Ali- Allana College of Pharmacy Akkalkuwa, District Nandurbar, MS, India
Transdermal patches distribute the medication through the skin in a precise and controlled manner, hence enhancing the medication's therapeutic efficacy. Triptan is a second-generation triptan with a good tolerance profile and higher patient satisfaction. The aim of the present work was to formulate and evaluate transdermal patches of Triptan. For the current study, the transdermal patch containing drug with different ratios of polymeric combinations and varying plasticizer concentration were prepared. The patch was fabricated by solvent evaporation method. An array of biological, physiological, pharmacological, and biophysical aspects affect how well a transdermal patch works. The stratum corneum's composition, integrity, and thickness must be taken into consideration. Diffusivity can be determined by looking at the molecule's size and structure. It depends on the transdermal drug delivery system's membrane permeability, the pH and moisture level of the skin, as well as other physiochemical drug features.
Transdermal Patch:
A transdermal patch or skin patch is a medicated adhesive patch that is placed on the skin to deliver a specific dose of medication through the skin and into the bloodstream. Often, this promotes healing to an injured area of the body. The first commercially available prescription patch was approved by the U.S. Food and Drug Administration in December 1979 containing scopolamine for motion sickness (1). The highest selling transdermal patch in the United States was the nicotine patch which releases nicotine to help with cessation of tobacco smoking. The first commercially available vapour patch to reduce smoking was approved in Europe in2007. In addition, various other patches are available in market including fentanyl, an analgesic for severe pain, nitroglycerin patches for angina, lidocaine patches, marketed as Lidoderm, relieve the peripheral pain of shingles (herpes zoster), Buprenorphine, marketed as BuTrans, as analgesia for moderate to severe chronic pain. The Duragesic product label was subsequently updated to add safety information inJune 2005. In 2009, the FDA announced a public health advisory warning of the risk of burns during MRI scans from transdermal drug patches with metallic backings. Patients should be advised to remove any medicated patch prior to an MRI scan and replace it with a new patch after the scan is complete. (2)
COMPONENTS OF TRANSDERMAL PATCH:
Polymers are the backbone of a transdermal drug delivery system. Systems for transdermal delivery are fabricated as multilayered polymeric laminates in which a drug reservoir or a drug–polymer matrix is sandwiched between two polymeric layers: an outer impervious backing layer that prevents the loss of drug through the backing surface and an inner polymeric layer that functions as an adhesive and/or rate?controlling membrane.(4)
The most important criteria for TDDS are that the drug should possess the right physicochemical and pharmacokinetic properties. Transdermal patches offer much to drugs which undergo extensive first pass metabolism, drugs with narrow therapeutic window, or drugs with short half-life which causes non? compliance due to frequent dosing. For example, drugs like rivastigmine for Alzheimer’s and Parkinson dementia, rotigotine for Parkinson, methylphenidate for attention deficit hyperactive disorder and selegiline for depression are recently approved as TDDS.
Ideal Properties of Drugs
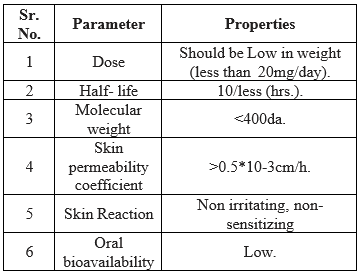
To increase permeability of stratum corneum so as to attain higher therapeutic levels of the drug permeation enhancers interact with structural components of stratum corneum i.e., proteins or lipids. The enhancement in absorption of oil soluble drugs is apparently due to the partial leaching of the epidermal lipids by thechemical enhancers, resulting in the improvement of the skin conditions for wetting and for trans-epidermal and trans-follicular permeation. The miscibility and solution properties of the enhancers used could be responsible for the enhanced transdermal permeation of water soluble drugs.(2)
A PSA maintains an intimate contact between patch and the skin surface. It should adhere with not more than applied finger pressure, be aggressively and permanently tachy, and exert a strong holding force. These include polyacrylates, polyisobutylene and silicon. The selection of an adhesive is based on numerous factors, including the patch design and drug formulation. PSA should be physicochemically and biologically compatible and should not alter drug release. The PSA can be positioned on the face of the device (as in reservoir system) or in the back of the device and extending peripherally (as in case of matrix system). (5)
The primary function of the backing laminate is to provide support. Backing layer should be chemical resistant and excipients compatible because the prolonged contact between the backing layer and the excipients may cause the additives to leach out or may lead to diffusion of excipients, drug or permeation enhancer through the layer. They should have a low moisture vapour transmission rate. They must have optimal elasticity, flexibility, and tensile strength. Examples of some backing materials are aluminium vapour coated layer, plastic film (polyethylene, polyvinyl chloride, polyester) and heat seal layer.
During storage release liner prevents the loss of the drug that has migrated into the adhesive layer and contamination. It is therefore regarded as a part of the primary packaging material rather than a part of dosage form for delivering the drug. The release liner is composed of a base layer which may be non?occlusive (paper fabric) or occlusive (polyethylene and polyvinylchloride) and a release coating layer made up of silicon or teflon. Other materials used for TDDS release liner include polyester foil and metalized laminate.
Various solvents such as chloroform, methanol, acetone, isopropanol and dichloromethane are used to prepare drug reservoir. In addition plasticizers such as dibutylpthalate, triethylcitrate, polyethylene glycol and propylene glycol are added to provide plasticity to the transdermal patch. (11)
Types of Transdermal Patches:
Single layer drug in adhesive;
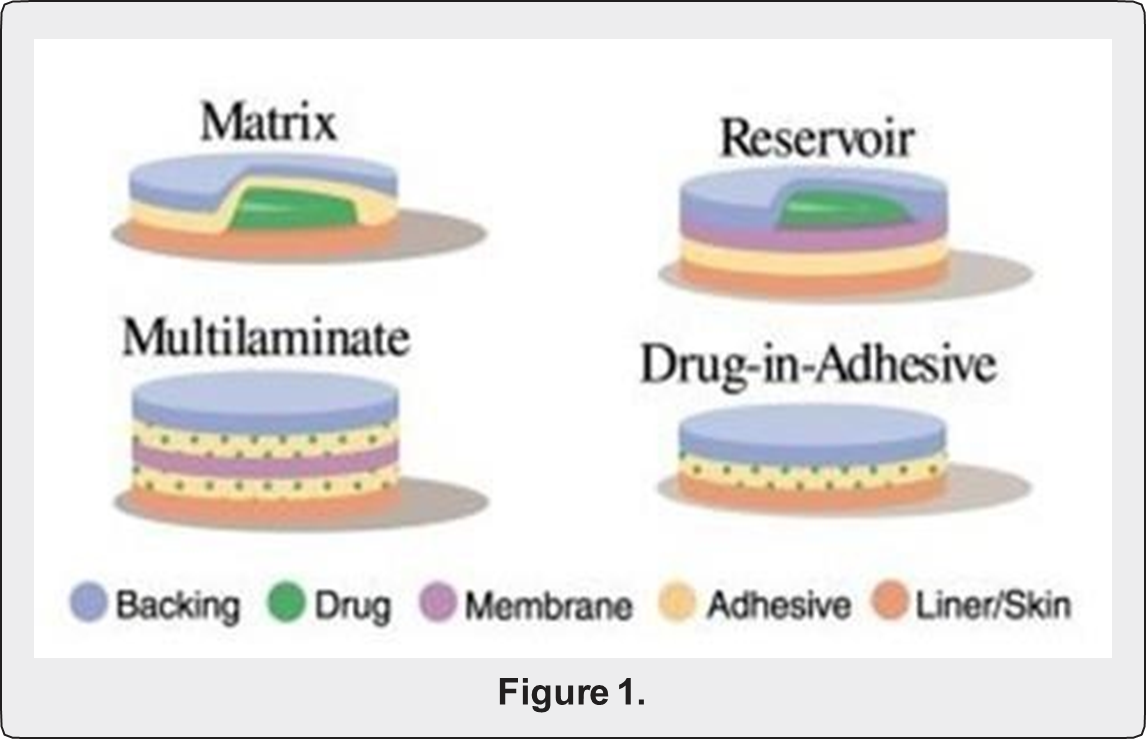
This type is also similar to the single layer but it contains an immediate drug-release-layer and other layer will be a controlledrelease along with the adhesive layer. The adhesive layer is responsible for the releasing of the drug. This patch also has a temporary liner-layer and a permanent backing.
The patch containing the adhesive layer not only serves to adhere the various surfaces together but also serves as to release the vapour. The vapour patches are new to the market, commonly used for releasing the essential oils in decongestion. Various other types of vapour patches are also available in the market which are used to improve the quality of sleep and reduces the cigarette smoking conditions. (5)
In this system the drug reservoir is embedded between an impervious backing layer and a rate controlling membrane. The drug releases only through the rate controlling membrane, which can be micro porous or non-porous. In the drug reservoir compartment, the drug can be in the form of a solution, suspension, gel or dispersed in a solid polymer matrix.(3)
Various methods for preparation of TDDS
Solutions containing polymers in various ratios are used in an organic solvent. Calculated amount of drug is dissolved in half the quantity of same organic solvent. Enhancers in different concentrations are dissolved in the other half of the organic solvent and then added. Plasticizer (e.g., Di-N-butylphthalate) is added into the drug polymer solution. The total contents are to be stirred for 12 hrs and then poured into a circular teflon mould. The moulds are to be placed on a levelled surface and covered with inverted funnel to control solvent vaporization in a laminar flow hoodmodel with an air speed of 0.5 m/s. The solvent is allowed to evaporate for 24 h. The dried films are to be stored for another 24 h at 25±0.5°C in a desiccators containing silica gel before evaluation to eliminate aging effects. These types of films are to be evaluated within one week of their preparation.(12)
A prototype patch can be fabricated for this a heat sealable polyester film (type 1009, 3m) witha concave of 1cm diameter will be used as the backing membrane. Drug sample is dispensed into the concave membrane, covered by a TPX {poly (4-methyl-1- pentene)} asymmetric membrane, and sealed by an adhesive. These are fabricated by using the dry/wet inversion process. TPX is dissolved in a mixture of solvent (cyclohexane) and nonsolvent additives at 60°C to form a polymer solution. The polymer solution is kept at 40°C for 24 hrs and cast on a glass plate to a pre- determined thickness with a gardner knife. After that the casting film is evaporated at 50°C for 30 sec, then the glass plate is to be immersed immediately in coagulation bath (maintained the temperature at 25°C). After 10 minutes of immersion, the membrane can be removed, air dried in a circulation oven at 50°C for 12 h.(12)
The drug is dissolved in polymer solution along with plasticizer. It is followed by stirring for 10- 15 minutes to produce a homogenous dispersion and poured into a levelled mercury surface, covered with invertedfunnel to control solvent evaporation (Wiechers 1992). Rathore et al., (2006) have studied that transdermal matrix type patches of terbutaline sulphate were fabricatedusing ethyl cellulose and cellulose acetate polymer. The transdermal patches of terbutaline sulphate were prepared by solvent casting technique employing a mercury substrate. In the present investigation various polymeric transdermal patches of terbutaline sulphate were prepared. The effect of permeability enhancer on the permeability of drug from cellulose acetate and ethyl cellulose patches was studies.
The drug is dispersed in a mixture of water and propylene glycol containing carbomer-940 polymers and stirred for 12 h in magnetic stirrer. The dispersion is to be neutralized and made viscous by the addition of tri- ethanolamine. Buffer (pH 7.4) can be used in order to obtain solution gel, if the drug solubility in aqueous solution is very poor.(10)
In order to prepare the target transdermal therapeutic system, 1?rbopol reservoir gel, polyethelene (PE), ethylene vinyl acetate copolymer (EVAC) membranes can be used as rate control membranes. If the drug is not soluble in water, propylene glycol is used for the preparation of gel. Drug is dissolved in propylene glycol; carbopol resin will be added to the above solution and neutralized by using 5% w/w sodium hydroxide solution. The drug (in gel form) is placed on a sheet of backing layer covering the specified area. A rate controlling membrane will be placed over the gel and the edges will be sealed by heat to obtain a leak proof device.
Transdermal drug delivery system may produce unstable matrices if the loading dose is greater than 10 mg. Aluminium backed adhesive film method is a suitable one. For preparation of same, chloroform is choice of solvent, because most of the drugs as well as adhesive are soluble in chloroform. The drug is dissolved in chloroform and adhesive material will be added to the drug solution and dissolved. A custom-madealuminium former is lined with aluminium foil and the ends blanked off with tightly fitting cork blocks. Shams et al., (2010) developed medicated films (containing Losartan Potassium - LP) using the polymers, Eudragit E 100 (EE 100)and polyvinyl pyrrolidone VA 64 (PVP VA 64), were prepared in a film casting assembly with aluminium foil. (11)
The proliposomes are prepared by carrier method using film deposition technique. From the earlier reference the drugand lecithin ratio (e.g., 0.1:2.0) may be used as an optimized one. The proliposomes are prepared by taking mannitol powder (e.g., 5 mg) in a round bottom flask which is kept on a heating water bath and the flask is rotated. It is followed by vacuum drying. Drug and lecithin are dissolved in a suitable organic solvent mixture. An aliquot (e.g., 0.5 ml) of organic solution is introduced into the round bottomed flask. After complete drying, second aliquot (e.g., 0.5 ml) of the solution is to be added. (6)
Free film of cellulose acetate is prepared by casting on mercury surface. A polymer solution (e.g., 2% w/w) is prepared using organic solvent (e.g., chloroform). The optimized concentration of plasticizer is incorporated to the polymer solution (e.g., 40% w/w of polymer weight). Small volume (e.g., 5 ml) of polymer solution is poured in a glass ring which is placed over the mercury surface in a glass petri dish. The rate of evaporation of the solvent is controlled by placing an inverted funnel over the petri dish. The film formation is noted by observing the mercury surface after complete evaporation of the solvent.
Merits and Demerits of TDDS
Merits of TDDS
Demerits as well as limitations of TDDS
Factors Affecting Transdermal Patches:
There are various factors which affects the action of transdermal patches.
These are given below:
a. Physicochemical Properties
b. Physiological & Pathological Conditions of Skin
Migraine:
The word "migraine" is derived from the Greek word "hemikrania," which means "half of the skull," because the majority of migraine sufferers will have a unilateral, throbbing or pulsating headache. Frequent migraine symptoms include headache nausea or vomiting, sensitivity to light, sound, or smell, as well as auras—signs of impending headaches. Many people who suffer from migraines wake up in the early morning when their attack is already well underway and accompanied by nausea and vomiting. To treat migraines quickly and effectively, a novel, non-invasive, non-oral administration technique is therefore required. An adhesive patch placed on the skin that contains medication that is intended to be absorbed into the bloodstream through the skin is called a transdermal patch, also known as a skin patch or skin patch. (9)
Preparation Techniques For Transdermal Patch For Migraine Treatment:
The given patch is prepared by Mercury Substrate method. This method is consisting of following steps
Preparation of Transdermal Patch:
Figure 1: Formulation of Transdermal Patch


EVALUATION PARAMETERS.
Physical appearance:
Visual evaluations for colour, clarity, flexibility, and smoothness are made for each prepared patch.
Thickness of the patch:
The thickness of the drug loaded patch is measured in different points by using a digital micrometer and the average thickness and standard deviation is determined to ensure the thickness of the prepared patch. The thickness of transdermal film is determined by traveling microscope dial gauge, screw gauge or micrometer at different points of the film (2).
Weight uniformity:
The prepared patches are dried at 60°c for 4hrs before testing. A specified area of patch is to be cut in different parts of the patch and weigh in digital balance. The average weight and standard deviation values are to be calculated from the individual weights (3).
Folding endurance:
A strip of specific area is to be cut evenly and repeatedly folded at the same place till it breaks. The number of times the film could be folded at the same place without breaking gives the value of the folding endurance (4)
Percentage Moisture content:
The prepared films are to be weighed individually and to be kept in a desiccators containing fused calcium chloride at room temperature for 24 hrs. After 24 hrs the films are to be reweighed and determine the percentage moisture content from the below mentioned formula 2, 13. % Moisture content = Initial weight – Final weight X 100 Final weight (5).
Content uniformity test:
10 patches are selected and content is determined for individual patches. If 9 out of 10 patches have content between 85% to 115% of the specified value and one has content not less than 75% to 125% of the specified value, then transdermal patches pass the test of content uniformity. But if 3 patches have content in the range of 75% to 125%, then additional 20 patches are tested for drug content. If these 20 patches have range from 85% to 115%, then the transdermal patches pass the test.
Moisture Uptake:
Weighed films are kept in desiccators at room temperature for 24 h. These are then taken out and exposed to 84% relative humidity using saturated solution of Potassium chloride in desiccators until a constant weight is achieved. % moisture uptake is calculated as given below 11, 13. % moisture uptake = Final weight – Initial weight X 100 Initial weight. (3)
Drug content:
A specified area of patch is to be dissolved in a suitable solvent in specific volume. Then the solution is to be filtered through a filter medium and analyze the drug contain with the suitable method (UV or HPLC technique). Each valuerepresents average of three different samples (8).
Shear Adhesion test:
Vapour Patch This test is to be performed for the measurement of the cohesive strength of an adhesive polymer. It can be influenced by the molecular weight, the degree of cross linking and the composition of polymer, type and the amount of tackifier added. An adhesive coated tape is applied onto a stainless steel plate; a specified weight is hung from the tape, to affect it pulling in a direction parallel to the plate. Shear adhesion strength is determined by measuring the time it takes to pull the tape off the plate. The longer the time take for removal, greater is the shear strength (11).
Peel Adhesion test:
In this test, the force required to remove an adhesive coating form a test substrate is referred to as peel adhesion. Molecular weight of adhesive polymer, the type and amount of additives are the variables that determined the peel adhesion properties. A single tape is applied to a stainless steel plate or a backing membrane of choice and then tape is pulled from the substrate at a 180º angle, and the force required for tape removed is measured (14).
Water vapor transmission studies (WVT):
For the determination of WVT, weigh one gram of calcium chloride and place it in previously dried empty vials having equal diameter. The polymer films are pasted over the brim with the help of adhesive like silicon adhesive grease and the adhesive was allowed to set for 5 minutes. Then, the vials are accurately weighed and placed in humidity chamber maintained at 68 % RH. The vials are again weighed at the end of every 1st day, 2nd day, 3rd day up to 7 consecutive days and an increase in weight was considered as a quantitative measure of moisture transmitted through the patch. In other reported method, desiccators were used to place vials, in which 200 mL of saturated sodium bromide and saturated potassium chloride solution were placed. The desiccators were tightly closed and humidity inside the desiccators was measured by using hygrometer. The weighed vials were then placed in desiccators and procedure was repeated. WVT = W/ ST W is the increase in weight in 24 h; S is area of film exposed (cm2); T is exposure time.(12)
Future of Transdermal Drug Delivery System;
Future aspects in Drug delivery system include liposomes, Niosomes and micro emulsion. Aim of this development is to improve delivery of drug that has low inherent solubility in most of classical formulation excipients. A wide range of potential drugs for delivery like steroids, antifungal, antibacterial, interferon, methotrexate, local anesthetics are formulated. The market for transdermal patches has been estimated to increase in future and has recently experienced annual growth of at rate of 25%.
CONCLUSION:
In compared to more conventional ways, transdermal drug delivery is a well- established route of administration that offers a number of advantages, including convenience, regulated and sustained distribution, and avoidance of the gastrointestinal tract. Given that the current oral, nasal, and subcutaneous formulations each have their own drawbacks, migraines may find these advantages to be appealing. Triptan is one of the more frequently prescribed migraine treatments, but new technologies, like the Zelrix iontophoresis patch, may provide migraine sufferers other therapeutic options. Only a few research have been done on TDDSs for migraine. However, because of its numerous benefits thathave been demonstrated, it is necessary to further investigate this system and its route of administration because, in addition to being therapeutic.
REFERENCES:

Aasim Shaikh Jameel, Majaz A. Qazi, Shaikh Aatif Jameel, Green Synthesis And Biological Evaluation Of ?, ? - Unsaturated Carbonyl Compounds By Microwave Irradiation And Conventional Methods, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 4, 915-924. https://doi.org/10.5281/zenodo.11046325
 10.5281/zenodo.11046325
10.5281/zenodo.11046325
