Department of pharmacy practice, Malla Reddy Institute of Pharmaceutical sciences, Maismmaguda, Telangana.
Chrono-therapeutics, the strategic timing of medication administration to align with the body's circadian rhythms, has emerged as a promising approach to enhance therapeutic efficacy and minimize adverse effects in various diseases. This review delves into the application of chrono-therapeutics in cancer and chronic diseases (CVDs, Diabetes) highlighting the underlying mechanisms, clinical evidence, and potential benefits. By examining studies from 2004 to 2025, we aim to provide a comprehensive understanding of how circadian biology influences disease progression and treatment outcomes, and how chronotherapy can be integrated into clinical practice.
The human body operates on a 24-hour cycle known as the circadian rhythm, which regulates various physiological processes, including hormone secretion, metabolism, and cellular functions. Disruptions in these rhythms have been linked to the pathogenesis of several diseases, notably cancer and few chronic diseases. Chronotherapy leverages the knowledge of circadian biology to optimize the timing of drug administration, aiming to maximize therapeutic benefits while reducing toxicity.
1. Chronotherapy
Chronotherapy is the science of synchronizing medical treatment with the body's biological rhythms to enhance therapeutic efficacy and minimize adverse effects. Unlike standard dosing regimens that disregard daily biological rhythms, chronotherapy exploits circadian changes in how drugs are absorbed, processed, and how targets respond, aiming to enhance therapeutic effectiveness. [1,2] This approach has gained traction in managing chronic diseases such as cancer, cardiovascular disorders, and diabetes, where both disease activity and drug response exhibit time-of-day dependence.[3] By aligning drug delivery with biologically favourable windows, chronotherapy offers a personalized and physiologically attuned strategy for disease management.
2. Circadian Rhythm
The circadian rhythm is an endogenous, approximately 24-hour cycle that governs a wide array of physiological processes, including sleep–wake cycles, hormone secretion, metabolism, immune function, and cellular repair.[4,5] This rhythm is orchestrated by the suprachiasmatic nucleus (SCN) in the hypothalamus, which synchronizes peripheral clocks in tissues such as the liver, pancreas, and heart through neural and hormonal signals.[6] At the molecular level, circadian rhythms are maintained by transcriptional–translational feedback loops involving core clock genes such as CLOCK, BMAL1, PER, and CRY.[7] These genes regulate downstream pathways that influence drug targets, metabolic enzymes, and inflammatory mediators—making circadian biology a critical determinant of pharmacological response.
Table 1. Physiological function under circadian control [8]
|
Cortisol (stress hormone) peak |
~6–8 AM |
|
Blood pressure peak |
~7–9 AM |
|
Melatonin secretion starts |
~9 PM |
|
Body temperature lowest |
~4 AM |
|
Highest alertness |
~10 AM |
|
Highest alertness |
~5 PM |
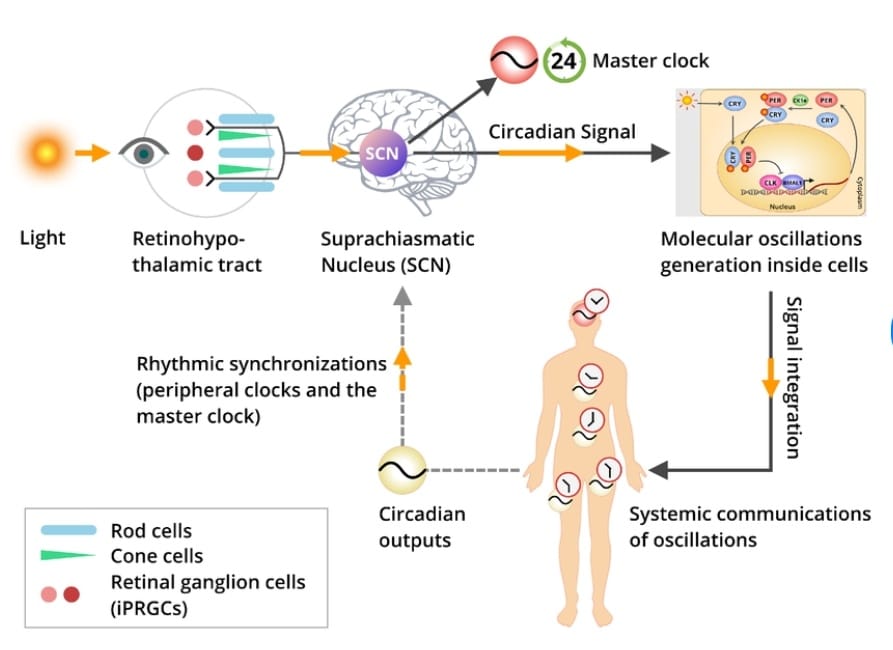
Figure 1. Signal transduction pathway [9]
3. Disease Physiology and Circadian Disruption
Disruption of circadian rhythms—whether due to lifestyle factors like shift work or intrinsic dysfunction—has been implicated in the pathogenesis of numerous chronic diseases. In cardiovascular disorders, circadian misalignment contributes to morning surges in blood pressure and platelet activity, increasing the risk of myocardial infarction and stroke.[10] In diabetes, circadian disruption impairs insulin secretion, glucose tolerance, and hepatic glucose output, exacerbating metabolic dysregulation.[11] In cancer, dysregulated clock gene expression alters cell cycle control, DNA repair, and apoptosis, promoting tumorigenesis and resistance to therapy.[12] These pathophysiological links underscore the rationale for integrating chronotherapy into clinical practice, not only to improve drug efficacy but also to restore circadian homeostasis.
Chrono-therapeutics in Cancer
Cancer is a profoundly circadian-influenced disease, with both tumour biology and treatment response exhibiting time-of-day variability. The circadian clock regulates key cellular processes such as DNA repair, apoptosis, cell cycle progression, and immune surveillance—all of which are critical in oncogenesis and cancer therapy.[12] Disruption of core clock genes like PER2, BMAL1, and CLOCK has been associated with increased tumorigenesis, altered p53 signaling, and impaired DNA damage response, underscoring the role of circadian dysregulation in cancer development. [7]. Chronotherapy in oncology takes advantage of these time-dependent patterns by delivering chemotherapy when cancer cells are at their most vulnerable and normal tissues are least likely to experience damage. At the molecular level, circadian oscillations in drug-metabolizing enzymes (e.g., CYP450s, UGTs), transporters (e.g., ABCB1), and DNA repair proteins (e.g., ATM, CHK2) further influence chronopharmacokinetic and chrono toxicity.[13] Despite compelling evidence, clinical implementation of cancer chronotherapy remains limited due to logistical challenges, interindividual variability in circadian phase, and lack of standardized protocols. However, advances in wearable circadian monitoring, AI-driven dosing algorithms, and personalized chrono biomarkers hold promise for integrating chronotherapeutic into routine oncology care. Ultimately, aligning cancer treatment with the body’s internal clock offers a powerful strategy to enhance efficacy, reduce toxicity, and personalize therapy in a disease where timing may be as critical as the drug itself. Cancer treatment often involves chemotherapy, which can have severe side effects. Chronotherapy has been investigated to enhance the efficacy and tolerability of anticancer agents.
Colorectal Cancer: Studies have demonstrated that administering chemotherapy drugs like 5-fluorouracil (5-FU) and oxaliplatin at specific times can reduce toxicity and improve outcomes. For instance, chrono modulated infusion schedules administering these drugs during the early night, when the body's detoxification processes are most active, have shown reduced gastrointestinal toxicity and improved patient outcomes.[14]
Breast Cancer: In breast cancer, timing chemotherapy to the body's circadian rhythms has been shown to minimize toxicity and maximize efficacy. For example, administering doxorubicin during the late rest phase or early activity phase can enhance therapeutic outcomes and reduce adverse effects.[15]
Lung Cancer: For non-small cell lung cancer (NSCLC), timing platinum-based chemotherapies like cisplatin and carboplatin during the evening can reduce renal damage due to the circadian regulation of renal function.[16]
Immune Checkpoint Inhibitors (ICIs): Emerging evidence suggests that the efficacy of ICIs may be improved by administering treatment at specific times of the day. Studies indicate that the time of day at which ICI therapy is administered can significantly influence its efficacy and potentially associated toxicities.[17]
Table.2 Time Dependent Chemotherapy Benefits [18,19]
|
Drug |
Best Time of Administration |
Benefit |
|
5-Fluorouracil (5-FU) |
Late night (around 4 AM) |
Reduced GI and haematological toxicity |
|
Oxaliplatin |
Afternoon to evening |
Reduced neurotoxicity |
|
Cisplatin |
Morning |
Improved tolerability |
|
Cyclophosphamide |
Evening |
Reduced cardiotoxicity |
Chrono-therapeutics in Cardiovascular Diseases
Cardiovascular diseases (CVDs) such as myocardial infarction (MI), hypertension, and heart failure exhibit strong circadian patterns in both symptom onset and physiological regulation, making them ideal candidates for chronotherapeutic strategies. Epidemiological studies have consistently shown that the incidence of MI, sudden cardiac death, and stroke peaks in the early morning hours—between 6 AM and 12 noon—coinciding with a surge in sympathetic activity, cortisol secretion, platelet aggregability, and vascular tone.[10] This morning vulnerability is particularly pronounced in hypertensive individuals, where abrupt increases in blood pressure (BP) and heart rate elevate cardiovascular risk. Chronotherapy aims to counteract these fluctuations by aligning drug administration with the body’s biological rhythms
Myocardial infarction follows a well-documented circadian pattern, with peak incidence occurring in the early morning hours between 6 AM and 12 noon. This timing corresponds with abrupt increases in blood pressure, heart rate, vascular tone, and platelet aggregability—all driven by heightened sympathetic activity and surges in cortisol and catecholamines.[10] The increased morning platelet reactivity and diminished fibrinolytic activity potentiate thrombus formation, making timing-critical interventions highly relevant. Chronotherapy in MI prevention involves administering antiplatelet agents such as aspirin at bedtime to maximize its effect during the high-risk early morning window. Studies have shown that evening aspirin dosing enhances inhibition of platelet aggregation during these hours, thus reducing thrombotic risk. Statins, particularly short-acting ones like simvastatin, are also more effective when taken at night due to alignment with nocturnal hepatic cholesterol synthesis peaks.[19] These strategies tailor secondary prevention of myocardial infarction by accounting for the time-related patterns of cardiovascular risk.
Hypertension is a prototypical chronotherapy target due to its clear 24-hour variation in blood pressure, with a nocturnal decline (dipping) in normotensive individuals and a morning surge upon awakening. Non-dippers or reverse dippers—commonly seen in diabetics, elderly, and patients with renal disease—are at higher risk for cardiovascular complications. Chronotherapy aims to reestablish the dipping pattern and blunt the morning surge by administering antihypertensives at bedtime. The MAPEC and Hygia Chronotherapy Trials showed that nighttime dosing of various drug classes (ACE inhibitors, ARBs, calcium channel blockers) improved 24-hour BP control and significantly reduced cardiovascular events, including stroke and heart attack.[20] Studies on controlled-onset extended-release formulations, particularly of calcium channel blockers like verapamil and diltiazem, have demonstrated enhanced nocturnal BP control and improved heart rate–BP product when dosed at bedtime.[21,22,23,24] White et al. reported that COER-verapamil taken at night significantly reduced morning BP surges in nondippers, with greater efficacy than conventional morning dosing or comparator drugs like nifedipine GITS.[25,26] Similar chronopharmacological benefits were observed with ramipril, where evening dosing provided more sustained 24-hour BP coverage compared to morning administration.[27,28] In patients with renal impairment, isradipine showed a time-dependent effect in controlling nocturnal hypertension when dosed appropriately.[28] Furthermore, graded-release diltiazem and bedtime aspirin were shown to attenuate morning peaks in BP and platelet activity, reducing thrombotic risk.[28] These findings collectively underscore that the timing of drug delivery—especially when aligned with circadian BP rhythms—can enhance antihypertensive efficacy and lower cardiovascular risk profiles, particularly in patients with disrupted dipping patterns or elevated morning pressures.
Table 3. Clock-based treatment strategy:[29]
|
Bedtime ARB/ACE-1 |
Better nocturnal BP control (-5mm Hg SBP) |
|
Single drug at bedtime |
Converts non?dipper to dipper (↑ BP control 37%) |
|
MAPEC trial |
~67% reduction in CV events |
|
Hygia trial |
45% drop in CV outcomes, –3.3?mm?Hg night SBP |
Heart failure (HF) involves maladaptive activation of neurohormonal systems—such as the renin–angiotensin–aldosterone system (RAAS) and sympathetic nervous system—that also follow circadian patterns. Nocturnal surges in norepinephrine, cortisol, and aldosterone exacerbate volume overload and ventricular remodeling, worsening HF symptoms and outcomes. Chronotherapy in HF targets these pathophysiological rhythms by timing beta-blockers and RAAS inhibitors to suppress nighttime neurohormonal activity. Evening dosing of ACE inhibitors like enalapril has shown improved hemodynamic response, natriuresis, and attenuation of sympathetic overdrive.[30] Additionally, chronopharmacological adaptation of diuretics or neprilysin inhibitors may improve sleep quality by reducing nocturnal dyspnea while preserving diurnal electrolyte balance. While there are fewer clinical studies on chronotherapy in heart failure compared to hypertension or myocardial infarction, growing evidence indicates that timing medication to biological rhythms may lower hospitalization rates and enhance cardiac function.
Chrono-therapeutics in Diabetes Mellitus
Diabetes mellitus, particularly type 2, is a chronic metabolic disorder intricately regulated by the body’s circadian system. The orchestration of glucose metabolism, insulin secretion, and energy homeostasis is influenced by both central and peripheral clocks, with the pancreatic β-cell clock playing a pivotal role.[11] Circadian fluctuations in insulin sensitivity and glucose tolerance—typically highest in the morning and declining by evening—underscore the temporal nature of metabolic control. The “dawn phenomenon,” a surge in early morning glucose levels, is driven by circadian-regulated hormones such as cortisol and growth hormone.[31] Disruption of these rhythms, as seen in shift workers or individuals with sleep disturbances, has been linked to impaired insulin signalling, β-cell dysfunction, and increased risk of metabolic syndrome and diabetes. This has paved the way for chronotherapy in diabetes management, wherein the timing of pharmacologic interventions is aligned with biological rhythms to optimize outcomes. Metformin, the cornerstone of type 2 diabetes therapy, demonstrates enhanced suppression of nocturnal hepatic glucose output when taken in the evening, improving fasting glucose control. Similarly, time-targeted insulin regimens, particularly those addressing pre-dawn hyperglycaemia, can mitigate the dawn phenomenon and reduce glycemic variability. Emerging research also suggests that the efficacy of GLP-1 receptor agonists and DPP-4 inhibitors may be modulated by administration timing, although standardized protocols are yet to be established.[32] At the molecular level, core clock genes such as BMAL1, CLOCK, PER, and CRY are intricately involved in pancreatic β-cell function and insulin exocytosis. Preclinical models show that disruption of these genes impairs glucose tolerance and promotes insulin resistance. Beyond pharmacotherapy, behavioral interventions like time-restricted feeding and circadian-aligned meal timing—collectively termed chrono nutrition—are gaining traction for their potential to enhance glycemic control and reduce systemic inflammation. Technological innovations such as pulsatile insulin pumps, smart insulin pens, and nanocarrier-based drug delivery systems are being developed to mimic endogenous insulin rhythms and deliver antidiabetic agents in synchrony with circadian glucose fluctuations.[33]
Chronotherapy in Asthma.
Asthma is a condition of the inflammatory airways where airflow is blocked by bronchoconstriction and increased mucus secretion, which causes inflammation of the bronchial walls. Asthma is characterized by exacerbations that worsen overnight and peak in the early morning. In asthma, nocturnal symptoms are typically observed and are thought to be significant while determining the timing of treatment.[34] Nocturnal symptoms such as coughing, wheezing, and dyspnoea are common in asthmatic patients, Sleep interruption may result from these symptoms. Additionally, lung function exhibits a circadian cycle, with the earliest hours of the day showing the lowest lung functionality. When compared to morning dosing, these characteristics imply that evening ICS (inhaled corticosteroid) dosing might have a greater effect.[35] The lungs and airways absorb a portion of the ICS, which is then ingested and absorbed into the systemic circulation. After ICS medication, endogenous cortisol levels are suppressed, which indicates an impact on the hypothalamic-pituitary-adrenal (HPA) axis and undesirable systemic activity. An ICS administered once daily (QD) in the afternoon or early evening is linked to the least amount of cumulative cortisol suppression. For individuals with persistent asthma, mometasone furoate delivered by dry powder inhaler (MF-DPI) is an ICS that is authorized for once-daily evening delivery as controller therapy.[36] Other ICS include Triamcinolone acetate increased morning and evening PEF similarly when taken four times a day (800 μg/day) or as a single dose at 5:30 pm, but not when administered as a single dose at 8:00 am. The morning PEF was better when ciclesonide was taken once a day in the evening than when it was administered only in the morning.[37] dose of prednisone was more effective than the same dose administered at 8:00 a.m. and 8:00 p.m. in improving lung function and reducing airway inflammation.[38] β2-agonists (BAs) mainly relax the smooth muscle in the airways, which raises the diameter of the airways and eases bronchoconstriction. BAs with anti-inflammatory properties include fenoterol and procaterol, The levels of plasma epinephrine exhibit a circadian cycle, peaking at 4 pm and falling at 4 am.[39]
CONCLUSION
Chronotherapeutics offers a promising approach to enhance the efficacy and safety of treatments for cancer and cardiovascular diseases by aligning therapy with the body's natural rhythms. Clinical evidence supports the benefits of timing medication administration to circadian patterns, leading to improved outcomes and reduced side effects. Further research is needed to personalize chronotherapy strategies and integrate them into standard clinical practice.
REFERENCES





Dr. Sadanandam A., Pooja A., Komsani Preethi, Radha M., Varshitha V., A Review on Chrono-therapeutics In Cancer and Chronic Diseases, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 2266-2274 https://doi.org/10.5281/zenodo.16924561
 10.5281/zenodo.16924561
10.5281/zenodo.16924561
