
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Samarth Institute of Pharmacy, Belhe, Junnar, Maharashtra, India
Natural polymers, gums, and mucilages have emerged as crucial bioadhesive components in various drug delivery routes, including oral, nasal, ocular, transdermal and vaginal applications. This study highlights the unique properties of these biopolymers, which enhance drug retention and absorption through mucoadhesion mechanisms. This comprehensive overview examines the advantages of these bioadhesives, focusing on their ability to enhance drug solubility, stability, and localized delivery. The mechanisms of adhesion, such as hydrogen bonding and van der Waals forces, are discussed in relation to different drug delivery systems. This overview explores the diverse functionalities of these biopolymers, focusing on their mucoadhesive properties that facilitate prolonged drug residence time and enhanced absorption. Case studies are presented, illustrating the various natural polymers in the pharmaceutical application like a suspending agent, emulsifying agent, mucoadhesive agent, binder, disintegrant, Drug release Biodegradable carrier for colon specific release, enteric resistant and sustained release substantial and many more. Additionally, the review addresses the physicochemical characteristics that contribute to bioadhesion and the implications for patient compliance and therapeutic efficacy. It concludes with insights into future research directions and the potential for these natural materials to improve drug delivery.
Bioadhesion is stated as the ability of a natural or synthetic polymer to stick to a biological article. The term is referred to as mucoadhesion when the biological substrate is a mucosal layer [1].
The adherence of two materials where at least one of the components is biological is known as bioadhesion. The delivery of drugs with improved bioadhesion has drawn a lot of interest in the last few decades. Bioadhesive dosage forms can be made to stay at the application site for extended periods of time, allowing for regulated drug release and better therapeutic results. Dosage forms that are not soluble in acid or undergo severe first pass digestion can be applied to mucosal surfaces to potentially benefit medication molecules that are not suited for oral administration. A dosage form's capacity for bioadhesion is contingent upon several elements, such as the characteristics of the mucosal tissue and the physical and chemical properties of the polymeric composition. Bioadhesive materials and their synthesis, variables influencing bioadhesion, assessment techniques, and, lastly, several features of bioadhesion include various bioadhesive pharmaceutical delivery methods (buccal, nasal, ophthalmic, gastro, vaginal, and rectal) [2].
Adhesion is the bond created when a surface and pressure-sensitive adhesive (PSA) come into contact [3]. Bioadhesion is the long-term attachment of two materials—at least one of which is biological. due to interfacial forces. It can also refer to a substance's ability, whether synthetic or biological, to adhere to biological tissue for an extended period of time [4].
There are three primary categories of bioadhesion in biological systems:
Type 1: biological stages adhering to one another, as in the case of wound healing, platelet aggregation, cell fusion, and normal cells adhering to diseased or foreign materials
Type 2: refers to the attachment of a biological phase to an artificial substrate, such as the development of biofilms on prosthetic devices and inserts, microbial fouling and barnacle adherence to ships, adherence of platelets to biomaterials, and cell adhesion to culture plates.
Type 3: adhesion of an artificial material to a biological substrate, such as the adhesion of synthetic hydrogels to soft tissues or sealants to dental enamel [5,6]A water-soluble polymer's ability to bioadhere, which turns adhesive upon hydration [7],makes it possible to target a drug to a specific area of the body for prolonged periods of time [8]
Theories Of Bioadhesion
1.1.1 The Wetting Theory:
The interaction between the thermodynamic work of adhesion, the bioadhesive, and its angle of contact are best described by the wetting theory when it comes to liquid bioadhesives. The Dupré equation describes how the work is connected to the surface tension of the adhesive and substrate [9]
WAB = γA + γB – γAB.
interfacial energy, γAB.
interface between phase A and air (γA)
the interface between phase B and air (γB).
When an electrical double layer arises between an adhesive and a substrate. electrostatic forces resulting from this formation must be overcome in order to separate two distinct substances. According to the electrostatic theory of repulsion, an electrical double layer is created when electrons are transferred across the adhesive interface, and a number of attractive forces keep the two layers in touch. The adhesive interface works similarly to a parallel-plate condenser, requiring labor against electrical charges to achieve separation. If no work is done to overcome van der Waal's forces, the work of adhesion can be associated to the energy of the condenser [10].
Mechanical Theory: According to this theory, bioadhesion occurs when a liquid or semi-solid bioadhesive polymer penetrates into the irregularities, pores, or crevices of a biological tissue (such as mucosa). After penetration, the polymer solidifies or swells, leading to mechanical anchoring that holds the dosage form in place.
Mechanism
Important Factors
Significance
Limitation
In summary, the mechanical theory states that bioadhesion occurs due to physical entrapment of the adhesive polymer within surface irregularities of the biological tissue.
Top of Form
Bottom of Form
Cohesive Theory of Bioadhesion
The cohesive theory of bioadhesion states that adhesion occurs due to the internal strength (cohesive forces) of the bioadhesive material rather than interactions with the biological surface. Once the bioadhesive polymer comes into contact with the tissue, it adheres and remains attached because of strong intermolecular forces within the polymer itself.
Mechanism
Important Factors
Significance
Limitation
In summary, the cohesive theory explains bioadhesion as a result of strong internal cohesive forces within the bioadhesive polymer that hold it in place on the biological tissue.
1.1.3 Theory of Diffusion:
Diffusion theory states that a semipermanent adhesive bond is formed when the polymer chains and mucus mix thoroughly enough. The diffusion coefficient and contact time determine the exact depth to which the polymer chains enter the mucus. As the cross-linking density rises, The diffusion coefficient, which is reliant on the molecular weight between cross-links, significantly decreases as shown in figure 1 [11].
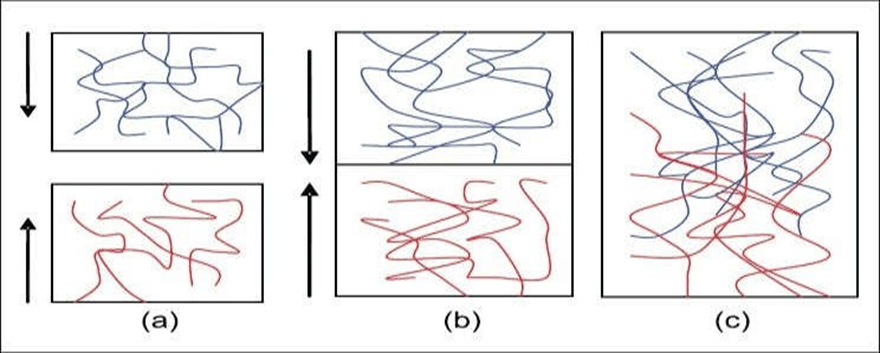
Fig.1: (a) Theory of diffusion -blue polymer layer and red mucus layer before interaction; (b) after interaction (c) The interface becomes diffuse after interaction for a period of time[11]
1.1.4 Adsorption Theory of Bioadhesion:
According to the adsorption theory, the adhesive interaction between the substrate surfaces is caused by intermolecular forces such as hydrogen bonding and VanderWaal's forces.
According to the theory, adherence to tissue is sustained by the combined effect of single or several secondary forces. The kinds of secondary forces are;
In bioadhesion, it is not desirable for primary chemical bonds to form between tissue and adhesives used in dentist and surgery. This is due to the possibility of permanent adhesion caused by the strong ionic or covalent bonds [12].
1.2.3. Physiological Variables:
I] Mucin Turnover
II] Sickness States
Vaginal bioadhesive preparations have emerged as a novel controlled-release form of medication for the management of systemic and topical conditions in recent years. The biggest benefit of these dosage
forms is that they can be kept in the vagina for long stretches of time, both during the day and at night, which allows for fewer dosing intervals. [13-17].
In recent years, there has been a growing investigation into the vagina as a potential site for drug delivery due to its anatomical position and physiological attributes. This approach, when combined with the bioadhesion phenomenon, has produced successful local and systemic drug delivery outcomes.
Treatment for vaginal disorders such as candidiasis, STDs, vaginal dryness, and others has been provided by bioadhesive vaginal drug delivery systems. Also, Studies have indicated that medications can be effectively absorbed into the bloodstream through the vaginal mucosa. Furthermore, this vaginal route has been employed for medication targeting in the uterus (18).
This is especially true for API that have low absorption rates following oral administration, which makes it necessary to take use of alternate drug delivery methods. Currently under investigation are the mucosal pathways of the nasal, ophthalmic, buccal, vaginal, and rectal regions. Among With these routes, vagina appears to be a viable site for medication delivery. The vagina is a tubular, fibromuscular organ that stretches from the uterine cervix to the vaginal vestibule and measures approximately 9 cm in length. [19].
The vagina is made up of four separate layers: stratified squamous epithelium, lamina propria, and muscle layer, and adventitia as shown in the below figure-2. The mucosal layer generates a series of transverse folds known as rugae, which drastically expand its surface. Even though considered a mucosal tissue, the normal vagina does not have glands, and vaginal discharge is a mixture of fluids from a variety of sources. This mucus covering has various critical physiological functions, including drug absorption or activity. It is also worth noting that vaginal characteristics alter with the menstrual cycle, particularly pH and vaginal fluid: the usual pH ranges from 4.5 to 5.5, while vaginal fluid changes greatly in volume, content, and rheological qualities. Lactobacilli are abundant in the healthy vagina and play a crucial function in maintaining vaginal pH and controlling infection by common pathogens [20,21].
Along with age as well as menstrual cycle Vaginal histology and physiology may differ. The thickness of the vaginal epithelium fluctuates with age because the levels of ovarian steroids change. From birth until adolescence, the vaginal epithelium is very thin, but after puberty, the usual thickness of the vaginal epithelium is roughly 200 pm [22].
The vaginal BDD (body dysmorphic disorder) system has been used for both local and systemic drug delivery, particularly in female-related disorders. Traditionally, the vaginal cavity has been utilized to administer locally acting medications such as antibacterial, antifungal, antiprotozoal, antiviral, labor- inducing, spermicidal, prostaglandin, and steroid. Formulations that can prevent the transmission of sexually transmitted diseases (STDs), including AIDS, have made significant progress during the last decade [21].

Fig. 2: Illustration of the vaginal wall structure [20]
The oral mucosa is composed of an outermost layer of stratified squamous epithelium (about 40-50 layers thick), a lamina propria followed by the sub mucosa as the innermost layer. The composition of the epithelium varies depending on the site in the oral cavity. The mucosa of the gingival and hard palate are keratinized similar to the epidermis contain neutral lipids like ceramides and acylceramides which are relatively impermeable to water. The mucosa of the soft palate, the sublingual, and the buccal regions, however, are not keratinized contain only small amounts of ceramides.
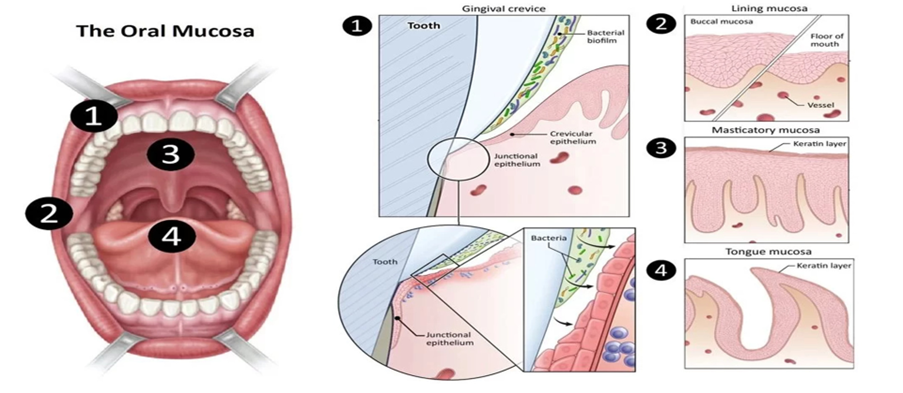
Fig 3: Illustration of the Oral Mucosa [23]
Novel buccal dosage forms: The novel type buccal dosage forms include buccal adhesive tablets, patches, films, semisolids (ointments and gels) and powders.
The oral cavity has a relatively small surface area (approximately 50 cm2). The oral mucosa is composed of stratified squamous epithelium, an outermost layer similar to that found in the rest of the body. It has a mitotically active basal cell layer, advancing through a number of differentiating. intermediate layers to the superficial layers, where cells are shed from the surface of the epithelium The turnover time for the buccal epithelium has been estimated at 5–6 days, a time probably representative of the oral mucosa as a whole. The oral mucosal thickness varies depending on the site: the buccal mucosa measures at 500–800 mm, while the mucosal thickness of the hard and soft palates, the floor of the mouth, the ventral tongue, and the gingivae measure at about 100-200 mm [23-25] .
An ideal polymer for an oral bioadhesive drug delivery system should have the following characteristics
1.4 OCULAR MUCOSA
Ocular mucosal drug delivery systems are designed to enhance the absorption and bioavailability of therapeutics applied to the eye. Traditional ocular formulations, such as eye drops, often suffer from rapid drainage and limited contact time with the mucosal surface. To address these challenges, various innovative approaches are being developed:
Overall, advancements in ocular mucosal drug delivery systems hold great promise for improving therapeutic outcomes in ophthalmic treatments. These innovative strategies aim to enhance drug absorption, reduce side effects, and increase the overall effectiveness of ocular therapies.
Anatomy of the Ocular Mucosa
Conjunctiva: A thin, transparent membrane covering the inner surface of the eyelids (palpebral conjunctiva) and the white part of the eyeball (bulbar conjunctiva). Contains goblet cells that produce mucus, contributing to tear film stability and ocular surface lubrication.
Cornea: The outermost layer of the eye, composed of five layers (epithelium, Bowman's layer, stroma, Descemet's membrane, and endothelium). The epithelium is rich in tight junctions, providing a barrier that regulates the permeability of substances.
Tear Film: A thin layer of fluid covering the ocular surface, composed of three layers like Lipid layer, Aqueous layer, Mucin layer
Sclera: The white, protective outer layer of the eye, providing structural support. Less permeable than the cornea but important in ocular drug delivery [28] .
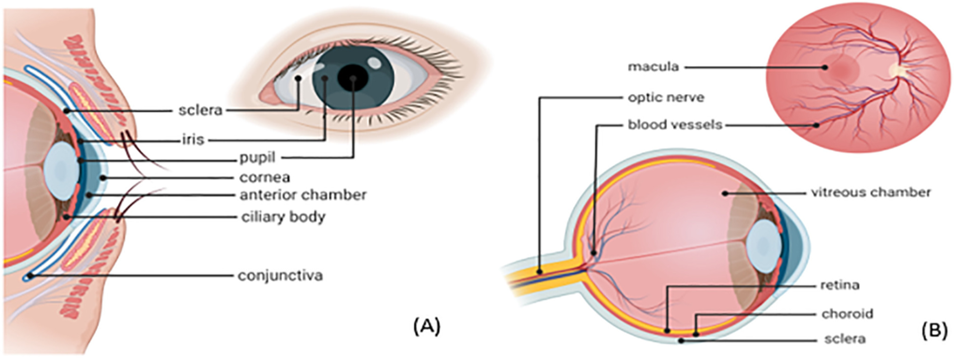
Fig 4: Schematic representation of the (A) anterior ocular anatomy (B) posterior ocular anatomy [28]
Rectal anatomy and scope of drug selection
Anatomically, the rectum forms the distal part of the large intestine. A normal adult human rectum is about 12–15 cm long and deviates in three lateral curves: upper, middle and lower.
It is considered a cylindrical organ that does not contain villi or microvilli on the luminal surface and is mainly associated with water absorption and re-absorption from the gastro intestinal (GI) contents. Average rectal surface area is reported to be around 200–400 cm2 and the pH is 7.2–7.4,
The rectum is structured with columnar epithelial cells along with goblet cells that are responsible for mucous secretion. The mucous forms a layer approximately 100 mm that acts as a protectant to the rectal epithelia and is also a barrier for drug absorption [29-30].
Dosage forms for rectal route
Solid rectal dosage forms, Suppositories, Rectal capsules, tablets or powder for reconstitution, Liquid rectal dosage forms, Semi-solid rectal dosage forms.
The nasal cavity is one of the most easily accessible and well tolerated drug delivery region in the body. It has the advantages like high surface area (approximately 150 cm2 ) with very rich blood vessels and good nasal cavity volume (approximately 15-20 ml). The mucus layer is regularly renewed every 15-20 min.
The turbinate region is the middle and the most important region of the nasal cavity. This area is the main area for the delivery of different formulations. It is composed of Superior, Middle and Inferior turbinate. The entire turbinate region is richly supplied with blood vessels and lymph vessels. The epithelial cells present in these regions are mainly ciliated/non-ciliated, basal and mucus secreting goblet cells. The ciliated cells are responsible for secretion of mucus, the ciliated and nonciliated cells have microvilli which provide very high surface area required for improved drug absorption. [31-33].
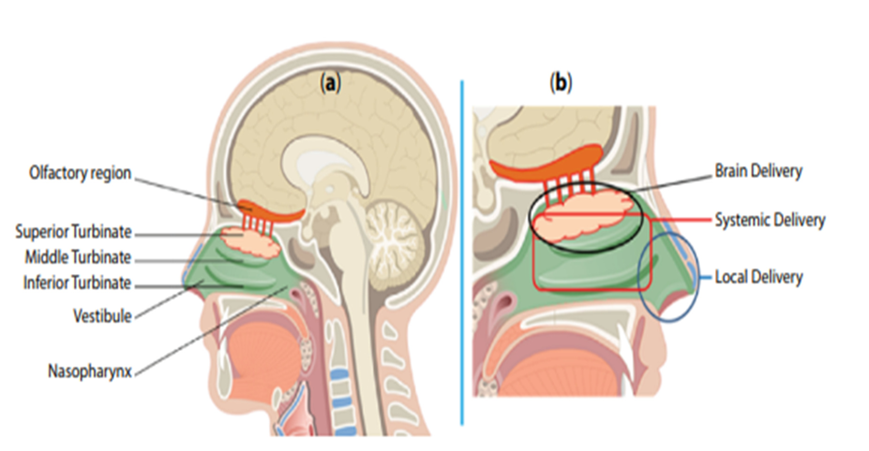
Fig 5: Illustration of the (a) Areas of Nasal Cavity (b) Possible drug delivery through nasal route [32]
Nasal Route for Brain Drug Delivery
Superior Turbinate region has a very rich supply of olfactory nerves and blood vessels. It is reported that the olfactory nerves reaching olfactory mucosa pass through cribriform plate of ethmoid bone. These nerves pass through the cribriform plate along with the arachnoid membrane which is filled with cerebrospinal fluid (CSF). The drugs to be delivered to the Central Nervous System (CNS), if delivered through nasal route, get adhered and lined to the olfactory mucosa of the Superior Turbinate region [34- 35].
Nasal Route for Local and Systemic Drug Delivery
The turbinate region of the nose is sectored as Superior, Middle and Inferior Turbinate. The whole turbinate area is richly supplied with blood and lymph vessels and thus is an important area for systemic drug and vaccine delivery. The cells present in turbinate region are mainly of four types: basal cells, ciliated cells, nonciliated cells, and goblet cells which are present on basement membrane and are richly supplied with blood vessels and thickly covered with mucus and pericillary fluid [36].
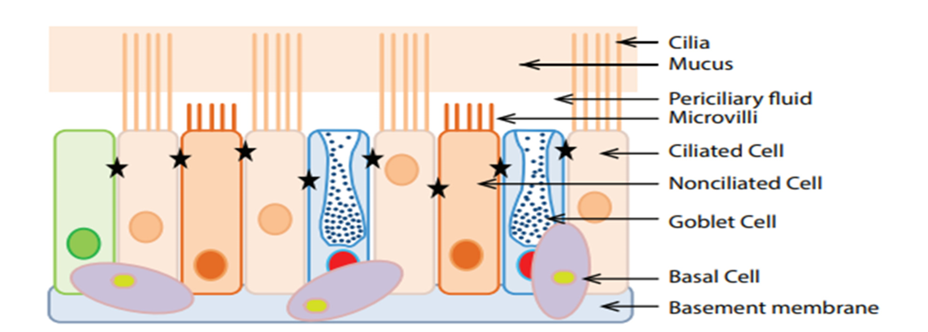
Fig 6: Cells in human nasal epithelium [32]
There are mainly four types of cells present in the nasal epithelium attached to basement membrane: Basal cells, goblet cells, ciliated cells, and nonciliated cells. Out of which goblet cells, ciliated cells and nonciliated cells are attached to each other through tight junction between cells (shown by blue star). The mucus layer is present over the periciliary fluid which acts as lubricating layer and provides sliding movement to mucus layer in ciliary clearance mechanism. These cells and tight junction also contribute to different drug absorption mechanisms [37].
TABLE 1: STUDIES ON NATURAL MUCILAGES AND GUMS [38-74]
|
Mucilage/ gums |
Botanical name |
Family |
Pharmaceutical Application |
Reference |
|
Lipidium sativum |
Lepidum sativum |
Cruciferae |
Suspending agent, emulsifying agent, |
38-39 |
|
Cordia gum |
Cordia dichotoma |
Boraginaecae |
Sustained release matrix |
40 |
|
Mucuna gum |
Mucuna flagillepes |
Papillionaceae |
Microspheres |
41 |
|
Okra mucilage |
Hibiscus esculentus |
Malvaceae |
Hydrophilic matrix for controlled |
42 |
|
Acacia |
Acacia Senegal |
Leguminosae |
Osmotic drug delivery |
43,44 |
|
Bhara gum |
Terminalia bellirica |
Combretaceae |
Sustained release |
45,46 |
|
Cactus mucilage |
Opuntia ficus-indica |
Cactaceae |
Gelling agent in sustained drug delivery |
47 |
|
Guar gum |
Cyamopsis tetraganoloba |
Leguminosae |
Colon targeted drug delivery, |
48-51 |
|
Locust bean gum |
Ceratania siliqua |
Leguminosae |
Controlled release agent |
52 |
|
Okra gum |
Abelmuschus esculentus |
malvaceae |
suitability as suspending and disintegrating agent |
53 |
|
Almond gum |
Prunus communis |
Rosaceae |
emulsifier, thickener, suspending pharmaceutical, adhesive, glazing agent and stabilizer. Gum obtained from Almond as a binder in tablet formulations |
54 |
|
Neem gum |
Azadirachta indica |
Meliaceae |
Binder |
55-57 |
|
Gellan gum |
Pseudomonas elodea |
|
Disintegrating agent |
58 |
|
Aloe mucilage |
Aloe barbadensis Miller |
|
A controlled delivery system |
59 |
|
Albizia gum |
Albizia zygia |
Leguminosae |
Binding agent, suspending agent |
60 |
|
Karaya gum |
Firmiana simplex |
Malvaceae |
gastric retentive dosage forms improve rate of dissolution of drug solid dispersions. Suspending agent Emulsifying agent. Dental adhesive Sustaining agent. Mucoadhesive |
61 |
|
Tamarind gum |
Tamarindus indica L. |
Fabaceae |
Drug release Biodegradable carrier for colon specific release |
62 |
|
Grewia gum |
Grewia mollis Juss |
Malvaceae |
Controlled release dose formulations. Suspending the agent increase. The release of cimetidine from tablets is controlled by the degree of packing and fluidity of the granules, which delay the release. Film making property |
63-68 |
|
Cashew gum |
Anacardium occidentale L. |
Anacardiaceae |
As suspending agent |
69 |
|
Cordia mucilage |
Cordia myxa |
Boraginaceae |
As enteric resistant and sustained release substantial |
70 |
|
Fenugreek gum |
Trigonella foenum graecum |
Leguminosae |
As an emulsifier and binding agent, suspending agent, mucoadhesive preparations. |
71 |
|
Moi gum |
Lannea coromandelica |
Anacardiacea |
As a microencapsulating agent, release rate control material. |
72 |
|
Moringa gum |
Moringa oleifera |
Moringaceae |
As a mucoadhesive agent, binder, disintegrant |
73 |
|
Xanthan gum |
Xanthomonas campestris |
Xanthomonadacae |
As a suspending agent, emulsifying agent, |
74 |
1. Grafted Polymers
Definition: Grafted polymers are copolymers in which one or more types of polymer side chains (grafts) are chemically attached to a main polymer backbone, forming a branched structure with different polymers in the backbone and the branches.
TABLE 2: STUDIES ON GRAFTED POLYMERS
|
SR. NO. |
Natural Gum / Mucilage |
Source / Botanical Origin |
Key Chemical Composition |
Important Properties |
Common Grafted Polymers (Graft Co-polymers) |
Applications of Grafted Polymer |
|
1 |
Lepidium sativum (Garden cress mucilage) |
Seeds of Lepidium sativum |
Polysaccharides (D-galactose, L-rhamnose, D-xylose), uronic acids |
High viscosity, gel-forming, biodegradable |
Polyacrylamide (PAM), Polyacrylic acid (PAA), Poly(N-vinyl-2-pyrrolidone) (PVP), Acrylic acid–Acrylamide copolymers |
Hydrogels, drug delivery matrices, thickener |
|
2 |
Cordia gum (Cordia dichotoma) |
Fruits of Cordia dichotoma |
L-arabinose, D-galactose, uronic acids |
High water absorption, film-forming |
Polyacrylamide, Polyacrylic acid, Methyl methacrylate (MMA) grafts |
Controlled drug release, bioadhesive films |
|
3 |
Mucuna gum (Mucuna pruriens) |
Seeds of Mucuna pruriens |
Galactomannans |
High viscosity, stable over pH, biodegradable |
Polyacrylamide, Polyacrylic acid, GMA (glycidyl methacrylate) grafts |
Hydrogels, tablets, biomedical coatings |
|
4 |
Okra mucilage (Abelmoschus esculentus) |
Okra pods |
Rhamnose, galactose, galacturonic acid |
Excellent thickening, mucoadhesive, non-toxic |
Polyacrylic acid, Acrylamide, Acrylic acid–Acrylamide copolymers |
Wound dressing, oral drug delivery, hydrogels |
|
5 |
Acacia gum (Gum Arabic) |
Acacia senegal tree exudate |
Arabinogalactan protein, rhamnose, glucuronic acid |
Emulsifying, soluble, film-forming |
Acrylamide, Acrylic acid, N-vinyl pyrrolidone |
Nanocomposites, controlled-release systems |
|
6 |
Bhara gum (Butea monosperma gum) |
Exudate of Butea monosperma tree |
Galactose, arabinose, rhamnose |
Swelling, gel-forming, biodegradable |
Polyacrylamide, Polyacrylic acid, Methyl methacrylate |
Drug release matrices, hydrogel films |
|
7 |
Cactus mucilage (Opuntia species) |
Opuntia ficus-indica and others |
Arabinose, xylose, galactose, pectic substances |
Water retention, flocculating, eco-friendly |
Polyacrylic acid, Acrylamide, Acrylic acid–Acrylamide |
Water treatment hydrogels, superabsorbents |
|
8 |
Guar gum |
Seeds of Cyamopsis tetragonoloba |
Galactomannan |
Excellent thickener, stable, high viscosity |
Polyacrylamide, Polyacrylic acid, Polyvinyl alcohol (PVA), GMA |
Superabsorbents, drilling fluids, drug carriers |
|
9 |
Locust bean gum (Carob gum) |
Seeds of Ceratonia siliqua |
Galactomannan (mannose:galactose 4:1) |
Synergy with other gums, gel-enhancing |
Polyacrylamide, Polyacrylic acid, Acrylamide-acrylate copolymers |
Hydrogels, packaging films, biomedical gels |
|
10 |
Okra Gum (Okra Mucilage) |
Pods of Abelmoschus esculentus |
Rhamnose, galactose, galacturonic acid |
Thickener, mucoadhesive, biodegradable |
Acrylic acid (AA), Acrylamide (AAm), Polyacrylic acid (PAA), N-vinyl pyrrolidone (NVP) |
Hydrogels, wound dressing, controlled drug release |
|
11 |
Almond Gum |
Exudates of Prunus amygdalus |
Arabinogalactans, glucose, uronic acids |
Film-forming, emulsifying |
Polyacrylamide, Polyacrylic acid, Methyl methacrylate (MMA) |
Drug carriers, biodegradable films |
|
12 |
Neem Gum |
Exudate of Azadirachta indica |
Arabinose, galactose, fucose |
Swellable, stable |
Polyacrylamide, Acrylic acid, AAm-AA copolymers |
Hydrogel beads, heavy metal adsorption |
|
13 |
Gellan Gum |
Produced by Sphingomonas elodea |
Glucose, rhamnose, glucuronic acid |
Strong gel former, thermostable |
Polyacrylamide, PEG-based grafts, Polyacrylic acid |
Tissue engineering, drug release |
|
14 |
Aloe Mucilage (Aloe vera Gel) |
Leaves of Aloe barbadensis |
Acetylated polysaccharides (acemannan) |
Hydrating, bioactive |
Polyacrylamide, Acrylic acid, Chitosan-graft polymers |
Wound healing gels, moisturizing hydrogels |
|
15 |
Albizia Gum |
Albizia zygia exudate |
Galactose, arabinose, rhamnose |
Thickening, bioadhesive |
Polyacrylic acid, Polyacrylamide |
Tablets, sustained release systems |
|
16 |
Karaya Gum (Sterculia Gum) |
Exudate from Sterculia urens |
Galactose, rhamnose, galacturonic acid |
Highly swellable, bioadhesive |
Polyacrylamide, Acrylic acid, GMA grafts |
Superabsorbents, colon-targeted drug delivery |
|
17 |
Tamarind Gum (Tamarind Kernel Powder) |
Seeds of Tamarindus indica |
Xyloglucan |
Gel-forming, stable viscosity |
Acrylic acid, Acrylamide, Polyacrylic acid, MMA |
Hydrogels, sustained release tablets |
|
18 |
Grewia Gum (Grewia Polysaccharide) |
Bark of Grewia mollis or Grewia gumifera |
Rhamnogalacturonan, arabinose, galactose |
Thickener, mucoadhesive |
Polyacrylamide, Acrylic acid, GMA |
Drug release beads, hydrogels |
|
19 |
Cashew Gum |
Exudate of Anacardium occidentale |
Arabinogalactan, glucose, glucuronic acid |
Soluble, emulsifying |
Polyacrylamide, Polyacrylic acid, MMA |
Nanoparticles, drug delivery, coatings |
|
20 |
Cordia Mucilage (Cordia gum) |
Fruits of Cordia myxa / Cordia dichotoma |
L-arabinose, D-galactose, uronic acids |
Water absorption, film-forming |
Polyacrylamide, Polyacrylic acid, MMA |
Bioadhesive films, hydrogels |
|
21 |
Fenugreek Gum (Fenugreek Galactomannan) |
Seeds of Trigonella foenum-graecum |
Galactomannan (mannose:galactose 1:1) |
Thickener, stabilizer |
Acrylic acid, Acrylamide, NVP, GMA |
Superabsorbents, drug delivery |
|
22 |
Moi Gum (Moi seed gum) |
Seeds of Bassia latifolia (also known as Mahua tree) |
Galactomannans (mannose + galactose), uronic acids, minor proteins |
High viscosity, strong gel-former, biodegradable |
Acrylic acid (AA), Acrylamide (AAm), Polyacrylamide (PAM), Methyl methacrylate (MMA) |
Superabsorbent hydrogels, drug controlled-release matrices, water retention polymers |
|
23 |
Moringa Gum |
Exudate from bark of Moringa oleifera |
Arabinose, galactose, xylose, rhamnose, uronic acids |
Thickener, emulsifier, bioadhesive, stable |
Polyacrylamide (PAM), Polyacrylic acid (PAA), N-vinyl pyrrolidone (NVP), Acrylamide-acrylate copolymers |
Bioadhesive tablets, hydrogels, flocculants, biomedical films |
|
24 |
Xanthan Gum |
Fermentation gum produced by Xanthomonas campestris |
Glucose, mannose, glucuronic acid; cellulose-like backbone |
High viscosity at low concentrations, shear thinning, stable across pH & temperature |
Polyacrylamide, Polyacrylic acid, GMA (glycidyl methacrylate), MMA, NVP |
Drug delivery hydrogels, sustained-release matrices, tissue engineering scaffolds, viscosity modifiers |
1.7 APPLICATION OF POLYMERS
1.8 ADVANTAGES
The mechanism of action of gums and mucilage on the vaginal route primarily involves their ability to provide lubrication, hydration, mucoadhesion, and potentially act as carriers for drug delivery systems.
Hydration and Lubrication: Gums and mucilage possess hydrophilic properties, enabling them to absorb water and form a gel-like consistency. When applied vaginally, they help hydrate the vaginal mucosa and provide lubrication, reducing friction and discomfort. This is particularly beneficial in cases of vaginal dryness [85].
Mucoadhesion: Gums and mucilage can adhere to the mucosal surfaces of the vagina dueto their adhesive properties. This mucoadhesive effect prolongs the residence time of drugs or formulations on the vaginal mucosa, enhancing their therapeutic efficacy [86].
Protective Barrier: Gums and mucilage may form a protective barrier on the vaginal mucosa, protecting it from irritants, pathogens, and other external agents. This function helps maintain the integrity of the vaginal epithelium and reduces the risk of infections or inflammation [87,88].
1.11 MECHANISM OF BIOADHESION
The mucus is secreted by the goblet cells. It is a highly viscous liquid covering the internal tract of the body. Its role is to protect the mucosa against various aggressions. Its exact composition varies, depending on its source and location. However, its major components are mucin, electrolytes, lipids, enzymes, sloughed epithelial cells, bacterial products and water (95%) [89].
Mucin is a glycoprotein in which 160-200 oligo-saccharides side-chains of the glycosylated regions
represent 50-60% of its weight. The mucus gel structure results from the intermolecular association of glycoproteins (mucin) in a polymeric network. The polymer is probably a terminally linked chain with numerous cross-linkings. A large proportion of the glycop~tein is not incorporated in the network, but present as a soluble fraction, enhancing the viscosity of the interstitial fluid.
Besides its protective role against chemical (pH) or enzymatic aggression, the mucus constitutes a diffusion barrier for molecules, not only against drug absorption but also against bioadhesive polymer molecular chain interdiffusion. Diffusion through the mucus layer depends largely on the physico- chemical characteristics of the diffusive molecule: molecule charge, hydration radius, ability to form hydrogen bonds and molecular weight [90].
1. Topical Bioadhesive Drug Delivery Systems (DDS)
Topical DDS aim to enhance drug residence time on the skin or mucosal surfaces (buccal, nasal, ocular, vaginal). Natural polymers provide adhesion, controlled release, and biocompatibility.
Common Natural Bioadhesive Polymers Used
Topical DDS Types & Their Features
a) Bioadhesive Gels
b) Bioadhesive Creams and Ointments
c) Bioadhesive Patches/Films
d) Bioadhesive Nanoparticles
e) Wound Dressings/Hydrogels
2. Gastrointestinal (GI) Bioadhesive Drug Delivery Systems (DDS)
GI DDS use mucoadhesive materials to prolong drug residence time in stomach or intestines, enhance absorption, and target specific regions.
Natural Bioadhesive Polymers Used
GI DDS Types & Characteristics
a) Mucoadhesive Tablets
b) Mucoadhesive Microspheres/Nanospheres
c) Floating Bioadhesive Systems
d) Colon-Targeted Mucoadhesive Systems
e) In-situ Gelling Systems
f) Bioadhesive Films for GI Delivery
Five Drug Properties Important for Bioadhesive DDS
1. Drug Solubility
2. Molecular Weight
3. Partition Coefficient (Lipophilicity)
4. Stability at the Application Site
5. Dose Requirement
Effect of Polymer Properties on Mucoadhesive Drug Delivery Systems
The performance of any mucoadhesive drug delivery system depends strongly on the physicochemical properties of the polymer used. These properties influence adhesion strength, swelling, drug release, residence time, and overall therapeutic effect.
1. Molecular Weight of Polymer
Effect:
? Strong adhesion, ? sustained release, ? slower hydration.
2. Degree of Crosslinking
Effect:
? Controls drug release rate, ? affects adhesive strength, ? excessive crosslinking reduces mucoadhesion.
3. Polymer Charge (Ionic Character)
Effect:
? Strong bonds with mucin, ? pH-dependent adhesion.
4. Functional Groups
Presence of –COOH, –OH, –NH2 enhances adhesion.
Effect:
? Increases chemical bonding with mucosal surface.
5. Swelling Ability
Effect:
? Improves adhesion and drug release, ? excessive swelling reduces retention.
6. Polymer Concentration
Effect:
? Optimal concentration needed for balance between viscosity and adhesion.
7. Polymer Flexibility
Effect:
? Improved chain interpenetration → stronger adhesion.
8. Hydrophilicity
Effect:
? Facilitates hydration, swelling, and adhesion.
9. pH Sensitivity
Effect:
? Determines site-specific adhesion in GI tract.
1. Adsorption Theory
Adsorption theory states that bioadhesion occurs due to the formation of weak chemical bonds between the polymer and the biological surface after initial contact. These include:
Key point: Adhesion results from secondary chemical interactions between polymer chains and mucin.
2. Mechanical Theory
Mechanical theory explains that bioadhesion occurs when the polymer penetrates into surface irregularities or pores of the mucosal membrane.
After penetration, the polymer locks into the surface, creating mechanical interlocking.
Key point: Adhesion results from physical interlocking between polymer and mucosa.
3. Cohesive Theory
Cohesive theory states that the internal strength of the polymer itself plays a major role in adhesion.
If the polymer has strong cohesive forces (good viscoelasticity and chain entanglement), it maintains integrity and adheres better.
Key point: Adhesion depends on internal strength and chain entanglement of the polymer.
What kinds of bioadhesive formulations exist (or have existed) on the market or in clinical/research use
• Buccal Films / Tablets / Patches
• Microspheres / Nanoparticles / Particulate Systems with Mucoadhesive Polymers
TABLE 2: APPLICATIONS OF NATURAL POLYMERS IN DRUG DELIVERY [91,92]
|
Mucilage/ Gum |
Dosage form |
Disease/ Disorder |
Application |
|
Xanthine |
Pellets |
Kidney stone |
Controlled drug delivery |
|
Tamarind |
Hydrogel |
Dry eye, glaucoma |
Ocular mucoadhesive drug delivery |
|
Pectin |
Beads, floating beads |
Colon cancer, chron’s disease |
Collon drug delivery |
|
Luciana seed gum |
Tablet |
Constipation and diarrhea |
Emulsifying agent, suspending agent |
|
Agar |
Gelletin agent in suppository |
Diarrhea, Laxative, purgative |
Suspending agent, emulsifying agent |
|
Gum ghatti |
Tablets, Emulsion and suspension |
Constipation and diarrhea |
Binder, emulsifying and suspending agent |
|
Acacia |
Tablet |
Throat and stomach inflammation |
Binder |
|
Albizia |
Tablet |
Arthritis and Burn |
Binder |
|
Galan |
Hydrogel, beads |
Correct vision |
Opthalmic drug delivery system |
|
Isapgol |
Powder, tablet |
Diarrhea |
Colon drug delivery and gastroretentive drug delivery |
Evaluation Parameters for Mucoadhesive Dosage Forms
In?Vitro Evaluation Parameters
In?Vivo Evaluation Parameters
Different Dosage Forms for Bioadhesive Drug Delivery Systems
|
Sr. No. |
Polymer Used |
Model Drug |
Dosage Form |
Result |
Reference |
|
1 |
Carbopol 934 |
Metronidazole |
Buccal Gel |
Prolonged mucosal residence time |
Lachman et al., Theory & Practice of Industrial Pharmacy |
|
2 |
Chitosan |
Insulin |
Nasal Microspheres |
Enhanced bioavailability |
Ahuja et al., Int. J. Pharm. |
|
3 |
HPMC |
Propranolol HCl |
Buccal Tablet |
Sustained drug release |
Banker & Rhodes |
|
4 |
Sodium Alginate |
Diclofenac Sodium |
Mucoadhesive Gel |
Improved retention at site |
Remington |
|
5 |
Polycarbophil |
Lidocaine |
Buccal Patch |
Increased contact time |
Smart JD, J. Pharm. Pharmacol. |
|
6 |
Xanthan Gum |
Theophylline |
Mucoadhesive Tablet |
Controlled drug release |
USP Monograph |
|
7 |
Pectin |
Clotrimazole |
Vaginal Gel |
Improved therapeutic efficacy |
Martin’s Physical Pharmacy |
|
8 |
Guar Gum |
Atenolol |
Oral Bioadhesive Tablet |
Enhanced absorption |
Indian Journal of Pharmaceutical Sciences |
|
9 |
Gelatin |
Amoxicillin |
Microspheres |
Sustained drug delivery |
International Journal of Pharmaceutics |
|
10 |
Carbopol 971P |
Fluconazole |
Buccal Film |
Increased residence time |
European Journal of Pharmaceutical Sciences |
|
11 |
Chitosan–Alginate |
Insulin |
Nanoparticles |
Improved permeation |
Journal of Controlled Release |
|
12 |
HPMC–PVA |
Nicotine |
Buccal Patch |
Reduced dosing frequency |
Drug Development and Industrial Pharmacy |
|
13 |
Tragacanth Gum |
Metformin |
Mucoadhesive Tablet |
Prolonged drug release |
Asian Journal of Pharmaceutics |
|
14 |
Sodium CMC |
Ibuprofen |
Oral Gel |
Improved patient compliance |
Pharmaceutical Development and Technology |
|
15 |
Aloe Vera Gel |
Acyclovir |
Mucoadhesive Gel |
Enhanced healing and retention |
Herbal Drug Research Review |
CONCLUSION
Natural polymers, gums, and mucilages represent a versatile and promising class of bioadhesive components in drug delivery systems across various routes, including oral, nasal, transdermal, and ocular and vaginal applications. Their biocompatibility, biodegradability, and inherent adhesive properties make them ideal candidates for enhancing drug retention and absorption, ultimately improving therapeutic efficacy and patient compliance. As research continues to elucidate the mechanisms behind their bioadhesive behavior and optimize their formulation strategies, these natural materials are poised to play an increasingly vital role in pharmaceutical innovations.
Moreover, the shift towards sustainable and eco-friendly materials in drug delivery highlights the importance of leveraging these natural resources. The utilization of gums and mucilage as bioadhesive agents in the various route holds significant promise for enhancing drug delivery systems and improving patient healthcare, it is important to acknowledge the challenges associated with formulation development, including stability, consistency and scalability. These challenges necessitate ongoing research and optimization efforts to ensure the reliability and efficacy of different drug delivery systems containing gums and mucilage. Looking ahead continued research endeavours are expected to further refine the use of gums and mucilage in drug delivery. This includes exploring novel natural polymers, improving bioadhesive properties and advancing formulation technologies. ultimately, these efforts have the potential to enhance patient healthcare.
REFERENCES

Omkar Joshi, Dr. Kuldeep Ramteke, Dr. Sachin Bhalekar, Dr. Rahul Lokhande, Ganesh Lamkhade, Bioadhesive Properties of Natural Polymer in Drug Delivery: An Overview, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 958-985. https://doi.org/10.5281/zenodo.18509299
 10.5281/zenodo.18509299
10.5281/zenodo.18509299