Medication Adherence is a critical component in the effective management of chronic disease such as Asthma, Coronary Obstructive Pulmonary Disease(COPD), Hypertension, Diabetes, and cardio vascular disorder such as Heart Attack, Strokes, Heart failure, Arrhythmias, Coronary Artery Disease(CAD), Cerebrovascular Disease, Peripheral Artery Disease(PAD), Rheumatic Heart Disease. Poor adherence to disease progression, complication, increased hospitalizations can lead, and higher healthcare costs .This review discusses the importance of medication adherence, the factors influencing it, and its impact on chronic disease outcomes. It also highlights strategies to improve adherence, including patient education, reminder systems, simplified drug regimens, and healthcare provider interventions.
Chronic diseases are among the leading causes of morbidity and mortality worldwide. Effective management of these conditions often requires long-term pharmacotherapy. Medication adherence—defined as the extent to which patients take their medications as prescribed—is vital for achieving optimal therapeutic outcomes. non-adherence to medication regimens remains a major public health concern. The World Health Organization (WHO) estimates that in developed countries, adherence among patients with chronic diseases averages only 50%, and is even lower in developing countries (WHO, 2003). This review aims to explore the relationship between medication adherence and chronic disease outcomes and to evaluate methods for improving adherence.
2. Understanding Medication Adherence
2.1 Definition and Types
Medication adherence refers to the extent to which a patient takes their medications correctly as prescribed by their healthcare provider. According to the WHO, medication adherence includes three components: initiation, implementation, and discontinuation. Non-adherence can be:
Types of medication adherence-Medication adherence can be categorized into three main types:
1. Primary Adherence:
Definition: When a patient fills and initiates a new prescription.
Non-adherence example: The patient never starts the prescribed medication.
Definition: The degree to which a patient follows the prescribed regimen after starting the medication.
Non-adherence example: Skipping doses, taking incorrect doses, or stopping early.
3. Persistence:
Definition: The duration of time a patient continues the treatment from initiation to discontinuation.
Non-adherence example: Stopping the medication prematurely without medical advice.
Other Related Types (Behavioral View):
Intentional Non-Adherence: The patient knowingly chooses not to follow the treatment (e.g., due to side effects, cost, or personal beliefs).
Unintentional Non-Adherence: The patient wants to follow the treatment but fails due to forgetfulness, misunderstanding, or complexity of the regimen.
2.2 Factors Influencing Non- Adherence
The factors can be related to patient, the disease, the doctor, the prescription and the pharmacist.
A. Patient related Factors:
Patient Age, Sex, Education, etc.: Generally, younger patients and elderly show poor adherence. Women tend to be more adherent than men.
Education: Illiteracy as opposed to educated people show poor adherence. Awareness regarding health, health problems, importance of health all play important role in matters of adherence.
Cultural Attitudes: Ignorance about importance of modern medicine, cultural, misbeliefs, preference for traditional remedies leads to poor adherence.
Economic Factors: Cost of medicines and affordability influence the purchase of medicines. Medicines are taken less frequently than prescribed or prematurely discontinued because of cost. This results into non-adherence.
B. Disease related Factors:
Worse Prognosis: Disease states with a known worse prognosis such as; cancer or rheumatoid arthritis elicits better adherence rates.
Specific Disease States: Hypertensive patients are asymptomatic i.e. they do not experience symptoms prior to initiating the therapy. Convincing them the importance of therapy is a difficult task and when are not convinced tend to non-adhere the therapy. Similarly, in epileptic patients, seizures occur at long intervals and only on occurrence of seizure the importance of therapy is realized.
C. Doctor related Factors:
Too many Drugs Prescribed: Thoughtlessly prescribing too many drugs (multidrug therapy) leads to a greater risk of non-adherence. Similarity in appearance (e.g. size, shape, colour) of prescribed drugs may lead to confusion of the patient and thus to the non-adherence.
Poor Interaction with Patient: The instructions regarding why, how and when to take medicines should be given to patients using effective communication skills. Effective interaction with patients largely results into adherence. Sometimes, patients do not follow the instructions or there may be wrong interpretation of the instructions given by physician, resulting into non-adherence.
Failure in Inspiring Confidence: Doctor’s overall attitude towards patient, failure in establishing good rapport with patient and demonstrating concern about patient all have powerful effect to encourage confidence in patient. Failing to inspire confidence in patients leads to non-adherence.
D. Prescription related Factors:
Illegible and Inaccurate Prescription: Illegible prescription may lead to conclusion that doctors concern to patient is questionable. Prescribing high dose leading to toxicity. Bad prescribing ultimately resulting into dispensing error, all these things lead to poor adherence
Failure to Refill Prescription: For different reasons, patients avoid or neglect the refilling of prescription especially in cases of chronic diseases.
Polypharmacy: Sometimes the prescription may be too complex due to multiple drug therapy prescribed. It has been shown that the greater the number of medications, the poorer the adherence. Multiple doses also decrease adherence if more than two doses per day are prescribed.
2.3 Measurement of Adherence
Common methods include:
Direct Methods: blood or urine drug level testing.
3. Impact of Medication Adherence on Chronic Diseases
3.1 Hypertension
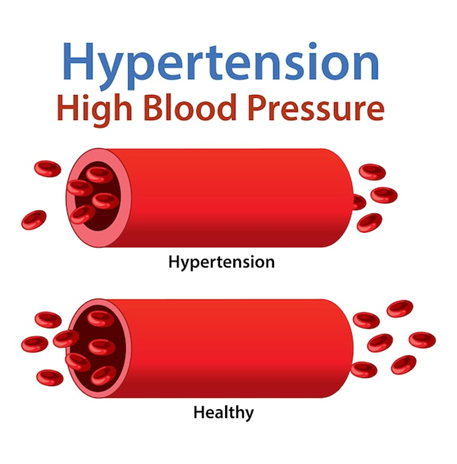
Hypertension, is also known as high blood pressure, is a condition where force of blood against the walls of the arteries is consistently high. Figure.1
Causes:
Kidney disease.
Thyroid problem.
Developes gradually over time.
Symptoms:
Headache.
Dizziness
Chest pain
Blurred vision
Figure.1
Non-adherence is a major cause of uncontrolled blood pressure. Studies show that adherence improves blood pressure control and reduces the risk of stroke and heart failure (Burnier & Egan, 2019).
3.2 Diabetes Mellitus
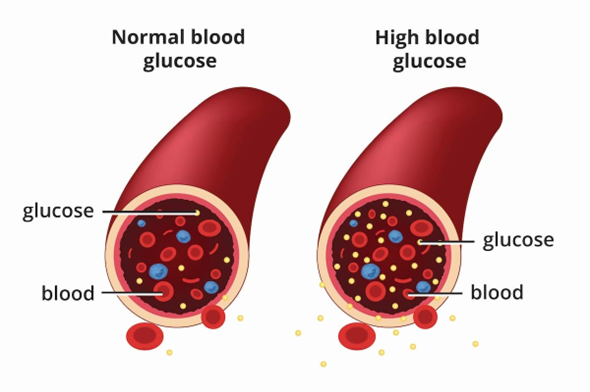
Diabetes mellitus is a chronic (long-term) medical condition that occurs when the body either: Does not produce enough insulin, orCannot effectively use the insulin it produces.
Figure.2
Causes :
Type 1 Diabetes Causes:
Autoimmune destruction of insulin-producing beta cells in the pancreas.
Genetic predisposition.
Possible viral infections triggering immune response.
Type 2 Diabetes Causes:
Obesity or being overweight.
Physical inactivity.
Unhealthy diet (high in sugar and fat).
Family history of diabetes.
Symptoms :
Frequent urination (polyuria)
Excessive thirst (polydipsia)
Extreme hunger (polyphagia)
Unexplained weight loss
Fatigue or tiredness
Blurred vision
Slow-healing wounds
In type 2 diabetes, poor adherence is linked to inadequate glycemic control and increased risk of complications such as nephropathy, neuropathy, and retinopathy (Polonsky & Henry, 2016).
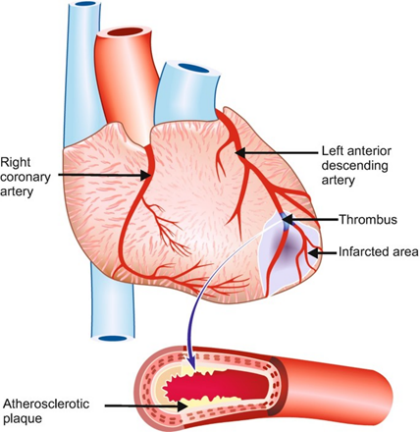
3.3 cardiovascular diseases
Cardiovascular disease (CVD) refers to a group of disorders that affect the heart and blood vessels. It includes conditions like:
Coronary artery disease (CAD) – narrowed or blocked heart arteries
Heart attack (myocardial infarction)
Stroke – blockage or rupture of blood vessels in the brain
Figure.3
Causes:
High blood pressure (hypertension)
High cholesterol levels
Smoking
Diabetes
Obesity or overweight
Physical inactivity
Symptoms:
Chest pain
Shortness of breath
Fatigue
Irregular heartbeat
Adherence to statins and antiplatelets significantly lowers the risk of myocardial infarction and mortality. A meta-analysis by Chowdhury et al. (2013) revealed that good adherence reduces cardiovascular events by 20–25%.
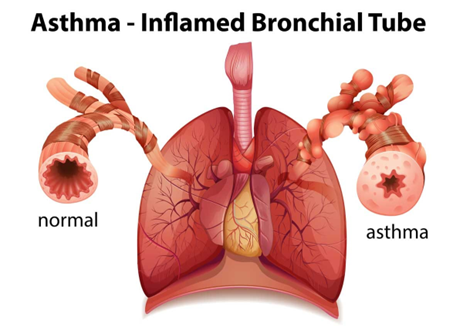
3.4 Asthma and COPD
Asthma is a chronic inflammatory disease of the airways that causes them to become narrow, swollen, and produce extra mucus. This leads to difficulty in breathing, especially during attacks or triggers.
Figure.4
Causes :
Allergens (dust, pollen, mold, pet dander)
Air pollution or smoke
Cold air
Exercise (especially in cold air)
Respiratory infections
Strong emotions or stress
Symtoms:
Shortness of breath
Wheezing (whistling sound while breathing)
Coughing (especially at night or early morning)
Chest tightness
Trouble sleeping due to breathing issues
Adherence to inhaled corticosteroids reduces hospital visits, improves quality of life, and prevents exacerbations (Williams et al., 2011).
Tailored education improves understanding of the disease and therapy, empowering patients to take an active role.
5.2 Simplified Regimens
Once-daily dosing or fixed-dose combinations reduce the pill burden and improve adherence.
5.3 Reminder Systems
Electronic reminders, mobile apps, and pillboxes help combat forgetfulness.
5.4 Healthcare Provider Involvement
Counseling, follow-up visits, and motivational interviewing enhance trust and commitment.
6. Challenges and Future Directions
Despite known strategies, maintaining long-term adherence remains challenging. Future efforts should include:
Development of digital health tools.
Personalized adherence interventions.
Integration of pharmacists in chronic care teams.
More real-world adherence data in low-income settings.
CONCLUSION
Medication adherence plays a pivotal role in the effective management of chronic diseases. Improving adherence not only enhances patient outcomes but also reduces healthcare costs and burden. A collaborative approach involving patients, providers, and the healthcare system is essential for sustaining long-term adherence.
REFERENCES
World Health Organization (2003). Adherence to long-term therapies: Evidence for action. Geneva: WHO.https://apps.who.int/iris/handle/10665/42682
Burnier, M., & Egan, B. M. (2019). Adherence in hypertension. Circulation Research, 124(7), 1124–1140. https://doi.org/10.1161/CIRCRESAHA.118.313220
Polonsky, W. H., & Henry, R. R. (2016). Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Preference and Adherence, 10, 1299–1307. https://doi.org/10.2147/PPA.S106821
Chowdhury, R., Khan, H., Heydon, E., et al. (2013). Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical consequences. European Heart Journal, 34(38), 2940–2948. https://doi.org/10.1093/eurheartj/eht295
Williams, L. K., Pladevall, M., Xi, H., et al. (2011). Relationship between adherence to inhaled corticosteroids and poor outcomes among adults with asthma. Journal of Allergy and Clinical Immunology, 127(6), 1481–1488. https://doi.org/10.1016/j.jaci.2011.01.
Reference
World Health Organization (2003). Adherence to long-term therapies: Evidence for action. Geneva: WHO.https://apps.who.int/iris/handle/10665/42682
Burnier, M., & Egan, B. M. (2019). Adherence in hypertension. Circulation Research, 124(7), 1124–1140. https://doi.org/10.1161/CIRCRESAHA.118.313220
Polonsky, W. H., & Henry, R. R. (2016). Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Preference and Adherence, 10, 1299–1307. https://doi.org/10.2147/PPA.S106821
Chowdhury, R., Khan, H., Heydon, E., et al. (2013). Adherence to cardiovascular therapy: a meta-analysis of prevalence and clinical consequences. European Heart Journal, 34(38), 2940–2948. https://doi.org/10.1093/eurheartj/eht295
Williams, L. K., Pladevall, M., Xi, H., et al. (2011). Relationship between adherence to inhaled corticosteroids and poor outcomes among adults with asthma. Journal of Allergy and Clinical Immunology, 127(6), 1481–1488. https://doi.org/10.1016/j.jaci.2011.01.
Rutuja Shinde
Corresponding author
Sinhgad Institute of Pharmaceutical Sciences, Kuagaon, Lonavla
Rutuja Shinde, Review on Medication Adherence and Its Effect on Chronic Disease, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 254-259. https://doi.org/10.5281/zenodo.17040762


 10.5281/zenodo.17040762
10.5281/zenodo.17040762