1 Department of General Medicine, Government Hospital, Vijayawada, Andhra Pradesh.
2 Department of Pharmacy Practice, NOVA College of pharmacy, Jupudi, Vijayawada, Andhra Pradesh.
Dextrocardia with situs solitus is a rare congenital anomaly where the heart is located in the right hemithorax, while thoracoabdominal viscera remain in normal orientation. Differentiating between true dextrocardia and acquired cardiac displacement is crucial, especially when coexisting thoracic pathology is present. We report a case of a 64-year-old male with a history of pulmonary tuberculosis presenting with acute chest pain. He was initially treated as a case of ST-elevation myocardial infarction (STEMI). However, further evaluation revealed normal coronary arteries, a destroyed right lung, and mediastinal shift consistent with acquired dextroposition rather than congenital dextrocardia. Imaging showed right ventricular dysfunction and preserved left ventricular function. The patient was managed conservatively with antiplatelets, anticoagulants, antibiotics, and antihypertensives, with complete resolution of symptoms.This case highlights the importance of recognizing anatomical variants, such as dextrocardia or acquired dextroposition, particularly in patients with a history of pulmonary pathology. Thorough imaging and a multidisciplinary approach are crucial for accurate diagnosis and effective management of cardiopulmonary complaints in such complex presentations.
Dextrocardia with situs solitus is a rare congenital condition and is often associated with structural heart anomalies[1]. However, acquired displacement of the heart to the right side, referred to as dextroposition, can occur secondary to conditions like unilateral lung destruction. Post-tuberculous sequelae, particularly involving massive cavitary lesions, can cause mediastinal shift and cardiac displacement.[2] Differentiating between true congenital dextrocardia and acquired dextroposition is vital for accurate diagnosis and management of cardiopulmonary presentations. Management of dextrocardia with situs solitus primarily depends on whether the condition is isolated or associated with structural cardiac anomalies.[3] In cases where dextrocardia is isolated and asymptomatic, no specific treatment is required other than periodic monitoring and patient reassurance.[4] However, when associated with congenital heart defects such as atrial or ventricular septal defects, transposition of great arteries, or pulmonary stenosis, management becomes more complex and typically requires surgical intervention tailored to the underlying anomaly[5]. Diagnostic imaging, such as echocardiography with segmental analysis, chest X-ray, and cardiac MRI or CT, is essential for precise anatomical delineation[6]. Electrocardiogram interpretation may be challenging due to the altered cardiac axis, often necessitating the use of right-sided precordial leads.[7] Preoperative planning and interventional procedures must consider the reversed anatomy, and a multidisciplinary approach involving cardiology, cardiothoracic surgery, and anesthesiology is crucial for optimal outcomes.[8]
CASE PRESENTATION:
A64-year-old male presented to the outpatient department with complaints of moderate to severe chest pain radiating to the upper back, persisting for the past two days. He had initially sought care at a local hospital, where an electrocardiogram (ECG)revealed ST-segment elevation consistent with an acute anterior wall myocardial infarction (ASWMI). He was managed with intravenous Tenecteplase for thrombolysis and received full loading doses of Aspirin 350 mg, Clopidogrel 300 mg, and Atorvastatin 80 mg. A diagnosis of acute coronary syndrome (ACS) with left ventricular dysfunction was made, and he was referred to our center for further evaluation and management.His medical history was notable for hypertension, managed with Telmisartan 40 mg and Hydrochlorothiazide 12.5 mg, and a psychiatric illness (unspecified), for which he had been receiving Clomipramine hydrochloride 25 mg for the past two years. He also reported a previous history of pulmonary tuberculosis (PTB), for which he had completed antitubercular therapy (ATT). Post-treatment, he developed a large residual cavity in the right lung, leading to destruction of the right lung and a mild mediastinal shift towards the right. On further evaluation at our facility,2D echocardiography revealed a left ventricular ejection fraction (EF) of 46%, with evidence of right ventricular dysfunction.
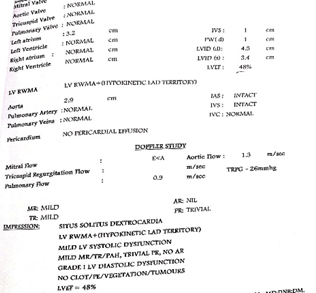
Fig 01: 2d Echo findings
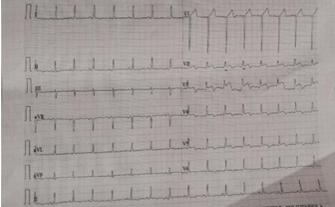
Fig 02: ECG Findings
Coronary angiography demonstrated essentially normal coronary arteries. Chest radiographyconfirmed a destroyed right lungwith amild rightward mediastinal shift. ECGcontinued to show persistent ST elevations. Laboratory investigations showed: Hemoglobin: 8.8 g/dL (indicating mild anemia), White blood cell and platelet counts: within normal limits, Serum creatinine: 1.0 mg/dL (normal), Mild elevations in serum sodium and potassium levels.
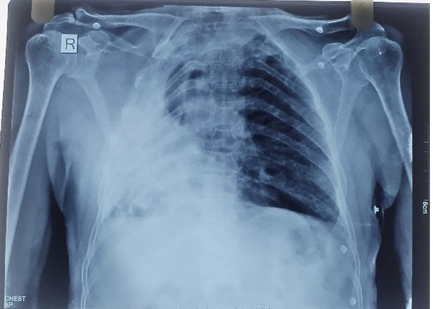
Fig 03: Chest X-Ray
Despite the initial concern for ACS, subsequent evaluation did not reveal any significant obstructive coronary pathology. The chest discomfort was attributed, in part, to underlying anatomical distortion due to post-tubercular structural lung damage and cardiac displacement.The patient was managed conservatively with antiplatelets, anticoagulants (heparin), antibiotics, and antihypertensive medications. He was thoroughly counselled regarding the anatomical findings, the benign nature of the current cardiac evaluation, and the potential impact of his past pulmonary pathology on current symptoms. After two days of observation and supportive care, his chest pain resolved completely, and he was discharged in stable clinical condition.
DISCUSSION
Dextrocardia with situs solitus is a rare and complex congenital cardiac malposition wherein the heart is located on the right side of the thoracic cavity, while the abdominal and thoracic viscera retain their normal left-right orientation. This condition is frequently associated with a broad spectrum of congenital heart anomalies, necessitating a detailed segmental analysis for accurate anatomical classification and clinical decision-making. One of the key challenges in patients with dextrocardia and situs solitus lies in the diagnostic and therapeutic implications for coexisting pathologies, particularly when cardiovascular or thoracic interventions are warranted. The atypical positioning of the heart and great vessels alters the usual anatomical landmarks, often requiring modified imaging techniques and surgical approaches. For example, access to the systemic and pulmonary vasculature, particularly the aortic arch, pulmonary arteries, and the entry points of the venae cava,can be technically demanding and mandates preoperative planning with advanced modalities such as three-dimensional computed tomography or magnetic resonance imaging. The presence of additional thoracic pathology, such as unilateral lung destruction as seen in post-tubercular cavitation, further complicates clinical management. In such cases, mediastinal shift and compensatory volume changes may lead to secondary dextroposition or exacerbate pre-existing dextrocardia, posing diagnostic dilemmas. This altered thoracovascular anatomy can significantly impact the feasibility and safety of procedures such as pacemaker implantation, coronary angiography, or cardiac valve surgery. Management of patients with dextrocardia and concomitant right lung destruction demands a multidisciplinary approach involving cardiologists, pulmonologists, radiologists, and cardiothoracic surgeons. Thorough anatomical assessment, precise imaging interpretation, and individualized surgical planning are essential to minimize procedural risks and optimize outcomes. Comprehensive echocardiographic and cross-sectional imaging play pivotal roles in delineating the anatomical relationships and guiding both medical and surgical management strategies.
CONCLUSION:
It is essential to recognize that atypical anatomical presentations, such as dextrocardia with situs solitus—or acquired dextroposition due to right lung destruction—can significantly complicate the diagnosis and management of acute cardiovascular events. Clinicians must maintain a high index of suspicion and consider anatomical variability when evaluating chest pain, especially in patients with a history of pulmonary tuberculosis or thoracic structural disease. Comprehensive imaging and cardiac evaluation are critical for accurate diagnosis and to avoid unnecessary or inappropriate interventions. Furthermore, patients with known thoracic abnormalities should be educated about their condition, the potential implications for future medical procedures, and the importance of informing healthcare providers during any hospital visit. Early recognition, multidisciplinary coordination, and individualized treatment strategies can improve diagnostic accuracy, enhance patient safety, and optimize clinical outcomes in such complex presentations.
ACKNOWLEDGEMENT
We want to express our sincere gratitude to the Superintendent and the Head of the Department of General Medicine, Government General Hospital, for their valuable support and guidance in the preparation of this case report. We also extend our heartfelt thanks to the patient and their family for providing informed consent and permitting the use of the patient’s clinical information for academic and reporting purposes.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest in the publication of this case report.
ABBREVIATIONS
ACS: Acute Coronary Syndrome, ASWMI: Anterior Segment Wall Myocardial Infarction,PTB: Pulmonary Tuberculosis, EF: Ejection Fraction,ECG: Electrocardiogram, LV: Left Ventricle, RV: Right Ventricle, ATT: Antitubercular Therapy, HTN: Hypertension, CT: Computed Tomography, CXR: Chest X-ray, OP: Outpatient, STEMI: ST-Elevation Myocardial Infarction.
PATIENT CONSENT
The patient described in this case report has provided informed written consent for the publication of the clinical details, investigations, and radiological findings. The patient understands that personal identity will remain confidential and that this report is intended for educational and academic purposes. The patient is satisfied with the care and treatment received.
SUMMARY
Dextrocardia with situs solitus is a rare congenital anomaly characterized by a right-sided cardiac apex with normal left-right orientation of the thoracoabdominal viscera. In this report, we present the case of a 64-year-old male with a prior history of pulmonary tuberculosis who presented with acute-onset chest pain. Initial evaluation suggested an acute ST-elevation myocardial infarction (STEMI), for which standard thrombolytic and antiplatelet therapy was initiated. However, subsequent diagnostic workup—including echocardiography, coronary angiography, and chest radiography—revealed normal coronary anatomy, destruction of the right lung parenchyma, and mediastinal shift, consistent with acquired cardiac dextroposition secondary to post-tuberculous sequelae, rather than true congenital dextrocardia. This unusual anatomical alteration complicated the initial interpretation of clinical and imaging findings, underscoring the diagnostic challenges posed by coexisting structural thoracic abnormalities. The patient was managed conservatively with dual antiplatelet therapy, anticoagulation, antibiotics, and antihypertensives, and demonstrated full clinical recovery.
This case highlights the critical importance of comprehensive anatomical assessment and high-resolution imaging in differentiating congenital anomalies from acquired thoracic displacements. It also emphasizes the need for heightened clinical vigilance and individualized diagnostic pathways when evaluating chest pain in patients with a history of significant pulmonary disease.
REFERENCES

P. Hussain Peera, Shaik. Iqra, Acquired Cardiac Dextroposition Due To Right Lung Destruction: A Diagnostic Mimic of Dextrocardia, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 2449-2453. https://doi.org/10.5281/zenodo.16029423
 10.5281/zenodo.16029423
10.5281/zenodo.16029423
