
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1Assistant Professor, Sat Kaival College of Pharmacy, Sarsa, Anand, Gujarat-388365.
2,3,4 UG Scholar, Neotech Institute of Pharmacy, Virod, Vadodara- 390022.
Anti-inflammatory drugs are used widely to reduce inflammation that is involved in various diseases such as Alzheimer, Parkinson, rheumatoid arthritis, asthma, infectious diseases including COVID-19 infections, etc. These drugs are used for acute as well as for chronic conditions. The well-known anti-inflammatory drugs that are available in the market are nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, naproxen, diclofenac, celecoxib, etc. The steroids are also used as anti-inflammatory agents especially in chronic and severe inflammation; however, long-term use of steroids is associated with various adverse drug reactions (ADRs). Thus, there is a need of more safe and efficacious anti-inflammatory drugs in the treatment of various diseases. Many anti-inflammatory drugs are under experimental investigation and some of them are in different phases of clinical trials. This chapter summarizes the information related to ongoing and completed clinical trials of anti-inflammatory drugs in various diseases along with their future perspectives.
Inflammation is a normal, protective response to tissue injury caused by physical trauma, noxious chemicals or microbiological agents. There are mainly two types of inflammation which are as follows Acute inflammation It is associated with increased vascular permeability, capillary infiltration and emigration of leukocytes. Chronic inflammation It is associated with infiltration of mononuclear immune cells, macrophages, monocytes, neutrophils, fibroblast activation, proliferation (angiogenesis) and fibrosis. Inflammation is a common clinical conditions and rheumatoid arthiritis (RA) is a chronic debilitating autoimmune disorder1 , that affects about 1% of the population in developed countries.The classic signs of inflammation are local redness, swelling, pain, heat and loss of function(1). Nitric oxide (NO) is a gaseous short lived free radical has been implicated as a mediator of inflammation and modulation of biosynthesis or activity of NO results in amelioration of acute inflammation and experimental arthiritis model. NO is generated via the oxidation of the terminal guanidine nitrogen atom of L-arginine by the enzyme Nitric Oxide Synthase (NOS). Three major isoforms of Nitric Oxide Synthase (NOS) have been identified. Two expressed constitutively, are calcium/calmodul independent and are classified together as constitutive NOS isoforms (cNOS). The third is cytokine-inducible, calcium/calmodulin independent isoform of NOS (iNOS) is regulated in the gene by a variety of inflammatory mediators(2). Increased NOS activity or NO release have been demonstrated in both acute and chronic models of inflammation. Further, administration of Larginine a precursor for NO synthesis increased the paw swelling in adjuvant arthiritis. NSAIDS are among the most commonly used drugs worldwide. They are prescribed for orthopaedic conditions such as osteoarthritis, soft-tissue injuries and fractures etc. NSAIDS e.g Ibuprofen and naproxen etc. are used in the above said conditions. The other class of drugs is glucocorticoids e.g cortisone and prednisone etc(3). However, besides their high costs, severe adverse reactions and toxicity, including some risk of infections in subsets of patients being treated with biological response modifiers e.g Tumour necrosis factor, alpha blocking agents. The side-effects with currently used drugs are G.I ulceration and bleeding, Renal damage, Hypertension, Hyperglycemia. Besides the above side-effects, the greatest disadvantage in presently available potent aynthetic drugs lies in their toxicity and reappearance of symptoms after discontinuation. Therefore, the screening and development of drugs for their anti-inflammatory activity is the need of hour and there are many efforts for finding anti-inflammatory drugs from indigenous medicinal plants. Plants as natural anti-inflammatory agents Unlike modern allopathic drugs which are single active components that target one specific pathway, herbal medicines work in a way that depends on an orchestral approach(4). A plant contains a multitude of different molecules that act synergistically on targeted elements of the complex cellular pathway. Medicinal plants have been source of wide variety of biologically active compounds for many centuries and used extensively as crude material or as pure compounds for treating various disease conditions. The use of herbal medicines becoming popular due to toxicity and side-effects of allopathic medicines. Medicinal plants play an important role in the development of potent therapeutic agents. There are over 1.5 million practitioners of traditional medicinal system using medicinal plants in preventive, promotional and curative applications. India with its biggest repository of medicinal plants in the world may maintain an important position in the production of raw materials either directly for crude drugs or as the bioactive compounds in the formulation of pharmaceuticals and cosmetics etc(5). Inflammation: Inflammation is a key aspect of the body’s immune defenses. It can be acute or chronic. Symptoms can include swelling, heat, pain, and more. Treatments can depend on the underlying cause.
Anti-inflammation: A drug or substance that reduces inflammation (redness, swelling, and pain) in the body. Anti-inflammatory agents block certain substances in the body that cause inflammation. They are used to treat many different conditions. Some anti-inflammatory agents are being studied in the prevention and treatment of cancer.
There are mainly two types of inflammation:
Classification Of NSAIDS (8, 9)
Table 1 Classification Of NSAIDS
|
Salicylate
|
Indoleacetic Acid Derivatives |
Aryl Acetic Derivatives |
Enolic Acids
|
|
|
Acetylsalicyclic aicd Lysine clonixinate Benorilate Diflunisal Salicylamide Etersalate Salsalate or salicyclic acid |
Acemethacin Glucamethacin Indomethacin Proglumethacin Oxamethacin Sulindac Difenpiramide |
Aceclofenac Diclofenac Etodolac Fentiazac Ketorolac Bufexamac Lonazolac Alclofenac Zomepirac |
Oxicans Droxicam Meloxicam Piroxicam Tenoxicam Oxaprozin Lornoxicam |
Pyrazolones Phenylbutazone Mofebutazone Oxyphenbutazone Kebuzone Metamizole(Dipyrone) Feprazone Nifenazone Suxibuzone Aminophenazone |
|
Arylpropionic Derivatives |
Phenemates |
Others |
||
|
Butibufen Phenoprofen Phenobufen Flurbiprofen Benoxaprofen Suprofen Ibuprofen Ibuproxam |
Ketoprofen Dexetoprofen Pyprophene Indoprofen Naproxen Oxaprozin Tiaprofen Phenoprofen |
Meclofenamic acid Mefenamic acid Flufenamic acid Tolipanic acid Niflumic acid Etofenamate |
Nabumetone Glucosamine Diacerhein Nimesulide Proquazone Azapropazone Benzidamine Orgotein Feprazone Morniflumato |
Coxibs: Celecoxib Rofecoxib Parecoxib Valdecoxib Etoricoxib 4-Aminophenol Paracetamol (Acetaminophen) |
Plants As Anti-inflammatory Agents(10, 11)
Table 2 Plants as Anti-inflammatory Agents
|
Sr. no. |
Plant Name |
Family |
Plant Part |
Type of Extract |
|
1 |
Achillea millefolium |
Asteraceae |
Whole Plant |
Aqueous, alcohol |
|
2 |
Aconitum heterophyllum |
Valeraneaceae |
Root |
Ethanol |
|
3 |
Aloe vera |
Asphodelaceae |
Leaves |
Pet.ether, Ethanol |
|
4. |
Boswellia serrata |
Burseraceae |
Resin |
Methanol |
|
5. |
Bursera simaruba |
Burseraceae |
Leaves,Bark |
Hexane,Ethanol |
|
6. |
Cassia fistula |
Caesalpiniaceae |
Leaves |
Methanol |
|
7 |
Citrus auranticum |
Rutaceae |
Fruit |
Not indicated |
|
8 |
Daphne pontica |
Thymelaeaceae |
Aerial Parts, Roots |
Methanol |
|
9 |
Elephantophs scaber |
Compositae |
Leaves |
Pet.ether |
|
10 |
Emblica officinalis |
Euphorbiaceae |
Fruit |
Ethanol |
|
11 |
Garcinia mangostana |
Guttiferae |
Fruit |
Methanol |
|
12 |
Hammada elegans |
Chenopodiaceae |
Aerial part |
Ethanol |
|
13 |
Iberis amara |
Brassicaceae |
Whole plant |
Ethanol |
|
14 |
Kirkia acuminata |
Simaroubaceae |
Leaves |
Methanol |
|
15 |
Lippia geminata |
Verbenaceae |
Leaves |
Pet.ether, Ethanol |
|
16 |
Mangifera indica |
Anacardiaceae |
Bark |
Aqueous |
|
17 |
Moringa olifera |
Moringaceae |
Root, Flowers |
Methanol, Aqueous |
|
18 |
Paederia foetida |
Rubiaceae |
Leaves |
Methanol |
|
19 |
Phyllanthus polyphyllus |
Euphorbiaceae |
Whole plant |
Ethanol |
|
20 |
Ricinus communis |
Euphorbiaceae |
Roots, leaves |
Methanol, pet ether |
|
21 |
Rubrus ellipticus |
Rubiaceae |
Leaves |
Ethanol |
|
22 |
Saussurea costus |
Asteraceae |
Whole plant |
Methanol |
|
23 |
Sesbania sesban |
Leguminosae |
Leaves and Bark |
Methanol |
|
24 |
Sidium guajava |
Myrtaceae |
Fruit |
Methanol |
|
25 |
T. buxifolium |
Rosaceae |
Leaves, Stem |
Methanol |
|
26 |
Tinospora diversifolia |
Menispermeaceae |
Aerial part |
Aqueous |
|
27 |
Vinca rosea |
Apocynaceae |
Leaves |
Not indicated |
|
28 |
Vitex negundo |
Lamiaceae |
Leaves |
Alcoholic |
|
29 |
Xeromphis spina |
Compositae |
Pulp |
Ethanol |
|
30 |
Zingiber officinalae |
Zingiberaceae |
Rhizome |
Ethanol |
The World Health Organization (WHO) estimates that approximately 65% of the world’s population incorporates traditional medicine (ethnobotanical uses) into medical care. Ethnobotanical studies over the years have allowed the association of highly diversified plants with biological activities, from observation, description, and experimental research, which has greatly contributed to the discovery of natural products with biological action. The use of medicinal plant-based natural compounds to treat many illnesses has become a great trend in clinical research. Polyphenolic compounds have drawn significant attention due to their modulation effects on inflammasomes. These multi-protein complexes are associated with the initiation and progression of metabolic disorders and chronic diseases, such as cancer and neurodegenerative diseases. Thus, plants have become the first source of substances for the development of new drugs, and a considerable part of the drugs prescribed in the world are derived from them(12). Plants contain reservoirs of potential secondary metabolites that are the major sources of drugs, which intensifies the interest of transnational industries in the search for substances obtained from plant sources, particularly since the great majority of species have not been studied chemically or biologically. The use of plants or plant products for medicinal purposes is mostly documented in books and, lately, on an enormous number of websites (the reliability of some of which must be examined carefully). In recent decades, hundreds of research and review articles have been published regarding the anti-inflammatory activities of plants. Other plant species with anti-inflammatory properties have already been described in the literature. However, the parts of the plants used and the compounds responsible for the anti-inflammatory activity have not yet been fully elucidated(13).
Phytoconstituents With Anti Inflammatory Activity
Phytochemical studies carried out with the species Myracroduo nurundeuva Allemão, Schinus terebinthifolius Raddi, Spondias mombin L., Spondias purpurea L. and Spondias tuberosa Arruda, belonging to the Anacardiaceae family, detected the presence of several secondary metabolites. The most abundant are phenols, triterpenes, flavonoids, and cinnamic acid, which are responsible for their anti-inflammatory action. The plants that make up the Euphorbiaceae family, such as the species Euphorbiaceae acalypha hispida Burm. f., Acalypha indica L., Phyllanthus niruri L., are rich mainly in phenolic compounds, saponins, tannins, and triterpenes, which are responsible for their anti-inflammatory action. Research with the species Ruellia asperula (Mart. Ex Ness) Lindau (family Acanthaceae), Achyranthes aspera L., Alternanthera brasiliana (L.) Kuntze (family Amaranthaceae), Himatanthus drasticus (Mart.) Plumel (family Apocynaceae), Matricaria chamomilla L. (family Asteraceae), Heliotropium indicum L. (family Boraginaceae), Momordica charantia L. (family Cucurbitaceae), Mimosa tenuiflora (Willd.) Poir (family Leguminosae), Borreria verticillata (L.) G.Mey. (family Rubiaceae), Solanum paniculatum L. (family Solanaceae), and Zingiber officinale Roscoe (family Zingiberaceae) also indicates the existence of compounds with anti-inflammatory activity. It is important to note that the extraction of plant materials is the first major step to test biological activities, presenting many advantages and some disadvantages compared to the isolation of pure active compounds(14). When an entire extract is used, there is a good chance of synergism between active components that can be lost when each of these components is isolated. This synergism was discovered in several medicinal tests, including those for anti-inflammatory activity. On the contrary, the mixture of different compounds together may also lead to inhibitory effects, namely, that one component may reduce the biological activity of the other. In line with this assumption, some studies have shown that the anti-inflammatory activity of pure compounds (such as amentoflavone, pseudohypericin, and hyperforin) is higher than that of the extracts. Medicinal plants are used instead of Non-steroidal anti-inflammatory drugs (NSAIDs) as the use of non-steroidal anti-inflammatory drugs is associated with several side effects, among which are unwanted effects on the gastrointestinal tract and the renal system. The biggest disadvantage of recently available potent synthetic drugs is concerning their toxicity and the reappearance of symptoms after discontinuation. Therefore, the screening and development of drugs with anti-inflammatory activity are necessary and there are many efforts to find anti-inflammatory drugs from medicinal plants(15). Inflammation is a huge challenge for human kind. Although many anti-inflammatory drugs are available, it is believed that these drugs, such as opioids and analgesia inducing drugs like NSAIDs, are not useful in all cases and these drugs also produce side effects, so to overcome these problems, new drug molecules need to be discovered from plants. Plants have many phytoconstituents helpful in reducing inflammation and fewer side effects. The objectives of the use of plants as therapeutic agents are: to concentrate and/or isolate bioactive substances for direct use as drugs; to produce bioactive compounds of novel or already known structures for semi synthesis to produce patentable entities of higher activity and/or lower toxicity; to use agents as pharmacological tools; and to use the whole plant or part of it as herbal remedy. It is worth mentioning that for the acquisition of new drugs, molecular diversity and biological function distinguish products of natural origin from synthetic products. The molecular diversity of natural products is far superior to that derived from synthesis processes, which, despite technological advances, are still restricted. This fact makes it possible for the chemical compounds present in plants to become potential drugs for different diseases. An example of a phytotherapeutic anti-inflammatory agent is Acheflan®, indicated for the local treatment of inflammatory processes, and Daflon 500 mg®, a drug composed of a purified flavonoid fraction that presents venotonic and vasoprotective action. Therefore, the study of the immunopharmacological activities of plant species has provided evidence on different extracts/fractions and chemical classes with high therapeutic potential, which represents a promising alternative to the inflammatory processes and diseases related to them, as well as a form of validation of their ethnobotanical use. Besides, data from the scientific literature have shown that molecules of plant origin present important anti-inflammatory activities and that many of their actions are related to the ability to inhibit the synthesis or action of cytokines, chemokines, and adhesion molecules, and arachidonic acid and nitric oxide pathways(16).
Alkaloids
Alkaloids are the basic nitrogenous compounds shown to have marked physiological action when given in low concentration. The important plant families containg alkaloids responsible for anti-inflammatory activities (AIAs) include Solanaceae, Leguminosae, Apocynaceae, Liliaceae, Papaveraceae, Rutaceae, and Ranunculaceae. One of the most promising compounds is tetrandine, which is chemically a bisbenzylisoquinoline alkaloid natural analogue of berbamine, and is extracted from the tuberous roots of creeper Stephania tetrandra S. Moore (Menispermaceae). It is used for the treatment of rheumatic diseases and is also efficacious in silicosis associated with inhibition of collagen synthesis, inhibits neutrophil and monocyte locomotion and lymphocyte transformation(17). Its AIAs are due to inhibition of both COX and lipooxygenase (LOX) pathways of inflammation. Like tetradine, berbamine is also found to have significantly greater inhibitory activity on prostaglandin E2 (PGE2) generation, with stronger inhibitory effects on natural-killer cell population. Tetrandine also suppresses the release and activity of inflammatory cytokines, lipid mediators, histamine as well as has an inhibitory capacity on monocytes to produce tumor necrosis factor (TNF)-α. Thus, tetrandrine is found as a prototypic tool compound for the development of new class of anti-inflammatory agents. Extract of Buxus papillosa (Buxaceae) is specially used in rheumatism and skin diseases(18). Likewise, the extracts of Buxus senzpervirens, used as a folk medicine in Turkey, have now regained potential interest for their anti-inflammatory action. The ethanolic extract of Adhatoda vasica has prominent activity against inflammations in cotton pellet induced granuloma model of inflammation.Similarly, a report by Rajput et al, on the alcoholic and aqueous extracts of the same plant also shows the extracts to have a considerable dose-dependent AIA against several animal models of inflammation.Newer alkaloids isolated from the extract of Sida cordifolia (Malvaceae) have shown high value of AIA when tested in several animal models like acetic acid induced writhing model, tail-flick latency in radiant heat tail-flick method in mice, and carrageenan-induced rat paw edema(19).

Figure 1 Chemical Structure of Berbamine
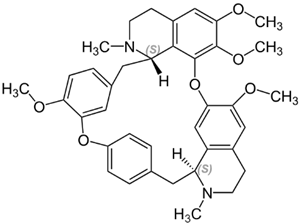
Figure 2 Chemical Structure of Tetrandrine
Glycosides
Like alkaloids, glycosides also possess potential AIA. These are found indigenously in the following families: Leguminosae, Scrophulariaceae, Polygonaceae, Solanaceae, and Myrsinaceae. Gomes and coworkers reported that the glycosidal fraction isolated from the leaves of Muesa chisia (Myrsinaceae) have profound pharmacological properties for curing inflammation. The activity was found to be mainly due to the aglycone tetrahydroxy triterpene of the oleanene series present in its glycosidal fraction. Similarly, M. chisiu is shown to have AIA resembling that of synthetic compounds like aspirin, phenylbutazone, indomethacin, in several animal models like carrageenan-induced pedal edema in rat, cotton pellet granuloma, formaldehyde-induced arthritis, and Freund's complete adjuvant induced polyarthritis(20). Akin to this, glycosides isolated from Harpagophytum procumbens (Pedaliaceae), a perennial herb indigenous to South Africa, were evaluated for their prominent AIA in carrageenan-induced pedal edema. Organic extract isolated from the aerial parts of Hypericum perforatum and Hypericum reflexum (Hypericaceae) using solvents like chloroform, methanol with subsequent fractionation, when examined for AIA showed significant restrain of acetic acid induced writhing in mice and formalin-induced pain, tail-flick test in rats. In addition to this, the phenolic glycosides isolated from the bark of Hydnocarpus annamensis were found to contain significant inflammation restraining components in its extract under spectroscopic studies. They were likely to be phenolic glycosides I and II. Similarly, profound research done on hexane and ethyl acetate fractions of the methanol extract of Dystaenia takeshimana (Umbelliferae) showed significant COX2, 5-lipoxygenase (5-LOX), prostaglandin D2 (PGD2) and leukotriene C4 (LTC4) inhibitory activity when examined in mouse bone marrow-derived mast cells(21). The spectroscopic and nuclear magnetic resonance (NMR) studies concluded that the probable constituents responsible for such activity may be coumarins, phenethyl alcohol derivatives, and two major steroidal principles, beta-sitosterol and dacusterol. Likewise, methanolic extract of leaf extracts isolated from the chromatographic fractionation of plant Andrographis stenophylla (Acanthaceae) suggested promising AIA against acute pedal paw edema in rats induced by carrageenan and Freund's adjuvant. Other uses of the extract is for treatment of snake bite caused by Naja naja venom, which causes cardiotoxicity, neurotoxicity and hemorrhagic events. Aesculushippo castanum (Hippocastanaceae), when assessed for its AIA on CoCl2-induced inflammation and hypoxia in human vascular endothelial cells, was found to give hopeful results due to the presence of a triterpenoid saponin glycoside, aescin. Xu et al, reported six different novel triterpenoid saponins which were found to have significant inflammation retarding activity when tested in xylene-induced mouse ear edema. These existed indigenously in roots of Codonopsis lanceolata (Campanulaceae). Among these, codonolaside I-III are of recent interest(22).
Terpenoids
Terpenoids are spread in several families of the plant world. The major plant families with terpenoids showing AIA include Umbelifereae, Lamiaceae, Taxodiaceae, Capparidaceae, Cucurbitaceae, Burseraceae, and Asteraceae, which have significance in the area of the research. Sesquiterpenes derived from the leaves and barks of Artemisia species like Artemisia annua and Artemisia sinica (Compositae) are of considerable interest nowadays due to several uses such as anti-inflammatory and antimalarial activity. Major constituent responsible for AIA includes diterpenoidal saponins like artemisin and artemisinin. Similarly, the extract isolated from the bark of Artemisia asiatica contains abundant amount of sesquiterpene lactones such as artemisolide, which exhibited inhibitory action against nuclear factor kB (NF-kB) cells in LPS-induced inflammation in macrophage RAW 264.7 cells, on lipopolysaccharide (LPS)-induced PGE2 and on nitric oxide (NO) production effectively. Dried rhizomes of Curcuma longa, Curcuma ambada and several other species of this family have been found to contain potential chemical constituents responsible for several useful pharmacological actions like antioxidant, antiallergic, AIA, and anticancer activities(23). Constituents like curcumin and zingiberene are found to be responsible for their prominent activities. Recently, research reported that Curcuma xanthorrhiza, Curcuma domestica and Zingiber cassumunar are of vital importance due to the presence of highly active constituent. Similarly, ethanolic extract of flowers of Arnica montana (Asteraceae) was found to contain newer anti-inflammatory principles like 1,5-trans-guaianolide on NF-kB EMSA cells and in the IL-8 ELISA cells in vitro as well as in vivo Aqueous ethanolic extracts of Lavandula multifida (Lamiaceae), a Moroccan traditional plant investigated for its activity in croton oil induced ear edema in mice followed by bioassay of the extract, was found to inhibit the inflammatory response positively in comparison to that of indomethacin(24). Constituents like styraxosides A and B, and lignans like eugenol and masutakeside I present abundantly in the stem barks of Styrax japonica (Styraceae), when subjected to preliminary screening for AIA in several models, showed potential AIA in LPS-induced NO and PGE2 production by the RAW 264.7 macrophage cell line. The activity of the plant may be probably due to its styraxoside A content, which is a potent inhibitor of NO and PGE2 production and responsible for release of TNF-α and IL-1β. Diterpenes present in the floral buds of Egletes viscosa (Asteraceae) have a topical AIA in dermal inflammation induced in mouse ear model due to the presence of centipedic acid and tanabalin. Sesquiterpenoids isolated from the whole plant extracts of Youngia japonica belonging to the family Asteraceae are now reported to exhibit a wide spectrum of AIA at doses of 50 mg/kg (i.p.) in mice(25).
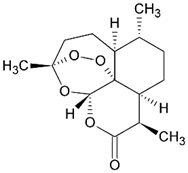
Figure 2 Chemical Structure of Artemisinin
Resins
Boswellia serrata (salai guggal) belonging to the family Burseraceae was found to possess significant AIA. When the ethanol extract of resin was injected in vivo against carrageenan-induced pedal edema in rats, mice and in adrenalectomized rat model, it showed prominent AIA, along with anti-arthritic activity against formaldehyde- and adjuvant-induced arthritis in rats. The probable mechanism may be inhibition of leukotriene production. In support to this, Ammon et al, reported AIA due to inhibition of leukotriene production in calcium-induced stimulation of 5-LOX in rat peritoneal polymorphonuclear (PMN) leukocytes in vitro(26). Recently, research done on several other species of Boswellia sp. like Boswellia carterii, commonly known as “Ruxiang Gummi olibanum”, revealed it to have a wider range of AIA in randomized, double-blinded clinical trials conducted by injecting oleoresin extract along with Complete Freund's adjuvant (CFA). Plants belonging to the Burseraceae family are reported to contain AIA due to presence of oleogum resin, boswellic acid. The action may be probably due to the inhibition of 5-LOX, leukocyte elastase enzyme and oxygen radicals competitively. Several uses of these plants include in autoimmune inflammatory diseases like Crohn's disease, ulcerative colitis, rheumatoid arthritis and bronchial asthma. Orhan et al, worked on the aqueous and ethanolic extracts of oleo gum resin obtained from Pistacia vera (Anacardiaceae). The extract evoked promising AIA on carrageenan-induced hind paw edema model in mice due to α-pinene content. Resin obtained from dragon's blood (Sanguis draconis) and from Daemonorops draco (Palmae) showed significant results for AIA and are used as a traditional medicine(27). Choy et al, reported that the ethanol extract of resin when tested against inflammation induced by LPS on RAW 264.7 cells showed positive AIA. The suggested mechanism may involve inhibition of NO and PGE2 by selective down-regulation of intrinsic nitric oxide synthetase (iNOS) and inhibition of COX2 gene expression via the suppression of NF-kB activation. In a study conducted by Seo and co-workers, where they worked on a resinous exudate obtained from the plant Pinus densiflora (Pinaceae), it was found that the resin is highly efficacious in treatment against inflammation along with several inflammatory diseases like periodontitis and gingivitis. Upon in vitro evaluation, the extract exhibited strong AIA against human gingival fibroblasts, with the strongest scavenging activity on superoxide anion radicals and on 2,2-diphenyl-1-picrylhydrazyl (DPPH) free radicals, and inhibition of hyaluronidase. When evaluated in animal models like arachidonic acid induced ear edema in mice and acetic acid induced writhing response test in mice, it exhibited 100% therapeutic value for counteracting inflammation, compared to that of the test drug, aminopyrine, whose activity was upto 76.9%(28).
Essential oils
Essential oils obtained from the roots of Carlina acanthifolia showed promising anti-inflammatory and antimicrobial activities against gram-positive bacteria. In vivo studies showed prominent AIA in a dose-dependent manner, which was comparable to that of indomethacin on carrageenan-induced rat paw edema model. Similarly, the essential oils of Cordia verbenacea (Boraginaceae) were found to reduce the carrageenan-induced paw edema in rats induced by bradykinin, substance-P, histamine, and platelet-activating factor (PAF) in mice. The major constituents of oil include sesquiterpene compounds like α-humulene and trans-caryophyllene(29). Gaultheria yunnanensis (Ericaceae) contains analgesic and anti-inflammatory principles due to the presence of active constituent, gaultherin (methyl salicylate diglycoside), and exhibited promising AIA in rats and against inflammation induced by carrageenan and croton oil in mice ear. Caryophyllene, thujopsene, α-humulene, β-acoradiene, germacrene-D, bicyclogermacrene, calamenene, germacrene-B, spathulenol and globulol are the major essential oils found abundantly in the leaf extract of Casearia sylvestris, and were found to be responsible for AIA. When tested in vitro, it showed a significant 36% reduction in paw size volume elicited by carrageenan in rats; when evaluated for gastric ulcers, it was found to reduce 90% of stress-induced gastric ulcers, as compared to cimetidine which inhibits only upto 70%. Essentials oils isolated from the n-hexane, chloroform, and methanol extracts of leaves of Rosmarinus officinalis (Labiatae) showed promising AIA when evaluated against croton oil induced inflammation in mice, topically in a dose-dependent manner which is comparable to that of indomethacin. Upon bioassay, it was demonstrated that the activity may be probably due to the presence of major active constituents like ursolic acid, oleanolic acid and micromeric acid(30).
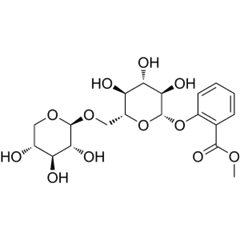
Figure 3 Chemical Structure of Gaultherin
Polysaccharides
The plants Echinacea purpurea and Echinacea angustifolia (Asteraceae) have been known since earlier days due to their immunostimulating and skin-repairing properties. Aqueous fractions obtained from the roots of these were found to have promising AIA in the skin of mice subjected to croton oil induced inflammation, due to the presence of echinacin, a polysaccharide found in high molecular weight fraction of the extract(31). Comaruman, a pectic polysaccharide extracted from the aerial parts of Comarum palustre (Rosaceae), has shown promising AIA when given orally. Comaruman was found to reduce the edema observed for 24 h after injection of 2% formalin in mice paw. In addition to this, the polysaccharide also activates adhesion of peritoneal leukocytes in vitro for AIA. Artemisia tripartita (Asteraceae) showed AIA due to the presence of polysaccharides which alter macrophage function, neutrophil count, and complement fixation function due to the presence of sulfated polysaccharides like xylose, glucose, arabinose, galactose and galactosamine(32).
Flavonoids
Kaempferol-di-coumaroyl-glucoside is the flavonol glycoside found abundantly in the extract of Quercus itex (Fagaceae). It showed prominent inhibitory activity against inflammation when applied topically. Prior evaluation for its in vitro activity in several animal models by inducing inflammatory response and dermatitis by phorbol ester (croton oil) gave satisfactory results. El-Ghazaly et al, studied that salicin is the major constituent of Populus tremula (Salicaceae) responsible for AIA using chorion allantoic membrane of hen's egg. Flavonoids like quercetin, morin, oleanolic acid, ursolic acid, glycyrrhetic acid, and caffeine were found to suppress ear edema in the inflammation induced using 12-O-tetradecanoylphorbol-13-acetate (TPA) in rabbits, predominantly due to inhibition of lipoxygenase(33). Biflavonoids including sumantoflavone and robustaflavone isolated from the extracts of Selaginella tamariscina were shown to inhibit the progression of inflammatory reactions dose dependently due to inhibition of NO production, while robustaflavone marginally affected iNOS gene expression responsible for NO synthesis. Caesalpinia pulcherrima showed prominent AIA due to the presence of flavonoids isolated from the leaf extract, and upon in vitro study, these exhibited strong AIA against LPS and IFN-γ induced inflammatory response in murine peritoneal macrophage cell lines. Eupalitin-3-O-β-D-glucoside, a flavonol glycoside isolated from the ethanolic extract of Tephrosia spinosa (Leguminosae), elicited significant AIA against carrageenan-induced paw edema, which was comparable to that of indomethacin. Similarly, phenolic flavonoids isolated from plants of indigenous origin were reported to have strong AIA by reducing the expression of adhesion molecules exhibited on endothelial cells along with selectins, VECAM-1, PECAM-1 and were shown to have prominent use in atherosclerosis(34). These include methoxyflavone and hydroxyflavone which were found to inhibit monocyte adhesions to TNF-α. Flavonoid isolated from the extract of leaves and roots of Scutellaria baicalensis (Lamiaceae), Ginkgo biloba (Ginkgoaceae) and Gentiana scabra (Gentianaceae) were reported to have topical AIA against chronic skin inflammation like atopic dermatitis. The preparation is being available in market as “SK Ato Formula” and is meant for topical application and contains flavonoids like gingkolide A and B (biflavonoids). It shows satisfactory effects in animal models with chronic type of skin inflammation induced by TPA treatment to mouse ear. The probable mechanisms behind its AIA are by inhibition of PGE2 synthesis, COX2 and consequent suppression of proinflammatory gene expression. Park et al. (2006) evaluated the extract of Ginkgo biloba and found that it exhibited inhibitory action against LPS-induced NO synthesis and PGE2 production in RAW 264.7 macrophage cell line. The major active principles found include terpenes and bi-flavonoids responsible for potent inhibition of NO and PGE2 production(35). Flavonoids like 5-O-demethylnobiletin isolated from several plant extracts are found to inhibit the inflammatory response elicited by TPA in mouse ear and acute mouse paw edema induced by carrageenan. The probable mechanism of action responsible for AIA may be inhibition of 5-LOX and elastase, respectively. The flavone was also reported to inhibit leukotriene B4 (LTB4) formation in rat neutrophils and elastase release in human neutrophils. Flavonoidal principles isolated from dichloromethane and ethanol extracts from the aerials part of Artemesia copa, such as spinacetin, jaceosidin, axillarin, penduletin, tricin and chrysoeriol, exhibited promising AIA against inflammatory mediators in mouse macrophage (RAW 264.7) cell line stimulated by LPS. Similarly, Achillea millefolium, a traditional herb used for the treatment of gastrointestinal and hepato-biliary disorders, has been found to inhibit the production of proteases, human neutrophil elastase and matrix metalloproteinase like enzymes responsible for initiation of inflammatory process, due to the presence of flavonoids and dicaffeoylquinic acids(36).
Phenolic compounds
Breu et al, investigated several phenolic compounds with saturated alkyl side chains and sulfur-containing components isolated from Allium spp. (Alliaceae) and they were found to inhibit 5-LOX against porcine leukocytes. The AIA was mainly due to the catechol content, cepaenes and unsaturated thiosulfinates. Similarly, Almeida et al, reported on lapachol, a phenolic compound isolated from the species belonging to the family Bignoniaceae. It exhibited a significant anti-inflammatory–antiedematogenic action on carrageenan-induced pedal edema by upto 57%. Sambucus ebulus (Caprifoliaceae) showed promising in vitro and in vivo AIA due to the presence of polyphenolic compound, caffeic acid, isolated from the methanolic extracts, in carrageenan-, serotonin-induced pedal edema and adjuvant-induced arthritis in rats(37). Wu and co-workers reported that the plant extract obtained from the aerial parts of Laggera alata (Asteraceae) had strong action against inflammation, due to the presence of phenolic principles, when evaluated on acute and chronic inflammations in vivo in carrageenan-induced rat paw edema, xylene-induced mouse ear edema and acetic acid induced vascular permeability in mouse. The probable mechanism may be the physiological inhibition of leukocyte migration, reduction of serum lysozyme levels, nitric oxide, PGE2 and malondialdehyde levels dose dependently(38).
Cannabinoids
Cannabinoids are now explored as a novel category of compounds occuring indigenously in fruits of Cannabis sativa (Cannabinaceae). The biological activity of the extract may be due to the Δ-tetrahydro cannabinol (Δ-THC) content. Formukong et al, showed that the presence of cannabinoids and olivetol inhibited the inflammation caused by tetradecanoyl phorbol-acetate induced erythema in mouse ear and phenylbenzoquinone-induced writhing response satisfactorily. The probable mechanism behind its AIA may involve its inhibitory activity against prostaglandin synthesis and mobilization. Recently, Zurier et al, isolated a dihydrostilbene containing compound, canniprene, from Cannabis sativa, and showed it to be most active against human neutrophils due to inhibition of 5-LOX. Similarly, olivetolic acid with a cannabinoid nucleus having free C-5 hydroxyl group is the novel anti-inflammatory principle that shows peripheral effects by inhibiting COX and LOX(39, 40).
Steroids
Steroidal and triterpenoidal saponins isolated from Ganoderma lucidum and Ganoderma tsugae exhibit AIA by inhibiting the release of β-glucuronidase from rat neutrophils stimulated by formyl-Met-Leu-Phe (fMLP)/cytochalasin B(20).
Fatty acids
Fatty acids are known from earlier days because of their several therapeutic activities like anti-inflammatory, antioxidant, free radical scavenging, antihyperlipidemic activities. Oil obtained from the leaves of Oenothera biennis (Onagraceae), called “evening primrose oil”, has gained popularity in orthodox system of medicine against inflammation seen in rheumatoid arthritis, due to the presence of fatty acids like cis-linoleic acid (γ-linoleic acid) abundantly (upto 9%). Fish oils obtained from marine organisms are of promising therapeutic value in several inflammatory disorders like psoriasis, eczema, allergy lipid lowering activity under various clinical studies(41). The proposed mechanism of action of oil includes reduction of lipid level which may be due to 5-LOX, 15-LOX, 15-HEPE inhibitory activity when examined on epidermal enzymes and basophilic leukemia cells of rat. The major constituents responsible include eicosapentaenoic acid and docosahexaenoic acid. Fixed oils obtained from the seeds of linseed Linum usitatissimum, soyabean, and Ocimum sanctum contain α-linolenic acid as the major constituent found to be responsible for prominent AIA against rat paw edema induced by arachidonic acid. The oil produced inhibition in leukotriene-induced paw edema; L. usitatissimum oil produced maximum percentage inhibition in carrageenan and arachidonic acid induced paw edema models(42).
Plant glycoproteins
Glycoproteins are of natural origin and found indigenously in animal body abundantly. Recent investigation made by Oho et al, reveals that Rhus verniciflua (Anacardiaceae) showed the presence of glycoproteins abundantly in its fruits. The glycoproteins showed promising AIA due to their inhibitory effect on proteins inducing inflammation and on no production in LPS-induced inflammation on RAW264.7 cell lines. Also, results reveal that the glycoprotein present in plant showed strong antioxidant activity against lipid peroxyl radicals in cell-free system. Similarly, the hydroalcoholic extract obtained from the most commonly available plant “Madder” Rubia cordifolia (Rubiaceae) was found to ameliorate the series of toxic inflammatory events produced by an anticancer drug, cisplatin, in Swiss Albino mice. It was found to inhibit the toxic responses like nephrotoxicity due to oxidative stress, lipid peroxidation, glutathione depletion, superoxide dismutase, and catalase(43). Lignans are the potential phytoconstituents obtained from hexane extracts of Phyllanthus amarus (Euphorbiaceae), which are found to inhibit carrageenan-induced paw edema and neutrophil influx in rats. These lignans include a group of phytoconstituents such as phyltetralin, nirtetralin, niranthin, phyllanthin. Among these, only nirtetralin was found to inhibit the inflammation induced by carrageenan, due to increase in IL1-β level in tissues, while the whole extract was found to reduce the paw edema elicited by bradykinins, platelet activating factors (PAF) and endothelin-1 prominently. Like lignans, the “neolignans”, isomeric structural analogues isolated from stem barks of several species of Piper kadsura (Piperaceae), are of promising value in the field of pharmacognosy for treatment of several inflammatory disorders of human ailments and in the inhibition of polymethacrylic acid induced production of reactive oxygen species (ROS) in human PMN neutrophils. Sosa and co-workers isolated a novel class of compounds with potent topical anti-inflammatory principle from the extract of Achillea pannonica (Asteraceae) by fractionation(44). These are derivatives of germacrane and were found to exhibit AIA against inflammatory events initiated by croton oil induced dermatitis in the mouse ear in a dose-dependent manner, by upto 61%. Verminoside (an iridoid glycoside) is found abundantly in the dichloromethane extract of Kigelia africana (Bignoniaceae) occurring in northern zones of Africa. When evaluated for its in vitro anti-inflammatory activity, this constituent showed higher potential of inhibiting the expression of iNOS and NO release in mouse J774.A1 macrophage cell line. Ethanolic extract of seeds obtained from the chromatographic fractionation of Nyctanthes arbortristis (Oleaceae) was found to contain analgesic–anti-inflammatory and antinociceptive activities due to the presence of arbortristoside-A. In an animal study, the extract exhibited significant action against carrageenan-, serotonin-, and histamine-induced inflammatory reactions, due to inhibition of arachidonic acid synthesis(45). Phenylpropanoids are the active antinflammatory principles isolated from the species of Illicium like Illicium tashiroi, Illicium anisotum, Illicium arborescens and are potentially found to have promising AIA due to inhibition of histamine release, when tested on rat basophilic RBL-2H3 leukemia cells stimulated by A23187. Plants belonging to the family of Iridaceae like Eleutherine americana contain a novel class of plant constituents such as naphthoquinones used for their AIA. When evaluated in vitro, they showed satisfactory action against inflammation induced by LPS in mouse macrophage RAW 264.7 cell lines. Similarly, luteolin is a newer flavone which occurs indigenously in several plants and helps a lot for its antioxidant, antinflammatory and antiallergic functions as compared to other flavonoids(46).
Clinical Trials
Table 2 Clinical Trials
|
Name of the herbal |
Active plant of herbal |
No. of subjects |
Type of trials |
Inference |
|
Puri?ed gugulu (Commiphora mukul) |
Ethyl acetate extract |
35 Patients of rheumatoid arthritis |
Randomized, double- blind trial |
Extract showed digestive and analgesic effect without any side effects |
|
Curcumin |
Turmeric extract
|
18 Rheumatoid arthritis patients
40 Male patients affected with inguinal hernia
|
Large, double-blind study
A placebo-controlled trial |
Improved symptoms in patients with osteoarthritis and rheumatoid arthritis More effective than placebo in reducing post-surgical edema, tenderness and pain, and was comparable to phenylbutazone |
|
Boswellia serrata extract |
Boswellin, boswellic acids
|
44 Patients
23 Males and 17 females
30 Patients of osteoarthritis of knee
|
Randomized, double-blind, verum-controlled, parallel group
Double-blind, placebo-controlled study
Randomized, double-blind, placebo-controlled, crossover study |
Study con? rms that therapy with Boswellia reduces in? ammation in the treatment of Crohn’s disease 70% of patients showed improvement in exacerbation of asthma with disappearance of physical symptoms and signs of asthma All patients receiving the herbal treatment reported decrease in knee pain, increased knee ? exion and increased walking distance |
|
White willow bark extract |
Salicin |
191 Patients
127 Outpatients |
A 4-week, double-blind, clinical trial
Randomized, double-blind, controlled trials |
Moderate ef?cacy was demonstrated with both doses of salicin for short-term treatment of acute episodes of chronic lower back pain Showed higher ef?cacy in the treatment of osteoarthritis and rheumatoid arthritis as comparable to diclofenac |
|
Devil's claw |
Ethanolic extract |
122 Patients |
Randomized, double-blind, parallel group study |
Showed higher ef? cacy in the treatment of osteoarthritis related knee and hip pain, lower back pain, and ef?cacious in rheumatism |
ADVANTAGES
In acute settings, the analgesic effects of non-aspirin NSAIDs are comparable to those of starting doses of opioids. However, unlike opioids, NSAIDs have a ceiling dose above which no additional pain relief occurs, although higher doses do mediate anti-inflammatory effects. Clinical studies in patients with arthritis have shown that non-aspirin NSAIDs are comparable to aspirin in reducing pain, joint swelling, and duration of morning stiffness, as well as in improving strength and mobility. In randomized, double-blind, controlled trials using acetaminophen as the comparator, diclofenac, a nonselective NSAID, and celecoxib, a COX-2-specific NSAID, demonstrated greater relief of pain and stiffness. A growing body of evidence has identified inflammation as an important component of the pathogenesis of OA and OA-related pain. Inflammatory cytokines and proteases contribute to a varying extent in the process of joint destruction and exacerbation of nociception. Individual differences in both the degree of inflammation and susceptibility to nociception sensitization may explain, at least in part, why some patients with limited disease radiographically have severe pain, while other patients with more severe deterioration of the joint have minimal pain. For this reason, the use of analgesics without anti-inflammatory properties in the joints, such as acetaminophen, would only provide pain relief without clinically beneficial anti-inflammatory activity. Among the nonselective NSAIDs, both ibuprofen and naproxen are available in OTC and prescription dosing options. The safety and efficacy of OTC dosing of ibuprofen and naproxen have been assessed in large clinical trials. OTC doses of both ibuprofen and naproxen provided significantly improved pain control over placebo. Similarly, ibuprofen and naproxen have been shown to be significantly more effective than acetaminophen for the treatment of pain associated with OA. A comparison of ibuprofen with acetaminophen found that pain relief was superior with ibuprofen, both after single dosing (ibuprofen 400 mg, acetaminophen 1000 mg) and after 14 days of treatment (ibuprofen 400 mg, acetaminophen 1000 mg). Similarly, pain relief with naproxen versus placebo at dosages of 660 mg/day (440 mg/day in patients ≥65 years old) was greater than that of acetaminophen versus placebo at dosages of 4000 mg/day. Patients without contraindicating conditions (pain persisting for >2 weeks, pain with nausea or severe vomiting, weakness in any limb, pain in a red, hot, or swollen joint, suspected fracture, pelvic or abdominal pain, suspected pregnancy, and increased intensity of pain or any change in the character of pain), can self-treat using OTC NSAIDs over a period of 10 days or less. Use of these agents for more than 10 days, even at recommended nonprescription doses, requires the supervision of a physician, as long-term self-treatment could mask a more serious condition requiring a physician's intervention(8, 10, 47-50).
DISADVANTAGES
Applications
Anti-inflammatory herbs can be used to treat a variety of conditions, including:
REFRENCES


Prajapati Rahul*, Gohil Malvi, Saiyad Suzannisha, Karodiya Snehal, A Systemic Review on Plant Based Anti-Inflammatory Agents, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 501-519. https://doi.org/10.5281/zenodo.14993026
 10.5281/zenodo.14993026
10.5281/zenodo.14993026