
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
New Montfort Institute of Pharmacy Ashti Dist. Wardha.
Peptic ulcer is a chronic disease affecting up to 10% of the world’s population. The formation of peptic ulcers depends on the presence of gastric juice pH and the decrease in mucosal defenses. Peptic ulcer disease occurs mainly due to consumption of NSAIDs, infection by H. pylori, stress, or due to a pathological condition such as Zollinger –Ellison Syndrome are the two major factors disrupting the mucosal resistance to injury. Conventional treatments of peptic ulcers, such as proton pump inhibitors (PPIs) and histamine-2 (H2) receptor antagonists, have demonstrated adverse effects, relapses, and various drug interactions. Mucoadhesion can be defined as a state in which two components, of which one is of biological origin, are held together for extended periods of time by the help of interfacial forces. Among the various transmucosal routes, buccal mucosa has excellent accessibility and relatively immobile mucosa, hence suitable for administration of retentive dosage form. The objective of this paper is to review the works done so far in the field of mucoadhesive buccal drug delivery systems (MBDDS), with a clinical perspective. Starting with a brief introduction of the mucoadhesive drug delivery systems, oral mucosa, and the theories of mucoadhesion, this article then proceeds to cover the works done so far in the field of MBDDS, categorizing them on the basis of ailments they are meant to cure. Additionally, we focus on the various patents, recent advancements, and challenges as well as the future prospects for mucoadhesive buccal drug delivery systems.
Peptic Ulcer
Peptic ulcer is one of the most common, chronic gastrointestinal disorder in modern era. Now it has become a common global health problem affecting a large number of people worldwide and also still a major cause of morbidity and mortality. Peptic ulcer disease can be characterized by inflamed lesions or excavations of the mucosa and tissue that protect the gastrointestinal tract. Damage of mucus membrane which normally protects the oesophagus, stomach and duodenum from gastric acid and pepsin causes peptic ulcer. The pathophysiology of this gastro-intestinal disorder is viewed as an imbalance between mucosal defensive factors such as bicarbonate, prostaglandin, nitric oxide, peptides, growth factors and injurious factors like acid, pepsin. Various factors are implicated that play a pivotal role in the pathogenesis of ulcerations like, sedentary life style, alcohol intake, spicy food, drugs and various bacterial infections. Prevalence of peptic ulcer has reduced from past few years mainly due to an effective treatment of H. pylori infection eradication, however widespread use of NSAIDs and aspirin (acetylsalicylic acid) causes certain gastrointestinal complications. NSAIDs and aspirin may lead towards gastrointestinal mucosal injury, and hence the complications. Various drug regimens available include proton pump inhibitors (PPIs), H2 receptor antagonist, antacids, antibiotics and mucosal protective agents. The diagnostic tests include blood tests, urea breadth test, stool antigen test and endoscopy.[1] Peptic ulcers are open sores that develop on the inside lining of your stomach and the upper portion of your small intestine, and in most cases, stomach pain is the most common symptom of a peptic ulcer. Peptic ulcer is an acid-induced lesion of the digestive tract that is usually located in the stomach or proximal duodenum, and is characterized by denuded mucosa with the defect extending into the submucosa or muscularis propria [2]. The estimated prevalence of peptic ulcer disease in the general population is 5–10% [3], but recent epidemiological studies have shown a decrease in the incidence, rates of hospital admissions, and mortality associated with peptic ulcer [4,5]. This is most likely secondary to the introduction of new therapies and improved hygiene, which resulted in a decline in Helicobacter pylori (H. pylori) infections. Traditionally, mucosal disruption in patients with the acid peptic disease is considered to be a result of a hypersecretory acidic environment together with dietary factors or stress. Risk factors for developing peptic ulcer include H. pylori infection, alcohol and tobacco consumption, non-steroidal anti-inflammatory drugs (NSAIDs) use, and Zollinger–Ellison syndrome [6]. The main risk factors for both gastric and duodenal ulcers are H. pylori infection and NSAID use [7]. However, only a small proportion of people affected with H. pylori or using NSAIDs develop peptic ulcer disease, meaning that individual susceptibility is important in the beginning of mucosal damage. Functional polymorphisms in different cytokine genes are associated with peptic ulcers. For example, polymorphisms of interleukin 1 beta (IL1B) affect mucosal interleukin 1β production, causing H. pylori-associated gastroduodenal diseases [8]. On the other hand, the risk of complications of peptic ulcer is increased four times in NSAID users, and two times in aspirin users [9]. The concomitant use of NSAIDs or aspirin with anticoagulants, corticosteroids, and selective serotonin reuptake inhibitors increase the risk of upper gastrointestinal bleeding [10]. Although many people who use NSAIDs or aspirin have concurrent H. pylori infection, their interaction in the pathogenesis of peptic ulcer disease remains controversial. A meta-analysis of observational studies resulted in a conclusion that NSAIDs, aspirin use, and H. pylori infection increase the risk of peptic ulcer disease independently [11]. H. pylori-negative, NSAID-negative, and aspirin-negative peptic ulcer disease, which is classified as an idiopathic ulcer, can be diagnosed in about one-fifth of cases [12]. It is caused by the imbalance between factors that contribute to mucosal integrity and aggressive insults, but the pathogenic mechanisms behind the development of idiopathic peptic ulcer are still unknown [6]. A Danish study showed that psychological stress could increase the incidence of peptic ulcer [13]. Other etiologies include ischemia, drugs (steroids, chemotherapeutic agents) and radiotherapy, viruses, histamine, eosinophilic infiltration, gastric bypass surgery, and metabolic disturbances [14].
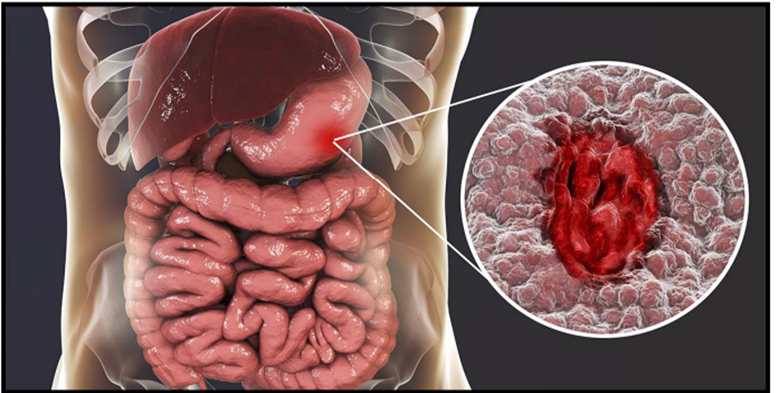
Figure 1. Peptic Ulcer
Epidemology
The presence or absence of Helicobacter pylori (H. Pylori) determines the incidence and prevalence of PUD. Countries with greater rates of H. pylori infection have higher rates. About 1 percent of those with H. pylori infection get PUD annually, which is 6–10 times higher than the rate for those without the infection. According to a population-based one-year prevalence of PUD of 0.1 to 1.5 percent based on physician diagnosis and 0.1 to 0.19 percent based on hospitalisation data, a systematic review of seven studies from affluent nations revealed. According to a study conducted in the United States, 2% of asymptomatic persons with H. pylori positivity had endoscopic point prevalence for peptic ulcers.Other studies, in presumably asymptomatic subjects in whom H. Pylori status was unknown, have reported an endoscopic point prevalence ranging from 1 and 6 percent. The incidence of peptic ulcer disease has changed from being more common in men to being equally common in women. For men, the lifetime prevalence is roughly 11%–14%, and for women, it is 8–11%. When it comes to ulcer occurrence, age trends show that older women have higher rates and younger men have dropping rates, especially for duodenal ulcers [15].
Etiology
A mucous layer covers your digestive tract, which often shields it from acid. However, an ulcer could form if there is a decrease in mucus or an increase in acid [16]. The most common causes of pud are.
· H pylori induced pud
· NSAIDS induced pud
· Stress induced pud
· Other medications
H pylori induced PUD This widespread bacterial illness affects about half of the world's population and is present in the stomach and/or duodenum. It doesn't seem to cause any problems for the majority of people. Children are primarily affected by H. pylori infection. It is more prevalent in underdeveloped nations. About 5% of children under the age of 10 in the United States have H. pylori bacteria. Children who live in crowded regions and unsanitary conditions are more likely to become infected[17]. It can spread from person to person by intimate physical contact, such kissing. H. pylori can also be acquired by eating and drinking [16].
NSAIDS induced PUD
NSAIDs or nonsteroidal anti-inflammatory medicines are the cause of the initial gastric ulcer and encourage its sequelae, including bleeding and perforation. Important risk factors for the formation of ulcers include age over 60, a history of ulcer illness in the past, and concurrent corticosteroid use [18]. The stomach lining may become immediately irritated by NSAID use, which facilitates the formation of ulcers. Prostaglandins are a class of substances that have the potential to regulate the stomach's protective lining. NSAIDs may interfere with these chemicals [19]. These medications include ibuprofen (Advil, Motrin IB, others), naproxen sodium (Aleve, Anaprox DS, others), ketoprofen and others [16].
Stress induced PUD
A stress ulcer result from physiological stress, not psychological, and can lead to the upper gastrointestinal bleeding. It may be a single or multiple mucosal defects and is often associated with shock, sepsis, trauma, or chronic illnesses. These ulcers are a major concern for patients in critical and intensive care settings[20].
Other medications
Taking certain other medications along with NSAIDs, such as steroids, anticoagulants, low-dose aspirin, selective serotonin reuptake inhibitors (SSRIs), alendronate (Fosamax) and risedronate (Actonel), can greatly increase the chance of developing ulcers[16].
Types of ulcer
Peptic Ulcer Peptic ulcer is a broad term which includes ulcers of digestive tract in the stomach or the duodenum. Earlier it was believed that one developed this type of ulcers due to stress and spicy food. However, recent research has shpwn that these are just the aggravating factors. The causative agent is infection caysed by the bacteria H. pylori or reaction to certain medicines like non-steroidal anti inflammatory drugs. Symptoms of peptic ulcers include weight loss, poor appetite, bloating, nausea, and vomit and black stools that indicate gastrointestinal bleeding.
Aphthous Ulcers
Sores that develop in the inner lining of the mouth are referred to as mouth ulcers. Mouth ulcers are common and are usually due to trauma such as from ill fitting dentures, fractured teeth, or fillings, Anemia, measles, viral infection, oral candidiasis, chronic infections, throat cancer, mouth cancer and vitamin B deficiency are some of the common causes of ulcers or sores in the mouth. Aphthous minor is amongst the most common from of oral ulcerative diseases and affects an estimated 15-20% of the population worldwide. In some populations, the prevalence has been documented as being as high as 50- 66% and it is especially common in North America. The incidence of aphthous ulcers has been found to be lower in smokers than in non -smokers.[21]
Causes Of Peptic Ulcer
1. Helicobacter pylori infection.
H.Pylori infection is the leading cause of stomach ulcers. After entering the stomach, this bacterium will get into the mucous layer of the gastric mucosa, secreting toxins that damage the gastric mucosa, inhibit the production of protective factors of the stomach lining, forming scars ulcer.
2. Long-term use of non-steroidal anti-inflammatory drugs (NSAIDs)
The long-term use of NSAID drugs such as ibuprofen, naproxen, diclofenac, etc. will cause stomach damage. These drugs inhibit the synthesis of prostaglandins, reducing the protective effect of the gastric mucosa, making the stomach susceptible to ulcers.
3. Other causative agents
Increased acid secretion in the stomach, this can happen for a variety of reasons, including genetic factors, smoking, stress, or the consumption of certain foods.
Peptic ulcer disease can also occur if you have a rare condition called Zollinger-Ellison syndrome. This condition forms a tumor of acid-producing cells in the digestive tract. These tumors can be cancerous or noncancerous. The cells produce excessive amounts of acid that damages stomach tissue.[1]
Symptoms
The most common peptic ulcer symptom is burning stomach pain. Stomach acid makes the pain worse, as does having an empty stomach. The pain can often be relieved by eating certain foods that buffer stomach acid or by taking an acid-reducing medication, but then it may come back. The pain may be worse between meals and at night. Many people with peptic ulcers don't even have symptoms. Less often, ulcers may cause severe signs or symptoms such as:
· Vomiting or vomiting blood
· Nausea or vomiting
· Unexplained weight loss
· Appetite changes
· Feeling faint
· Trouble breathing
· Dark blood in stools, or stools that are black or tarry
If symptoms remain untreated, it may lead to complications like gastrointestinal bleeding, perforations, penetration, narrowing and obstruction.[1]
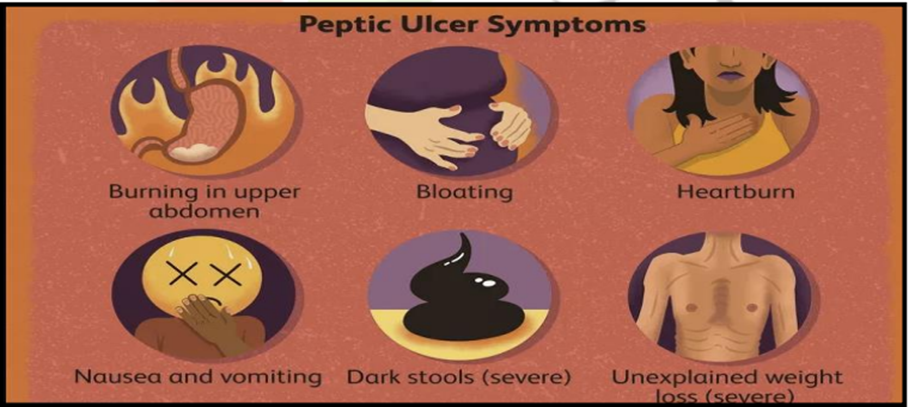
Figure 2. Peptic Ulcer Symptoms
Mucoadhesive tablets
The oral route of drug administration is the most common and preferred route for drug delivery, as it enables easy ingestion, selfmedication, accurate dosage, flexible and controlled dosing schedule, and patient compliance with a low chance of administration difficulty [22, 23]. It also has some major disadvantages such as the first-pass effect, gastrointestinal enzymatic degradation, and slow onset of action [24]. To overcome these disadvantages, mucoadhesive drug delivery and sublingual drug delivery could be better alternatives [25]. Mucoadhesive dosage forms are specially designed to adhere to the mucosal surface, thus intensifying retention of the drug at the site of application, while providing a controlled rate of drug release for better therapeutic outcome [26]. To mention, a few mucoadhesive drug delivery systems are adhesive patches, adhesive gels, adhesive tablets, adhesive films, adhesive discs, etc. [27]. Several regions such as the gastrointestinal (GI) tract, the urogenital tract, the ear, the nasal route, and the airways in the body are lined by the mucosal layer. These are either single-layered epithelium found in the GI tract, bronchi, and intestines or multilayered stratified epithelium found in the esophagus, vagina, and cornea and are the potential sites where mucoadhesive drug delivery systems can be useful [27, 28]. Buccal mucosa is one of such mucosal site which has a high extent of vascularization and enables direct drain of blood flow into the jugular vein, which helps to avoid the possible metabolism of drugs by the gastrointestinal route and liver [29]. The buccal delivery thus implies the absorption of medication through the mucosal lining of the buccal cavity. Easier drug administration, the possibility of prompt termination in the condition of unpredicted side effects and emergencies, the possibility of incorporating enzyme inhibitor/permeation enhancer, etc. are other major advantages of this drug delivery system [30, 31]. Various mucoadhesive polymers (natural, semi-synthetic, and synthetic) used in this delivery system become adhesive on hydration [32], therefore can be used for targeting a drug to a particular region of the body. Initially, when the mucoadhesive product is in contact with the mucosal membrane, it swells and spreads, initializing deep contact with the mucosal layer and then mucoadhesive materials (polymers) are activated by the presence of moisture and drug releases slowly [33]. On the other hand, aceclofenac is a potent cyclooxygenase-2 (COX-2) inhibitor, a newer non-steroidal anti-inflammatory drug (NSAID) with good anti-inflammatory, analgesic, and anti-pyretic activity, most commonly used for the treatment of osteoarthritis, rheumatoid arthritis, dental pain, and other rheumatoid disorders. It is an aryl acetic acid derivative, insoluble in water and highly permeable. It is characterized as a biopharmaceutical classification system (BCS) class II drug [34, 35]. It is highly protein-bound and possesses a short biological half-life of 4–4.3 h. The usual dose of aceclofenac is 100 mg twice or thrice daily [36]. The conventional dosage form of aceclofenac leads to a lot of inconvenience and fluctuations in therapy, with some adverse effects like gastrointestinal disturbances, peptic ulceration, and gastrointestinal bleeding. Thus, devising sustained-release medication is a good alternative for reducing its dosing frequency, for prolonged effect with improved bioavailability, while also improving safety and efficacy of the medication [34]. This study was designed to formulate the different batches of mucoadhesive aceclofenac tablets by using different polymers like carbopol 934, hydroxypropyl methylcellulose, and sodium carboxymethylcellulose along with their quality control evaluation.
Mechanism of mucoadhesion
Usually four categories of bio-adhesion have been notable within the biological process. They are commonly stated as a unification of (i) a normal cell to a further normal cell; (ii) a standard common cell to a pathological cell (iii) a cell to a foreign matter; and (iv) an bonding agent to biological substances. In case of mucoadhesion, the foremost phase includes a friendly get in touch with a muco-adhesive material as well as mucus or a biological membrane by each, because of a superior wetting or swelling of the bio-adhesive. The overall mechanism basically includes creation of mucoadhesive bond. Broadly the stages of mucoadhesion composed of two important stages i.e. contact stage (primary) and consolidation stage (secondary).
Step I (contact stage)
It involves the wetting and consequently swelling of the bioadhesive or polymer which takes place when a polymer is placed on the mucous membrane and results in to a deep contact. Here polymer swelling arises since the substances of polymer have an attraction for water.
Step II (polymer chains and mucosal membrane Interpenetration)
Just like that in the second phase, the polymer chains of mucoadhesive and the mucosal layer can interact and entangles by formation of adhesive bonds. Later on the contact has been recognized and perforation of the bioadhesive into the crevices of tissue exterior portion. Afterwards a correlation exists and bioadhesive chains impregnate with those of mucus. This phenomenon also had been occurred by force of bonds which rely on extent of perforation among two polymer groups.
Step III (bonds creation among the entwined chains)
Here both collectively recognized as consolidation stage. In this case, the weak chemical bonds can resolve at that time which was depicted in Figure 1. Other types of bond comprise covalent bonds and secondary interactions like hydrogen bonds as well as Vander Waals bonds.
Factors affecting mucoadhesion
A. Polymer related factors: Several properties or characteristics of the active polymer play a vital role in mucoadhesion. Among them, polymer molecular weight, concentration, swelling, of polymer chains flexibility, and particular confirmation which may affect the mucoadhesion.
B. Environment associated factors: pH of the polymersubstrate interface, functional strength and first contact time is able to influence the mucoadhesion.
C. Physiological factors: Disease state and mucin turn over are the important physiological factors, which can also affect mucoadhesion.
Mucoadhesion theories
Mucoadhesion will be able to outline and it is concerned with molecular interactions. The interaction between two molecules is composed of repulsion as well as attraction. The attractive interface would be superior to that of non-specific repulsion. The appropriate occurrence of mucoadhesion, these diverse forces of interactions is entirely narrated by the subsequent theories.
Electronic theory
Electronic hypothesis concerned to the principle that jointly mucoadhesive and biological materials acquire divergent electrical charges, thus when both resources make contact with, each other, then they swap over electrons foremost to construct a twofold electronic layer at the boundary, where the striking forces within this electronic twofold layer, found out the mucoadhesive potency.
Adsorption theory
As stated by the adsorption theory, the mucoadhesive machine coheres to the mucus by means of secondary chemical interactions, for example in Vander Waals forces and electrostatic attraction hydrogen bonds, or by means of hydrophobic interactions.
Wetting theory
The wetting theory implies to liquid systems which related to the current affinity to the surface in order to broadcast over it. Contact angle which is considered as one of the prime measurement tools for the creation of such kind of affinities. The universal rule indicates that the greater affinity correlates to lower the contact angle. The contact angle is supposed to be the identical or close up to zero in order to afford sufficient spreadability.
Diffusion theory
Diffusion theory narrated to the inter-perforation together of mucin as well as chains of polymer up to an adequate depth in order to build up a semi-permanent adhesive bond. Such a penetration rate absolutely be contingent on the several parameters such as nature of the mucoadhesive chains, diffusion coefficient, flexibility, motility in association with contact time.
Fracture theory
This is probably one of prime well-known theory in studies, associated to the mucoadhesion measurement by mechanical processes. Once complete formation of adhesion, it totally examine the force required to take apart both thesurfaces.
Mechanical theory
By proper packing of the irregularities upon a mucoadhesive liquid coarse surface that finally taken as one of the important factor which leads to consideration of adhesion phenomenon by mechanical concepts. In addition to this, such coarseness or roughness steadily grows the interfacial area that’s obtainable for interactions by the subsequent addition of squandering energy and it will be take into account of most significant observable fact of the procedure.
Mucosal docked vesicle theory
This theory implies about at specific mucosal epithelium vital absorption merely takes place. It may probable that the globules simply can interrelate with the mucous as well as mucosal basal membrane exclusively. Pharmacologically active drugs secluded, in the vesicle that may be liable to spread transversely to the basal membrane of mucosal layer and come into the blood stream for effective distribution at the time of occurrence of docking or releasing.[37]
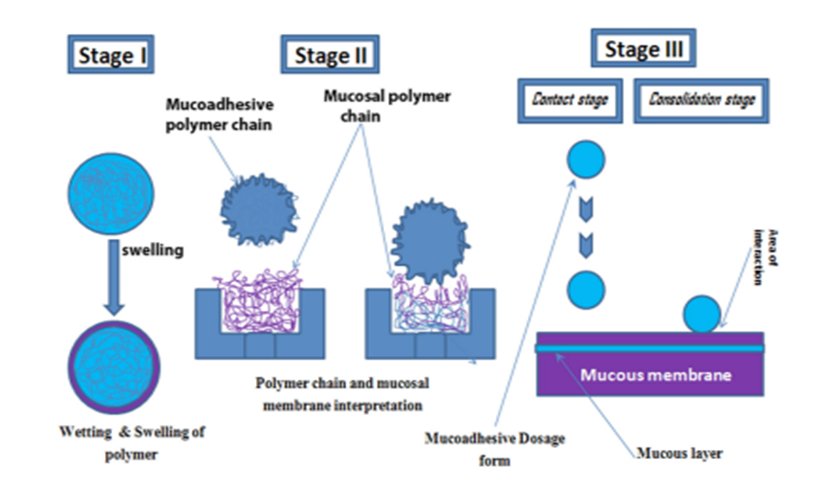
Figure 3. Steps Involved in Mechanism of Mucoadhesion.
Mucoadhesive materials
A supreme mucoadhesive substance should exhibit the capability to integrate jointly hydrophilic and lipophilic drugs. They must illustrate properties of mucoadhesive in its both liquids as well as solid forms. They supposed to be restraining the enzymes of local region otherwise to elevate absorption and should own definite molecular weight and chain length. They should be restricted for meticulous cellular site. They should have an extensive safety range and also they induces endocytosis. Bioadhesive materials are invoked just because of absorption promotes for several routes of administration. Considering the polymers discovery in the earlier year and the later year (20thcentury), they are broadly divided into two categories: (i) First generation or earlier generation mucoadhesive materials and (ii) Second generations or novel mucoadhesive materials.
First generation mucoadhesive materials
The first generation mucoadhesive substances are often natural molecules or sometimes of synthetic hydrophilic substances enclosing abundant organic functions (carboxyl, hydroxyl and amino groups) that generate hydrogen bonds, which do not stick on especially onto numerous surfaces. Denture fixers were found to be the foremost utility of mucoadhesive materials and the wellknown specimens are alginates, chitosans, derivatives of cellulose and carbomers. These are broadly categorized into three types.
A. Cationic: The Cationic molecules will be capable of interrelate with the surface of mucous, because of its charged which is negative at physiological pH. Mucoadhesion takes place by electrostatic interactions of mucin, containing sialic category along with the amino category in layer of mucous.
B. Anionic: The polymers of synthetic variety have been derived from poly acrylic acid (Carbomer) which are not only mucoadhesive but also it bears negative charge. In such conditions the physical-chemical yields and parameters (just as instance: van der Waals and hydrogen bonds, hydrophobic interactions,) plays a vital role in the configuration of mucoadhesion that are regulated by the ionic composition as well as pH. One of the broad utility of mucoadhesive systems are polyacrylic acid hydrogels. c. Non-ionic polymers: Non-ionic polymers include hydroxyl propyl-methyl cellulose, hydroxyethyl cellulose, and methyl cellulose, a current weaker force of mucoadhesion compared to anionic polymers.[38]
Second generation materials
New mucoadhesive systems composed of multifunctional materials. They are an alternative to non-specific bioadhesives since they stick on to definite chemical structures upon the surface of mucous or cell. Generally proteins of fimbrial types, lectins, invasions as well as which are acquired by the thiol groups containing cations are to identify, the molecules are some of the instance of these substances.[39]
Aim:
Formulations and evaluation mucoadhesive tablet of treatment peptic ulcer
Objective:
1. Formulate mucoadhesive tablets
2. Evaluate mucoadhesive properties
3. Determine in vitro drug release
4. Optimize tablet formulation
5. Evaluate tablet stability
6. Investigate in vivo performance
MATERIALS AND METHODS
Formulation of mucoadhesive buccal tablets of aceclofenac
Drug and chemicals
Aceclofenac (99.97% pure with loss on drying 0.34%) was obtained as a gift from Time Pharmaceuticals Pvt. Ltd, Nepal. Carbopol 934 (CP) was purchased from Himedia Laboratories India. Hydroxypropyl methylcellulose (HPMC) and sodium carboxymethylcellulose (SCMC) were purchased from Loba Chemie Pvt. Ltd, Mumbai. Magnesium stearate, micro crystalline cellulose powder 200 (MCCP 200), and talc were purchased from Sigma-Aldrich, Inc. (St Louis, MO, USA). All the chemicals and reagents used were of analytical grade.
Instruments
High Performance Liquid Chromatography (HPLC) (prominence-i LC2030, Shimadzu, Japan), FTIR Spectrophotometer (Perkin-Elmer FTIR, Perkin-Elmer, USA), Dissolution apparatus and digital hardness tester (Electrolab India), Friability tester (Toshiba, India), UV spectrophotometer and vernier caliper (Shimadzu, Japan), laboratory water purification system (HiTech Instruments Co. Ltd, China), Tablet compression machine (punch) 10 station (Shiva Pharma Engineering India).
Formulation of aceclofenac mucoadhesive tablets
Mucoadhesive tablets were prepared by adopting a previously established method with slight modification. Direct compression technique was applied for the tablet compression, using varying proportions of different grades of polymer. All the powders in pure form were accurately weighed. Aceclofenac was then mixed with CP. The remaining polymers were mixed with talc in a separate pouch. These two mixtures were then mixed for 5 min after passing through a 40 mesh sieve. MCCP 200 and aerosil were mixed in a separate pouch for 2 min. Then it was mixed with the previous mixture for 5 min. Finally, magnesium stearate was added and the resultant mixtures were mixed and the blend was then compressed into tablets having an average weight of 250 mg, using a ten station tablet punch. Twelve batches were prepared and coded from B1 to B12. The details of the composition of each batch were obtained from the previous study.
Evaluation of tablet properties
Different quality control parameters of all the batches of mucoadhesive aceclofenac tablets were analyzed by adopting the method described in Indian Pharmacopeia 2018.
Weight variation
Twenty tablets (n ¼ 20) from each batch were weighed using electronic balance and their average weight was calculated.
Friability
Twenty tablets (n ¼ 20) of each batch were weighed and put into the friabilator drum. After 100 revolutions of friabilator, tablets were recovered. The tablets were then freed from dust and weighed. Friability was calculated from the Eq.
Hardness
Twenty tablets (n ¼ 20) were taken for the hardness test using a hardness tester. The tablet was placed between the two probes, of which, one is a movable probe and another is an immovable probe of the hardness tester. Then the force was applied from the movable probe. The force to break the tablet was recorded, which was taken as the hardness of the tablet.
Drug content
HPLC chromatographic condition for drug content determination.
For the drug content assay of newly formulated batches, a reverse phase HPLC system was used. The chromatographic condition for the analysis was selected from pharmacopeial assay for aceclofenac tablets (IP 2018). The system consisted of a UV-visible detector set at 275 nm, and an autosampler set at 20 μL injections with a 1.5 mL/min flow rate. The output signal of the UV-visible detector was recorded by using data-based lab solution software. The chromatographic separation was carried out using a C18 column (Shimadzu, 4.6 mm i.d, 5.0 μm particle size, 150 mm length). The mobile phase consisted of the isocratic elution of solution (A). The elution of the solvent system was continued up to 1.5 times of the retention time for the standard aceclofenac. To confirm the system suitability, standard solution was injected 5 times consecutively, and then average tailing factor, average number of theoretical plate (NTP), and RSD of the area were calculated. Solution A- A mixture of 55 volumes of buffer solution prepared by adding 1.0 mL of glacial acetic acid in 1000 mL of water and 45 volumes of acetonitrile.
Preparation of standard and sample solution for HPLC.
For the assay, 1 mg/mL of aceclofenac standard stock solution was prepared by dissolving 100 mg of standard in 100 mL HPLC grade acetonitrile, with the help of ultrasonic water bath. The stock solution was subjected for 10 fold dilution in 50 mL volumetric flask by using solvent mixture (55 volumes of acetonitrile and 45 volumes of water). Similarly, to prepare the sample solution, 20 tablets from each batch were crushed into very fine powder in a dried mortar and pestle. Drug powder equivalent to 100 mg of active material (around 250 g drug powders) was weighed and transferred into 100 mL of volumetric flask. Around 60 mL of acetonitrile was poured and all samples were subjected to sonication for 30 min, volume was diluted up to 100 mL. After the filtration, the sample solution was again diluted 10 fold same as the standard solution. Finally, both sample and standard solutions were filtered by using 0.22 μm filters (PTFE filters, Thermo Scientific, Waltham, MA, USA) for the injection. The assay of each batch was determined by Eq.
Mucoadhesion test
Porcine buccal mucosa was used as a model mucosal surface for bioadhesion test. Immediately after slaughter, the buccal mucosa was removed from the pig and transported to the laboratory in tyrode solution and kept at room temperature. Mucoadhesive forces of the tablets (n ¼ 3) were determined utilizing modified balance using strips of the porcine buccal mucosa washed with tyrode solution. The mucoadhesive forces of the tablets were determined by the modified pan balance. The porcine buccal mucosa was cut into the appropriate size pieces and washed with tyrode solution. During the test, a section of buccal mucosa (c) was fitted on the upper glass vial (b) using a rubber band. The exposed mucosa had a diameter of 1 cm. The vial with buccal mucosa (b) was stored in the tyrode solution for 10 min at room 37 degree Celcius. Then, the vial with buccal mucosa (b) and another vial (e) were fixed on adjusted height which was equal to the thickness of the tablet. To the lower vial, the tablet was placed with the help of bilayered adhesive tape. The position of both vials was adjusted so that the adhesive tape and the buccal mucosa get attached. A constant force was applied to the upper vial to get the tablets attached to buccal mucosa uniformly for 2 min, and then the upper vial was connected to the balance. Then the weight on the right pan was slowly increased by 0.5 g until two vials get detached from each other. The total weight (g), to detach was recorded as the measure of mucoadhesive strength.
Swelling test
From each batch, three tablets were individually weighed (W1) and placed separately in petri dishes with 5 mL phosphate buffer of pH 6.8. At the time interval of 1, 2, 4, and 8 h, they were taken out from the petri dish and excess water was removed by using filter paper. The swollen tablets were reweighed (W2) and the percentage of hydration was calculated for each tablet, using the Eq.

In vitro dissolution studies
In vitro dissolution was conducted by using the method, specified in the Indian Pharmacopoeia 2018. The rotating paddle method was used to study drug release from the tablets. Six tablets (n ¼ 6) were taken for the dissolution study. The dissolution medium consisted of 900 mL of phosphate buffer of pH 7.4. The test was performed at 37 C, 0.5 C at a rate of 50 rpm. Total 5 mL samples were withdrawn at every hour and the same volume was replaced with a fresh medium. Samples withdrawn were diluted to 50 mL with the buffer. The samples were filtered and analyzed by using an ultraviolet spectrophotometer at 273 nm. The percentage of drug release was calculated using the calibration curve of the standard drug. For the calibration curve, the stock solution of aceclofenac was prepared in phosphate buffer pH 7.4, at a concentration of 32 mg/mL. The stock solution was diluted to prepare the solution of different concentrations from 0.25 μg/mL to 13 μg/mL and the absorbance was measured using a UV spectrophotometer at a wavelength of 273 nm.
Compatibility study
For the drug excipient compatibility study, infrared (IR) spectroscopy was conducted using a FTIR spectrophotometer and the spectrum was recorded in the wavelength region of 1950 to 400 cm1. The procedure consisted of dispersing a sample (drug alone or mixture of drug and excipients) in potassium bromide and compressed into discs by applying a pressure of 5 tons for 5 min in a hydraulic press. The pellet was placed in the light path and the spectrum was obtained.
Surface pH studies
The pHs of three tablets (n ¼ 3) from each batch were determined. The tablets were placed in distilled water maintained at pH 6.8 and allowed to swell up to 2 h. The surface pH of the tablet was determined by using a pH meter electrode.
Determination of release kinetics
Dissolution data obtained were fitted to zero-order, first-order, Higuchi, Hixson Crowell, and Korsmeyer-Peppas equations to understand the rate and mechanism of aceclofenac release from the prepared batches. The zero-order release rate describes the system where the drug release rate is independent of its concentration. The first-order release rate describes the release from the system as concentration-dependent, which shows log cumulative percent drug remaining versus time. Higuchi's model describes the release of the drug from an insoluble matrix as a square root of a time-dependent process based on Fickian diffusion. Higuchi's root kinetics shows the cumulative percentage drug release versus the square root of time. Hixson Crowell model describes the drug release from the system where there is a change in surface area and diameter of particles or tablets. R2 is a statistical measure of how close the data are to the fitted regression line. The value close to 1 was considered as the most preferred one.
Statistical analysis
Values were expressed as mean SD. Post Hoc Tukey test followed by one way-ANOVA was used for statistical analysis of mucoadhesive strength of different batches. P-value less than 0.05 (p?0.05) was considered to be statistically significant. For kinetic studies Kinet DS 3.0 software was used.[40]
RESULT
Mucoadhesive tablets have been shown to Provide prolonged release of the active ingredient leading to improved bioavailability and therapeutic efficacy. The tablets mucoadhesive properties allow them to target the site of the ulcer reducing systemic side effects and improving Patient campliance. A study published in Heliyon found that mucoadhesive buccal tablets of aceclofenac showed promising results, with a maximum release of 109.41% and a minimum release of 44.82% ¹. Another study focused on bilayer mucoadhesive buccal films for treating mucosal ulcers, which could also be relevant for peptic ulcer treatment.These findings suggest that mucoadhesive tablets can be effectively formulated for treating peptic ulcers, with carbopol-934P being a promising mucoadhesive polymer.
CONCLUSION
Peptic ulcer illness is still a common clinical concern in our society, affecting people of all ages. Peptic ulcer disease is predicted to continue to have a large global influence on health-care delivery, health economics, and patient quality of life as the prevalence of the illness rises with age. Peptic ulcer illness continues to be a problem in medical visits. The majority of people who present with dyspepsia should be examined for peptic ulcer disease. Gastric acid secretion must be understood in order to determine which portion of the stomach is most impacted by the etiologic agent of peptic ulcer disease. H. pylori has remained a risk factor for the development of peptic ulcer disease until now. This bacteria's predilection location determines its clinical prognosis. Understanding the pathophysiology of peptic ulcers can help doctors be more aware of potential complications, such as stomach cancer. The phenomenon of mucoadhesion can be used as a model for the controlled drug delivery approaches for a number of drug candidates. The various advantages of the oral mucoadhesive drug delivery systems like prolongation of the residence time of the drug which in turn increases the absorption of the drug are important factors in the oral bioavailability of many drugs. The factors which are determinant in the overall success of the mucoadhesive drug delivery are the polymer physicochemical properties and the in-vivo factors such as the mucin turnover rate, mucin flow.
REFERENCES


Poonam Ganphade*, Dr. G. R. Dixit, Irshad Ahmad, A Systematic Review: Oral Mucoadhesive Drug Delivery for Peptic Ulcer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 3172-3187 https://doi.org/10.5281/zenodo.15110772
 10.5281/zenodo.15110772
10.5281/zenodo.15110772