirring or gentle heating to form a uniform and viscous gel-like system. The resulting semisolid blend is carefully cast onto a non-stick surface such as a Teflon plate using a calibrated applicator to ensure even spreading. After that, it is left to dry at a regulated room temperature or slightly higher temperatures to promote solvent evaporation without sacrificing the consistency or integrity of the medicinal content. After drying, the film is peeled off and cut into the desired dimensions. The semisolid casting method offers several advantages, including better content uniformity for viscous or particulate formulations, enhanced film mechanical properties, and suitability for thermolabile drugs due to low drying temperatures. Additionally, the method allows for precise control over film thickness and texture, resulting in films that are both robust and flexible, making them ideal for rapid disintegration and improved patient compliance.
3) Hot melt extrusion method
The hot melt extrusion (HME) method is a modern, solvent-free technique increasingly used for the formulation of mouth dissolving films (MDFs), especially for poorly water-soluble drugs and heat- stable compounds. This technique involves physically combining the medication with thermoplastic film-forming polymers, such as hydroxypropyl cellulose (HPC), polyethylene oxide (PEO), or ethyl cellulose, as well as appropriate plasticizers and other excipients, such as sweets, flavoring agents, and disintegrants. This dry blend is then fed into an extruder equipped with a heated barrel and rotating screws. The material is exposed to controlled heat and mechanical shear, which soften or melt the polymers and uniformly disperse the drug at the molecular or particulate level. The molten mass is then forced through a flat die to form a thin, continuous film of uniform thickness. Immediately after extrusion, the film is passed through rollers and cooled, either at room temperature or with a cooling device, to solidify and retain its shape. The resulting film is cut into the desired sizes and stored in moisture-resistant packaging. Hot melt extrusion method offers several advantages, such as the elimination of organic solvents (making it environmentally friendly and safer), better drug dispersion, and the possibility of improving drug bioavailability through amorphous solid dispersions. Additionally, it allows continuous production, which is highly suitable for large-scale manufacturing. However, the method is generally limited to drugs and excipients that are thermally stable, as the processing temperatures may range from 70°C to 150°C. All things considered, the hot melt extrusion process creates mouth dissolving films with superior mechanical strength, homogeneity, and quick disintegration qualities, making it a useful approach in the production of contemporary pharmaceutical films.
4) Solid dispersion extrusion method
A specific approach for creating mouth-dissolving films that improve the solubility and bioavailability of medications that are not very water soluble is the solid dispersion extrusion method. In this method, a solid dispersion is first prepared by dispersing the active pharmaceutical ingredient (API) within a suitable hydrophilic carrier matrix such as polyethylene glycol (PEG), polyvinylpyrrolidone (PVP), or other water-soluble polymers. This is typically achieved through processes like melt mixing or solvent evaporation, resulting in the drug being molecularly dispersed or present in an amorphous form within the carrier. Once the solid dispersion is formed, it is blended with film-forming polymers (e.g., HPMC, PVA) and plasticizers to create a uniform mass. This mixture is then subjected to extrusion using a heated barrel extruder, similar to hot melt extrusion, but with a focus on incorporating the pre-formed solid dispersion rather than melting all ingredients together simultaneously. The extruded mass is passed through a flat die to form thin films, which are then cooled and cut into desired sizes. This method's key benefit is its capacity to keep poorly soluble medications in a more soluble amorphous state, which greatly increases their rate of dissolution. Moreover, this approach provides uniform drug distribution within the film matrix, enhances content uniformity, and eliminates the use of solvents, making the process environmentally friendly. However, it is best suited for heat-stable drugs, as thermal processing is involved. All things considered, the solid dispersion extrusion approach works well for creating fast- dissolving oral films by combining improved solubility with successful film formation.
5) Rolling method
A novel and effective approach for creating mouth-dissolving films, the rolling process is particularly well-suited for large-scale production and medications that are heat-sensitive. Unlike other methods that rely on casting or extrusion, the rolling method involves the continuous feeding of a viscous, drug- loaded film-forming solution or suspension between two rollers that compress and shape the material into a thin, uniform film. The formulation typically consists of a water-soluble polymer (such as hydroxypropyl methylcellulose or polyvinyl alcohol), the active pharmaceutical ingredient, plasticizers, sweeteners, and other additives dissolved or dispersed in a suitable solvent system, often water or hydro- alcoholic mixtures. As the solution passes through the gap between the rollers, it is spread into a consistent film layer, and the mechanical action ensures even distribution of the drug and excipients. After being rolled into a thin sheet, the film is dried using controlled heat and airflow to evaporate the solvent without degrading the drug or altering the film properties. The dried film is then collected, cut into appropriate sizes, and packaged. The rolling method's capacity to create films with exceptional consistency in thickness and drug content is one of its main benefits, along with a smooth texture and high flexibility. Additionally, since the process operates at relatively low temperatures and does not involve high-shear forces, it is well-suited for drugs that are sensitive to heat or mechanical stress. The rolling method also supports continuous manufacturing, making it ideal for commercial production. Overall, this method provides an effective, scalable, and drug-friendly approach to producing high- quality mouth dissolving films.
Evaluation Of Mouth Dissolving Film:
The thickness of mouth dissolving films is a critical physical parameter that directly impacts the drug content uniformity, mechanical strength, and disintegration profile of the film. Uniform thickness is essential to ensure accurate dosing, especially in formulations where the drug is uniformly dispersed throughout the polymeric matrix. Variations in thickness can lead to inconsistency in drug release, reduced efficacy, or potential overdose. To evaluate the thickness, films are typically measured using precise instruments such as a micrometer screw gauge or digital Vernier caliper, which offer accuracy up to 0.01 mm (10 µm). To account for any anomalies in film casting, the measurement is done at several points on the film, usually at the center and at least two to four corners. The ultimate film thickness is stated as the mean of these measurements. The optimal thickness for MDFs typically falls between 50 and 200 micrometers, contingent upon the kind and concentration of polymer employed. Factors such as polymer viscosity, solvent volume, plasticizer content, and drying conditions significantly influence the final thickness of the film. A film that is too thick may disintegrate slowly and cause discomfort in the oral cavity, while an excessively thin film might lack mechanical integrity and tear easily. Therefore, maintaining a uniform and appropriate thickness is essential for both functional performance and patient compliance.
2) Weight Variation:
Weight variation is an essential evaluation parameter for mouth dissolving films (MDFs), as it directly correlates with the uniformity of drug distribution and consistency of dosage. Since MDFs are thin polymeric matrices that carry the active pharmaceutical ingredient (API) uniformly throughout the film, any variation in weight can indicate inconsistencies in the amount of drug present in each unit. This is particularly critical for potent drugs like Vildagliptin, where dose accuracy is crucial for therapeutic efficacy and patient safety. To assess weight variation, individual film samples—typically of uniform size (e.g., 2 cm × 2 cm)—are cut from a larger sheet and weighed using a high-precision analytical balance. Several samples (usually 5 to 10) are weighed, and the mean weight is calculated. Each sample's weight is then compared to the average, and the percentage deviation is determined. According to standard pharmaceutical guidelines, the weight of individual films should not deviate by more than ±5% from the mean weight. Significant deviations may result from improper mixing of the film-forming solution, non-uniform spreading or casting, or inconsistencies in drying. Maintaining consistent weight across all film units ensures not only uniform drug content but also consistent mechanical and disintegration properties. Thus, the evaluation of weight variation serves as a quality control measure to guarantee the reproducibility and reliability of the final product.
3) Folding Endurance:
One important mechanical characteristic used to evaluate the strength and flexibility of mouth dissolving films (MDFs) is folding endurance. It shows if the film can be folded repeatedly in the same place without breaking, which is crucial for guaranteeing the film's longevity during handling, packing, and administration. The dosage and patient experience may be jeopardized if a film with low folding endurance tears or breaks too soon. A particular section of the film, typically measuring 2 cm by 2 cm, is manually folded repeatedly at the same spot until it breaks or exhibits obvious symptoms of cracking in order to assess folding durability. The number of times the film can be folded without breaking is recorded as its folding endurance value. A value greater than 300 folds is generally considered acceptable for a film intended for oral use, although this may vary depending on the film composition and intended application. The flexibility of a film is influenced by the type and concentration of the polymer used, as well as the type and amount of plasticizer, which improves elasticity by reducing intermolecular forces within the polymer matrix. A balance must be maintained; while high flexibility enhances handling, excessive softness may reduce structural integrity. Therefore, folding endurance provides a quick and effective way to screen the mechanical robustness of MDFs and ensures the formulation can withstand normal stresses encountered during production and use.
4) Surface pH:
One of the most important factors in evaluating mouth dissolving films is the surface pH. (MDFs), as it helps predict the potential for mucosal irritation when the film comes into contact with the oral cavity. Since MDFs are intended to disintegrate and dissolve rapidly in the mouth, it is essential that their surface pH is close to the natural pH of saliva, which typically ranges from 6.5 to 7.5. A surface pH that is too acidic or too alkaline can cause discomfort, irritation, or even damage to the delicate mucosal tissues, thereby affecting patient compliance. A tiny section of the film, typically measuring 2 cm by 2 cm, is put in a Petri dish and moistened with a few drops of distilled water or artificial saliva to allow the surface to gently swell without disintegrating in order to determine the surface pH. A pre-calibrated pH electrode or pH indicator paper is then gently placed on the moistened surface of the film, and the pH is recorded after stabilization. Ideally, the surface pH should lie within the neutral range (approximately 5.5 to 7.0), depending on the nature of the polymer and additives used in the formulation. Factors such as the presence of acidic or basic excipients, buffer systems, and the type of drug can influence surface pH. Regular monitoring and adjustment of this parameter during formulation development are vital to ensure the film is non-irritant and safe for oral administration.
4) Appearance and transparency:
The appearance and transparency of mouth dissolving films (MDFs) are important aesthetic and quality attributes that influence patient acceptability and provide an initial indication of the film’s uniformity and integrity. A pharmaceutically elegant film should have a smooth surface, uniform color, and be free from physical defects such as air bubbles, cracks, wrinkles, or uneven edges. These visual characteristics are typically assessed through simple visual inspection under adequate lighting and, in some cases, under magnification. Transparency, on the other hand, is a measure of how much light can pass through the film, andIt displays how evenly the medication and excipients are distributed throughout the polymeric matrix. High transparency often indicates homogeneity and absence of particulate matter, while cloudiness or opacity may suggest poor mixing, drug crystallization, or the presence of incompatible excipients. Transparency can be quantitatively evaluated using a UV-Visible spectrophotometer by measuring the percent transmittance of light at a specific wavelength (usually around 600 nm). A transparent or semi-transparent film is generally preferred for aesthetic reasons and to enhance patient compliance, especially in pediatric and geriatric populations. However, complete transparency is not always required, particularly if the film contains light-sensitive drugs or colored excipients. Overall, the evaluation of appearance and transparency provides a quick and effective assessment of the film's visual quality, formulation homogeneity, and potential patient acceptability.
Tensile Strength: Tensile strength is a critical mechanical parameter used to evaluate the robustness and elasticity of mouth dissolving films (MDFs), reflecting the film's ability to withstand mechanical stress during handling, packaging, and administration. It is defined as the maximum stress that a film can endure while being stretched before it breaks. When a film has sufficient tensile strength, it won't tear easily when handled or inserted into the mouth cavity, which is especially important for ensuring dose integrity. The tensile strength is typically measured using a texture analyzer or universal testing machine, where a strip of the film (commonly 2 cm × 5 cm) is stretched steadily until it breaks while clamped at both ends. The force required to break the film is recorded, and the tensile strength is calculated using the formula:
Tensile Strength (N/mm²) = Force at Break (N)
Cross-sectional Area of the Film (mm²)
The kind and concentration of polymer utilized, the kind and quantity of plasticizer, and the existence of additional additives are some of the variables influencing tensile strength. Polymers such as hydroxypropyl methylcellulose (HPMC), polyvinyl alcohol (PVA), and pullulan provide good film-forming and tensile properties, while plasticizers like glycerin or polyethylene glycol (PEG) enhance flexibility but may reduce strength if used excessively. Ideally, Tensile strength and flexibility should be balanced in a mouth dissolving film to maintain mechanical integrity without sacrificing comfort or disintegration time. Therefore, tensile strength evaluation plays a vital role in the formulation development and quality control of MDFs.
2) Percent Elongation:
Percent elongation is a vital mechanical property used to assess the flexibility and elasticity of mouth dissolving films (MDFs). It indicates a film's capacity to tolerate stress without losing its integrity by measuring the amount of stretch it can withstand before breaking. This characteristic is particularly important for MDFs, as films with poor elongation may crack, tear, or break during handling, packaging, or administration, leading to dose loss and reduced patient compliance. The test is typically performed alongside tensile strength measurement using a texture analyzer or universal testing machine. In this method, a standardized film strip (commonly 2 cm × 5 cm) is fixed between two clamps and stretched until it breaks. The increase in length is recorded, and percent elongation is calculated using the formula:
Percent Elongation = Increase in Length at Break)Original length × 100
Higher percent elongation indicates greater flexibility and ductility, which is often enhanced by the presence of plasticizers like glycerin, polyethylene glycol (PEG), or propylene glycol. However, tensile strength may be weakened by an excessive concentration of plasticizer, thus the ideal balance needs to be preserved. Films with moderate to high elongation values are generally preferred as they are less brittle and more resilient during practical use. Therefore, evaluating percent elongation is essential for ensuring that the MDFs are not only strong but also flexible enough to maintain their form and function throughout their shelf life and during administration.
3) Youngs Modulus:
Young’s modulus, also known as the elastic modulus, is a key mechanical property used to evaluate the stiffness or rigidity of mouth dissolving films. Within the material's elastic limit, it is defined as the ratio of strain (relative deformation) to stress (force per unit area). Essentially, Young’s modulus provides insight into how much a film will deform when a certain amount of force is applied. A higher Young’s modulus indicates a stiffer and less flexible film, while a lower value suggests greater elasticity and flexibility. This parameter is particularly important in MDFs, as the film must be strong enough to resist tearing during handling and packaging, yet flexible enough to conform to the contours of the oral cavity and disintegrate rapidly. Usually, a texture analyzer or universal testing machine is used to do the test. The stress-strain curve is plotted after a standard-sized film strip is clamped and stretched. Young’s modulus is calculated from the initial linear portion of this curve using the formula:

The modulus is influenced by the type and concentration of polymers and plasticizers used in the formulation. Films with high polymer content and low plasticizer concentration generally exhibit higher stiffness, whereas higher plasticizer levels lower the modulus and improve flexibility. An optimal Young’s modulus ensures that the film can be handled easily without breaking while maintaining patient comfort and rapid disintegration. Thus, evaluating Young’s modulus is essential for achieving a balance between mechanical durability and flexibility in mouth dissolving films.
4) Disintegration Time:
The evaluation of disintegration time is a critical quality assessment for mouth dissolving films (MDFs), as it directly determines how quickly the film will disintegrate in the oral cavity and begin releasing the active pharmaceutical ingredient (API). Disintegration time is defined as the time required for a film to completely break apart or dissolve when in contact with saliva or a simulated saliva environment, typically at body temperature (37 ± 0.5°C). A rapid disintegration ideally within 30 seconds to 1 minute—is essential to ensure that the film delivers immediate therapeutic action, particularly for patients who have difficulty swallowing, such as pediatric, geriatric, or bedridden individuals. To evaluate disintegration time, a small square section of the film (commonly 2 cm × 2 cm) is placed in a petri dish or small beaker containing distilled water or a predetermined volume of artificial saliva solution kept at 37°C to replicate physiological conditions. Visual observations of the film are made, and the amount of time it takes for it to totally dissolve without leaving behind any discernible bulk or film residue is noted. In some studies, slight shaking or gentle agitation may be applied to simulate oral movement, although standardized shaking is generally avoided for reproducibility. Several formulation factors influence disintegration time, including the nature and concentration of hydrophilic polymers (e.g., HPMC, PVA, pullulan), the type and amount of plasticizer (e.g., glycerin, PEG), film thickness, as well as the existence of substances that stimulate saliva or super disintegrants. Thinner films and higher concentrations of water-soluble excipients generally lead to faster disintegration. It is important to optimize the formulation to balance rapid disintegration with good mechanical strength and patient acceptability. Overall, disintegration time is a vital parameter for ensuring the effectiveness and performance of MDFs, and therefore needs to be closely assessed and managed throughout the formulation and quality assurance processes.
5) In-Vitro Dissolution Studies:
In-vitro dissolution studies are an essential part of the evaluation of mouth dissolving films (MDFs), as they provide critical information on the rate and extent of drug release from the film matrix under simulated physiological conditions. These research' main goal is to guarantee that the medication is released from the film entirely and quickly after it comes into touch with the oral cavity's moisture, allowing for a quick commencement of action. Since MDFs are designed for quick disintegration and dissolution in the mouth without the need for water, it is important that they release the drug efficiently in a short period. Dissolution testing of MDFs is typically carried out using the USP Type I (basket) or Type II (paddle) dissolution apparatus. The film is usually cut into a specific size equivalent to the unit dose and placed in a suitable dissolution medium, most commonly phosphate buffer of pH 6.8, which simulates the pH of saliva. The temperature is maintained at 37 ± 0.5°C, and the medium is stirred at a controlled speed (commonly 50–100 rpm). Samples are withdrawn at predetermined time intervals (e.g., 0.5, 1, 2, 3, 5, 10 minutes), filtered, and analyzed typically using UV-Visible spectrophotometry orUsing high-performance liquid chromatography (HPLC), the amount of medication released can be measured. The dissolution profile obtained helps in assessing the release kinetics of the drug from the film, which may follow zero-order, first-order, or diffusion-controlled mechanisms depending on the formulation matrix. Factors influencing dissolution include polymer type and concentration, drug solubility, plasticizer content, and film thickness. A rapid and complete drug release (typically more than 80% within 5–10 minutes) is indicative of a well-formulated MDF. In-vitro dissolution studies not only help in optimizing the formulation during development but are also essential for quality control and establishing in-vitro–in-vivo correlations (IVIVC). Thus, they play a crucial role in ensuring the therapeutic efficacy and performance consistency of mouth dissolving films.
A crucial quality control factor in the assessment of mouth-dissolving films is the consistency of the drug content, as it ensures that each film strip delivers the intended dose of the active pharmaceutical ingredient (API) consistently and accurately. Uniform distribution of the drug throughout the film matrix is essential not only for therapeutic efficacy but also for patient safety, especially in low-dose formulations where slight variations can significantly impact clinical outcomes. Content uniformity is particularly important in MDFs due to the thin and lightweight nature of the films, which makes even distribution of the drug a formulation challenge.To assess drug content uniformity, individual film strips (usually of known dimensions and weight, such as 2 cm × 2 cm) are selected randomly from a batch. Each film is dissolved in a suitable solvent or buffer (commonly phosphate buffer pH 6.8 or methanol, depending on drug solubility), and the resulting solution is filtered to remove any particulate matter. The amount of drug contained in each unit is then determined by analyzing the filtrate using a suitable analytical technique, such as High-Performance Liquid Chromatography (HPLC) or UV-Visible Spectrophotometry. The drug content of individual films should ideally fall within the acceptable pharmacopeial range, typically 85% to 115% of the labeled amount, with a relative standard deviation (RSD) not exceeding a defined limit (usually not more than 6%). Factors influencing drug content uniformity include the solubility and homogeneity of the drug in the film-forming solution, the mixing method, viscosity of the casting solution, and the drying technique. Proper optimization of formulation and manufacturing processes is necessary to achieve uniform drug distribution. Overall, content uniformity testing is essential for confirming dosage accuracy, ensuring batch-to-batch consistency, and complying with regulatory quality standards for mouth dissolving films.
7) Moisture content & Moisture uptake:
Moisture content and moisture uptake are crucial parameters in the evaluation of mouth dissolving films as they significantly affect the physical stability, mechanical properties, and shelf life of the films. Moisture content refers to the amount of water present within the film matrix immediately after preparation or during storage, while moisture uptake describes the film’s ability to absorb moisture from the surrounding environment. Both parameters must be carefully controlled to ensure optimal film performance. Moisture content is typically determined using methods such as Karl Fischer titration or by drying the film at a specified temperature (e.g., 105°C) until a constant weight is achieved, allowing the calculation of water percentage lost. Low moisture content is desirable to prevent microbial growth, degradation of moisture-sensitive drugs, and undesirable changes in film texture such as stickiness or brittleness. However, excessively low moisture may cause films to become brittle and prone to cracking. Moisture uptake is evaluated by exposing pre-weighed, dried film samples to environments of controlled relative humidity (usually 75% RH, maintained by saturated salt solutions) at room temperature for a specific duration (commonly 1–7 days). The increase in weight due to moisture absorption is calculated as a percentage of the original dry weight. High moisture uptake may lead to swelling, loss of mechanical integrity, and premature disintegration, negatively impacting the film’s handling and performance. The amount of drug contained in each unit is then determined by analyzing the filtrate using a suitable analytical technique, such as High-Performance Liquid Chromatography (HPLC) or UV-Visible Spectrophotometry, and storage conditions. Polymers like hydroxypropyl methylcellulose and polyvinyl alcohol tend to absorb moisture readily due to their hydrophilic nature. Proper packaging using moisture-resistant materials and optimizing formulation components help control moisture-related issues. Therefore, to guarantee the physical stability, it is crucial to monitor the moisture content and absorption, mechanical strength, and efficacy of mouth dissolving films throughout their shelf life.
8) Swelling Index:
The swelling index is an important parameter in the evaluation of mouth dissolving films as it reflects the film’s ability to absorb saliva or moisture and swell before disintegration, which can influence the rate of drug release and overall patient experience. Swelling behavior indicates how the film interacts with the aqueous environment in the oral cavity, affecting its disintegration time and the drug’s bioavailability. To guarantee that the film swells enough to allow for quick breakdown without becoming unduly sticky or gelatinous, a controlled swelling index is ideal, which could cause discomfort or affect handling. To determine the swelling index, a pre-weighed film sample is placed in a suitable medium, usually simulated saliva or distilled water at 37 ± 0.5°C, andpermitted to swell for a predetermined amount of time, usually a few seconds to several minutes. At predetermined intervals, the film is carefully removed, gently blotted to remove excess surface moisture without squeezing out the absorbed fluid, and reweighed. The swelling index is then calculated as the percentage weight gain in relation to the film's initial dry weight, calculated using:
Swelling Index (%) = [(Wt – W0) / W0] × 100
Where, Wt is the weight of the swollen film at time t and W0 is the initial weight of the dry film.
The swelling index depends on the type and concentration of hydrophilic polymers used in the film formulation, such as hydroxypropyl methylcellulose, sodium starch glycolate, or pullulan, as well as the presence of plasticizers and other excipients. Higher swelling index films usually absorb more moisture, allowing for quicker medication release and breakdown. However, excessive swelling may compromise the mechanical integrity of the film. Therefore, optimizing the swelling index is critical in achieving a balance between rapid disintegration and sufficient mechanical strength, ensuring patient compliance and therapeutic efficacy of mouth dissolving films.
Drug Profile:
Property Description
Chemical Name: Vildagliptin
Chemical Structure:
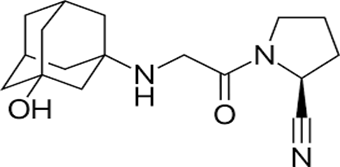
Fig 2.
Structure of Vildagliptin
Molecular Formula: C??H??N?O?
Molecular Weight: 303.4 g/mol
Solubility: Organic solvents such as ethanol, DMSO, and DMF can freely dissolve it; its solubility is approximately 16 mg/ml in ethanol and DMSO and 20 mg/ml in DMF.
Melting Point: 148-152 °C
Appearance: White to off-white solid or powder
Stability: Vildagliptin's stability is susceptible to various environmental factors, including acidic, basic, and oxidative conditions, as well as aqueous environments.
Half-Life: 2-3 hrs
Route of Administration: By Mouth
Absorption:
Vildagliptin is rapidly absorbed from the gastrointestinal tract after oral administration, contributing to its fast onset of action in controlling blood glucose levels in patients with type 2 diabetes mellitus. It has a high oral bioavailability of approximately 85%, indicating efficient systemic absorption. Peak plasma concentrations (Tmax) are typically reached within 1.5 to 2 hours, making it suitable for formulations requiring rapid therapeutic effect. The drug is absorbed mainly in the upper part of the small intestine through passive diffusion, owing to its favorable solubility and molecular properties. Food has minimal impact on the overall extent of absorption (AUC), although it may slightly delay the time to peak concentration, allowing flexibility in dosing with or without meals. These absorption characteristics, along with its low dose requirement, make vildagliptin an excellent candidate for novel dosage forms such as mouth dissolving films, which aim to improve patient compliance and provide quicker relief in diabetic management.
Distribution:
After absorption, vildagliptin is distributed rapidly throughout the body. It exhibits a moderate volume of distribution of approximately 71 liters, indicating its ability to penetrate into various tissues beyond the vascular compartment. Vildagliptin has a relatively low plasma protein binding of around 9.3%, which suggests that a large portion of the drug remains unbound and pharmacologically active in the bloodstream. This low binding also reduces the likelihood of drug-drug interactions related to displacement from plasma proteins. Vildagliptin does not cross the blood-brain barrier in significant amounts, and its distribution is largely limited to peripheral tissues, particularly those involved in glucose metabolism. The favourable distribution profile of vildagliptin contributes to its consistent pharmacokinetics and therapeutic effectiveness in the treatment of type 2 diabetes mellitus.
Metabolism:
Vildagliptin is primarily metabolized through hydrolysis of its amide bond by non-hepatic enzymes, forming the inactive metabolite LAY151. Around 69% of the administered dose undergoes metabolism, with minimal involvement of cytochrome P450 enzymes, which reduces the risk of drug interactions. Most of the drug is eliminated via the renal route, and only a small fraction is excreted unchanged. Its metabolism is predictable and does not produce active metabolites, contributing to its safety and effectiveness in type 2 diabetes management.
Elimination:
Vildagliptin is mainly eliminated through the kidneys, with Approximately 15% of the dose is eliminated in the feces and 85% in the urine. Approximately 23% is excreted unchanged, while The remaining metabolites are removed as inactive ones. The medication's effect on DPP-4 lasts longer while having a brief elimination half-life of roughly three hours, allowing once or twice-daily dosing. Due to its renal clearance, dose adjustments may be needed in patients with kidney impairment.
Therapeutic Class:
Vildagliptin belongs to the therapeutic class of antidiabetic agents, specifically classified as a Dipeptidyl Peptidase-4 (DPP-4) inhibitor. It is used to enhance glycaemic control in the treatment of type 2 diabetes mellitus. By preventing the DPP-4 enzyme from vildagliptin increases the levels of incretin hormones (GLP-1 and GIP), which enhance insulin secretion and suppress glucagon release in a glucose- dependent manner. This mechanism helps lower blood glucose levels without causing significant hypoglycemia.
Mechanism of Action:
Vildagliptin works by selectively inhibiting the enzyme Dipeptidyl Peptidase-4 (DPP-4), which is responsible for the rapid degradation of incretin hormones, primarily glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). Vildagliptin raises these incretin levels and prolongs their activity by inhibiting DPP-4, which enhance glucose-dependent insulin secretion from pancreatic beta cells and suppress glucagon release from alpha cells. This dual action helps lower blood glucose levels effectively, especially after meals, without causing excessive insulin release or hypoglycemia. The glucose-dependent nature of its action makes vildagliptin a safer option for managing type 2 diabetes compared to some other antidiabetic drugs.
Uses & Applications:
Type 2 diabetes is treated with vildagliptin by improving blood sugar control. It can be given alone or with other antidiabetic medications like metformin. Its primary advantage is that it has a minimal chance of producing hypoglycemia while reducing fasting and post-meal glucose levels. It assists people in safely and successfully managing their diabetes. It helps patients manage diabetes effectively and safely.
? Challenges In Formulating Mouth Dissolving Films:
1) Poor Aqueous Stability
One of the significant challenges in formulating modified drug delivery systems (MDFs) with vildagliptin is its poor aqueous stability. Vildagliptin is known to undergo hydrolytic degradation when exposed to moisture, especially under acidic or basic pH conditions. This instability becomes a critical concern during the formulation, processing, storage, and in vivo performance of MDFs, where the drug may be in prolonged contact with water or humidity. Moisture presents in excipients, manufacturing environments, or even within the gastrointestinal tract can trigger degradation, leading to reduced potency, altered release profiles, and compromised therapeutic efficacy. This makes it particularly difficult to use conventional aqueous granulation or coating techniques. To address this, formulators often resort to dry granulation or direct compression methods to minimize water exposure. Additionally, incorporating moisture-barrier packaging, such as aluminium blister packs with desiccants, and using stabilizers or buffering agents in the formulation can help protect the drug from hydrolysis. The need for moisture control at every stage from excipient selection to final packaging makes the development of stable MDFs with vildagliptin a complex and sensitive task.
2) Short Biological Half-Life
After oral administration, the drug is rapidly eliminated from the body, necessitating multiple doses throughout the day to maintain effective plasma concentrations. Frequent dosing not only reduces patient compliance but also increases the risk of fluctuations in blood glucose levels, which is undesirable in managing type 2 diabetes. Modified-release formulations are therefore desirable to prolong the drug's therapeutic effect and reduce dosing frequency. However, designing an MDF that can consistently release vildagliptin over an extended period is challenging due to its high solubility and rapid absorption. Strategies such as the use of hydrophilic matrix systems (e.g., hydroxypropyl methylcellulose), hydrophobic polymers (e.g., ethylcellulose), or osmotic pump systems are employed to control the release rate. These systems simulate several quick release dosages by delivering the medication gradually over a period of 12-24 hours. However, careful polymer selection, process optimization, and a thorough understanding of the drug's pharmacokinetics are necessary to ensure consistent drug release without an initial burst and to maintain stability throughout the release period.
3) High Water Solubility
High solubility is generally favourable for rapid absorption in immediate-release formulations, it poses serious obstacles in sustained or controlled-release systems. In MDFs, highly water- soluble drugs like vildagliptin tend to dissolve quickly upon contact with gastrointestinal fluids, leading to a burst release an initial rapid release of the drug which defeats the purpose of extended drug delivery. This can cause plasma drug levels to spike early, followed by a rapid decline, potentially leading to reduced efficacy or increased side effects. Since water quickly enters the dosage form and dissolves the medication before the controlled-release mechanism can control it, achieving a consistent, extended release becomes challenging. To mitigate this, formulators often use rate-controlling polymers such as ethyl cellulose or Eudragit variants, which create barriers to water ingress and drug diffusion. Alternatively, matrix systems using high-viscosity hydrophilic polymers (e.g., HPMC) can slow drug release by forming a gel layer upon hydration. In some cases, lipid-based systems or drug-resin complexes are also explored to retard the release of water-soluble drugs. However, balancing sustained release with adequate bioavailability remains a formulation challenge, especially with a drug like vildagliptin that is readily soluble in gastrointestinal fluids.
4) Chemical Instability:
Chemical instability is another critical challenge in the formulation of modified drug delivery systems (MDFs) containing vildagliptin. The drug is chemically sensitive and prone to degradation under various environmental conditions, including heat, humidity, light, and oxidative stress. Its molecular structure makes it particularly vulnerable to hydrolytic and oxidative degradation, which can occur during manufacturing, storage, or upon exposure to gastrointestinal conditions. In MDFs, where the drug is expected to remain stable over an extended release period, any chemical breakdown can significantly compromise the safety, efficacy, and shelf life of the dosage form. This instability necessitates strict control over formulation and processing conditions. For instance, exposure to high temperatures during processes like hot-melt extrusion or certain drying methods must be avoided. Antioxidants, buffering agents, or chelating agents are examples of stabilizing techniques that shield the medication from breakdown pathways. Additionally, encapsulation techniques, such as coating with inert polymers or embedding the drug within protective matrices (e.g., lipids or polymers), can help isolate it from harmful environmental factors. Proper packaging using moisture-proof and light-resistant materials like aluminum blisters or amber glass containers is also essential to preserve chemical integrity throughout the product’s shelf life. Thus, ensuring chemical stability in MDFs with vildagliptin requires a holistic approach involving careful material selection, controlled manufacturing processes, and robust packaging solutions.
5) Lack of Strong Binding Sites for Complexation
Complexation techniques, such as those involving cyclodextrins or ion-exchange resins, are commonly used in MDFs to control drug release, enhance solubility, or improve stability. These approaches rely on the drug molecule having functional groups such as aromatic rings, charged moieties, or hydrogen bond donors/acceptors that can interact strongly with the host molecule (e.g., through inclusion complex formation or ionic interactions). However, vildagliptin's molecular structure lacks prominent sites for such interactions, making it poorly suited for forming stable inclusion or ionic complexes. This restriction limits the application of several formulation techniques that would otherwise be useful for altering the release of medications with appropriate chemical characteristics. For example, cyclodextrin-based systems, which can modulate release by trapping the drug in their hydrophobic cavity, are less effective with vildagliptin due to weak affinity. Likewise, ion-exchange resins, which are frequently employed for taste masking or prolonged release, do not efficiently bind vildagliptin because of its neutral or weakly basic nature under physiological pH conditions. As a result, formulators must rely on physical entrapment methods such as polymeric matrices or coated multiparticulate systems to control release, rather than leveraging chemical interactions. This can make the design and optimization of MDFs more complex, as physical methods may not offer the same level of control or predictability as chemical complexation. Therefore, the lack of strong binding sites in vildagliptin adds another layer of difficulty in achieving desired release profiles in modified formulations.
6) Variable Gastrointestinal Absorption
Variable gastrointestinal (GI) absorption presents another significant challenge in formulating modified drug delivery systems (MDFs) for vildagliptin. Although vildagliptin exhibits relatively good oral bioavailability (~85%), its absorption can still vary depending on GI transit time, pH variations, enzymatic activity, and site of release. Vildagliptin is primarily absorbed in the upper part of the gastrointestinal tract, particularly the duodenum and jejunum, where conditions are most favorable for its uptake. In MDFs designed for extended or controlled release, there is a risk that a substantial portion of the drug may be released in distal regions (e.g., ileum or colon), where absorption is less efficient or inconsistent. This variability can lead to fluctuating plasma drug concentrations, potentially reducing therapeutic efficacy or increasing the risk of subtherapeutic exposure. Furthermore, since GI motility varies among patients and is influenced by food intake, disease state (e.g., diabetic gastroparesis), and circadian rhythms, maintaining consistent drug release and absorption becomes even more challenging in MDFs. To address this, formulation strategies may include the development of gastro-retentive systems (e.g., floating tablets or bioadhesive systems) that prolong gastric residence time, ensuring that vildagliptin is released where absorption is optimal. Alternatively, pH-independent release mechanisms using polymers that release drug uniformly across the GI tract can be employed to minimize regional variability. The ultimate objective is to create a delivery method that, in spite of the physiological variability of the gastrointestinal environment, not only prolongs the release of vildagliptin but also guarantees consistent and effective absorption.
Manufacturing Complexity and Cost
Manufacturing complexity and cost represent important practical challenges in formulating modified drug delivery systems (MDFs) for vildagliptin, especially when scaling up for commercial production. MDFs typically require advanced technologies such as multilayer tablet compression, coating, extrusion, or microencapsulation, all of which demand specialized equipment, skilled personnel, and strict process controls. In the case of vildagliptin, these challenges are compounded by the drug’s chemical instability, moisture sensitivity, and need for precise release control, which further increase formulation and processing demands. Maintaining the stability of vildagliptin during manufacturing often requires dry processing techniques (like dry granulation or direct compression) and low-humidity environments, which limit formulation options and raise infrastructure costs. Additionally, achieving controlled release for a highly water-soluble drug like vildagliptin may involve multiple functional excipients—such as rate-controlling polymers, protective coatings, and stabilizers—each contributing to formulation complexity and cost. Quality assurance processes, including in- process testing and validation of release profiles, also become more demanding in MDFs, further increasing production expenses. These factors can limit the feasibility of MDFs in cost- sensitive markets or for generic manufacturers, where economic efficiency is crucial. Therefore, formulation scientists must strike a balance between performance and manufacturability, opting for cost-effective materials and scalable processes without compromising product stability or therapeutic efficacy. Simplifying the design (e.g., using matrix tablets instead of multiparticulate systems) and optimizing process parameters are common strategies to reduce manufacturing burden while still achieving the desired controlled- release profile.
? Recent Studies and Findings:
1. Formulation Strategies and Polymer Innovations
• Polymer Selection and Combination: Recent research emphasizes the use of both natural polymers (e.g., chitosan, pectin, sodium alginate) and synthetic polymers (e.g., hydroxypropyl methylcellulose (HPMC), polyvinyl alcohol (PVA), pullulan). Combining these polymers can balance film strength, flexibility, and rapid dissolution. For example, a study formulated chitosan/pullulan nanofiber films that showed improved mechanical strength and enhanced water solubility, resulting in fast disintegration times without compromising film integrity.
• Plasticizer Optimization: Plasticizers such as glycerol, polyethylene glycol (PEG 400), sorbitol, and triethyl citrate are optimized to improve flexibility and prevent brittleness. Studies indicate that the plasticizer-to-polymer ratio critically influences tensile strength and folding endurance. Films with optimal plasticizer content maintain mechanical strength while dissolving rapidly in the oral cavity.
• Incorporation of Nanocarriers and Nanoparticles: Some recent formulations integrate drug-loaded nanoparticles or nanomicelles into MDFs to enhance drug solubility and bioavailability. For instance, incorporating lipid-based nanoparticles into films has improved the dissolution rate of poorly soluble drugs and offered controlled release profiles.
2. Drug Release Profiles and Pharmacokinetics
• Rapid Disintegration and Drug Release: Studies on drugs like clopidogrel hydrogen sulfate and captopril formulated as MDFs showed rapid disintegration within 10-30 seconds and almost complete drug release (over 90%) within 5 minutes, enabling faster onset of action compared to conventional tablets. This is especially valuable for drugs requiring quick relief, such as analgesics or cardiovascular agents.
• Taste Masking: Since MDFs dissolve in the mouth, taste masking is crucial for patient acceptance. Recent techniques involve using sweeteners, flavouring agents, and inclusion complexes with cyclodextrins to mask bitter or unpleasant drug tastes. Newer approaches also use polymer coatings or microencapsulation within the film matrix to improve palatability.
3. Evaluation and Quality Control
• Mechanical Properties: Tensile strength, elongation at break, and folding endurance are measured to ensure films can withstand handling and packaging stresses. Recent studies recommend standardized testing protocols to compare films and improve reproducibility.
• Disintegration Time: Evaluated using in vitro models simulating saliva conditions, films typically show disintegration times between 10 to 60 seconds. A key trend is developing films with faster disintegration without sacrificing mechanical stability.
• Moisture Uptake and Stability: MDFs are highly sensitive to moisture, which affects mechanical strength and drug stability. New packaging solutions like aluminum blister packs with desiccants are being paired with formulation tweaks (e.g., hydrophobic polymer coatings) to improve shelf life.
4. Clinical and Market Insights
• Patient Compliance and Convenience: Recent clinical studies confirm high patient acceptability for MDFs, especially among children, elderly, and patients with swallowing difficulties. Ease of administration without water and rapid onset of action improve adherence.
• Expanding Therapeutic Areas: MDFs are increasingly being explored for neurological drugs (e.g., anti-migraine, anti-epileptics), cardiovascular agents, and vaccines due to their quick absorption and potential for bypassing first-pass metabolism.
• Market Growth: The global market for oral thin films is expanding rapidly, with an expected CAGR (compound annual growth rate) of around 10-12% over the next 5 years. Industry trends favor combination therapies and personalized medicine delivered via MDFs.
CONCLUSION:
Mouth dissolving films (MDFs) represent an innovative and patient-centric oral drug delivery system, particularly advantageous for drugs like vildagliptin that benefit from rapid onset of action and enhanced patient compliance. This review highlights the significant progress made in the formulation and characterization of vildagliptin-loaded MDFs, including the selection of suitable film-forming polymers, plasticizers, and taste-masking agents to overcome formulation challenges such as chemical instability and bitter taste. The use of hydrophilic polymers like HPMC, pullulan, and natural gums, along with optimized plasticizer concentrations, has been shown to yield films with acceptable mechanical strength, uniform drug content, and fast disintegration times—key parameters for successful MDF development.Evaluation studies, including in vitro disintegration, dissolution, and stability assessments, have demonstrated the potential of these films to deliver vildagliptin effectively and consistently. Although current studies are promising, further research involving in vivo pharmacokinetic and pharmacodynamic evaluations, stability studies under ICH guidelines, and scalability assessments is essential for clinical translation and commercial development. In conclusion, vildagliptin-loaded MDFs offer a promising alternative to conventional dosage forms, particularly for improving therapeutic outcomes and adherence in diabetic patients.
REFERENCES



Gadakh Abhishek*, Dhere Pallavi, Dr. Wagh Jyoti, A Review Article on Development and Characterization of Vildagliptin- Loaded Mouth Dissolving Films, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 506-527. https://doi.org/10.5281/zenodo.16747584
 10.5281/zenodo.16747584
10.5281/zenodo.16747584
