
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Biotechnology, K.S. Rangasamy College of Technology, KSR Kalvi Nagar, Namakkal – 637215, Tamil Nadu, India.
Endometriosis is a chronic inflammatory disease dependent on estrogen that affects 10% of women of reproductive age. It is characterized by the ectopic growth of endometrium-like tissue that causes pain, infertility, and compromised quality of life. The pathogenesis of endometriosis is multifactorial and involves hormonal disturbance, dysregulation of the immune system, a genetic predisposition, and environmental factors. The older theories, such as retrograde menstruation, do not provide adequate explanatory power and therefore further explores stem cell and epigenetic mechanisms. The diagnosis of endometriosis is challenging due to nonspecific symptoms and the reliance on invasive laparoscopy for confirmation in the context of few reliable non-invasive biomarkers. Next-generation sequencing (NGS) and RNA-sequencing (RNA-seq) have radically changed the landscape of molecular diagnostics in identifying key gene expression signatures, dysregulated pathways, and epigenetic marks reflective of immunity, hormonal-signaling, and inflammation. While single-cell RNA-seq has identified cellular diversity within lesions, highlighting population of interest in the immune and stromal compartments that drive disease progression. Circulating biomarkers, including cell-free DNA, exosomal RNA, and microRNAs, has demonstrated utility in their early detection and potential to as a non-invasive diagnostic tool. Targeted NGS gene expression panels have implications for patient stratification and prognostication as somatic mutations and microsatellite instability can be interrogated. Multi-omics and bioinformatics approaches can enable precision diagnostics and personalized therapeutic regimens. This paper provides a comprehensive review of the literature, and outlines the transformative role of RNA-sequencing and NGS in diagnosing endometriosis.
Endometriosis is a chronic inflammatory and estrogen-dependent gynecological disorder defined by the presence of endometrial-like tissue — containing glands and stroma — outside of the uterine cavity. It affects approximately 10% of women of reproductive age worldwide and up to 50% of women with infertility or chronic pelvic pain.[39][24][12]. Endometriotic lesions are most commonly found in the ovaries, fallopian tubes, and pelvic peritoneum, but can also be identified in extrapelvic sites such as the diaphragm, lungs, and even the brain. Clinically, the disease is represented by symptoms including dysmenorrhea, dyspareunia, dysuria, dyschezia, and infertility, with severity not necessarily correlated with lesion size or location. [12][15]The disease has a multifactorial origin, with components including aberrant hormonal regulation, immune dysfunction, environmental factors, and genetic and epigenetic factors. Although endometriosis is histologically benign, it has several malignant-like features, including infiltration, angiogenesis, metastasis, and invasion, highlighting the complex pathology of the disease
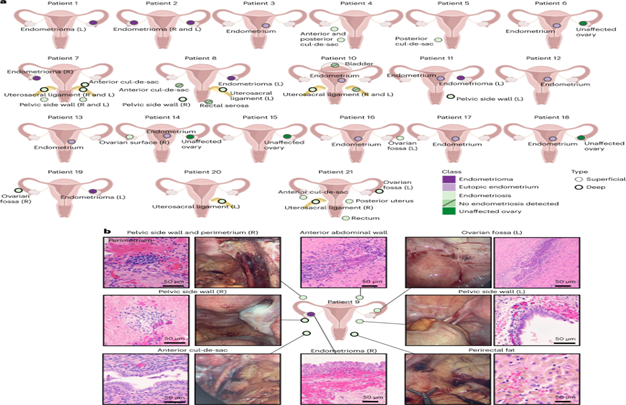
Fig 1.1: Histologic classification of specimens from women affected by superficial endometriosis, deeply infiltrating endometriosis, and ovarian endometriomas. (Kamergorodsky, G., Ribeiro, P. A. A., Galvão, M. A., Reinberg, K., & Leão, A. S. (2009))
EPIDEMIOLOGY, CLINICAL BURDEN AND BRACKET
Endometriosis is a condition that affects about 190 million women globally, and is one of the most prevalent causes of pain and infertility in women, and a major public health issue with a high societal cost. The classic clinical trifecta includes chronic pelvic pain, dysmenorrhea, and infertility. Notably. Endometriosis is found in 30–50% of women with infertility, and a large percentage of this group has chronic pelvic pain. [5][23].This condition is variable in its presentation. Endometriosis is typically categorized by location and type of lesion into three categories: superficial peritoneal endometriosis, ovarian endometriomas, the classic "chocolate cyst" and deep infiltrating endometriosis. Staging systems, such as the revised American Society for Reproductive Medicine (rASRM), stag/endometriosis on an anatomical basis for extent of lesion and degree of pelvic adhesions. However, clinical stage does not always correlate with pure lesion burden, and there is substantial variability in lesion characteristics. [39][12].
PATHOGENESIS OF ENDOMETRIOSIS:
The pathogenesis of endometriosis is multifaceted, involving an interplay of hormonal, immunological, inheritable, and environmental components. The classical retrograde menstrual theory, proposing movement of potential endometrial cells through the fallopian tubes into the peritoneal cavity, does not adequately account for all clinical and pathologic contributions. Competing theories such as coelomic metaplasia, which relates to the transformation of peritoneal cells into endometrial tissue, and stem cell theories, that intertwine with misplaced endometrial or stem cell progenitor cells capable of producing ectopic lesions, provide new insight into the origin and development of disease [39][24].
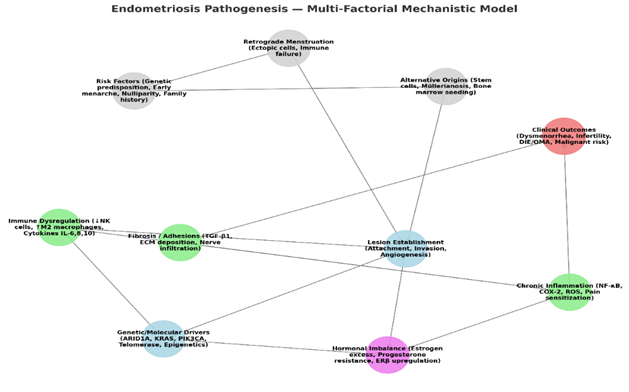
Fig 1.2: Endometriosis Pathogenesis – Multi Factorial Mechanistic Model
THEORIES OF PATHOGENESIS:
Endometriosis is a chronic, inflammatory disease of endometrial tissue growing outside of the uterus, most commonly affecting the ovaries, fallopian tubes, and peritoneum. The pathophysiology of endometriosis continues to be a debated topic [5][23].
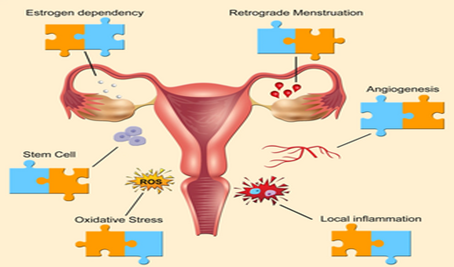
Fig 1.3: The diagram traces endometriosis pathogenesis from genetic/immune susceptibility and retrograde menstruation → cell adhesion, invasion, angiogenesis → lesions causing pain/infertility. (Kamergorodsky, G., Ribeiro, P. A. A., Galvão, M. A., Reinberg, K., & Leão, A. S. (2009))
RETROGRADE MENSTRUATION:
As suggested by John Sampson in 1927, it remains the most widely respected explanation. Retrograde menstruation is the idea that endometrial cells flow back through the fallopian tubes into the peritoneal cavity and implant and grow onto the peritoneal surfaces or other surfaces within the cavity - taking place during menstruation where they implant and grow. Approximately 76 - 90 percent of women have retrograde menstruation, but only 10 percent of women develop endometriosis. Retrograde menstruation does not account for the fact that only a subset of women develop endometriosis, creating a space for new theories that take into account other factors such as immune dysfunction, altered apoptosis, stem cell migration, genetic/ epigenetic factors and environmental factors [24][10].
METAPLASIA AND STEM CELL THEORIES:
The coelomic metaplasia theory postulates that under hormonal and inflammatory influences, peritoneal mesothelial cells change into endometrial-like cells. The stem cell theory takes this further and says that multipotent stem/progenitor cells - either from the basalis layer of the endometrium or from bone marrow - migrate and differentiate at ectopic locations, resulting in endometriotic lesions. Endometrial epithelial stem cells that are expressing markers such as SSEA-1 and N-cadherin and mesenchymal stem cells marked by CD146 and PDGFR-β have been implicated in this procedure. Mechanisms that may better explain endometriosis include coelomic metaplasia (a process of metaplasia leading to ectopic endometrial tissue derived), benign metastasis via lymphovascular spread, and recruited endometrial and bone gist-derived stem/ancestor cells. The stimulated processes indicate a complex, multifactorial processes, where dysregulated utilization of the system in conjunction with refluxed endometrial tissue combined with baseline hormonal dysregulation, promote the establishment and persistence of lesions. [24][39].
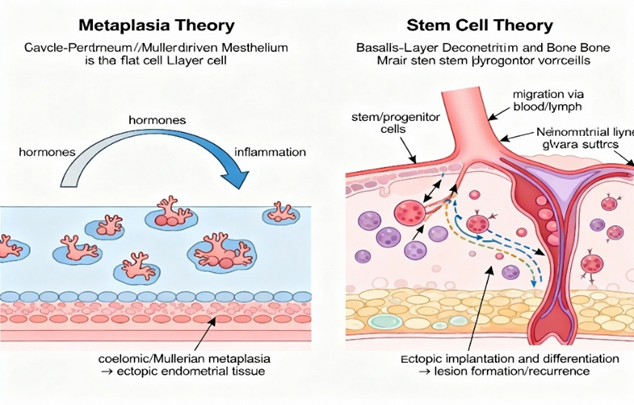
Fig 1.4: Left: Peritoneal mesothelial cells transform into endometrial-like tissue via hormones/inflammation (coelomic/Müllerian metaplasia). Right: Endometrial/bone marrow stem cells migrate via blood/lymph to implant and differentiate into ectopic lesions (see the generated image above). (Kamergorodsky, G., Ribeiro, P. A. A., Galvão, M. A., Reinberg, K., & Leão, A. S. (2009))
IMMUNOLOGICAL FOUNDATIONS AND DYSREGULATION
Immunological Basis and Changes Endometriosis is defined, pathologically, as an illness of immune dysfunction. Under normal physiologic conditions, the immune system continuously monitors the peritoneal cavity, quickly rejecting all excursive endometrial cells. In women afflicted by endometriosis, both the innate and adaptive immune systems demonstrate significant contrasts in immune involvement, providing a permissive environment to ectopic cell implantation, survival, and growth.A core concept of endometriosis is immune dysregulation, defined by aberrant macrophage activation, decreased cytotoxic potential of natural killer (NK) cells, and the geratic states of T-helper cell subsets (Th1, Th2, and Th17), which promote a chronic, pro-inflammatory microenvironment that facilitates lesion implantation, angiogenesis, and neuronal development. In conjunction with hormonal dysregulation, including increased estrogen and decreased progesterone signaling, these mechanisms enhance inflammatory and proliferative responses. These processes are mediated through the altered expression of enzymes such as aromatase and hormone receptors such as estrogen receptor beta (ERβ) [7][2].
At the molecular level, genetic susceptibility combined with well-characterized epigenetic changes, including hypermethylation of regulatory genes such as HOXA10, and dysfunctional microRNAs, disrupt cellular isolation and immune homeostasis perpetuating disease persistence. Collectively, these mechanisms create a self-sustaining cycle of inflammation, hormonal dysfunction, and immune evasion that sustain endometriosis during and after stress in individuals at risk for endometriosis [10][2][7]. In addition to well-defined changes in immune response variability and dysregulated T-cell states and functions, key innate and adaptive immune cell populations implicated in the pathogenesis include
MACROPHAGES:
Categorical and Phenotype Macrophages are significantly increased in both the eutopic endometrium and peritoneal fluid of women with endometriosis, and their cyclic variation becomes deregulated in disease states. In normal endometrium, anti-inflammatory M2 macrophages predominate facilitating tissue repair. In endometriosis, however, there is a bias toward the pro-inflammatory M1 phenotype, particularly in lesions. Functional Changes These macrophages secrete increased levels of cytokines (IL-1β, IL-6, IL-8, TNF-α), chemokines, and angiogenic factors such as VEGF, which keep inflammation going, support angiogenesis, and promote pain. In endometriosis, their phagocytic activity is impaired, leading to the persistence and ectopic implantation of endometrium [23][14][37].
NEUTROPHILS:
Role in Inflammation Neutrophil infiltration is increased in the peritoneal cavity and lesions, especially in early disease states. These cells exacerbate the inflammatory milieu by secreting IL-17A, IL-8, and VEGF which recruit more immune cells and induce angiogenesis. Depletion of neutrophils in animal models decreases the number of early endometrial lesions [24].
NATURAL KILLER (NK) CELLS:
Dysfunctional Cytotoxicity The cytotoxicity of NK cells is continuously impaired in the eutopic endometrium, peritoneal fluid, and peripheral blood of women with endometriosis. This impairment is linked with increases in inhibitory receptors and suppressive cytokines (e.g., IL-6, TGF-β, IL-15). The reduced activity enables endometrial fragments to escape immune recognition and implant ectopically Dendritic Cells (DCs): Altered Development and Function DCs are required for antigen presentation and adaptive T cell activation. The development of myeloid DCs is impaired in endometrial tissue and peritoneal fluid of women with endometriosis, resulting in inadequate antigen presentation and defective T cell-mediated recognition of ectopic tissue [32][35][2].
T CELLS AND REGULATORY T CELLS (TREGS):
CD4+ and CD8+ T Cells The immune microenvironment in endometriosis is characterized by a Th2-dominated response and suppressed Th1 response, with an increased CD4/CD8 ratio in peritoneal fluid, and increased T cells overall. Regulatory T Cells There is a primary increase in FoxP3+ Tregs in ectopic tissue and peritoneal fluid that promote immune tolerance and allow survival of endometrial implants. Th17 Cells Levels of Th17 cells are higher in peritoneal fluid and lesions and these cells cache IL-17, fortifying inflammation and lesion persistence. B Cells and Autoimmunity. Autoantibody Production There is greater likelihood/ activation of B cells along with autoantibodies (against endometrial antigens) appearing in the serum and peritoneal fluid, which indicates a relationship between endometriosis and/or systemic dysregulation of immune function and greater prevalence of autoimmune comorbidities [24][7].
CYTOKINE NETWORKS AND INFLAMMATORY MILIEU:
At the heart of the immune environment in endometriosis is a dense and dysregulated cytokine environment. Fluid samples from the peritoneal and systemic compartments in women with endometriosis have elevated levels of interleukins (IL-1, IL- 6, IL- 8, IL-10), tumor necrosis factor-alpha (TNF-α), interferons, growth factors (VEGF), and chemokines (MCP- 1, RANTES), which work together to cause leukocyte recruitment, lesion vascularity, pain, and fibrogenesis. These cytokine and chemokines not only promote cell viability they also inhibit normal reproductive function, normal endometrial receptivity, and implantation
[14][22][30].
CYTOKINE AND CHEMOKINE IMBALANCE
Pro-inflammatory Cytokines Increased local and systemic levels of IL- 1β, IL- 6, IL- 8, TNF- α, IL- 10, and IL- 17 occur in endometriosis. Angiogenesis Factors Elevated VEGF and other growth factors promote vascularization of lesions. Chemokines There are increased levels of monocyte chemoattractant protein- 1 (MCP- 1) and RANTES, retaining further susceptible cells to the peritoneal microenvironment [19][17][30].
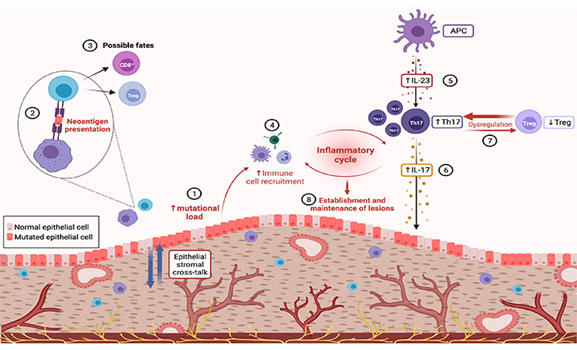
Fig 1.5: Flowchart of immune dysregulation in endometriosis: normal surveillance (balanced macrophages/NK/T cells) → dysfunction (reduced cytotoxicity, Th1/Th2 shift, high IL-6/TNF-α) → lesion survival via inflammation, angiogenesis, pain/infertility. (Kamergorodsky, G., Ribeiro, P. A. A., Galvão, M. A., Reinberg, K., & Leão, A. S. (2009))
IMMUNE ESCAPE AND IMPAIRED APOPTOSIS
Fas/FasL Pathway Endometriotic cells evade immune-mediated apoptosis by dysregulating the Fas/FasL pathway — supported by elevated local expression of FasL, which causes apoptosis in recruiting immune cells, allowing ectopic those are cells survive. Decreased susceptibility to Cell Death Aberrant apoptosis perpetuates the survival of both stromal and epithelial cells at ectopic sites [5][24][32].
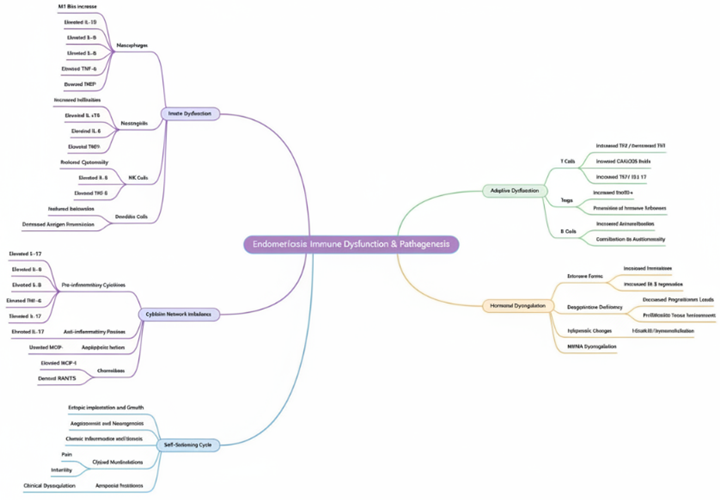
Fig 1.5: Central pathways include immune dysregulation (e.g., proinflammatory cytokines, NK cell defects), stem cell/metaplasia origins, hormonal influences (e.g., estrogen excess), and adaptive processes (e.g., angiogenesis, fibrosis), leading to ectopic lesion establishment and progression.
ENDOCRINE-IMMUNE-MICROBIOME AXIS:
Endometriosis is reliant upon estrogen and is characterized by a resistance to progesterone. Both altered natural estrogen production and dysregulation of estrogen and progesterone receptor expression (especially reduced PR-B and altered ER/PR ratios) stimulate the growth of endometriotic lesions and compromise immunity and endometrial receptivity. The reproductive tract and gut microbiomes affect circulating estrogen levels and immunity; dysbiosis increases chronic inflammation and interferes with immune regulation. Hormonal Influence Estrogen dominance and progesterone resistance disturb immune homeostasis, impair NK and Treg function, and induce anti-apoptotic, pro-inflammatory states [41][12].
MICROBIOME INTERACTIONS
Microbial Dysbiosis Changed gut and genital tract microbiota change the natural immune response, increasing inflammation and inhibiting immune tolerance in the endometrium [41][12].
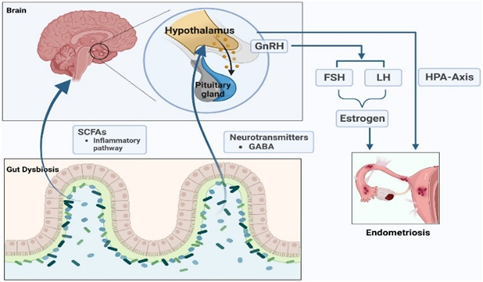
Fig 1.6: Microbiome boosts E2/immune suppression; cytokines worsen dysbiosis; E2 alters microbiota/immunity, sustaining hyperestrogenic inflammation → lesions/pain. (Kamergorodsky, G., Ribeiro, P. A. A., Galvão, M. A., Reinberg, K., & Leão, A. S. (2009))
GENETIC, EPIGENETIC, AND STEM CELL FINDINGS
Heritable predisposition plays an important role, with genome-wide association studies linking risk loci that contain genes that regulate hormone pathways, immunity, and cell adhesion (e.g., ESR1, FSHB, WNT4). Also, somatic mutations in oncogenes such as KRAS, ARID1A, and PIK3CA are found in endometriotic lesions, suggesting clonal expansion rather than malignanc [39][3]. Epigenetic factors, including DNA hypermethylation of HOXA10 and dysregulated micro-RNAs (e.g., miR-135; miR-223), also help to produce aberrant hormone responses, further diminishing apoptosis and degrading immunity. [4][2]. Genetic examinations have identified SNPs and epigenetic modifications in genes involved with hormone metabolism, immune regulation, and cellular adhesion. Stem/ancestral cells from the endometrium and the bone marrow are hypothesized to contribute to initiation and/or maintenance of ectopic lesions. [39][24]. These cells may be marked and triggered by chemokines (e.g., CXCL12/CXCR4 axis), and add an extra layer of complexity to the diversity of lesions and treatment resistance. Immune Genes GWAS and transcriptomics have identified multiple immune- and autophagy- related genes (IRGs and ARGs) such as CSF1, CD86, and S100A11 — as central to endometriosis vulnerability and immune/inflammatory dysfunction [19][44].
IMMUNE CELL INTERACTIONS AND LESION DEVELOPMENT:
Failure of immunosurveillance the immune system of women with endometriosis fails to clear refluxed endometrial cells, and if they implant, they are able to persist due to background immunosuppression, poor NK/DC function, and pro-angiogenic/anti-apoptotic signaling. [1][18]. Fibrosis and Pain: crosstalk between immune cells (particularly activated macrophages), stromal cells, and neurons augments innervation of lesions, pain sensitization, and fibrosis [23][38].
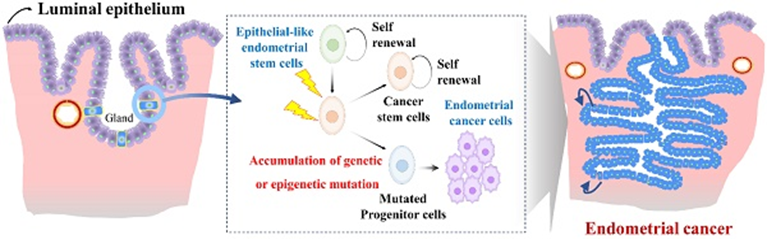
Fig 1.7: Genetic variants alter epigenetics (↑ stem clonogenicity); epigenetics reprogram stem cells (↑ invasion); genetics prime stem niches → hyperestrogenic, invasive lesions. (Kamergorodsky, G., Ribeiro, P. A. A., Galvão, M. A., Reinberg, K., & Leão, A. S. (2009))
HORMONAL, MICROBIOME, AND STEM CELL INTERSECTIONS
Endometriosis is fundamentally dependent on estrogens and resistant to progesterone. Estrogen receptor β (ERβ) overexpression and progesterone receptor-B (PR-B) downregulation result in both inflammatory and proliferative signaling. Aromatase upregulation in lesions increases local estrogen production, contributing to survival and neuroangiogenesis [3][17]. This altered balance, accompanied by progesterone resistance, perpetuates aberrant decidualization and immune sensitization necessary for implantation. Local hormonal activity and the so-called "hormone immune interaction" regulate immune cell recruitment, phenotype, and function. Altered estrogen metabolism (potentially influenced by gut and reproductive tract microbiomes), progesterone resistance, and chronic endometritis (microbiome dysbiosis) further propagate immune cell activation and lesion [38]. Elevated oxidative stress markers have also been observed in the culture medium, resulting in DNA damage and chronic inflammation that may define a link between endometriosis and increased risk of particular ovarian cancers in a minority of cases. Epigenetic modifications, such as altered DNA methylation, histone acetylation, and microRNA dysregulation, affect gene expression patterns that are essential for the survival of lesions, immune evasion, and possibly malignant transformation. Recent investigations have provided specific interest into endometrial and bone marrow-derived stem/progenitor cells. Through inflammatory and chemokine signaling (e.g., the CXCL12/CXCR4 axis), these cells are recruited, contributing to tissue remodeling and aberrant lesion formation [39][24].
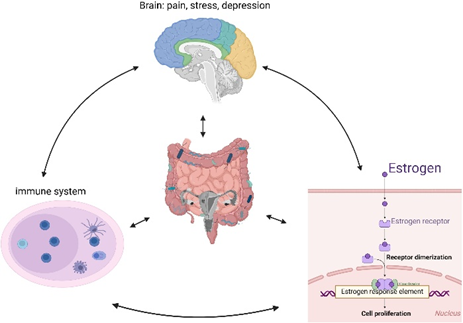
Fig 1.6: Hormonal-microbiome (estrobolome boosts E2 → stem cell proliferation); microbiome-stem (LPS/inflammation promotes stem homing); hormonal-stem (E2 drives stem differentiation); central triple overlap (“hyperestrogenic inflammatory niche sustains ectopic lesions, pain, infertility”) (Kamergorodsky, G., Ribeiro, P. A. A., Galvão, M. A., Reinberg, K., & Leão, A. S. (2009))
MATERIALS AND METHODOLOGY
Qualitative Methods: Comprehending the Experience of Patients and Physicians
Numerous approaches have been used in endometriosis research, including gene panel development, immunohistochemistry, next-generation sequencing, experimental cellular assays, qualitative patient-doctor surveys, and bioinformatics. One qualitative study used open-ended questionnaires for patients and semi-structured phone interviews for general practitioners (GPs) to collect patient experiences and GP viewpoints on endometriosis pain communication in the UK in order to better understand patient-practitioner dynamics. Online platforms were used to gather responses, and NVivo 11 software was used for analysis through thematic coding and verification by a medical anthropologist and linguist. GP demographic data was gathered along with clinical themes that surfaced from the responses of both groups, and pain descriptions were examined in terms of both qualitative descriptors and metaphorical language use [10].
MOLECULAR PROFILING: SEQUENCING AND MUTATION ANALYSIS:
Targeted next-generation sequencing (NGS) has been essential for molecular research. In one proof-of-principle study, 48 women with endometrioid-type endometrial adenocarcinoma had peripheral blood samples and matched tumor samples taken. Using common commercial kits, DNA was extracted from buffy coat, plasma, and tumor tissue that had been formalin-fixed. They evaluated tissue and circulating cell-free DNA using Illumina sequencing platforms and created a custom amplicon panel that targets common mutations in genes related to endometrial cancer (PTEN, PIK3CA, KRAS, and CTNNB1). High-depth sequencing, careful validation of low-frequency variants, and cross-confirmation with digital PCR were all part of the variant calling process in earlier research. Additionally, the researchers used PCR-based microsatellite instability analysis and immunohistochemistry for mismatch repair proteins. ANOVA, Kruskal-Wallis, chi-square, and Fisher's exact tests were used in statistical comparisons in order to establish a relationship between molecular findings and tumor characteristics and clinical outcomes [25].
COMBINING TRADITIONAL AND CUTTING-EDGE DIAGNOSTIC METHODS
In other research, traditional and molecular approaches for detecting microsatellite instability (MSI) in endometrial cancer were compared. In one such study, a focused panel for the mismatch repair genes MLH1, MSH2, MSH6, and PMS2 was used in conjunction with NGS and immunohistochemistry (IHC). Fresh and paraffin-embedded tumor tissues were used to extract DNA, and platforms like the DNBSEQ-G400 were used to apply focused NGS gene panels or whole-exome sequencing [37]. While IHC used validated antibody-based detection protocols and scored both the intensity and proportion of stained cells, data analysis was carried out using Python scripts and third-party kits. The study used clinical and histopathological staging as references to compare the practical value, accuracy, and cost-effectiveness of IHC versus molecular sequencing for MSI [28].
FUNCTIONAL VALIDATION, TRANSCRIPTOMICS, AND BIOINFORMATICS
Gene expression landscapes in endometrial lesions were delineated using high-throughput RNA sequencing, single-cell RNA-seq, and multi-omics data integration for immunogenomics and biomarker discovery [21]. Bioinformatics pipelines examined transcriptomic, mutational, and copy number variation data from public databases such as Gene Expression Omnibus (GEO) and The Cancer Genome Atlas (TCGA) in these investigations [28]. Clustering algorithms, gene set variation and enrichment analyses (e.g., GSVA, fgsea, KEGG), and unsupervised machine learning techniques like lasso regression and non-negative matrix factorization (NMF) were all used in these studies. Using commercial reagents, real-time quantitative PCR, Western blotting, and image analysis tools, immunohistochemical staining and a variety of cell biology assays, including proliferation, migration, and invasion, were used to validate the cells and tissues [29].
INTEGRATIVE RESEARCH: TOWARD BETTER DIAGNOSIS AND CARE
Combined, these approaches demonstrate how qualitative, molecular, analytical, and experimental approaches have come together in modern endometriosis research to produce Integrative Research: Toward Better Diagnosis and Care [31]. They serve as the foundation for initiatives aimed at enhancing biomarker development, disease characterization, diagnostics, and, eventually, patient care. With each technique designed to extract clinically relevant insights, whether from genetic changes, molecular phenotyping, patient narratives, or cell-based experimentation, endometriosis and related gynecologic diseases can be thoroughly understood [41].
METHODS OF GENE EXPRESSION AND BIOMARKER IDENTIFICATION
In order to find modules of co-expressed genes that are suggestive of endometriosis pathology, researchers commonly employ weighted gene co-expression network analysis (WGCNA) for gene expression and biomarker discovery. To compare diseased and control tissues, differential expression analysis is usually carried out using the limma package in R. Gene Ontology (GO) and KEGG enrichment databases are used to map genes that pass significance thresholds to biological pathways. Finding sets of signature genes with diagnostic value is aided by machine learning techniques like LASSO, XGBoost, support vector machine recursive feature elimination (SVM-RFE), and binary logistic regression. Cross-validation and independent validation datasets, which are occasionally displayed using ROC curves, are used to verify the accuracy of the model [19][27][29].
NETWORKS OF PROTEIN INTERACTIONS AND IMMUNE ANALYSIS
Finding important "hub" genes and functional networks involved in disease processes is aided by the construction of protein-protein interaction (PPI) networks, usually using the STRING database and visualized using Cytoscape [19]. Using tools like CIBERSORT, immune infiltration analysis compares the prevalence of immune cells in normal and endometriotic tissues, establishing a connection between changes in the immune landscape and gene expression [43]. Wet-lab methods like immunofluorescence, western blots, and quantitative real-time PCR (qRT-PCR) are used to validate signature genes found using these in-silico approaches. Additionally, animal models are used to replicate human pathology and test therapeutic interventions (e.g., determining the effect of tretinoin treatment on lesion size and the expression of key genes) [44].
MOLECULAR AND CLINICAL DIAGNOSTIC TECHNIQUES
Targeted next-generation sequencing (NGS) of tumor and blood samples allows for the identification of cell-free DNA mutations unique to endometriosis or endometrial cancer for clinical and molecular diagnostics [28]. Following well-defined DNA extraction procedures, amplicon-based sequencing is performed on Illumina or comparable platforms [37]. Well-known genes linked to cancer or endometriosis are the focus of gene panel design. Custom or commercial pipelines process sequence data, set thresholds for mutation calling, and, if necessary, cross-check the results using orthogonal techniques like digital PCR. For more comprehensive molecular subtyping, PCR-based microsatellite instability (MSI) analysis and immunohistochemistry (IHC) are carried out concurrently. The trade-offs between IHC and molecular profiling in terms of cost, sensitivity, and clinical utility are highlighted by comparative studies. Buffy coats, matched patient samples, and uniform management of pre-analytical factors like fixation time and plasma processing are examples of experimental controls [31].
EXPERIMENTAL VALIDATION AND INTEGRATIVE MULTI-OMICS
Utilizing transcriptomics, genomic variants, and occasionally proteomics, integrative studies also apply clustering, gene set variation analysis, and machine learning to multi-omics datasets in order to uncover functional pathways, cell type diversity (e.g., via single-cell RNA-seq), and clinically significant molecular subtypes [27]. Model animal experiments are robustly designed as double-blind, randomized, placebo-controlled trials, frequently with sample size justification and error analysis, and they validate in-silico findings [10].All studies' statistical interpretation includes standard evaluations of variance, significance, and model performance (sensitivity, specificity, PPV, NPV, accuracy, and AUC) using programs like R, SPSS, or Graphpad Prism) [16].
TABLE 1.1: INTEGRATED RNA/NGS-BASED MOLECULAR SIGNATURES FOR ENDOMETRIOSIS AND RISK STRATIFICATION.
|
Diagnostic Approach |
Key RNA/NGS Targets |
Performance (AUC) |
Tissue/ Source |
Clinical Utility |
|
Machine Learning Signatures |
SLC7A11, IQGAP1 (eutopic); MYH10, CD2AP, PDLIM1 (ectopic) |
0.80–0.96 |
Eutopic/ ectopic endometrium |
Non-invasive prediction; immune correlation |
|
Disulfidptosis DEGs |
20 eutopic/16 ectopic (e.g., ACTB, CAPZB) |
>0.7 (nomogram) |
Serum/ peritoneal fluid |
Early detection; therapeutic monitoring |
|
NGS Mutations |
KRAS, ARID1A |
N/A (progression risk) |
Lesion biopsies |
Cancer risk stratification |
Note: This table summarizes key RNA-based and next-generation sequencing (NGS) diagnostic approaches for endometriosis, highlighting biomarkers, their performance metrics (e.g., AUC values), tissue sources, and clinical applications. Machine learning panels using ectopic endometrial transcripts like SLC44A1, IQGAP1, CTGF, and PD-L1 achieve high AUCs (0.80-0.96) for non-invasive immune monitoring via serum or peritoneal fluid. In contrast, targeted NGS detects oncogenic mutations such as KRAS and ARID1B in lesion biopsies, aiding progression risk assessment and cancer stratification [26][27][19][39].
CHALLENGES IN DIAGNOSIS:
Even with new knowledge, endometriosis management is still very difficult. An average of 7 to 10 years pass before a diagnosis is made because of overlapping symptoms with other pelvic disorders and the need for invasive laparoscopic procedures [38]. Early detection and prompt intervention are hampered by the lack of sensitive and specific non-invasive biomarkers. Clinical and molecular heterogeneity brought on by the complex etiology makes it more difficult to develop standardized diagnostic and treatment strategies [12][33]. Hormonal therapies have side effects and are frequently inappropriate for women seeking fertility. Current treatments, such as surgery and hormonal therapy, provide symptomatic relief but neither prevent recurrence nor cure the disease [10][1]. Furthermore, advancements in targeted immunotherapy are constrained by our limited knowledge of the immune pathways maintaining inflammation and lesion survival. These challenges underscore the urgent need for personalized diagnostic and therapeutic strategies based on detailed molecular and immune profiles:
1. Diagnostic Difficulties: Accurate diagnosis remains difficult due to the invasive nature of standard laparoscopic detection, lack of reliable non-invasive biomarkers, and symptom overlap with other pelvic conditions. This leads to significant diagnostic delays averaging 7-10 years, impacting patient outcomes and management.
2. Heterogeneity and Complex Pathogenesis: The multifactorial origin of endometriosis—including genetic, epigenetic, hormonal, immune, and environmental factors—creates wide clinical and molecular heterogeneity. This complexity complicates the development of universal diagnostic criteria and effective targeted therapies.
3. Treatment Limitations: The disease, which has a high recurrence rate, cannot be cured by current hormonal and surgical treatments; they only alleviate its symptoms. Hormonal treatments are not recommended for women who want to preserve their fertility because they frequently have unfavorable side effects.
4. Immunological Dysregulation: Although the exact relationships between immune dysfunction and lesion establishment and survival are still unclear, they do contribute. Immune system and inflammatory pathway targeting are new areas that need more study before they can be used in clinical settings.
5. Need for Personalized Medicine: Considering the complexity of the illness, it is critical to develop individualized diagnostic and treatment plans based on immunological and molecular profiling [40][25].
SYSTEMIC EFFECTS AND COMORBIDITIES
Beyond the reproductive system, endometriosis has a systemic impact that includes an increased risk of infertility, autoimmune diseases, cardiovascular disease, allergic reactions, mental health issues, and certain types of cancer, particularly breast and ovarian cancers. Many of these associations may be causally related to immune dysregulation and the chronic inflammatory state. [40][10]
UNMET NEEDS AND FUTURE RESEARCH PATHS
The lack of sensitive and specific non-invasive biomarkers, the limited effectiveness of current treatments (particularly with regard to fertility preservation), and difficulties with recurrence and individualized treatment, despite significant advancements, highlight the critical need for more research. Integrating immune phenotyping, genomics, single-cell and microbiome analyses, and the creation of targeted, non-hormonal immunotherapies is anticipated to lead to future advances [31].
CLINICAL IMPLICATIONS AND RESEARCH FRONTIERS
Beyond the development of lesions, immune dysregulation in endometriosis can lead to infertility, aberrant endometrial receptivity, increased pain sensitivity, and even a higher risk of developing some autoimmune and malignant diseases [10]. Almost all phases of the reproductive process, including folliculogenesis, oocyte maturation, embryo quality, and implantation, are impacted by immune dysfunction. Finding precise biomarkers for diagnosis and staging as well as efficient non-hormonal, immunomodulatory treatments continue to be top research priorities. More efficient, customized management approaches could be possible with developments in immune phenotyping, single-cell analyses, microbiome research, and targeted interventions [35][36][29].
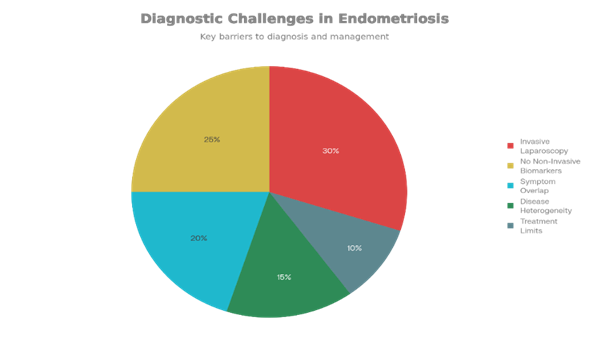
Fig 1.7: Invasive laparoscopy (30%) dominates due to procedural risks/delays; lack of non-invasive biomarkers (25%) prevents early detection; symptom overlap (20%) confuses with IBS/adenomyosis; disease heterogeneity (15%) from genetic/immune factors hinders uniform criteria; treatment limitations/recurrence (10%) reflects hormonal/surgical shortfalls.
RNA SEQUENCING AND NEXT-GENERATION SEQUENCING AID IN THE NON-INVASIVE DIAGNOSIS AND BIOMARKER DISCOVERY:
Because invasive laparoscopy is the gold standard for diagnosing endometriosis, there are significant diagnostic challenges, with average delays of 7–10 years from symptom onset to diagnosis. The sensitivity and specificity of non-invasive diagnostic techniques like imaging and serum biomarkers are insufficient. The urgent need for innovative, minimally invasive molecular diagnostic techniques is highlighted by this diagnostic gap. By capturing the entire transcriptome at single-nucleotide resolution, RNA sequencing, or RNA-Seq, has become a potent, high-throughput technology that has the potential to completely transform disease diagnosis [12][33]. In contrast to conventional microarray-based methods, RNA-Seq provides thorough molecular portraits of disease states by concurrently detecting and quantifying messenger RNAs (mRNAs), long non-coding RNAs (lncRNAs), microRNAs (miRNAs), alternative splicing isoforms, and gene fusion events.The identification of differentially expressed genes (DEGs) between eutopic endometrium from endometriosis patients and healthy controls, as well as between ectopic lesions and normal endometrium, has been made easier in endometriosis research thanks to RNA-Seq. Researchers have discovered dysregulated pathways involving immune response, inflammation, angiogenesis, cell adhesion, extracellular matrix remodeling, and hormonal signaling through transcriptomic profiling. These pathways are all essential to the pathophysiology of endometriosis. Diagnostic biomarker signatures can be systematically identified from thousands of candidate transcripts using machine learning algorithms combined with RNA-Seq data analysis. Filtering noise, reducing dimensionality, and selecting robust gene signatures with high diagnostic accuracy have all been accomplished with the help of techniques like random forest (RF), support vector machines (SVM), extreme gradient boosting (XGBoost), and least absolute shrinkage and selection operator (LASSO) regression [20][21].
Genes linked to inflammation and the immune system have been found to be potential diagnostic markers for endometriosis in recent studies using RNA-Seq in conjunction with bioinformatics and machine learning. In endometrial tissues from patients with endometriosis, for instance, immune infiltration analyses using algorithms such as CIBERSORT have shown changed distributions of neutrophils, T cells, B cells, natural killer (NK) cells, and macrophages [19][26][27]. In independent validation cohorts, signature genes found using these methods—MET, IL4R, BST2, ACKR1, LMNB1, MFAP4, NMU, and SEMA3C—have demonstrated encouraging diagnostic performance with high area under the curve (AUC) values. Moreover, even greater resolution has been made possible by single-cell RNA sequencing (scRNA-Seq), which has made it possible to analyze cellular heterogeneity and pinpoint changes in endometriosis gene expression that are specific to particular cell types. This technology has provided insight into immune evasion mechanisms and cellular crosstalk by revealing unique transcriptomic changes in stromal, epithelial, and immune cell populations [31][20]. When paired with sophisticated computational tools and machine learning, RNA-Seq-based transcriptomic profiling represents a paradigm shift in the diagnosis of endometriosis. This method holds great promise for creating precise, non-invasive diagnostic tests that could significantly cut down on diagnostic delays and enhance clinical outcomes for women with endometriosis by identifying and validating molecular signatures obtained from minimally invasive samples like blood, menstrual fluid, or endometrial biopsies [24][8]. The complex molecular heterogeneity of endometriotic lesions is captured by RNA-seq through transcriptomic profiling, which reveals networks linked to inflammation, hormone signaling pathways, and dysregulated immune response genes. This has revealed new potential therapeutic targets and diagnostic markers, especially genes related to inflammation, immune regulation, angiogenesis, and epigenetic control. Furthermore, developments like single-cell RNA-seq offer resolution of transcriptomic alterations specific to cell types, identifying unique stromal and immune cell populations that contribute to the development of disease [10]. The discovery of circulating RNA biomarkers, like microRNAs, that have potential for use in upcoming minimally invasive diagnostic procedures has also been made easier by RNA-seq research. The molecular landscape of endometriosis can be decoded using RNA sequencing, which improves knowledge of the disease's intricate biology and increases the likelihood of accurate diagnosis and individualized treatment based on molecular signatures [31].
THE ROLE OF NEXT-GENERATION SEQUENCING (NGS) IN ENDOMETRIOSIS DIAGNOSIS
In terms of molecular profiling and endometriosis diagnosis, next-generation sequencing (NGS) has become a game-changing technology. While traditional diagnostic techniques like polymerase chain reaction (PCR) and immunohistochemistry (IHC) only examine a small number of targets, next-generation sequencing (NGS) provides extensive, high-throughput information on tumor mutational burden (TMB), microsatellite instability (MSI), and genetic changes [25].
NGS-BASED MOLECULAR CLASSIFICATION
DNA polymerase epsilon (POLE), TP53, mismatch repair (MMR) genes (MLH1, MSH2, MSH6, PMS2), and oncogenes like PTEN, PIK3CA, KRAS, and CTNNB1 are among the genes that are simultaneously analyzed by NGS-Based Molecular Classification (NGS) and linked to the pathophysiology of endometriosis and overlapping endometrial cancers. In contrast to histopathology alone, this allows molecular classification into clinically meaningful subtypes, such as POLE-ultramutated, MMR-deficient/MSI-high, p53-abnormal, and no specific molecular profile (NSMP), which correlate with prognosis and direct individualized treatment [35].
DETECTION OF MICROSATELLITE INSTABILITY AND TUMOR MUTATION BURDEN:
The capacity of NGS to simultaneously evaluate TMB and MSI status across a large number of microsatellite loci (from 17 to more than 100 markers) is a crucial benefit. In situations where IHC is unclear, NGS results frequently exhibit superior sensitivity and demonstrate high concordance (>90%) with IHC and PCR-based techniques. NGS is crucial for determining appropriate candidates for immunotherapies because MSI-high status and elevated TMB are predictive biomarkers for responsiveness to immune checkpoint inhibitors [25].
IDENTIFICATION OF THERAPEUTICALLY ACTIONABLE MUTATIONS AND BIOMARKERS
Finding Biomarkers and Mutations That Can Be Therapeutically Actionable Targeted therapy decisions are informed by the clinically significant, actionable mutations that NGS finds in genes like PIK3CA, ERBB2 (HER2), and ESR1. Additionally, it detects circulating tumor DNA (ctDNA) in plasma and low-frequency somatic mutations, facilitating early relapse detection and minimally invasive disease monitoring. Additionally, NGS-based microRNA profiling makes it possible to find new prognostic and diagnostic biomarkers for non-invasive uses [37].
BENEFITS OF CLINICAL UTILITY AND WORKFLOW
Compared to conventional techniques that call for distinct IHC, PCR, and Sanger sequencing, NGS reduces turnaround times and resource consumption by combining several diagnostic assays into a single, scalable, and affordable platform. Eight to sixty gene targets are included in endometriosis-specific customized NGS panels, which can be modified for environments with limited resources. Furthermore, by decreasing reliance on invasive tissue biopsies, compared to conventional tissue biopsies, using NGS on liquid-based cytology (LBC) samples is less invasive. By accurately identifying genetic mutations, microsatellite instability (MSI), and tumor mutational burden (TMB), next-generation sequencing (NGS) is a proactive method of risk assessment. In order to categorize endometrial tumors into subtypes with different prognoses and treatment options, this thorough molecular profiling is essential [36]. The study shows that NGS reduces ambiguity in results and helps clinicians identify high-risk patients effectively by combining multiple diagnostic tests, including PCR and immunohistochemistry (IHC), into a single, efficient platform. MicroRNAs can be found using NGS and PCR methods as minimally invasive endometriosis biomarkers. The paper identifies particular dysregulated microRNA signatures in endometriosis that have a strong correlation with the course of the illness. It offers a non-invasive diagnostic option by showing promise in identifying these microRNA markers in readily accessible fluids like blood or menstrual fluid. In order to guarantee clinical utility and reliability, the manuscript also emphasizes the necessity of validating these biomarkers using both technologies [11].
APPLYING NGS TO LIQUID-BASED CYTOLOGY (LBC) SAMPLES:
Compared to conventional tissue biopsies, using NGS on liquid-based cytology (LBC) samples is less invasive. It provides a highly sensitive and trustworthy molecular diagnostic platform by confirming that NGS can be successfully carried out on these samples with little DNA input. This method makes molecular diagnosis more accessible to patients, which is particularly helpful in environments with limited resources. Custom-made NGS panels that incorporate important genes linked to endometriosis and associated cancers offer strong diagnostic coverage at the lowest possible cost [30][26][45].
HIGHLIGHTS OF NGS INCORPORATED INTO CLINICAL WORKFLOWS:
It describes how NGS makes personalized medicine possible by assisting medical professionals in choosing the best course of action based on each patient's distinct genomic profile. In order to improve patient outcomes through more accurate diagnosis and customized interventions, the paper recognizes the comprehensive nature of NGS in identifying novel therapeutic targets and prognostic biomarkers. For endometriosis molecular profiling, NGS is a potent, integrative tool that outperforms conventional diagnostics in terms of sensitivity, specificity, and informational breadth. Its ability to perform thorough genomic characterization facilitates prognostic stratification, individualized treatment selection, and the discovery of new therapeutic targets, all of which significantly improve endometriosis precision management in clinical practice [31][26].
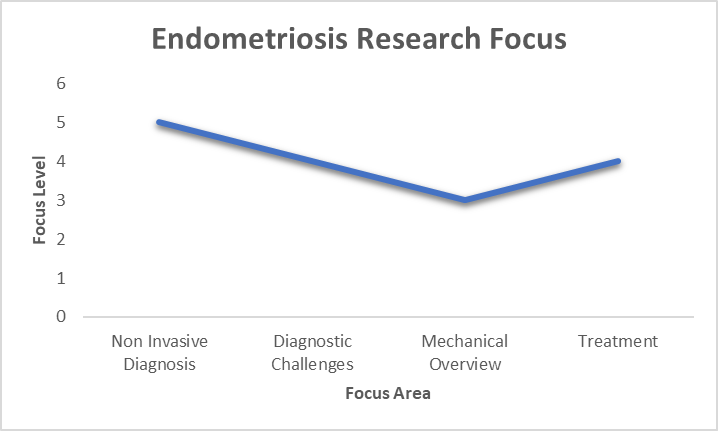
Fig 1.8: Distribution of Endometriosis research focus areas, showing peak emphasis on mechanisms (High Level)
Note: This chart depicts the relative emphasis in endometriosis exploration across crucial focus areas, revealing the loftiest on mechanistic studies (peak at 5-6 units), followed by a decline toward treatment 1 unit). Individual styles, both non-invasive and conventional, and treatment admit comparatively less concentrate, pressing a exploration imbalance amid ongoing clinical requirements for better diagnostics and curatives.
CONCLUSION
The presence of endometrial-like tissue outside the uterus, usually on the ovaries, pelvic peritoneum, and fallopian tubes, is the hallmark of endometriosis, a chronic, estrogen-dependent illness. It affects about 10% of women who are of reproductive age and has a major negative influence on quality of life. Symptoms include pelvic pain, dysmenorrhea, dyspareunia, and infertility. Pathogenesis is multifaceted and intricate, involving a number of interconnected theories and molecular mechanisms.
Retrograde menstruation, in which viable endometrial cells move backward through the fallopian tubes into the peritoneal cavity during menstruation, is the traditional and most widely accepted theory. Lesion formation results from these cells adhering to the peritoneal mesothelium, surviving immune clearance because of immunological dysfunction, and proliferating by creating a local blood supply.
While most women experience retrograde menstruation, only a small percentage go on to develop endometriosis, suggesting that other factors are crucial. Other theories include the stem cell theory, which postulates that circulating epithelial progenitor or stem cells from the uterus or bone marrow become lodged ectopically and clonally expand to form lesions, and coelomic metaplasia, which suggests that peritoneal or other pluripotent cells transform into endometrial-like tissue under particular stimulatory conditions. Another important factor is genetic susceptibility; several risk loci have been found that may affect hormone signaling, immune responses, and cellular proliferation.
Immune dysregulation, which is typified by compromised macrophage function, modified T-cell subsets (including regulatory T cells), reduced natural killer cell cytotoxicity, and a persistent pro-inflammatory milieu, is essential to the disease's persistence. Overexpression of cytokines, chemokines, and growth factors, including TNF-α, IL-1β, IL-6, VEGF, and others, promotes angiogenesis, fibrosis, and inflammation surrounding ectopic lesions.
Endometriotic tissue exhibits hormonal imbalances at the molecular level, with progesterone resistance and estrogen dominance caused by altered progesterone receptor function and overexpression of estrogen receptor beta. Defective cellular differentiation and immune tolerance are caused by epigenetic modifications, such as DNA methylation and histone acetylation of genes like HOXA10. Additionally, oxidative stress brought on by reactive oxygen species and iron deposition exacerbates DNA damage and persistent inflammation. Some endometriotic lesions have somatic mutations similar to those found in related ovarian cancers, and they display characteristics similar to benign tumors, such as invasive behavior, angiogenesis, and clonal expansions.
The disease state is sustained by persistent cyclic bleeding of ectopic tissue, which causes tissue damage, repair, and fibrosis. The purpose of this review paper is to provide a thorough analysis of the benefits of Next-Generation Sequencing (NGS) and RNA sequencing (RNA-seq) technologies in the diagnosis of endometriosis. The combination of several studies demonstrates how important these cutting-edge transcriptomic and genomic tools are in finding new molecular biomarkers that enable accurate and timely diagnosis. Personalized diagnostic criteria and new therapeutic targets can be developed thanks to the thorough bioinformatics analysis made possible by multi-omic NGS datasets. The current endometriosis treatment restrictions and diagnostic delays can be overcome with the help of such molecular precision.
In conclusion, the review clarifies how RNA-seq and NGS technologies revolutionize endometriosis diagnosis and clinical management by facilitating the identification and validation of reliable biomarkers, ushering in an era of personalized medicine with better patient outcomes and quality of life.
ACKNOWLEDGEMENT
We are grateful to Mohammad Khaja and an anonymous reviewer for useful comments. Any errors remain entirely ours.
REFERENCES


Ilakiya Mohankumar, Sathviga, A Review on Integrated Transcriptomic and Immunogenic Epitope Analysis for Non-Invasive Diagnosis of Endometriosis, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 2178-2198. https://doi.org/10.5281/zenodo.19118692
 10.5281/zenodo.19118692
10.5281/zenodo.19118692