Shree Dev Bhoomi Institute of Education Science and Technology.
One of the most prevalent dermatological issues in the world today is fungal skin infections. It's According to research; 40 million people have fungal infections. Surface-level and Skin, keratinous tissues, and mucous membranes are all impacted by subcutaneous fungal infections. What superficial candidiasis of the mouth, skin, or genital tract, dermatophytic infections, and infections brought on by Malassezia folliculitis and pityriasis versicolor are the primary conditions caused by Malassezia. circumstances. One of two possible causes of systemic fungal infections is an opportunistic organism that infects an at-risk host, be connected to a more invasive organism, or be unique to a particular geographical region. These consist of. High bioavailability, lack of hepatic first-pass metabolism, consistent drug plasma concentrations and the non-invasiveness of the treatment. The primary barrier to the stratum corneum, the skin's outermost layer, penetrates drug molecules. As a result, overcoming this layer to improve transdermal drug delivery (TDD) is a prime area of research. curiosity. The purpose of this review article is to offer coverage and commentary on the most recent developments. in methods for improving TDD.
Because they are non-invasive, simple to administer, and capable of maintaining controlled and prolonged drug concentrations in plasma. In contrast to parenteral or oral methods, TDDS avoids the hepatic first-pass metabolism and the gastrointestinal tract, which lessens gastrointestinal irritation, enzymatic breakdown and erratic drug absorption. Humans coexist peacefully with the microbes in their environment, but an infection could arise from the nearby microbes when the immune system is compromised or the Pathogen concentrations can reach extremely high densities, but infectious diseases are a condition where the body reacts to the infecting agents, resulting in clinically exhibit symptoms and indicators. Prions, worms, helminths, fungi, viruses, bacteria, and parasites have all contributed to the spread of infectious diseases. Many antifungal medications are used in clinical settings to treat fungal infections, and they can be widely divided into five main classes: griseofulvin, echinocandins, azoles, allylamines, and flucytosine [1] Thus, there is an urgent need to find new antifungals. The phytochemistry of different plants species have suggested that phytochemicals may be a more effective source of medication than drugs that are manufactured artificially.
Advantages of Transdermal Drug Delivery system:
Disadvantages of Transdermal drug delivery system:
Anti-fungal agent:
A class of pharmaceutical substances known as antifungal agents is used to treat and prevent infections with fungi [26]. Fungi are a broad category of microorganisms that cause a variety of diseases that affect humans, animals, and plants [27]. These infections can range in severity from benign skin symptoms to potentially lethal systemic conditions [28, 29]. Antifungal medications have their effectiveness by preventing fungal organisms from proliferating and reproducing, interfering with fungi's distinct biological processes without harming host organisms [30]. They Agents may target vital elements, like the structural integrity of vital biosynthetic pathways or the production of essential cellular components like ergosterol, ultimately lowering the pathogenic fungus [31].
The antifungal agents are divided into several classes, each with its own unique mechanisms of action and range of activities [32]. The deliberate choice of an antifungal medication depends on elements like the fungal infection's type and location, the patient's medical condition, as well as possible drug interactions [33]. A few antifungal medications are given Some are applied topically to target localized infections [35], while others are applied systemically [34]. Lately, Research on the application of transdermal delivery for antifungal medications as a potentially effective delivery system [36]. We have examined and evaluated studies conducted between 2010 and the present on the transdermal administration of antifungal medications, highlighting important discoveries, explanations of the newly created formulations, and tactics used in administering the antifungal medications, as well as possible clinical results or uses.
The majority of antifungal medications disrupt the primary sterol ergosterol's biosynthesis or integrity. in the membrane of fungal cells [37]. The fungal cell wall is disrupted by others [38]. Considering their Antifungal agents can be divided into five classes based on their mechanisms of action: Polyenes, azoles, echinocandins, allylamines, and additional substances such as tolnaftate, flucytosine, and griseofulvin [39, 40].
TYPES OF FUNGAL INFECTIONS:
Topical/superficial disease caused by fungal pathogens:
The outermost layers of the skin, nails, hair, and mucous membranes can develop superficial fungal infections.[6] membranes Dermatophytosis, Tinea corporis (neck, trunk, extremities), Tinea pedis (foot), Tinea unguium or onychomycosis/nails (90% of toenail infections), Tinea capitis (childhood), and 50% of nail infections) [7,8], superficial candidiasis, oral, vaginal, and gastrointestinal tract. Oral thrush or oropharyngeal candidiasis (acute or chronic infection), Pregnancy vaginal discharge combined with candidiasis/vaginal thrush. Additionally, pruritus and recurrent episodes are possible. are prevalent), skin candidiasis (infections of the nail folds),
Malassezia infection:
Are typical surface commensals of oily skin, such as the chest and scalp, and they are connected to folliculitis, seborrheic dermatitis, and pityriasis versicolor [9].
Pityriasis versicolor:
A scaly, hypopigmented or hyperpigmented rash on the trunk, pityriasis versicolor is frequently Scaling is common in tropical areas, although the patches may resemble vitiligo.
Seborrheic dermatitis:
A common scaly condition that affects the face, front of the chest, and the skin is seborrheic dermatitis. skull. Patients with AIDS or chronic conditions are more likely to have severe seborrheic dermatitis. Parkinson's disease that is neurological.
Malassezia folliculitis:
An itchy, follicular rash on the shoulders and upper back caused by Malassezia folliculitis can resemble [10] acne.
Subcutaneous infection:
Subcutaneous mycoses typically only affect the dermis, though they can spread. tissues beneath the skin. For instance, chromoblastomycosis, sporotrichosis, and persistent mucocutaneous candidacy.
Systemic fungal infections:
There are two different categories of systemic fungal infections: The dimorphic or endemic Ecosse. These infections have a high mortality rate and are potentially fatal.
Egpathogens that are opportunistic. [11, 12].
Table 1:
The physicochemical properties of azoles, polyenes, echinocandins, allylamines, and other antifungal agents
|
Class |
Antifungal agent |
Physical appearance |
Molecular weight(g/mol) |
Melting point |
Log p |
Water solubility (mg/ml) |
Reference |
|
Azoles |
Ketoconazole Miconazole Clotrimazole Econazole Fluconazole Itraconazole Voriconazole Posaconazole |
Colourless crystals or powder White powder White to pale yellow crystalline powder White powder White crystalline powder White powder White powder White powder |
531.4 416.1 344.8 381.7 306.27 705.6 349.31 700.8 |
146 170 148 162 138-140 166.2 134 170-172 |
4.34 6.1 6.1 5.5 0.5 5.66 1 5.5 |
0.00029 at (at 20°C) 0.000763 (at 25°C) 0.00049 0.00148 0.0349 Insoluble 0.00978 Insoluble |
[41] [42] [43] [44] [45] [46] [47] [48] |
|
Polyenes |
Nystatin Natamycin Amphotericin-B |
Light yellow powder White to creamy crystalline powder Bright yellow powder |
926.1 665.7 924.1 |
160 290 170 |
-0.2 -1.3 0.8 |
0.104 0.03-0.05 <0.001 |
[49,50] [51,52] [53,54] |
|
Echinocandins |
Caspofungin Micafungin Anidulafungin |
Hygroscopic white to off-white powder Solid powder Solid powder |
1093.3 1270.3 1140.2 |
N/A N/A 234-238 |
0.3 -1.6 2.3 |
0.028 >0.2 0.05 |
[55,56] [55,57] [55,58] |
|
Allylamines |
Terbinafine Naftifine Butenafine |
Powder Powder White crystalline powder |
291.4 287.4 353.93 |
195-198 177 164-166 |
5.6 5.1 5.2 |
0.000738 0.000229 0.1 |
[59] [60] [61,62] |
|
Other antifungal agent |
Flucytosine Griseofulvin Tolnaftate |
White crystalline solid White to pale cream crystalline powder White crystalline powder |
129.09 352.8 307.4 |
296 220 111 |
-0.9 2.2 5.5 |
15 8.64 0.12 |
[63] [64] |
Definition:
A transdermal patch, also known as a skin patch, is a medicated adhesive patch that is applied to the skin in order to transfer a particular dosage of medication through the skin and into the bloodstream. [13]

Figure.1
Anatomy and physiology of skin
Three separate but interdependent tissues make up human skin: The cellular, vascular, and stratified layer known as the "epidermis" Hypodermis, the dermis beneath connective tissues.
Epidermis.
The thickness of the multilayered epidermis varies from 0.8 mm on the palms and soles to 0.06 mm on the eyelids, depending on the size and number of cell layers. Ten to twentyfive layers of corneocytes—dead, keratinized cells—are present. It is possible to model the horny layer's architecture as a wall-like structure. The keratinized cells serve as protein "bricks" embedded in lipid "mortar" in this model.
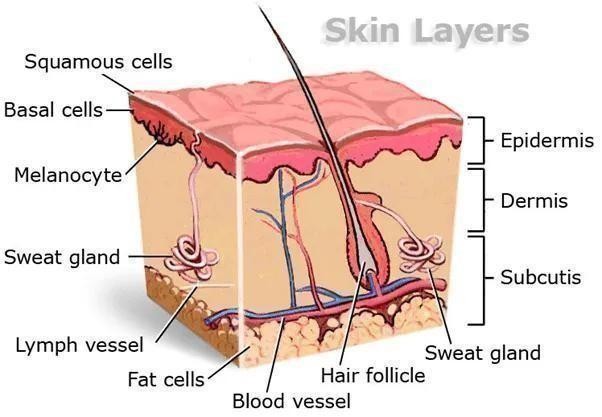
Fig.2 Structure of human skin Dermis:
Dermis:
The connective tissue matrix that makes up the 3–5 mm thick layer of dermis contains blood vessels, lymph vessels, and nerves. The majority of molecules that penetrate the skin barrier find a sink in capillaries, which extend to within 0.2 mm of the skin's surface.
Hypodermis:
The dermis and epidermis are supported by the hypodermis, or subcutaneous fat tissue. It acts as a place to store fat. This layer offers mechanical protection, nutritional support, and aids in temperature regulation. [14]
Components of transdermal patches:
Polymer Matrix: The drug's release from the device is regulated by the polymer. For a polymer to be utilized in transdermal patches, it must meet the following requirements.
Types of polymers: -
Physiochemical properties:
Biological properties:
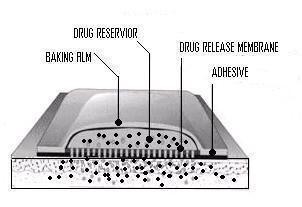
Fig. 3: Different parts of transdermal patch Permeation Enhancer:
Other excipients: a) Adhesives
Linear: Protect the patch during storage. The linear is removed prior to use.
Backing: Protect the patch from the outer environment. [15-16]
Factors affecting transdermal bioavailability: Two major factors affect the bioavailability of the drug via transdermal routes:
1.Physicochemical Factors: -
Skin hydration: Skin becomes much more permeable when it comes into contact with water. The most crucial element boosting skin penetration is hydration. Humectant is therefore used in transdermal delivery.
Temperature and pH: When the temperature changes, the drug's penetration increases tenfold. Therefore, pH and temperature have a significant impact on drug penetration.
Diffusion coefficient: Penetration of drug depends on diffusion coefficient of drug. Drug concentration: The concentration gradient across the barrier determines the flux, and a higher concentration gradient will result from a greater concentration across the barrier.
Partition coefficient:
Good action requires the optimal partition coefficient (K). High K drugs are unable to exit the lipid layer of the skin. Additionally, medications with low K won't penetrate.
Molecular size and shape:
Molecular weight and drug absorption are inversely correlated; small molecules enter the body more quickly than large ones. Biological Factors:
Types of transdermal patches:
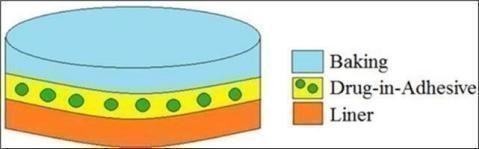
Single-layer Drug-in Adhesive: - The medication is also present in this system's adhesive layer. It is in charge of the drug's release in addition to transporting the entire system to the skin. A backing and a temporary liner encircle the adhesive layer. [17]
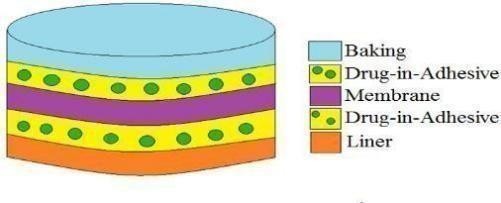
Multi-layer Drug-in-Adhesive: - The single-layer system and the multi-layer drug-in adhesive patch are comparable in that the drug is released by both adhesive layers. Additionally, this patch has a permanent backing and a temporary liner layer. [18]
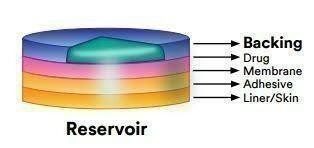
Reservoir: - The reservoir transdermal system has a distinct drug layer, in contrast to single-layer and multi-layer drug-in adhesive systems. The adhesive layer separates the drug layer, which is a liquid compartment with a drug suspension or solution. The backing layer supports this patch as well. The rate of release in this kind of system is zero order. [19]
Matrix: - The drug layer of the Matrix system is a semisolid matrix that holds a drug suspension or solution. In this patch, the drug layer is partially covered by the adhesive layer. [20]
Vapour Patch: - The adhesive layer in this kind of patch releases vapor in addition to holding the different layers together. The vapor patches are brand-new on the market and they release essential oils for up to 6 hours. Vapour patches that reduce the quantity of cigarettes
that one smokes in a month are also available on the market. [21]
Basic Components of TDDS:
•Polymer matrix / Drug reservoir
•Drug
•Permeation enhancers
•Pressure sensitive adhesive (PSA)
•Backing laminates
•Release liner and other excipients like plasticizers and solvents Polymer matrix / Drug reservoir:
The foundation of TDDS is made up of polymers, which regulate the drug's release from the apparatus. Drug dispersion in a liquid or solid-state synthetic polymer base can create a polymer matrix. The polymers used in TDDS should be chemically and biocompatible with the medication and other system elements like PSAs and penetration enhancers. The polymers utilized for TDDS can be classified as: Natural Polymers: e.g. cellulose derivatives, zein, gelatine, shellac, waxes, gums, natural rubber and chitosan etc.
Synthetic Elastomers: e.g. polybutadiene, hydrin rubber, polyisobutylene, silicon rubber, nitrile, acrylonitrile, neoprene, butyl rubber etc.
Synthetic Polymers: such as polyvinyl alcohol, polyvinyl chloride, polyethylene, polypropylene, polyacrylate, polyamide, polyurea, polyvinylpyrrolidone, polymethylmethacrylate, etc.
Drug:
For medications with suitable pharmacology and physical chemistry, the transdermal route is a very appealing choice. Transdermal patches are a great option for medications that go through a lot of first pass metabolism, have a limited therapeutic window, or have a short half-life that makes frequent dosing difficult.
Permeation Enhancers: Three pathways—polar, non-polar, and polar/non-polar—are proposed for drug penetration through the skin. One of these pathways is changed by the enhancers. The secret to changing the polar pathway is to induce solvent swelling or a change in the conformation of proteins. There are two types of methods used to modify the SC's barrier properties in order to improve drug penetration (and absorption) through the skin: (1) chemical methods and (2) physical methods of enhancement. [22]
Chemical Enhancers:
Chemical enhancers act by
Physical enhancers:
Physical methods of enhancement, such as iontophoresis and ultrasonography (also called phonophoresis or sonophoresis), have been employed to improve the percutaneous penetration (and absorption) of different therapeutic agents.
Pressure sensitive adhesives:
A PSA is a substance that aids in preserving close contact between the skin's surface and the transdermal system. The diffusing medication must not have an impact on the face adhesive in reservoir systems.
Backing Laminate:
The most crucial factor to take into account when designing a backing layer is the material's chemical resistance. The backing with the lowest modulus, or high flexibility, good oxygen transmission, and a high rate of moisture vapor transmission will be the most comfortable.
Release Liner:
When designing a backing layer, the material's chemical resistance is the most important consideration. The most comfortable backing will have the lowest modulus, or high flexibility, good oxygen transmission, and a high rate of moisture vapor transmission.
Other excipients:
Drug reservoirs are prepared using a variety of solvents, including dichloromethane, methanol, acetone, isopropanol, and chloroform. To give the transdermal patch flexibility, plasticizers like di-butylpthalate, triethyl citrate, polyethylene glycol, and propylene glycol are also added.
Evaluation of transdermal patches: -These studies are predictive of transdermal dosage forms and can be classified into following types:
Physicochemical evaluation: -
Thickness: A traveling microscope, dial gauge, screw gauge, or micrometer is used to measure the thickness of transdermal film at various film locations.
Uniformity of weight: A digital weighing machine was used to weigh each patch in order to conduct a weight variation test. For every formulation, the measurements were made in triplicate. Next, the average weight and standard deviation were computed. Folding Endurance: The purpose of this test was to evaluate the strength of the patch made with various polymers and the effectiveness of the plasticizer. The number of folds needed to shatter any polymeric patch is known as folding endurance.
Drug content determination: A precisely weighed amount of film (roughly 100 mg) is dissolved in 100 mL of an appropriate drug-soluble solvent, and the mixture is then continuously shaken for 24 hours in a shaker incubator. After that, the entire mixture is sonicated. The drug in solution is measured spectrophotometrically using the proper dilution following sonication and filtration.
Moisture content: The prepared films are weighed separately and stored for 24 hours at room temperature in a desiccator with calcium chloride. After a predetermined amount of time, the films are weighed once more until their weight remains constant. Surface pH: For one hour, patches were placed in glass tubes with 0.5 ml of doubledistilled water and allowed to swell. After a minute of equilibration, a combined glass electrode was brought close to the patch's surface, and pH readings were obtained.
In vitro evaluation: -
Two features of the dosage forms that are crucial in characterizing the drug dissolution profile from controlled release dosage forms and, consequently, there in vivo performance are drug release mechanisms and kinetics. The drug release rate of TDDS can be determined using a variety of techniques, and several mathematical models have been developed to describe the drug dissolution kinetics from controlled release drug delivery systems.
To evaluate the effectiveness, risk, side effects, patient compliance, etc., clinical trials have been carried out. Phase II clinical trials assess short-term safety and primarily efficacy in patients, while phase I clinical trials focus primarily on safety in volunteers. Phase IV trials are conducted at post-marketing surveillance for marketed patches to identify adverse drug reactions, while phase III trials show the safety and efficacy in a large patient population. [23, 24]
In vivo evaluation: -
The real representation of the drug's performance is found in in vivo evaluations. In vivo studies allow for a thorough exploration of the variables that cannot be considered in in vitro studies. TDDS can be evaluated in vivo using the following methods: [25]
CONCLUSION
The controlled and continuous delivery of drugs into the systemic circulation is made possible by the transdermal drug delivery system (TDDS), an efficient, secure, and patient-friendly technique. TDDS is especially useful for antifungal agents because it avoids first-pass metabolism, lessens gastrointestinal irritation, and keeps drug levels constant, all of which increase therapeutic efficacy.
Transdermal patches present a promising and cutting-edge alternative for antifungal therapy in light of the growing prevalence of fungal infections, the scarcity of effective medications, and the rise in resistance. The potential of TDDS has been further enhanced by the use of polymer matrices, permeation enhancers, and cutting-edge technologies like microneedles and 3D printing.
TDDS is still developing and has great potential as a dependable and cutting-edge platform for upcoming antifungal treatments, despite issues like skin permeability, drug potency, and local irritation.
REFERENCES
Glibenclamide Lowers Blood Glucose Levels in Rats.Diabetes Res.Clin. Pract.1990; 8:19- 22.
Permeation Enhancement in Vivo in Humans. Jour. Control. Release. 1995; 37:299306.
Glibenclamide Lowers Blood Glucose Levels in Rats.Diabetes Res.Clin. Pract.1990; 8:19- 22.
Permeation Enhancement in Vivo in Humans. Jour. Control. Release. 1995; 37:299306.

Anand Kumar, Vandana Sahani, Dr. Shivanand Patil, A Review on Transdermal Patch of Clotrimazole for Fungal infection., Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 01-13, https://doi.org/10.5281/zenodo.19368548
 10.5281/zenodo.19368548
10.5281/zenodo.19368548
