
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Dept of Pharmacology, Krupanidhi College of Pharmacy, Bangalore, Karnataka.
Acute pancreatitis (AP) is an inflammatory condition of the pancreas, marked by sudden onset of abdominal pain and, in severe cases, systemic complications such as multi-organ failure and pancreatic necrosis. Recent global data indicate a notable increase in AP incidence, with a 59% rise reported between 1990 and 2021. The highest burden has been observed in regions with high Socio-Demographic Index values, particularly North America and Europe. Gallstone-related biliary obstruction and chronic alcohol use account for the majority of cases worldwide. Additional causes include metabolic disturbances, certain medications, infections, and post-procedural complications, particularly following ERCP. While many cases resolve with supportive care, severe presentations require prompt fluid resuscitation, pain management, and nutritional support. The Revised Atlanta Classification remains the standard for diagnosis and severity stratification. Despite numerous clinical trials, no drug has yet demonstrated definitive efficacy in altering the course of the disease. However, early-phase trials of agents such as CM4620 (a CRAC channel inhibitor) have shown promise. This review consolidates current evidence on the causes, diagnostic approaches, and conservative management strategies for AP, with emphasis on recent developments and the ongoing need for targeted pharmacological therapies.
Acute pancreatitis (AP) refers to an inflammatory disorder of the pancreas clinically presented by visceral pain and systemic malfunctions such as that of multi-organ failure. In advanced cases it has also been reported to induce pancreatic necrosis and organ failure associated with mortality (1). An epidemiological study carried out at a global scale in the year 2024 has marked an upward trend in the global prevalence for pancreatitis cases nearly by fifty nine percent between 1990-2021 and is likely to rise in the coming years. Geographically regions with high Socio-Demographic Index are reported with the greatest burden of pancreatitis (2). Supporting these observations, Xiao et al. reported that the incidence of acute pancreatitis increased by an average of three percent per year between 1961 and 2016. The most significant rises were observed in North America (3.67% annually) and Europe (2.77% annually), whereas the incidence in Asia remained relatively unchanged over the same period (3). The underlying cause of AP has been linked with multiple factors causing premature activation of enzymes that leads to inflammation which may extend locally or systemically. Across the globe, biliary obstruction due to gallstones and chronic alcohol consumption account for approximately seventy to eighty percent of AP cases (4). In addition, several other etiological factors have been identified. Metabolic disorders, particularly hypertriglyceridemia and hypercalcemia, are well-documented contributors. Drug-induced pancreatitis with medications such as azathioprine and diuretics frequently implicated. Infectious agents, including viruses like mumps and cytomegalovirus (CMV), and bacteria such as Mycoplasma and Campylobacter, have also been associated with the onset of the disease. Furthermore, post-procedural pancreatitis, especially following endoscopic retrograde cholangiopancreatography (ERCP) and major abdominal surgeries, represents a significant clinical concern. Less commonly, cases may be linked to pancreatic trauma, structural anomalies such as pancreas divisum, or autoimmune and hereditary forms of the condition (5,6,7). It has been observed that the acute stages of pancreatitis are often mild and self-limiting and with timely fluid resuscitation, pain management and early enteral feeding—mortality can be reduced with minimal complications (8). Despite the presence of several classification systems for the diagnosis and clinical management of acute pancreatitis, the Revised Atlanta Classification (2012) continues to be widely regarded as the gold standard for diagnosis, severity assessment, and clinical decision-making (9). Numerous clinical trials have been conducted to evaluate a wide range of pharmacotherapeutic agents (10,11) for their effectiveness in treating acute pancreatitis; however, most have yielded limited or inconclusive results, with no significant breakthroughs reported to date. Preliminary findings from Phase 2 trials of the CRAC channel inhibitor CM4620 (Auxora) have demonstrated encouraging improvements in clinical outcomes among patients with acute pancreatitis; however, as of mid-2025, the drug has not yet received regulatory approval (12). Though significant progress has been made in understanding acute pancreatitis in recent years, there remains a lack of any globally approved pharmacological therapy capable of altering its natural disease progression marking the need for drug development. The purpose of this review aims to bring together current knowledge for providing a comprehensive summary on recent discovered causes, diagnosis, and non-surgical treatment of acute pancreatitis. It also focuses on outlining the main risk factors, recent updates in diagnostic practices, and the importance of supportive care, which continues to be the mainstay of management in the absence of specific drug therapies.
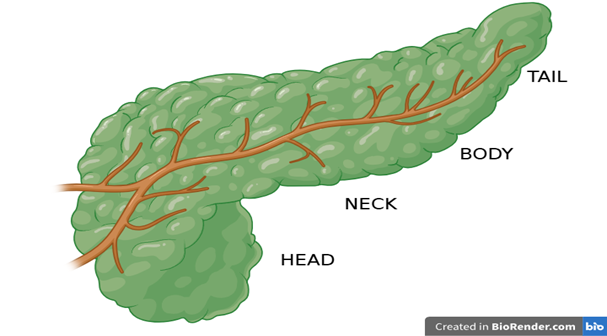
Fig 1. Anatomical Segments of Pancreas.
Structure and Function of the Pancreas
The pancreas is also known as the heterocrine gland, as it serves the dual purpose of both the endocrine and exocrine function and is the 2nd largest gland of the digestive system. The exocrine region of the pancreas is mainly responsible for the production and secretion of digestive enzymes and that of endocrine region is responsible for maintaining the production and balance in the secretion of insulin and glucagon involved in glucose homeostasis. Anatomically pancreas is distinguished into four different segments: the head, neck, body and tail (13) as depicted in Figure 1. The pancreas receives a small amount of blood supply about one percent of cardiac output with arterial supply from the celiac trunk and superior mesenteric artery, and drainage mainly into the portal and splenic veins. A network of looped/arched vasculature supplies the blood to the head segment, while a branched artery from the spleen supplies the body and the tail region (14). A rich network of autonomic fibres from the celiac and superior mesenteric plexuses is supplied to the pancreas innervated to different regions of the gland. Lymphatic drainage occurs via internal and external networks that transport fluid to regionally grouped nodes, with its dysfunction linked to pancreatitis pathogenesis (15). The cellular body of the exocrine region is mainly constituted with zymogen-rich acinar cells that makes up the tubuloacinar gland attached with a duct that drains into the duodenum, facilitating enzyme secretion. The acinar and the ductal cells releases the pancreatic juice mainly consists of bicarbonate and digestive enzymes driven by the hormonal signals essential for neutralization of gastric acid and facilitating nutrient digestion and absorption. The composition of pancreatic juice inculdes ions and proteins like amylase, lipase, trypsin, and nucleases, with secretion impairments leading to mal-absorption syndromes (16).Endocrine secretion occurs from the islets of Langerhans predominantly in the tail of the pancreas, comprising distinct hormone-secreting cells (α, β, δ, and PP cells). α cells located at the periphery contributes to about 20% of cellular composition that secretes glucagon, a peptide hormone which raises blood glucose by promoting glycogen breakdown in the liver, while the β cells located centrally contributes to a maximum of about 80% cellular composition within the islet that produce insulin, a key hormone that facilitates glucose uptake and storage, thus lowering blood glucose levels. The δ cells is distributed in between the α and β cells and contributes to about 5 % of its cellular contribution, these cells release somatostatin, that has an antagonistic effect limited locally on the actions of insulin, glucagon, and pancreatic polypeptide secretion. Pancreatic polypeptide cells are few in number and often found near ducts or in the head of the pancreas. They release pancreatic polypeptide, which modulates exocrine secretion, gallbladder contraction, and gastrointestinal motility. These islets, richly vascularized and comprising ~1.5% of pancreatic volume, regulate glucose homeostasis through hormone release into the bloodstream (13).
Etiology of Acute Pancreatitis
Initially the pathogenetic mechanism of AP was hypothesised to be a result of bile reflux within the common bile duct (17), not sooner but lately a study concluded that migration of gallstones within this duct can lead to AP too (18) and since then a number of other factors have been highlighted. A bias in the gender based disease development was found and it was seen that women are very much prone to developing gallstones than in men where alcohol abuse is a major concern that contributes to the development of AP(19), The above mentioned other factors are described below individually.
Alcoholism
In this present era alcohol consumption is a major issue to be dealt with especially among youngsters however in the pretext of AP chronic alcohol consumption is listed as second most common cause for the development of AP. Retrospective studies have depicted a higher hospital readmission rate among patients with alcohol related AP development primarily due to its relapse (20). Additionally, case reports have highlighted that prolonged alcohol intake can lead to a marked increase in triglyceride levels, a factor that appears to be associated with the onset of AP as discussed in lower sections however, the exact link between hypertriglyceridemia and pancreatitis in the context of alcohol use is still not fully understood. While experimental studies indicate that intracellular enzyme activity might play a role in the degradation of acinar cells, it has not been firmly established as a primary mechanism in the development of alcohol-induced pancreatitis, particularly in relation to autodigestive fat necrosis within the human pancreas (21). This highlights the complex nature of alcohol mediated AP thus emphasizing the on-going need for more deeper and much insightful investigation for having a better understanding of its link and improving therapeutic interventions and strategies.
Cholelithiasis
A recent analysis based on Mendelian randomization showed that there is a existing link between formation of gallstones and the risk for the development of AP and pancreatic cancer. The association was supported across various robust statistical methods, thus highlighting the importance of gallstone in pancreatic disease (22). This was supported by an epidemiologic study which highlighted the presence of gallstones in 1/5 patients characterized with acute alcoholic pancreatitis, also a associated risk of developing pancreatitis was found in patients with gallstones (23). In patients with gallstone associated AP, gallstones were detected in the stools of most cases shortly after symptomatic relief and biochemical normalization. This contrasts sharply with control patients, where stool stones were rare. These findings point to temporary obstruction at the hepatopancreatic ampulla by migrating stones as a likely trigger for pancreatitis (24). Collectively, these observations emphasize the critical role of gallstones in the development of pancreatic disorders. Their involvement ranges from contributing to long-term cancer risk to directly initiating acute inflammation through transient biliary obstruction, making early recognition and intervention in gallstone disease essential for reducing pancreatic complications.
Lipid Profile:
Studies have reported for the existence of a link between hypertriglyceridemia and AP based on case reports. However, the actual risk within the broader population remains unclear (23). A follow up study for a period of 15 years in patients with rising triglyceride levels were strongly linked to increased risk for AP. Individuals with moderate and severe hypertriglyceridemia had 1.5x and 3.2x higher risk respectively. Moderate hypertriglyceridemia accounted for a larger proportion of cases due to its prevalence. Gallstones, renal failure, and chronic pancreatitis were major contributors. Statin use was associated with reduced AP risk (24). With increasing evidence linking hypertriglyceridemia to acute pancreatitis, understanding its causal role has become a subject of clinical interest. One proposed explanation is that extremely high triglyceride levels result in the release of free fatty acids, which may directly damage pancreatic acinar cells and initiate inflammation. Another perspective suggests a gradient of risk, where the likelihood of developing acute pancreatitis escalates progressively with rising triglyceride concentrations, even outside traditionally recognized high-risk groups (25).
Drug Induced Pancreatitis:
One of the underrecognized factor during diagnosis of AP is the use of Drugs that requires precise and important consideration. Subsequently after alcohol abuse, it is considered to be the most commonly identified cause of AP. Thought the onset of drug induced AP may vary after the intake of an offending drug from less than 24 hours to more than a month (26).Data from the FDA Adverse Event Reporting System (FAERS) indicate that 1,175 different medications have been linked to cases of acute pancreatitis. Among these, medications used to treat diabetes—especially metformin, a widely prescribed drug for managing Type II diabetes—had the highest number of reported adverse reactions. Other frequently reported drug groups include medications that suppress the immune system, drugs that affect the central nervous system such as sedatives or antipsychotics, treatments for stomach acid-related conditions (like antacids or acid blockers), and pain relievers (27). With the increasing use of a wide range of medications, including newer treatments like DPP-4 inhibitors and GLP-1 receptor agonists, the risk of drug-induced acute pancreatitis is becoming more relevant in clinical practice (28). Given the potential for serious outcomes, it is important for healthcare providers to consider medication history when evaluating patients with pancreatitis. Recognizing the signs early and discontinuing the suspected drug can significantly improve patient outcomes and help prevent future episodes.
Post- ERCP pancreatitis (Endoscopic Retrograde Cholangiopancreatography Pancreatitis):
Endoscopic retrograde cholangiopancreatography (ERCP) is a widely used procedure essential for diagnosing and treating conditions affecting the bile ducts and pancreas. Although ERCP has been a standard practice for over 40 years, it continues to carry a significant risk of complications, with pancreatitis following the procedure being the most common(29). A review of 145 randomized controlled trials that included placebo or no-stent groups found that post-ERCP pancreatitis (PEP) occurs in 10.2% of cases overall, with the rate increasing with risk of clinical factors to 14.1% among patients (30). The incidence of PEP varies depending on patient-related and procedural risk factors, with reported overall rates ranging from 3% to 15%, and higher rates among high-risk patients. PEP is believed to occur due to a combination of mechanical blockage and/or pressure-related damage, which triggers the premature activation of pancreatic enzymes, causing inflammation both locally and sometimes throughout the body (31). While the risk of death from post-ERCP pancreatitis is low, multiple underlying mechanisms contribute to its development. These include reduced blood flow to the small vessels in the pancreas, ischemic damage, and activation of digestive enzymes triggered by acidosis. Although intravenous fluid resuscitation is commonly used in treatment, its true effectiveness remains unclear, highlighting the need for further research to better understand the role of hydration in managing this condition (32). Understanding the diverse causes of acute pancreatitis is essential for accurate diagnosis and effective management. Recognizing both common and less frequent factors—ranging from gallstones and alcohol use to drug-induced and metabolic causes—helps guide appropriate treatment and prevention strategies, ultimately improving patient outcomes.
Pathophysiology:
Acute pancreatitis results from a complex interplay of genetic and environmental factors. A central component in its pathogenesis is the tightly regulated intracellular calcium signaling within pancreatic acinar cells, where calcium serves as a crucial secondary messenger in the secretion of digestive enzymes. Insults such as gallstone obstruction of the hepatopancreatic ampulla or common bile duct elevate intraductal pressure, facilitating abnormal calcium influx. Concurrently, bile acids activate G-protein-coupled bile acid receptors, stimulating the IP3-DAG signaling cascade, which mobilizes calcium from intracellular stores. The combined effect leads to a sustained rise in intracellular calcium, a key driver of cellular injury (33,34). This calcium overload compromises mitochondrial integrity by enhancing the permeability of mitochondrial permeability transition pores (MPTPs), modulating the function of cyclophilin D and disrupting the mitochondrial membrane potential. As a consequence, ATP production declines, impairing ATP-dependent ion transporters such as the Ca²?/Na? exchangers. The failure of these pumps further amplifies intracellular calcium accumulation (35). The excessive accumulation of intracellular calcium ultimately triggers the premature conversion of trypsinogen to trypsin within pancreatic acinar cells (36). This activated trypsin, along with lysosomal enzyme cathepsin B, contributes to the formation of the necrosis complex comprising RIP1 and RIP3, thereby promoting necroptosis of the acinar cells. Preclinical studies have identified RIPA-56 as a selective inhibitor of RIP1, demonstrating its potential to attenuate TNF-α–induced cell death and mitigate organ damage associated with systemic inflammatory response syndrome (SIRS) (37). Additionally, trypsin initiates autodigestion of pancreatic tissue and compromises lysosomal membrane integrity, resulting in the release of pro-apoptotic factors. This culminates in the activation of the intrinsic apoptotic pathway, specifically through the cytochrome c–caspase cascade, ultimately leading to programmed cell death of the pancreatic cells (38,39,40). Although several pathogenic mechanisms have been implicated in the development of acute pancreatitis—such as impaired autophagy, endoplasmic reticulum (ER) stress, and exosome-mediated signalling —disruption of calcium homeostasis and premature activation of trypsinogen continue to be recognized as central contributors to disease pathogenesis. In acute pancreatitis (AP), both selective and non-selective autophagy processes become activated; however, instead of restoring cellular balance, these pathways often become dysfunctional. Non-selective autophagy engulfs random cytoplasmic content, while selective autophagy targets damaged organelles like mitochondria and the endoplasmic reticulum. A characteristic feature of AP is the accumulation of autophagic vacuoles—autophagosomes and autolysosomes—in pancreatic acinar cells, which reflects a disruption in autophagic flux. Key regulatory proteins such as LC3, ATG5, ATG7, and VMP1 are essential for autophagosome formation, and their altered expression is linked to inflammation and fibrosis in the pancreas. Moreover, non-coding RNAs, including microRNAs like miR-141, miR-148a, miR-155 and long non-coding RNAs like FENDRR, influence autophagy by modulating genes involved in autophagy initiation, such as Beclin-1, ATG7, and mTOR. Compromised lysosomal function further aggravates autophagy failure, as seen in decreased LAMP1/2 expression, impaired cathepsin activity, and unstable lysosomal membranes, all of which contribute to premature trypsin activation and acinar cell damage. Regulatory proteins including TFEB, AMPK, SIRT1, and Galectin-9 also play vital roles in maintaining lysosomal integrity and autophagy progression. Additionally, mutations like those affecting the GNPTAB gene impair lysosomal enzyme trafficking, while mitochondrial dysfunction—especially through cyclophilin D-mediated mPTP opening—disrupts cellular energy balance and further impairs autophagic flux. Altogether, the breakdown in autophagy mechanisms leads to cellular stress, enzyme activation, and inflammation, underscoring its critical role in the development and severity of acute pancreatitis (41,42). Endoplasmic reticulum (ER) stress is yet another mechanism involved in the pathogenesis of acute pancreatitis. ER stress arises from the calcium overload which leads to premature activation of trypsin along with the upregulation of inflammatory and apoptotic cascade resulting in inflammation and cellular death of the pancreas (43). The major mechanism involved is known to be the action of c-Jun and cathepsin B pathway for its trypsinogen activation process that leads to necrosis (38). Additionally, Pre-clinical studies has shown the existing relationship between ER stress and necroptosis, a new pathway associated with TNF alpha induced necroptosis of pancreatic acinar cells which also highlights the potential for identifying newer therapeutic target (44). The development of acute pancreatitis has been linked to polymorphisms in the promoter regions of genes encoding inflammatory cytokines such as IL-1β, IL-6, IL-8, and IL-10, which are considered potential risk factors. Notably, a moderate increase in risk has been associated with the IL-8 -251T polymorphism, whereas other variants have not shown similar associations (45). Among genetic factors, mutations in the cationic trypsinogen gene (PRSS1) are the most commonly implicated in hereditary pancreatitis, as they lead to premature activation of trypsinogen. In addition, variations in genes such as serine protease inhibitor Kazal type 1 (SPINK1), carboxypeptidase A1 (CPA1), the CEL-HYB1 allele of carboxyl ester lipase, and chymotrypsinogen C (CTRC) have also been associated with susceptibility to acute pancreatitis (46).
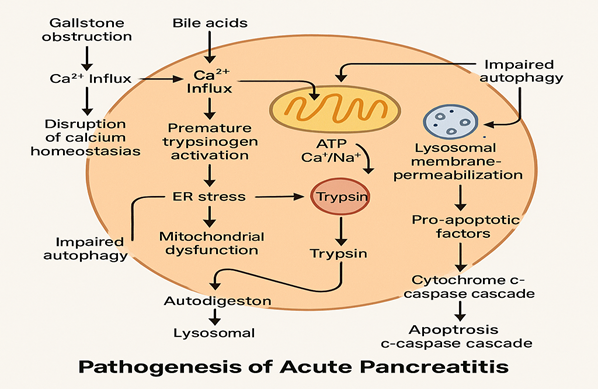
Figure 2: Pathogenesis of AP
Diagnostic Challenges & Approaches
Current diagnostic criteria for Patients with Acute pancreatitis presents themselves clinically with major complaints of pain arising from the upper central region of the abdomen where the pancreas are located followed by complaints of emetic sensation and emesis, secondary symptoms include feeling of abdominal tightness, fever, irritability, low oxygen saturation etc. Biochemical markers include findings of serum amylase/lipase levels 3-fold more than normal and findings consistent for pancreatitis based on abdominal imaging (computed tomography (CT) or magnetic resonance imaging (MRI) or transabdominal ultrasound (TUS)) (47). The major diagnostic challenge in acute pancreatitis lies in distinguishing it from other conditions that present with similar clinical features. The classical symptom of severe, radiating epigastric pain may also occur in disorders such as peptic ulcer disease, cholecystitis, or even myocardial infarction, making differential diagnosis essential. As such, confirmatory biochemical and imaging studies are critical to establishing an accurate diagnosis. Serum amylase and lipase are routinely utilized in clinical practice; however, their diagnostic sensitivity is imperfect. Approximately 20–30% of patients—particularly those with delayed presentation, hypertriglyceridemia, or chronic pancreatitis—may have normal amylase levels. Moreover, elevated enzyme levels may be misleading in non-pancreatic conditions such as renal failure and perforated peptic ulcers (48). Contrast-enhanced computed tomography (CT) is a key tool for evaluating pancreatic necrosis and local complications. Nevertheless, when performed within the first 48 to 72 hours of symptom onset, CT may fail to detect necrotic changes, potentially underestimating the severity of inflammation (49). Ultrasound is the preferred initial imaging modality for assessing gallstones, one of the leading causes of acute pancreatitis. However, its diagnostic utility can be significantly limited in patients with obesity or excessive bowel gas, which may obscure pancreatic visualization (Medscape; Radiology Assistant). Regarding etiology, gallstones and chronic alcohol consumption account for approximately 70–80% of cases. About 10% remain idiopathic after initial evaluation, while other contributors include medications, abdominal trauma, and metabolic disturbances such as hypertriglyceridemia (50). Accurate early severity assessment remains a clinical challenge. Although scoring systems such as Ranson’s criteria, BISAP, and APACHE II are widely used, their predictive accuracy can be variable. The CT Severity Index (CTSI) provides a more detailed assessment by quantifying pancreatic necrosis and peripancreatic involvement but is most informative when CT imaging is delayed beyond 72 hours after symptom onset (51). Although serum amylase and lipase are commonly used to diagnose acute pancreatitis, they provide limited information about disease severity in the early stages. New research has pointed to several biomarkers that show promise for early assessment. For instance, higher levels of interleukin-6 (IL-6) and procalcitonin within the first two days after symptom onset are linked to more severe inflammation and worse outcomes. Additionally, proteins associated with neutrophil activity, like calprotectin (S100A8/A9), and changes in circulating microRNAs may help identify patients at greater risk early on. According to a 2023 review by Smith and colleagues, using these biomarkers alongside clinical scoring systems enhances the ability to predict complications and mortality in acute pancreatitis. However, more studies involving larger patient groups are necessary before these markers can be widely adopted in clinical practice (52). New biomarkers are being studied to better predict the severity of acute pancreatitis, as traditional tests like amylase and lipase have limitations. Recent research by Nesvaderani et al. identified a set of four genes—S100A8, S100A9, MMP25, and MT-ND4L—that may help identify patients at risk of severe disease. Inflammation-related markers such as interleukin-6 and tumor necrosis factor-alpha also show promise in assessing disease progression. Markers related to immune cell activation and mitochondrial function have been linked to worse outcomes. Although these findings are encouraging, more studies are needed before these biomarkers can be routinely used in clinical practice. Incorporating them could improve early diagnosis and treatment, reducing complications (53).
Conservative Management Strategies
In addition to invasive treatments, there has been progress in identifying non-invasive approaches that allow for less aggressive management. Early-stage care generally includes fluid replacement, infection prevention, nutritional support, and pain relief. Recent advances in acute pancreatitis management favour less aggressive treatments focused on safety and efficiency. Moderate fluid resuscitation with Ringer’s lactate is now preferred, aiming to restore volume without causing fluid overload or worsening organ dysfunction. Early “on-demand” oral feeding helps maintain gut integrity and shortens hospital stays by preventing complications from fasting. A multimodal pain management approach, including epidural analgesia, effectively controls pain while minimizing opioid-related side effects. Routine prophylactic antibiotics are discouraged; instead, biomarkers like procalcitonin guide targeted use, reducing resistance and adverse effects. Infected necrosis should be managed conservatively with antibiotics when possible—delaying drainage lowers the risk of invasive complications. When drainage is necessary, less invasive methods like lumen-apposing metal stents reduce surgical burden. Immunomodulatory therapies, though promising in theory, have yet to yield consistent benefits in trials. Preventing post-ERCP pancreatitis relies on proven strategies like high-dose rectal NSAIDs and duct stenting to lower inflammation and injury risk. Overall, these evolving strategies aim to optimize outcomes while avoiding overtreatment (54). Even though Recent randomized controlled trials in acute pancreatitis have questioned several established management strategies, particularly regarding fluid resuscitation, antibiotic use, treatment of infected necrosis, and the early application of endoscopic retrograde cholangiopancreatography (ERCP) (55). Minimally invasive techniques—such as laparoscopic surgery, percutaneous drainage, and endoscopic necrosectomy—are now preferred for managing pancreatic necrosis, especially after 4 weeks when the necrotic tissue is better organized. The step-up approach, starting with drainage and escalating to surgery only if needed, has shown lower complications and mortality than open surgery. Endoscopic methods have shown comparable or superior outcomes to surgery in recent trials. Not all cases require intervention; many patients, especially with sterile necrosis, recover with supportive care alone. Treatment should be individualized and managed in experienced centers for best outcomes (56). Ultimately, careful timing and an individualized approach, supported by experienced teams, are key to achieving the best outcomes in patients with pancreatic necrosis.
CONCLUSION
To sum up, acute pancreatitis continues to pose a significant health burden worldwide, with incidence steadily increasing. While supportive care has improved outcomes, no specific medical therapy has yet proven effective in altering disease progression. Early recognition and careful management remain vital. New insights into biomarkers and less invasive treatments are encouraging. Ongoing research is crucial to develop targeted therapies and improve patient care.
REFERENCES



G. Yamini Durga*, Rohit Chettri, Anjali Yadav, A Review on Acute Pancreatitis: 2025 Update, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 2685-2698. https://doi.org/10.5281/zenodo.16151236
 10.5281/zenodo.16151236
10.5281/zenodo.16151236