
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Womens College of Pharmacy, Peth-Vadgaon.
Polycoria is a rare ocular condition characterized by the presence of multiple pupillary openings within a single iris, which may be functional or non-functional. It can be congenital or acquired and is sometimes associated with other eye anomalies such as corectopia, coloboma, and glaucoma. Clinical presentation varies from being asymptomatic to experiencing symptoms like glare, double vision, and reduced visual acuity. This review outlines the classification, etiology, clinical features, diagnostic methods, differential diagnoses, and current management options for polycoria. Diagnostic tools include slit-lamp examination, pupil reflex tests, anterior segment imaging, and visual assessments. Treatment ranges from observation in mild cases to surgical correction in symptomatic individuals. Recent advances, including artificial iris implants and improved imaging technologies, have enhanced diagnostic accuracy and treatment outcomes. However, further research is needed to understand the underlying genetic and developmental factors. Early diagnosis and a tailored multidisciplinary approach are crucial to preventing complications and preserving vision.
Polycoria is an exceptionally rare and intriguing condition of the eye, specifically affecting the iris, which is the colored part of the eye responsible for regulating the amount of light that enters the pupil. In normal ocular anatomy, the iris contains a single central pupil—a round aperture that dilates and constricts in response to light and visual focus, facilitating optimal vision. In individuals with polycoria, however, there exists more than one pupillary opening within the same iris. This anomaly may present as two or more holes that resemble pupils. [1]
These additional openings can vary in terms of structure and function:
Occurrence and Development :
Polycoria is typically congenital in origin, meaning it is present at birth and arises from abnormal development of the iris during embryogenesis. However, there are instances where polycoria may be acquired later in life due to: [3]
This condition may occur in isolation or in association with other ocular anomalies, such as: [4]
Clinical Relevance :
The clinical impact of polycoria varies depending on whether the additional pupils are functional, their location, and their size. Some patients may have no symptoms at all and the condition might be discovered incidentally during an eye examination. However, others may experience significant visual disturbances, including: [5]
If left undiagnosed, particularly in pediatric patients, polycoria can result in amblyopia (lazy eye) or strabismus (misalignment of eyes) due to disrupted visual development.
Significance of the Review
Despite its rarity, polycoria can have profound visual, functional, and cosmetic implications, especially when associated with other ocular abnormalities. There is currently limited literature and clinical guidance on the diagnosis and management of this condition, largely because it is so uncommon. [6]
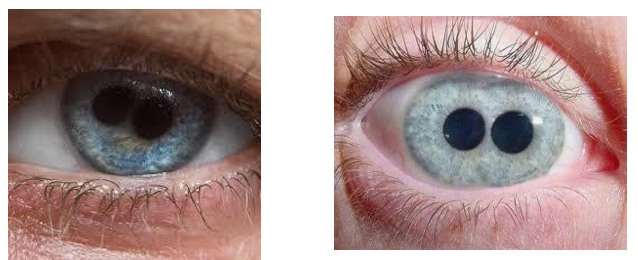
Figure 01. Polycoria condition. [54]
This review aims to:
In essence, this review serves as an essential resource to bridge the gap in knowledge and provide a reference framework for both researchers and clinicians who encounter this rare but potentially impactful ocular condition. [7]
Classification of Polycoria:
Polycoria is an unusual anomaly of the iris and pupil that can be classified into two main categories based on the anatomical structure and functional capability of the additional pupillary openings. A clear understanding of this classification is essential for accurate diagnosis and management, as each type differs significantly in both origin and clinical implications. [8]
a) True Polycoria
True polycoria is an extremely rare congenital anomaly of the eye characterized by the presence of two or more pupillary openings, each possessing an independent sphincter pupillae muscle. This muscular ring is crucial because it allows each pupil to respond independently to light and accommodation, performing constriction and dilation much like a normal pupil. [9]
Key Characteristics:
Pathophysiology:
The condition arises due to abnormal development of the iris musculature during embryogenesis. It is believed that improper separation of the pupillary membrane or irregular formation of iris muscles leads to multiple fully structured pupils. [11]
Clinical Relevance:
Due to its rarity, only a few documented cases of true polycoria exist in the literature, making it a subject of both academic and clinical curiosity.
b) Pseudopolycoria (False Polycoria)
Pseudopolycoria, or false polycoria, is a more commonly encountered form of the condition. While the iris appears to have multiple pupillary openings, only one central pupil is functional, and the additional holes are simply defects in the iris tissue without independent muscular control. [13]
Key Characteristics:
Etiology:
Pseudopolycoria can be: [14]
Diagnosis:
Clinical Management:
Etiology and Risk Factors
Polycoria arises from either congenital malformations or acquired damage to the iris. Understanding the etiology is essential for accurate diagnosis, especially in distinguishing between true and pseudopolycoria. [16]
a) Congenital Polycoria [17,20]
Congenital polycoria results from abnormal iris development during embryogenesis. The condition is typically present at birth and may occur in isolation or alongside other ocular anomalies.
Causes and Associations:
Risk Factors:
b) Acquired Polycoria (Pseudopolycoria) [21-23]
More common than the congenital form, acquired polycoria involves secondary defects in the iris without functional sphincter muscles.
Causes:
Pathophysiology
The pathophysiology of polycoria is rooted in the embryological development of the eye, particularly the formation of the iris. During normal fetal development, the iris arises from a combination of neuroectodermal and mesenchymal tissues. A crucial structure called the pupillary membrane forms over the developing lens and eventually regresses as gestation progresses, allowing for the formation of a single, central pupil. [24] In individuals with polycoria, this normal resorption or differentiation process is disrupted, resulting in the formation of one or more additional pupillary openings within the iris. These extra openings can be a result of retained remnants of the pupillary membrane or faulty morphogenesis of the iris tissue. The result is a condition where more than one opening appears in the iris, and the functional capacity of these openings defines whether the polycoria is true or pseudo. In true polycoria, each pupillary aperture has its own independently functioning sphincter pupillae muscle. This means that each pupil can constrict and dilate in response to light stimuli, although this condition is exceptionally rare. The true form implies a complete duplication of the muscular and neural elements responsible for pupil function — an anomaly that stems from a very specific and rare developmental error. [25] On the other hand, pseudopolycoria is more commonly observed and represents an incomplete or structurally defective form of the condition. In this case, the additional pupillary openings lack a sphincter muscle and thus do not react to light. These are often just holes or defects in the iris tissue, which may occur congenitally or be acquired later due to trauma, surgery, inflammation, or degenerative iris changes. Furthermore, structural abnormalities in the iris may extend to adjacent ocular structures. For example, maldevelopment of the trabecular meshwork, the eye’s drainage system for aqueous humor, may accompany polycoria. This can result in impaired outflow of intraocular fluid, leading to elevated intraocular pressure. Over time, such pressure changes can predispose the individual to secondary glaucoma, which is one of the most clinically significant complications associated with polycoria, particularly in syndromic or developmental cases.
In summary, the pathological basis of polycoria lies in developmental errors of the iris and associated ocular tissues, with implications not only for pupil structure and function but also for visual performance and intraocular pressure regulation. [26]
Clinical Features and Symptoms
The clinical presentation of polycoria is highly variable and largely depends on the nature of the condition specifically whether the individual has true polycoria or pseudopolycoria, and whether the associated pupillary defects cause functional impairment. Some individuals may remain entirely asymptomatic throughout life, while others may suffer from significant visual disturbances that interfere with daily activities. [27]
Asymptomatic Cases
In many cases, especially those involving pseudopolycoria with small or poorly positioned secondary openings, the condition may be clinically silent. These individuals typically present with normal visual acuity and no noticeable visual complaints. Polycoria in such cases is often detected incidentally during a routine ophthalmologic examination or while investigating unrelated eye issues. The secondary openings may be small and located peripherally, not significantly affecting the passage of light through the central visual axis. [28]
Symptomatic Cases [29,32]
When symptoms do occur, they can vary in severity and impact, depending on the size, location, and number of pupillary openings, as well as whether they distort the central visual pathway.
1. Diplopia (Double Vision)
One of the hallmark symptoms in symptomatic polycoria is diplopia, particularly if multiple functional pupils transmit light to the retina in a disorganized manner. This can create the perception of overlapping images, making visual tasks challenging, especially reading or driving.
2. Glare and Photophobia
Individuals may experience excessive glare, light sensitivity (photophobia), or discomfort in bright environments. These symptoms arise because light enters the eye through multiple pupillary openings that lack appropriate constriction control, resulting in scattered light hitting the retina.
3. Blurred or Reduced Visual Acuity
Multiple pupils may disrupt the eye's ability to focus light sharply on the retina, leading to blurred vision or decreased sharpness. The visual axis may be distorted, and the image quality can degrade, especially in cases of true polycoria.
4. Difficulty Focusing in Dim Lighting
The inability of the eye to regulate the amount of incoming light properly (due to dysfunctional or duplicated pupil muscles) can result in poor adaptation to low-light conditions. This is particularly problematic at night or in dim rooms, where patients may struggle to see clearly.
5. Visual Fatigue, Eye Strain, and Headaches
As the brain attempts to reconcile multiple visual inputs or cope with constant light scatter, patients may experience eye strain, visual fatigue, or even headaches during or after prolonged visual activities such as reading or screen use.
6. Pediatric Manifestations: Strabismus and Amblyopia
In children, the altered visual input from polycoria can interfere with the development of normal binocular vision. This may lead to strabismus (misalignment of the eyes) or amblyopia (lazy eye), especially if the condition is not detected and managed early. These complications emphasize the importance of early diagnosis in pediatric patients.
Associated Clinical Findings
In more complex cases, polycoria may be seen alongside other ocular abnormalities such as corectopia (displaced pupil), coloboma, or glaucoma, which can further influence the clinical presentation and complicate the visual outcome.
Diagnosis:
The diagnosis of polycoria requires a meticulous ophthalmologic evaluation, combining both clinical examination and advanced imaging techniques. The primary goal is to accurately differentiate between true polycoria and pseudopolycoria, assess pupillary function, and identify any associated ocular abnormalities, such as glaucoma or structural anomalies of the anterior segment. Because of its rarity and the potential for misdiagnosis, especially in cases of pseudopolycoria or acquired iris defects, clinicians must adopt a comprehensive approach. [33]
a) Slit-Lamp Biomicroscopy
The slit-lamp examination is a fundamental and initial diagnostic tool. It enables detailed visualization of the anterior segment of the eye, including the iris architecture.
b) Dilated Fundus Examination
A comprehensive fundus examination, typically performed after pharmacologic pupil dilation, helps rule out any posterior segment pathologies that could be contributing to visual symptoms or coexisting with polycoria.
• While polycoria primarily affects the anterior segment, underlying or concurrent retinal or optic nerve pathologies (e.g., coloboma, optic nerve hypoplasia) should be excluded, especially in congenital cases. [35]
c) Pupil Function Tests
Functional evaluation of each pupil is crucial in the diagnostic process.
The near reflex test (accommodation response) further evaluates the integrity of the pupillary sphincter mechanism.
Anterior Segment Imaging
Advanced imaging techniques such as:
• Ultrasound Biomicroscopy (UBM)
• Anterior Segment Optical Coherence Tomography (AS-OCT)
These modalities provide high-resolution cross-sectional imaging of the anterior segment structures.
e) Gonioscopy
Gonioscopic examination is performed to evaluate the iridocorneal angle—the drainage angle of the eye.
f) Visual Acuity and Visual Field Testing
Assessment of the functional impact of polycoria on vision is essential:
Visual acuity testing determines the extent of central vision impairment.
Visual field testing helps identify any field defects, which may occur due to light scatter from multiple pupils or underlying optic nerve pathology.
These evaluations also provide a baseline for monitoring progression and the effectiveness of any interventions. [39]
Differential diagnosis:
Accurate diagnosis of polycoria necessitates careful differentiation from other conditions that may mimic its appearance, particularly those involving structural abnormalities of the iris. Several other ocular pathologies can present with similar visual findings—such as irregular or multipleappearing pupillary openings—but differ significantly in etiology, pathophysiology, and management. The key conditions to consider in the differential diagnosis include: [40]
1. Corectopia
Corectopia refers to the displacement of a single pupil away from its normal central position. It may appear superficially as if there are multiple pupillary openings due to irregular iris pigmentation or shadows.
2. Iris Coloboma
Coloboma of the iris is a congenital defect resulting from incomplete closure of the embryonic fissure during ocular development. It typically presents as a keyhole-shaped notch or gap in the inferior portion of the iris.
• Distinguishing Features: Unlike polycoria, an iris coloboma does not form a separate pupillary opening. The defect is usually contiguous with the normal pupil and does not have a sphincter muscle.
Visual Impact: It may cause light sensitivity due to unregulated light entry but does not create a duplicate pupil. [42]
3. Iridodialysis
Iridodialysis refers to a tear or separation of the iris from its attachment at the ciliary body, usually as a result of blunt ocular trauma.
4. Surgical Iris Defects
Surgical interventions, such as iridectomy or iris manipulation during intraocular surgery (e.g., cataract extraction or glaucoma filtration procedures), may lead to iatrogenic defects in the iris.
Complications associated with polycoria:
Management and treatment:
Management of polycoria depends on the type, symptoms, and any associated ocular issues. Treatment aims to improve vision, reduce discomfort, and address complications.
a) Observation and Monitoring
Many patients with asymptomatic or mild polycoria require only regular observation. Routine eye exams monitor for changes in vision or development of complications such as glaucoma. This conservative approach is preferred when the condition is stable and non-progressive. [46]
b) Optical Correction
For patients with mild symptoms like glare or diplopia, tinted contact lenses or pupil occluders can be used. These devices block light entering through accessory pupils, improving focus and reducing visual disturbances without invasive procedures. [47]
c) Surgical Intervention
Surgery is reserved for symptomatic cases causing significant vision problems. Procedures include:
d) Management of Associated Conditions
Polycoria may coexist with other eye disorders:
Prognosis:
The prognosis of polycoria varies widely depending on several factors, including the severity of the condition, the presence of associated ocular complications, and the timing of diagnosis and intervention. In cases of congenital polycoria without any accompanying anomalies such as glaucoma or severe iris malformations, the outlook is generally favorable. Many individuals maintain good visual acuity and may remain asymptomatic throughout life. However, when diagnosis is delayed, particularly in pediatric patients, there is a significant risk of developing amblyopia (lazy eye) due to abnormal visual input during critical periods of visual development. If untreated, this can lead to permanent vision impairment. For symptomatic patients who undergo timely surgical correction—including iridoplasty or artificial iris implantation—there is often a substantial improvement in symptoms such as glare, double vision, and photophobia. Surgical outcomes are generally positive when performed by experienced surgeons with appropriate patient selection. [50] Overall, early detection and appropriate management are key to optimizing visual prognosis and minimizing long-term complications in patients with polycoria.
Recent advances and research perspectives:
Recent developments in ophthalmology have contributed significantly to the understanding and management of polycoria, opening new avenues for diagnosis and treatment.
Artificial Iris Implants
One of the most promising advances is the development of custom-made artificial iris implants. These prosthetic devices are designed to replace or reconstruct a damaged or malformed iris, providing both functional and aesthetic benefits. They help restore a single, central pupil, improving vision by reducing glare and photophobia, while also enhancing the cosmetic appearance for patients with severe iris defects. Modern implants can be tailored to match the patient’s natural iris color, allowing for personalized treatment options. [51]
Genetic and Molecular Research
Ongoing genetic studies are exploring the underlying hereditary factors and mutations associated with polycoria and related anterior segment dysgenesis syndromes such as Axenfeld-Rieger syndrome and aniridia. Understanding the molecular pathways involved in iris development could lead to earlier diagnosis, risk prediction, and potentially novel therapeutic approaches in the future. [52]
Imaging Advances
The advent of high-resolution imaging technologies, particularly anterior segment optical coherence tomography (OCT) and ultrasound biomicroscopy (UBM), has greatly enhanced clinicians’ ability to visualize fine iris details and associated structures. These imaging modalities provide precise information about the number, size, and location of accessory pupils and the condition of the iris sphincter muscles, which is critical for surgical planning and outcome prediction. [53]
CONCLUSION:
Polycoria is a rare and complex ophthalmic disorder characterized by the presence of multiple pupillary openings within a single iris, which can lead to a range of visual disturbances including glare, double vision, and reduced visual acuity. While some individuals remain asymptomatic, others—especially pediatric patients—may experience significant complications such as amblyopia and secondary glaucoma if diagnosis and management are delayed. Early and precise diagnosis using thorough clinical evaluation alongside advanced imaging techniques like anterior segment OCT is crucial to guide appropriate treatment. Management strategies vary widely, from simple observation in mild or asymptomatic cases to optical correction with tinted lenses and surgical interventions like iridoplasty or artificial iris implantation in more severe cases. Recent technological advances have improved both functional and cosmetic outcomes, yet the rarity of polycoria means that its genetic and developmental causes are still not fully understood. Continued research is essential to unravel the underlying mechanisms, optimize therapeutic approaches, and improve long-term prognosis. Ultimately, a multidisciplinary, individualized approach remains vital for preserving vision and enhancing quality of life for patients affected by this uncommon but potentially vision-impairing condition..
REFERENCES





Amruta Patil*, Sayali Patil, Iftesam Momin, Vaishnavi Khot, Aniket Thanekar, Dhanraj Jadge, A Review on Polycoria Condition, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 2196-2209. https://doi.org/10.5281/zenodo.15641510
 10.5281/zenodo.15641510
10.5281/zenodo.15641510