Department Of Pharmaceutical Chemistry, Shivlingeshwar College of Pharmacy, Almala. Tq. Ausa, Dist. Latur-413520, Maharashtra (MH), India.
The most common metabolic and endocrine condition is diabetes mellitus (DM), which is defined by a complete decrease in insulin production and peripheral resistance. But adipocyte insulin resistance, elevated glucagon secretion, elevated renal glomerular glucose absorption, and neurotransmitter dysfunction are also part of the pathophysiology of diabetes mellitus. Despite a broad range of glycemic control treatments, managing diabetes mellitus is still difficult and complicated since different pathologic factors of the disease have been identified. In order to regulate blood glucose levels, antidiabetic medications are used to treat diabetes mellitus. With a few exceptions, such insulin, exenatide, and pramlintide, the majority of the medications are taken orally. The hallmark of diabetes mellitus (DM) is an absolute to reduce complications and maintain a high quality of life, type 2 diabetes (T2D) therapy requires a multimodal strategy that incorporates behavioral and pharmaceutical therapies. Treatment includes using medication and lifestyle changes to control weight, comorbidities, cardiovascular risk factors, glucose levels, and related problems.
Diabetes is one of the largest worldwide health emergencies of this century and is the third major cause of death in the USA after heart disease and cancer [1]. India being the “Diabetes metropolis” of the planet influences almost every community whether it is metropolitan or agrarian. Diabetes mellitus (DM) is characterized by hyperglycemia resulting from insulin resistance, inadequate insulin secretion, or excessive glucagon secretion. DM is a non-infectious disease caused by the disruption of carbohydrate metabolism, which culminates in persistent hyperglycemia [2]. Despite the fact that thousands of new anti-diabetic medications are created every year, the illness is extremely tough to eradicate. Diabetes is a global non-communicable disease that has a significant impact on mortality and lethality. Diabetes can cause a number of consequences, including cardiovascular disease [3], retinopathy [4], nephropathy [5], neuropathy [6], eating disorders [7], pregnancy issues [8], dental disease, renal disease [9], and more. Additionally, diabetes can impede the healing of wounds [10]. Ketoacidosis, hyperosmolar coma, and weakened resistance to influenza and pneumonia are a few other consequences of diabetes. The main cause of diabetes mellitus is chronic hyperglycemia, which is fuelled by innate insulin resistance and insufficiency and leads to aberrant glucose metabolism. Chronic hyperglycemia combined with insulin insensitivity, or the inability of insulin to dock adipocyte and myocyte receptors to facilitate intracellular downstream processes that determine blood glucose regulation, alters metabolic pathways and triggers the accumulation of glycogen, which can lead to additional complications such as liver disease and cardiac hypertrophy [11]. It is commonly known that the primary cause of insulin resistance in type 2 diabetes is abnormal post-receptor insulin signaling, which in turn affects insulin signaling-related metabolic pathways. Alterations in the downstream pathways of insulin signaling, such as insulin receptor internalization, destabilization of serine/threonine phosphorylation, or insulin receptor tyrosine dephosphorylation, may also result from this [12]. Diabetes mellitus type 1 is an autoimmune condition. It is typified by a reduction in pancreatic β-cells, which hinders the generation of insulin [13]. On the other hand, obesity and a sedentary lifestyle are significant risk factors for type 2 diabetes mellitus (T2DM), a condition in which insensitivity and malfunctioning pancreatic β-cells result in hyperglycemia, or elevated blood glucose levels [13,14].
Table 1: Antidiabetic Drugs [15]
|
Drug Group |
Specific Drug |
Effects |
Adverse Effects |
|
Alpha-Glucosidase inhibitors |
Acarbose |
HbA1c ↓ Body weight ↓ |
Gastrointestinal disorders ↑ Serum transaminases (AST, ALT) ↑ |
|
Biguanides |
Metformin |
HbA1c ↓ Body weight ↓ Cancer ↓ |
Gastrointestinal disorders ↑ Reversible vitamin B12 deficiency↑ |
|
Thiazolidineidiones |
Pioglitazone |
HbA1c ↓ BP ↓ NAFLD↓ MACE ↓ |
Peripheral edema ↑ Anemia ↑ Hospitalization for HF ↑ Bone fracture in women ↑ |
|
Sulfonylureas |
Glimepiride Gliclazide |
HbA1c ↓ |
Body weight ↑ Hypoglycemia ↑ Lack of durable effect |
Five to ten percent of all cases of diabetes are of this type. Since type 1 diabetes is diagnosed in children, adolescents, and young adults, it is also referred to as insulin-dependent diabetes mellitus or youthful-onset. However, in the past ten years, it has been found that it can occur at any age [16]. Because of the body's autoimmune reaction, which involves antibodies destroying beta cells, the pancreatic beta cells in type 1 diabetes are unable to produce insulin.[17, 18] For those with type 1 diabetes, insulin injections or continuous insulin infusions using an insulin pump are crucial to their health.
kind 2 diabetes, sometimes referred to as adult-onset diabetes or non-insulin-dependent diabetes, is the most prevalent kind of the disease, making up 85–90% of all cases. Although younger generations are also affected, those 45 years of age or older are diagnosed with it the most frequently [19]. The β cells of the pancreas produce insulin in type-2 diabetes, but insulin receptors or insulin-responsive cells in the cell membrane do not react to insulin as they should. "Insulin resistant" refers to a receptor's inadequate or nonexistent response, which raises blood glucose levels.
Another form of diabetes that is typically detected in latter stages of pregnancy in pregnant women is called gestational diabetes. Regular exercise and particular diets are two ways to treat gestational diabetes. Sometimes, a few anti-diabetic drugs required to maintain normal blood glucose levels[20]. The risk factors associated with developing gestational diabetes mellitus include a previous diagnosis of gestational diabetes mellitus, overweightness, obesity, etc.[21,22]
Insulin, often known as the main hormone, transfers glucose from the blood to the tissue, regulating blood glucose levels in our bodies. The pancreatic beta cells produce insulin [23], which is then stored in the body in units of six molecules. The active form of insulin is a monomer. Insulin's primary function is to regulate blood glucose levels that are derived from carbohydrates and travel throughout the body, particularly when they reach tissues through insulin receptors or cells that respond to insulin .Type 1 diabetes arises because beta cells are unable to synthesize insulin, whereas type 2 diabetes arises when insulin receptors or cells that respond to insulin are unable to respond to insulin. Insulin and its equivalents are the usual treatment for type 1, gestational diabetes, and some types of type-2 diabetes, according to the UK Prospective Diabetes Study.[24, 25]
Drug Classes for The Treatment of Diabetes
Pioglitazone:
When treating type 2 diabetes, pioglitazone is used either by itself or in conjunction with insulin, metformin, or sulfonylurea to lower blood glucose levels [26]. In a Cochrane systematic review, pioglitazone's effects were compared to those of other blood sugar-lowering medications, such as metformin, acarbose, and repaglinide, as well as with a healthy diet and regular exercise. The results showed no benefit in lowering the risk of type 2 diabetes in individuals who were at risk.[27]
Mechanism of action
The nuclear receptor peroxisome proliferator-activated receptor gamma (PPAR-γ) and, to a lesser extent, PPAR-α are selectively stimulated by pioglitazone. It alters the transcription of the genes that regulate the liver, adipose tissue, and muscle's metabolism of fats and carbohydrates. Consequently, pioglitazone lowers the amount of glucose and glycated hemoglobin in the plasma, lowers gluconeogenesis in the liver, and lowers insulin resistance in the liver and peripheral tissues. [28, 29]
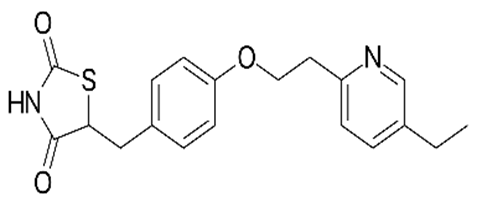
Rosiglitazone:

Rosiglitazone is used along with a diet and exercise program and sometimes with one or more other medications to treat type 2 diabetes (condition in which the body does not use insulin normally and therefore cannot control the amount of sugar in the blood). Rosiglitazone is in a class of medications called thiazolidinediones. It works by increasing the body's sensitivity to insulin, a natural substance that helps control blood sugar levels [30,31]
Pharmacology
Rosiglitazone is a member of the thiazolidinedione class of drugs. Thiazolidinediones act as insulin sensitizers. They reduce glucose, fatty acid, and insulin blood concentrations. They work by binding to the peroxisome proliferator-activated receptors (PPARs). PPARs are transcription factors that reside in the nucleus and become activated by ligands such as thiazolidinediones. Thiazolidinediones enter the cell, bind to the nuclear receptors, and alter the expression of genes. The several PPARs include PPARα, PPARβ/δ, and PPARγ. Thiazolidinediones bind to PPARγ. PPARs are expressed in fat cells, cells of the liver, muscle, heart, and inner wall (endothelium) and smooth muscle of blood vessels. PPARγ is expressed mainly in fat tissue, where it regulates genes involved in fat cell (adipocyte) differentiation, fatty acid uptake and storage, and glucose uptake. It is also found in pancreatic beta cells, vascular endothelium, and macrophages Rosiglitazone is a selective ligand of PPARγ and has no PPARα-binding action. Other drugs bind to PPARα. Rosiglitazone also appears to have an anti-inflammatory effect in addition to its effect on insulin resistance. Nuclear factor kappa-B (NF-κB), a signaling molecule, stimulates the inflammatory pathways. NF-κB inhibitor (IκB) downregulates the inflammatory pathways. When patients take rosiglitazone, NF-κB levels fall and IκB levels increase. [32]
Thiazolidinediones
Thiazolidinediones (TZDs) act as insulin sensitizers which activate peroxisome proliferator-activated receptors (PPARs), a broad family of nuclear receptors. The first TZD drug, troglitazone, was approved by the FDA in 1997; however, it was discontinued in 1999 due to severe hepatotoxicity. Currently, there are two marketed TZDs, rosiglitazone and pioglitazone, which were FDA-approved in 1999. TZD use has previously been limited due to concerns with safety issues and side effects. In addition, there was some controversy over cardiovascular toxicity with rosiglitazone and an increase in bladder cancer with pioglitazone. However, recent studies show no longer significant issues [33] Furthermore, the beneficial effects of TZDs on the cardiovascular risk factors associated with insulin resistance have been well documented. TZD drugs can be effective as a monotherapy or in a combination regimen. One combination regimen that consists of pioglitazone and metformin is currently marketed. Four TZD monotherapies and one combination with a dipeptidyl peptidase-4 (DPP4) inhibitor are in trials in clinical development. The most clinically advanced is lobeglitazone, which has already been approved in South Korea and is currently in phase III trials for additional combination treatments. TZD molecules can interact with PPAR-α and PPAR-γ isoforms expressed primarily on fatty tissues and skeletal muscle. This leads to activating these receptors and stimulating complexation with another essential constituent–the retinoid X receptor. The triple complex can bind specifically to DNA by peroxisome proliferative response elements (PPRE) and act as a target gene promoter, thus stimulating gene expression. This therapeutic method leads to increased adiponectin levels, decreased gluconeogenesis, and increased glucose uptake in the muscle and fat. Adiponectin is a hormone secreted in adipose tissue that regulates glucose concentration by improving insulin sensitivity. [34]
Meglitinides
Two meglitinides have been FDA-approved: nateglinide in 2009 and repaglinide in 2013. Currently, there are no meglitinides in clinical trials. Meglitinides share a similar mechanism of action to sulfonylurea agents in that they increase insulin secretion in the pancreas. They bind to SURs in pancreatic beta cells but at a binding site different than SUs and induce the same reaction cascade that leads to insulin secretion.[35] In contrast to SUs, meglitinides, exhibit glucose-sensitive action whereby their potency increases at higher glucose concentrations. Meglitinides are short acting and associated with lower hypoglycemia risks, weight gain, and chronic hyperinsulinemia than sulfonylurea drugs. Other studies have since demonstrated that meglitinides could be associated with increased risk of hypoglycemia in diabetic patients with advanced chronic kidney disease. [36]
Biguanides
The approval of the biguanide metformin in 1995 significantly changed T2DM therapy and is the only FDA-approved antihyperglycemic agent in this drug class. Metformin selectively inhibits the mitochondrial isoform of glycerophosphate dehydrogenase, indirectly activates adenosine monophosphate-activated protein kinase (AMPK), and reduces cytosolic dihydroxyacetone phosphate while raising cytosolic NADH/NAD ratio. This results in decreased plasma glucose and lactate levels, reduced liver gluconeogenesis, hepatic glucose secretion, and endogenous glucose production. Moreover, metformin can increase insulin sensitivity in muscle tissues. Currently, metformin is the only antihyperglycemic drug recommended by the American Diabetes Association and the European Association for the Study of Diabetes as initial oral therapy for patients with T2DM. [37]
REFERENCES




Mahesh Bhakare*, Syed A. A., Dinesh Gujrathi, Vaishnavi Siral, Sonal Doltade, Antidiabetic Medications: An Oral Treatment Approach for Regulating Blood Glucose Levels, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 1600-1606 https://doi.org/10.5281/zenodo.15205150
 10.5281/zenodo.15205150
10.5281/zenodo.15205150
