
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Department of Pharmacology, Dr. Rajendra Gode Institute of Pharmacy.
Breast cancer is the most frequently diagnosed cancer among women globally and poses a significant public health issue due to its elevated incidence and mortality rates. This disease is heterogeneous, categorized into various molecular subtypes such as hormone receptor-positive, HER2-positive, and triple-negative breast cancer (TNBC), each exhibiting distinct biological characteristics and clinical outcomes. The identification of biomarkers such as the estrogen receptor (ER), progesterone receptor (PR), and HER2 has significantly improved diagnostic precision and facilitated the development of targeted treatments. Progress in diagnostic methods, including imaging techniques such as mammography, ultrasound, and MRI, along with histopathological and molecular evaluations, has improved early detection and precise tumor classification. Treatment approaches for breast cancer are increasingly informed by tumor biology and individual patient factors, incorporating surgical procedures, radiotherapy, chemotherapy, hormonal treatments, and targeted biological therapies. The rise of personalized medicine has resulted in better therapeutic effectiveness and minimized treatment-related side effects. Nevertheless, challenges persist in managing aggressive subtypes like TNBC and in overcoming treatment resistance. This review offers a comprehensive overview of breast cancer classifications, biomarkers, diagnostic innovations, and current treatment strategies. A thorough understanding of these elements is crucial for enhancing patient outcomes and directing future research in precision oncology and personalized care.
With an estimated 1,152,161 new cases annually, breast cancer is the second most frequent cancer worldwide and the most common kind among women.[8] In Asia, breast cancer affects one out of every 35 women. Women are more likely than males to get breast cancer, with women accounting for 99% of cases and men for 2.5–1%. Nearly 40,000 people lose their lives to breast cancer each year, and over 2,30,000 receive a diagnosis. It is the second greatest cause of cancer-related mortality and the most often diagnosed malignancy in women.[1] The hallmark of breast cancer is aberrant cell proliferation that spirals out of control and develops into a tumour. According to the World Health Organization, in 2022, breast cancer was identified in 2.3 million women around the globe, which led to 670,000 deaths. Estimates worldwide highlight considerable inequalities in the burden of breast cancer, influenced by human development factors. For instance, in countries with a very high Human Development Index (HDI), the probability of a woman being diagnosed with breast cancer in her lifetime is 1 in 12, with a mortality rate of 1 in 71. In contrast, in nations with a low HDI, the diagnosis rate is 1 in 27, but the death rate is higher, with 1 in 48 women dying from the disease. In 2022, the highest number of breast cancer cases was reported in China, the United States, and India, which also accounted for a significant number of breast cancer-related deaths. Breast cancer is typically detected via mammography and later verified through tissue sampling. Following this diagnosis, patients receive targeted therapies based on their specific type of breast cancer, which is primarily categorized by the presence or absence of Estrogen Receptors (ER), Progesterone Receptors (PR), and Human Epidermal Growth Factor Receptor 2 (HER-2). Research has indicated that within these subgroups, there are unique mutations that can aid in evaluating disease severity, predicting treatment responses, and facilitating rapid and minimally invasive monitoring of therapy, Notable mutations include those in PIK3CA, ESR1, TP53, MAP3K1, GATA3, RPTOR, ERBB2, and ERBB3.[1] The existing strategy for managing breast cancer prioritizes early detection and treatment. In the United States, this approach results in an impressive 85% survival rate over a decade. The stage at which the cancer is diagnosed plays a critical role in survival outcomes; for instance, patients diagnosed at stage 0 have a ten-year survival rate of 98%, compared to just 65% for those diagnosed with stage III disease. To enhance survival rates, it is vital to identify more patients at earlier stages of the disease. As a result, we have examined both current and emerging technologies for breast cancer screening and detection to uncover areas for potential improvement. This paper begins with a discussion of commonly used breast cancer detection methods and subsequently explores treatment strategies.[8]In 2023, breast cancer was projected to be the most commonly diagnosed cancer among both men and women, ranking as the second deadliest cancer globally. In the United States alone, there were an estimated 300,560 new cases and 43,700 fatalities. The subtype characterized by overexpression of the human epidermal growth factor 2 (Her2) represents 15-20% of all breast cancer diagnoses.[42]
Breast cancer is defined by the unregulated proliferation of atypical cells within the breast.Although it can affect both genders, women are at a higher risk due to their breast development and continuous exposure to estrogens. These abnormal cells can develop into tumors, and breast cancer is defined by the dissemination of these tumors. Generally, there is a prolonged period between alterations in breast tissue and the emergence of breast cancer. The process of breast cancer development includes the function of DNA. It is pivotal in the onset of all cancers, including breast cancer. Breast cells, similar to all other cells in the body, possess DNA that governs cell growth and division. When a cell divides, its DNA is accurately copied; however, errors can occasionally occur, leading to genetic changes referred to as "mutations." These mutations may be inherited by other cells, resulting in abnormal growth. Over time, the accumulation of mutations can lead to the development of a malignant breast tumor. The risk of mutations increases with the frequency of cell division.According to molecular and histological evidence, breast cancer (BC) can be classified into three distinct categories: those that express hormone receptors (either estrogen receptor positive (ER+) or progesterone receptor positive (PR+)), those that express the human epidermal growth factor receptor 2 (HER2+), and triple-negative breast cancer (TNBC), which is characterized by the absence of estrogen receptors (ER−), progesterone receptors (PR−), and HER2 (HER2−) .Moreover, TNBC is subdivided into six categories: Basal-Like 1 (BL-1), Basal-Like 2 (BL-2), Immunomodulatory (IM), Mesenchymal (M), Mesenchymal Stem Cell-Like (MSL), and Luminal Androgen Receptor (LAR) [2]. The specific mechanisms that lead to the onset of breast cancer are not well understood .The hormone receptor-positive breast cancer (HR-positive BC) is the most common form of breast cancer, accounting for 60–70% of cases in developed nations, particularly among premenopausal women. Consequently, hormone therapy is the predominant treatment method utilized. Key medications in this category include tamoxifen, which serves as an estrogen blocker, and aromatase inhibitors like Letrozole, Anastrozole and Exemestane, which prevent the ovaries from producing hormones.[3]
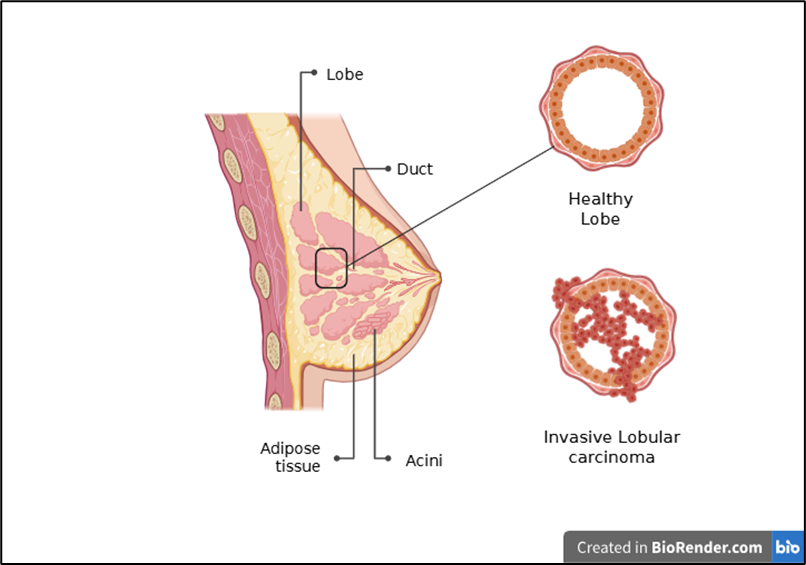
Figure 1: Comparison of Normal cell and Invasive carcinoma
2.Biomarkers:
2.1. Presence and number of axillary node metastases:
The degree of axillary node indolent is not a determining factor for disease outcomes. A report revealed that 30% of untreated breast cancer patients without nodal metastasis progressed to a metastatic or recurrent form of the disease after ten years, while nearly 50% of patients with nodal involvement were successfully cured through local treatment .[2]
2.2. Tumor size and Tumor grade :
This method is commonly employed however, tumor grading is not without its limitations, including issues reproducibility and differing interpretation among pathologist. Furthermore, tumor heterogeneity remains a critical concern, as the majority of tumors are classified as grade two.[2,4] In recent years , a significant amount of research has been directed towards the identification and validation of molecular biomarkers intended for prognostic and predictive purposes. some of the validated tests are Oncotype DX, Mammaprint and uPA /PAI -1 .[5]
2.3. MammaPrint :
This validated molecular test utilizes microarray technology to analyze the expression of 70 genes that play a crucial role in cancer regulatory pathways. Patients are classified into two categories—low risk and high risk for cancer recurrence—based on the relative expression of these genes. The MammaPrint test has undergone validation and is widely recognized for its ability to predict cancer recurrence, serving as a vital marker for treatment strategies.[2,6]
2.4. uPA and PAI-1 markers :
This analysis focuses on evaluating the specified markers at the protein level in extracts obtained from breast cancer tissue. It has been observed that patients with higher concentrations of these proteins generally face more unfavorable outcomes than those with lower concentrations.[2]
2.6. IHC4 :
It is Immunohistochemical biomarker which is consists of ER, PR, HER2, and Ki67 markers and serves as an inexpensive prognostic test for patients with breast cancer .The evaluation of the biomarkers listed requires tumor tissue; however, due to the limitations of obtaining such tissue, it is advisable to focus on strong and clinically validated circulating biomarkers. The most significant predictive biomarker currently available for breast cancer is the Estrogen Receptor (ER) marker. It is crucial for all newly diagnosed breast cancer patients to undergo ER evaluation. While the ER can serve as both a prognostic and predictive biomarker for therapy. The basis for evaluating Progesterone (PR) alongside estrogen receptor (ER) lies in the ability of estrogen to induce PR. Additionally, the presence of PR is interpreted as a sign of an active ER. [2,7]
2.7.HER 2 : It is crucial to evaluate another predictive biomarker alongside estrogen receptor (ER) status in all patients who have recently been diagnosed. High HER2 expression, driven by the activation of signaling pathways such as PI3K/AKT and MAPK, along with changes in cell membrane integrity, facilitates the metastasis, invasion, and growth of cancer cells. Furthermore, the presence of mi-RNAs, circulating tumor DNA (ctDNA), and circulating tumor cells (CTCs) has been documented.[2]
2.8. Other: Recently, a growing number of researchers have been engaged in the study of circulating tumor cells (CTCs), microRNAs (miRNAs), and DNA mutation testing, including the evaluation of circulating tumor DNA (ctDNA), to discover new prognostic and predictive markers. It is imperative that these novel biomarkers undergo rigorous clinical and analytical validation before they can be applied in clinical practice. This validation is crucial for paving the way toward personalized treatment for patients with early-stage breast cancer, requiring the combination of established prognostic biomarkers with validated prognostic and predictive factors.[2]
3. Commonly Used Cancer Detection Technique:
Breast Self-Examinations (BSE), Clinical Breast Examinations (CBE), and Mammography are critical techniques for the detection of breast cancer. CBE demonstrates a sensitivity of 57.14% and a specificity of 97.11%. [9] Although it does not yield a conclusive diagnosis of cancer, it is proficient in identifying suspicious breast abnormalities.[8] Research by Kosters and Gotzsche indicated that there was no notable reduction in breast cancer mortality rates among individuals who underwent BSE and CBE when compared to those who did not participate in screening, even though the screened population experienced twice the number of biopsies. Nevertheless, proponents of CBE and BSE argue for their continued application, particularly for women under 40 and those who lack regular access to mammography.[8]
Imaging Technique:
Mammography, commonly known as the gold standard in breast imaging, is the most widely used method for this purpose. This involves performing an X-ray examination of the breast as it is being compressed. The true-positive detection rate for mammography ranges from 83% to 95%, while the false-positive rate is between 0.9% and 6.5%. The application of imaging techniques provides clear insights into the morphology and location of tumor tissues, offering valuable clinical information for healthcare professionals. However, the use of contrast agents and high-energy radiation in these imaging methods can pose risks to patients. Consequently, it is essential to evaluate these imaging techniques and select the most suitable diagnostic approach for breast cancer (BC) patients. The primary imaging modalities include mammography (MG), ultrasonography (US), magnetic resonance imaging (MRI), positron emission tomography (PET), computed tomography (CT), and single-photon emission computed tomography (SPECT). While PET, CT, and SPECT are not typically recommended for diagnosing BC, they may serve as supplementary diagnostic tools in specific scenarios, such as assessing metastatic BC or identifying bone and lymphatic metastases. Therefore, we will focus on MG, US, and MRI as the preferred screening methods for breast cancer.[8,10]
3.1. Mammography:
Mammography exhibits reduced sensitivity in women who have radiographically dense breast tissue. This imaging technique has specific constraints; it necessitates specialized equipment, radiographic film, and developing chemicals, along with the expertise of a trained X-ray technologist and a radiologist to interpret the results. Additionally, the procedure involves exposing the breast to radiation, which raises concerns regarding the potential risk of radiation-induced cancer.[8]
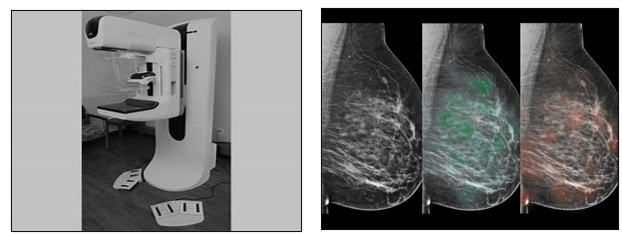
Figure 2: Digital Tomosynthesis Mammograph and Digital Mammogram of Patient
Advance Application of Digital Mammography [8,15,16]
3.2. Nuclear Medicine [8,12,17]
Nuclear medicine methods produce functional images that are derived from molecular characteristics. They do not show negative effects associated with breast density. Furthermore, these methods necessitate minimal or no compression of the breast. Although nuclear medicine techniques are costly and involve radiation exposure for the patient, they hold significant potential for cancer detection, particularly in individuals at high risk
3.2.1. Radioimmunoscintigraphy
In radioimmunoscintigraphy (RIS), a radiopharmaceutical agent is administered to target tumour-associated antigens. The identification process relies on the variations in antigen expression between normal and cancerous cells. This technique focuses on several antigens, such as carcinoembryonic antigen, polymorphic breast epithelial mucin antigen, and TAG72 antigen. Additionally, RIS can be utilized for receptor imaging, particularly involving somatostatin receptors. The process may additionally include perfusion agents such as thallium-201, 99mTc-sestamibi, 99mTc-tetrofosmin, 99mTc-methylene diphosphonate, and 99mTc-diethylene triamine penta-acetic acid. However, RIS is characterized by high costs and moderate sensitivity and specificity rates, which suggests it is not an ideal method for screening purposes.
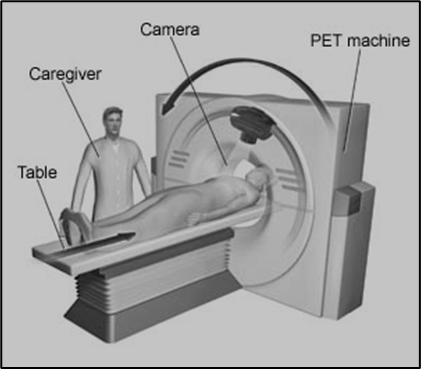
3.2.2. Positron Emission Tomography
Positron emission tomography (PET), generally using 18F-fluorodeoxyglucose (18F-FDG or FDG), takes advantage of glucose metabolism to facilitate the detection of cancer. This radiotracer is characterized by a high lesion-to-background ratio. FDG-PET has a proven history of effectively identifying malignancies, particularly metastatic diseases in solid organ tumors. Additionally, another radiotracer, 18F-fluoro-L-thymidine (FLT), is employed to assess thymidine kinase-1 activity, which correlates with S-phase DNA synthesis. The uptake of FLT is less affected by inflammation resulting from needle biopsies, offering a significant advantage in such contexts. Imaging typically takes place 40 to 60 minutes post-injection. However, research by Boerner et al. Indicates that extending the waiting period enhances the detection rate. Additionally, it has been demonstrated that performing PET imaging in a prone position, utilizing a breast positioning device, significantly boosts the cancer detection rate of this modality .However, PET faces challenges in identifying small primary cancers , which limits its potential as an effective screening tool.
Advanced application of Nuclear Medicine [8]
3.3. Ultrasonography:
Ultrasonography (US) is utilized to examine the morphology and variations in tumor tissues, allowing for precise localization of lesions. This imaging technique is non-invasive and safe for all individuals. The advancement of three-dimensional US technology has enabled detailed imaging of tumor structures and vascular distribution, which is particularly beneficial during patient diagnosis. Among the various forms of three-dimensional US, color Doppler ultrasound stands out as it effectively illustrates tumor conditions and blood flow dynamics, thereby equipping physicians with critical clinical insights that help in identifying the differences between benign and malignant tumors . Mammography is the preferred technique for identifying calcifications in breast cancer, it often struggles to detect very small calcifications through either mammography or standard ultrasound. To address this challenge, a novel ultrasound image-processing technique known as MicroPure has been introduced. This innovative method minimizes speckle by examining spatial features and frequency in images, resulting in high-contrast resolution and improved tissue uniformity. Ultrasound offers numerous benefits, including the use of minimal contrast agents, the absence of high-energy radiation, and its applicability across all age groups. Additionally, when mammography is not feasible, ultrasound serves as a viable alternative for breast cancer diagnosis. Nevertheless, ultrasound does have its drawbacks, including the necessity for skilled operation and lower definition and resolution compared to computed tomography. [18]
Advanced application of ultrasound: [8]
3.4. Magnetic Resonance
Imaging:
Magnetic Resonance Imaging (MRI) facilitates the early identification of familial breast cancer (BC) across all age groups, irrespective of breast density or individual risk factors. The water dispersion coefficient varies among different tissues, and magnetic resonance diffusion-weighted imaging (MRDW) is a technique that effectively illustrates the movement of water molecules within the body. As a result, MRDW has emerged as a valuable diagnostic tool for breast cancer patients. A review of existing literature indicates that malignant tumors exhibit distinct water diffusion-limited effects when compared to benign tumors, enabling researchers to differentiate between the two by measuring the apparent diffusion coefficient (ADC) values, which reflect these diffusion-limited effects (with ADC values ranking as follows: normal breast group > benign group > malignant group) Dynamic contrast-enhanced MRI (DCE-MRI) offers superior soft tissue resolution compared to MRDW, allowing for a clearer visualization of the morphological and hemodynamic characteristics of lesions in vivo. Additionally, magnetic resonance spectroscopy (MRS) serves as a non-invasive technique that enhances the diagnostic accuracy for breast cancer by assessing the risk associated with the disease and informing treatment strategies. Magnetic resonance elastography (MRE) is a specialized magnetic resonance technique that assesses tissue elasticity through the propagation of mechanical waves within the tissues. The combination of positron emission tomography (PET) with MRI, known as PET/MRI, offers detailed visualization of soft tissue structures in the breast and chest wall. PET provides valuable molecular-level insights in vivo, and the integration of PET with MRI enhances the positive predictive value for patients, proving to be particularly beneficial in the assessment of breast cancer metastasis. Magnetic resonance imaging serves as a supportive diagnostic tool with numerous advantages in identifying breast cancer.Despite its benefits, the widespread use of MRI is hindered by several factors, including prolonged imaging durations, high costs, and limitations related to the presence of metal implants in a patient's body. [18]
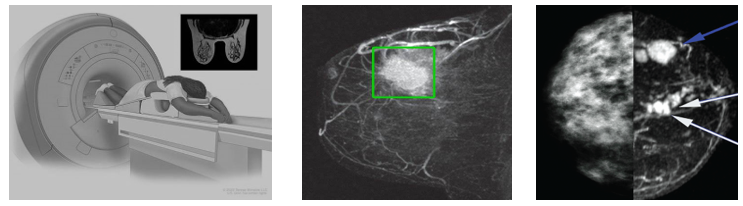
Figure 4: Detection of Breast Cancer Through MRI
Advanced application of MRI [8]
Molecular Biotechnology Examination:
Molecular biotechnology assessments can detect breast cancer earlier than imaging methods; however, they do not serve as a substitute for these imaging techniques and should be considered supplementary methods for breast cancer diagnosis. Their aim is to analyze specific biomarkers, including nucleic acids, proteins, cells, and tissues from patients. [18] These assessments provide physicians with valuable clinical information at the molecular level and encompass the following techniques;
Nucleic Acid Hybridization Technique:
Nucleic acid hybridization methods primarily encompass fluorescence in situ hybridization (FISH) and aptamer probe hybridization (APH). These techniques are instrumental in identifying specific fragments of tumor biomarkers and in the discovery of new tumor biomarkers during breast cancer (BC) diagnosis. FISH has significantly advanced the field of molecular biology diagnostics, operating on the principle of base pairing. Research indicates that approximately 25-30 percent of all breast cancers are positive for the human epidermal growth factor receptor 2 (HER-2). FISH demonstrates high efficacy in amplifying the HER-2 gene and reveals a substantial number of HER-2 copies per cell. The detection of HER-2 through FISH is crucial in determining the necessity of the medication Herceptin for BC patients. Furthermore, FISH is regarded as the 'gold standard' for assessing the activation of the HER-2 gene, and it offers additional benefits such as reproducibility, stability, and high sensitivity. However, these factors hinder its promotion, particularly due to the necessity for intricate probe designs and specialized fluorescence detectors. [18]
Some other techniques in the diagnosis of breast cancer [18]
• Gene chip and next generation sequencing
• Real-time fluorescence quantitative PCR system
• Protein hybridization system
• Immunochemistry
• Western blot
• Flow cytometer
• Puncture biopsy system
4. Risk Factors:
Risk factors include following two types:
4.1. Non-Modifiable Factors:
1) Sex/gender
The female sex is a significant factor contributing to a heightened risk of breast cancer, primarily due to increased hormonal stimulation. In contrast to men, who have minimal estrogen levels, women possess breast cells that are particularly susceptible to hormones, especially estrogen and progesterone, as well as any imbalances in their levels. Variations in the physiological levels of endogenous sex hormones lead to an increased risk of breast cancer among both premenopausal and postmenopausal women. Although less than 1% of all breast cancer cases occur in men, when diagnosed, male breast cancer is often at a more advanced stage compared to that in women, with the average age of diagnosis being approximately 67.Key risk factors for men include older age, mutations in BRCA2/BRCA1, elevated estrogen levels, Klinefelter syndrome, a family history of breast cancer, and exposure to radiation. [19,20 ,21]
2) Older Age
Currently, around 80% of individuals diagnosed with breast cancer are aged 50 and above, with over 40% being older than 65 years. The probability of developing breast cancer increases as one ages , showing a 1.5% risk at 40 years, 3% at 50 years, and exceeding 4% at 70 years. The triple-negative subtype of breast cancer is predominantly identified in individuals under 40, whereas theb luminal A subtype is more prevalent in patients over 70. [19 ,22]
3) Family History
A familial history of breast cancer is a significant factor that correlates with an elevated risk of developing the disease. Research indicates that around 13–19% of individuals diagnosed with breast cancer have family history of this illness. Regardless of age, the occurrence of breast cancer is significantly greater in individuals who have a family history of the disease. Additionally, a family history of ovarian cancer, particularly those associated with BRCA1 and BRCA2 gene mutations, may further heighten the risk of breast cancer.The risk appears to escalate further if the relatives diagnosed are under the age of 50. [23 , 24]
4) Genetic Mutations
Numerous genetic mutations have been identified as significantly correlated with a heightened risk of developing breast cancer. The two main genes recognized for their significant penetrance are BRCA1, found on chromosome 17, and BRCA2, which is positioned on chromosome 13. These genes are predominantly associated with an elevated likelihood of breast carcinogenesis. The mutations found in these genes are typically inherited in an autosomal dominant fashion, although sporadic mutations are frequently observed as well. Additionally, other breast cancer genes with high penetrance include TP53, CDH1, PTEN, and STK11. In addition to the increased risk of breast cancer, individuals carrying these mutations also face a greater vulnerability to ovarian cancer.[25,26]
5) Reproductive History
Extensive research has established a significant correlation between the levels of endogenous hormones, particularly estrogen and progesterone, and an elevated risk of breast cancer in women. Consequently, factors such as pregnancy, lactation, the onset of menstruation, and menopause, along with their respective durations and any associated hormonal fluctuations, play a vital role in potentially triggering carcinogenic processes within the breast microenvironment. Furthermore, women who have experienced preeclampsia during pregnancy or have children born from a preeclamptic pregnancy exhibit a reduced likelihood of developing breast cancer. To date, no link has been identified between an increased risk of breast cancer and the occurrence of abortion.Prolonged breastfeeding has been shown to decrease the likelihood of developing both ER/PR-positive and -negative breast cancers. Additionally, an early onset of menarche is identified as a risk factor for breast cancer, potentially correlating with tumor grade and lymph node involvement. Furthermore, an earlier age at which menstruation begins may lead to a less favorable prognosis. In contrast, experiencing early menopause, whether through natural means or surgical intervention, is associated with a reduced risk of breast cancer. [19]
6) Density of Breast Tissue
Breast tissue density varies throughout a woman's life, with established classifications such as low-density, high-density, and fatty breasts in clinical settings. Typically, higher breast density is found in younger women with a lower body mass index (BMI), particularly those who are pregnant, breastfeeding, or undergoing hormonal replacement therapy.Research indicates that increased breast tissue density is associated with a heightened risk of breast cancer, a pattern evident in both premenopausal and postmenopausal women. Consequently, it has been suggested that assessing breast tissue density may serve as a promising, non-invasive, and efficient approach for monitoring women who are at an elevated risk of developing cancer.[27,28]
7) Previous Radiation Therapy
The likelihood of developing secondary malignancies following radiotherapy is a personalized issue that varies based on the characteristics of the patient, despite being a relatively common occurrence that raises significant clinical concerns. The incidence of cancer resulting from radiation therapy is closely linked to the age of the individual; those who undergo radiation treatment before the age of 30 face an increased risk of developing breast cancer. The choice of an appropriate radiotherapy technique is vital in mitigating the risk of secondary cancers. Furthermore, a family history of breast cancer in patients undergoing radiotherapy further elevates the likelihood of cancer development. Nevertheless, research by Bartelink et al. indicates that administering an additional [16 Gy] of radiation to the tumor bed, in conjunction with standard radiotherapy, may reduce the risk of local recurrence. [19,29]
4.2. Modifiable Factors
1)Chosen Drugs
Research indicates that the consumption of diethylstilbestrol during pregnancy may be linked to an increased risk of breast cancer in mother and children although this studies needs futher evaluation . The likelihood of developing breast cancer rising with age; women aged 40 and above are approximately 1.9 times more likely to be affected compared to those under 40.Furthermore, the risk of breast cancer escalates with higher doses of diethylstilbestrol.In terms of hormonal replacement therapy, numerous studies suggest that Women who engage in hormone replacement therapy (HRT) for prolonged durations, especially those exceeding 5 to 7 years, encounter a heightened risk of developing breast cancer. Additionally, the use of certain antidepressants, particularly paroxetine, tricyclic antidepressants, and selective serotonin reuptake inhibitors, has been associated with a higher risk of breast cancer. Research has indicated that the risk of breast cancer is particularly elevated with the use of tetracyclines. Efforts to explore a potential connection between antihypertensive medications, non-steroidal anti-inflammatory drugs, and statins with an increased risk of breast cancer have been made, yet the data remains largely inconsistent. [19,30,31]
2)Physical Activity and body mass index
Engaging in regular physical activity is regarded as a protective factor against the incidence of breast cancer. Research conducted by Chen et al. indicated that among women with a familial history of breast cancer, physical activity was linked to a decreased risk of developing the disease, although this association was confined to the postmenopausal phase.[19,32] It is suggested that physical activity may mitigate cancer risk by lowering exposure to endogenous sex hormones, modifying immune responses, or influencing levels of insulin-like growth factor-1.[19,33]Furthermore, epidemiological studies have established a correlation between obesity and an increased likelihood of breast cancer, particularly pronounced in obese postmenopausal women who are more likely to develop estrogen-receptor-positive breast cancer.[34] Wang et al. found that women over the age of 50 with a higher Body Mass Index (BMI) face a greater risk of cancer compared to those with a lower BMI. The accumulation of body fat may exacerbate inflammatory conditions and alter circulating hormone levels, thereby promoting pro-carcinogenic processes. Consequently, women with a BMI of 25 kg/m2 or higher tend to experience poorer clinical outcomes.[19,35]
3)Alcohol Intake and Smoking
Extensive research indicates that high levels of alcohol consumption are associated with an increased risk of cancers in the gastrointestinal tract, and it has also been established that it correlates with a heightened risk of breast cancer. The type of alcohol consumed is less significant than the overall alcohol content in beverages when considering cancer risk. Furthermore, alcohol intake is often linked to weight gain and elevated body mass index (BMI), which further exacerbates this risk.Studies have shown that alcohol consumption particularly raises the risk of estrogen-positive breast cancers. Regarding smoking, the carcinogens present in tobacco are transported to breast tissue, which increases the likelihood of mutations in oncogenes and tumor suppressor genes, particularly p53. Consequently, both active and passive smoking play a significant role in promoting pro-carcinogenic processes.[19]
4) Exposure to Artificial Light and chemicals:
Recent studies have established a connection between artificial light at night (ALAN) and an elevated risk of breast cancer. Research indicates that individuals exposed to higher levels of ALAN face a significantly increased risk of developing breast cancer compared to those with reduced exposure. Numerous chemicals have been identified as potential contributors to breast carcinogenesis, with dichlorodiphenyltrichloroethane (DDT) and polychlorinated biphenyl (PCB) being the most extensively studied due to their early exposure effects on mammary gland development. Additionally, a possible correlation has been noted with increased exposure to polycyclic aromatic hydrocarbons (PAH), synthetic fibers, organic solvents, oil mist, and insecticides.[19,36,37]
5) Intake of Processed Food/Diet
The World Health Organization (WHO) has classified highly processed meats as a Group 1 carcinogen, indicating that their consumption may elevate the risk of various cancers, including gastrointestinal and breast cancer. Additionally, similar findings have been noted regarding the excessive consumption of saturated fats. Ultra-processed foods, which are typically high in sodium, fat, and sugar, contribute to obesity, a recognized risk factor for breast cancer. Research suggests that a rise in the consumption of ultra-processed foods is associated with an elevated risk of breast cancer. Conversely, a diet rich in n-3 polyunsaturated fatty acids (PUFA), vitamin D, fiber, folate, and phytoestrogens may offer protective benefits against breast cancer .[19,38]
6) Other Drugs
Additional medications that may pose potential risk factors for breast cancer encompass antibiotics, antidepressants, statins, antihypertensive agents such as calcium channel blockers and angiotensin II-converting enzyme inhibitors, along with nonsteroidal anti-inflammatory drugs (NSAIDs) like aspirin and ibuprofen.[19]
5. Types Of Breast Cancer:
Breast cancer encompasses a variety of diseases, which can be classified as either invasive or non-invasive. Invasive breast cancer occurs when cancer cells have spread outside the ducts or lobules into the adjacent tissues, whereas non-invasive breast cancer, also referred to as in situ, indicates that the cancer cells have not yet invaded surrounding tissues. Non-invasive breast cancer signifies an initial phase of the illness, remaining localized within the ducts or lobules of the breast. The predominant form of non-invasive breast cancer is ductal carcinoma in situ (DCIS), which, if not treated, has the potential to progress to an invasive form. Another prevalent type of non-invasive breast cancer is lobular carcinoma in situ (LCIS), which is not classified as cancerous and does not spread; however, its presence is associated with a heightened risk of developing cancer in the future.
Breast cancers are generally categorized into seven distinct subtypes:
Luminal A (ER positive and histologic low grade) , Luminal B (ER positive and histologic high grade), HER2 overexpressing, Basal-like (2 types – BL1 and BL2), Immunomodulatory (IM), mesenchymal (M), mesenchymal stem-like (MSL) and Normal Breast-like tumours. Invasive ductal carcinoma, Triple negative breast cancer and invasive Lobular carcinoma are most common breast cancer While Inflammatory breast cancer , Paget’s disease of the breast ,Phyllodes tumors , Angiosarcoma of the breast are the least common breast cancer. Breast cancer is identified by the presence of estrogen or progesterone hormone receptors (HR) along with HER2 proteins. Tumors that are positive for estrogen (ER+) and/or progesterone (PR+) receptors are driven to proliferate by the interaction of these hormones with their respective receptors. In contrast, HER2-positive breast cancers exhibit elevated levels of the HER2 protein, which accelerates tumor development. Approximately 80% of breast cancers are classified as estrogen receptor-positive. When a breast cancer is identified as positive for estrogen, progesterone, or HER2 receptors, it indicates that treatment options targeting these hormones and proteins are available to help inhibit tumor growth.
According to the SEER database from the National Cancer Institute, these elements indicate to doctors the level of aggressiveness of the cancer and how it might react to various treatment methods:
Doctors test the cancer cells to determine their subtype. The four main breast cancer subtypes are :
HER2-enriched (HR-/HER2+), This does not indicate the presence of HR, but it does indicate HER2 expression. During the early 2000s, advancements in high-throughput technology facilitated the analysis of gene expression for thousands of genes within a single experiment. This progress revealed that breast cancer consists of a minimum of four distinct molecular diseases, each characterized by unique features, clinical behaviors, and responses to treatment. The intrinsic molecular subtypes identified include basal-like, human epidermal growth factor receptor 2 (HER2) –enriched, as well as luminal A and B subtypes.[41]
Luminal A (HR+/HER2-) is the most common subtype of breast cancer, accounting for about 68% of all cases, according to the SEER database of the National Cancer Institute. In comparison to other subtypes, luminal A is characterized by a slower growth rate, reduced aggressiveness, and generally more favourable prognoses.[42]
Following are the Symptoms of luminal A breast:
Luminal type A breast cancer demonstrates a more favorable prognosis compared to other subtypes. Oncologists characterize luminal A by specific criteria: estrogen receptor (ER) levels exceeding 1%, progesterone receptor (PR) levels at or above 20%, negative human epidermal growth factor receptor-2 (HER2) status, and a Ki-67 index of less than 14% in clinical cases.[39] This subtype is distinguished by its elevated hormone receptor expression, absence of HER2 expression, and a low proliferation rate, all of which contribute to its improved prognosis.[40] Treatment options for breast cancer typically encompass drug therapy, radiotherapy, and surgical intervention. In the context of luminal type A, endocrine therapy is frequently the preferred approach. Nonetheless, there is ongoing debate regarding the inclusion of chemotherapy for patients with lymph node-positive luminal A breast cancer, as lymph node positivity is considered a high-risk factor. Some patients with positive luminal type A lymph nodes may derive benefits from chemotherapy,while other research has not demonstrated significant advantages from chemotherapy in this group. Even among those with positive lymph nodes, chemotherapy has not consistently shown to enhance prognosis. Consequently, the clinical relevance of chemotherapy for luminal A type, particularly in patients with positive lymph nodes, remains an open question.[39]
5.2. Luminal B Type:
According to the full report of Cleveland clinic.org.;Luminal B breast cancer represents a subtype of hormone receptor-positive (HR+) breast cancer. This type of cancer is characterized by the presence of specific proteins, known as receptors, within the cancer cells that promote growth in response to the hormone estrogen. The term 'luminal' refers to the cells found in the inner lining of the breast ducts.[43] Luminal B cancer cells are identified by the positive presence of estrogen receptor (ER) proteins, indicating their responsiveness to estrogen. In contrast, these cells are negative for progesterone receptor (PR) proteins, which distinguishes them from luminal A cells that typically express these receptors. Additionally, luminal B cells may exhibit variability in the presence of human epidermal growth factor receptor 2 (HER2), being classified as either HER2-positive or HER2-negative; this receptor is crucial for normal cell growth, but its overproduction can occur in certain breast cancer types. Furthermore, luminal B cancers are marked by a high level of Ki-67, a protein associated with rapid cell division, contributing to their generally faster growth rate compared to luminal A cancers. Lastly, luminal B cancers tend to be of a higher grade, indicating they are larger, more aggressive, and have a greater likelihood of recurrence than their luminal A counterparts. Luminal B breast cancer accounts for approximately 15% to 20% of all breast cancer diagnoses, making it less prevalent than luminal A breast cancer. Healthcare professionals typically identify luminal B breast cancer during onset of symptoms. Common indicators include a firm, rubbery lump in the breast screenings conducted prior to the that is not easily movable, discomfort in one or both breasts, discharge from the nipple, changes in the skin such as dimpling, thickening, or discoloration, and swelling in the area beneath the arm. Luminal B breast cancer occurs when normal breast cells undergo changes that lead to uncontrolled growth, although the precise reasons for this transformation remain unclear to researchers. The cells classified as Luminal B possess proteins that promote cancer proliferation upon the binding of estrogen. Consequently, individuals who began menstruating at an early age, experienced menopause later than usual, or have undergone hormone replacement therapy may face a slightly elevated risk of developing Luminal B breast cancer. Additional risk factors include a family history of breast or ovarian cancer, being over the age of 50, possessing dense breast tissue, carrying specific genetic mutations, and having previously received radiation therapy targeting the chest or breast area.[43]
5.3. Novel Her 2 Types of Breast Cancer:
HER-2 belongs to the HER family, which consists of four transmembrane tyrosine kinase receptors . The activation of HER-2 triggers intracellular pathways that promote cell growth, resulting in excessive cell proliferation and the avoidance of programmed cell death. Its overexpression was identified in certain breast and ovarian cancer patients in the late 1980s,prompting the urgent pursuit of targeted therapies. This effort culminated in the development of trastuzumab in the early 1990s, which received approval in 1998 for the treatment of metastatic breast cancer characterized by HER-2 overexpression.[43]HER-2, along with HER-1 (epidermal growth factor receptor), HER-3, and HER-4, forms a group of tyrosine kinase receptors that, upon ligand binding, undergo heterodimerization and stabilize in the cell membrane. This process activates critical intracellular signaling pathways, including the mitogen-activated protein kinase (MAPK) pathway, phosphatidylinositol 3-kinase (PI3K), AKT, and the mammalian target of rapamycin (mTOR), all of which are vital for cell division and growth, thereby contributing to cancer progression.[43] The HER-2 receptor, which is encoded by the HER-2 oncogene (also referred to as neu or c-erbB-2), has been identified as being overexpressed in numerous solid tumors, including those of the breast, lung, colorectal, and gastric regions.[44] This overexpression, along with its abnormal activation independent of ligands in cancer cells, contributes to unchecked cell proliferation, the ability to evade programmed cell death, and an increased potential for metastasis, thereby exemplifying four of the fourteen recognized hallmarks of cancer. The HER2 receptor is a transmembrane glycoprotein made up of 1255 amino acids and has a weight of 185 kD, found on the long arm of human chromosome 17. It is present in various tissues, where its primary function is to promote excessive and uncontrolled cellular growth, leading to tumor development.[43] The amplification or overexpression of the HER2 gene is observed in roughly 15–30% of breast cancer cases.[45] As our comprehension of HER2 biology has advanced, it has become evident that HER2 overexpression is also present in various other cancer types, including those of the stomach, ovary, uterine serous endometrial carcinoma, colon, bladder, lung, uterine cervix, head and neck, and esophagus.[46] In addition to its role in the advancement of various cancers, HER2 has been thoroughly investigated as a possible therapeutic target. [45] For patients with breast cancer (BC) who exhibit HER2 expression, there are various anti-HER2 monoclonal antibodies available, including trastuzumab and pertuzumab, which target distinct regions of the HER2 protein. The standard treatment protocol for BC patients with positive HER2 involves a combination of anti-HER2 monoclonal antibodies and chemotherapy. In contrast, treating triple-negative breast cancer (TNBC) presents greater challenges compared to other BC subtypes, with chemotherapy being the primary treatment option for this group.[43]
5.4. Triple Negative Breast Cancer:
Triple-negative breast cancer (TNBC) is characterized as a form of breast cancer that does not express oestrogen, progesterone, or HER2 receptors. This subtype is more frequently diagnosed in younger women and is characterized by its aggressive nature and challenges in treatment. In cases of metastasis, the prognosis for TNBC patients is significantly poorer compared to those with hormone-receptor positive or HER2-positive breast cancers. This type of cancer is predominantly found in younger African American and Hispanic women who possess a mutation in the BRCA1 gene. TNBC is noted for its unique molecular characteristics, aggressive behavior, and the absence of specific targeted treatment options.[47] Patients diagnosed with TNBC exhibit a wide range of clinical outcomes, which include differing rates of pathologic complete response (pCR) following neoadjuvant chemotherapy (NACT) in early-stage cases, as well as variable responses to treatment and survival rates in metastatic scenarios. [47]The epidermal growth factor receptor (EGFR), a receptor tyrosine kinase from the ErbB family, plays a crucial role in processes such as angiogenesis, cell growth, metastasis, and the prevention of programmed cell death. Research indicates that the expression of EGFR protein is significantly more prevalent in TNBC compared to other breast cancer subtypes, with overexpression rates ranging from 13% to 76%. [48] Furthermore, EGFR expression has been identified as an independent prognostic factor associated with poorer disease-free survival (DFS) and overall survival (OS).[47]The majority of triple-negative breast cancers (TNBC) belong to the basal-like subtype; however, it is important to note that these two classifications are not synonymous in terms of gene expression profiles and immunohistochemical (IHC) analysis.[49]Basal-like breast cancer is defined through gene expression profiling, and despite their apparent similarities, there can be a discordance of up to 30% between these classifications.[50]Basal-like breast cancers are characterized by low levels of estrogen receptor (ER), progesterone receptor (PR), and HER2, alongside elevated expression of markers such as CK5, CK14, caveolin-1, CAIX, p63, and EGFR (Epidermal Growth Factor Receptor)/HER1, which are indicative of the mammary gland's basal and myoepithelial cell components.[49] Epidemiological research, such as the Carolina Breast Cancer Study, has demonstrated that basal-like tumors are more prevalent in women who experience early menarche, have a higher number of childbirths, are younger at the time of full-term pregnancy, breastfeed for shorter periods, possess a higher body mass index, and exhibit a greater waist-to-hip ratio, particularly among pre-menopausal individuals, when compared to luminal A tumors.[51] Triple-negative breast cancer (TNBC) is recognized for its aggressive nature, typically presenting at a younger age, with larger average tumor sizes, higher tumor grades, and an increased likelihood of lymph node involvement.[49] This subtype is also notable for experiencing a significant peak in recurrence rates within the first three years post-diagnosis, alongside more aggressive metastatic behavior, particularly affecting visceral organs such as the lungs and brain, while showing a reduced tendency to metastasize to bone.[52] Histological analyses indicate that most cases of TNBC are of ductal origin, although other aggressive variants, including metaplastic, apocrine, and adenoid cystic types, are also frequently observed.[49]
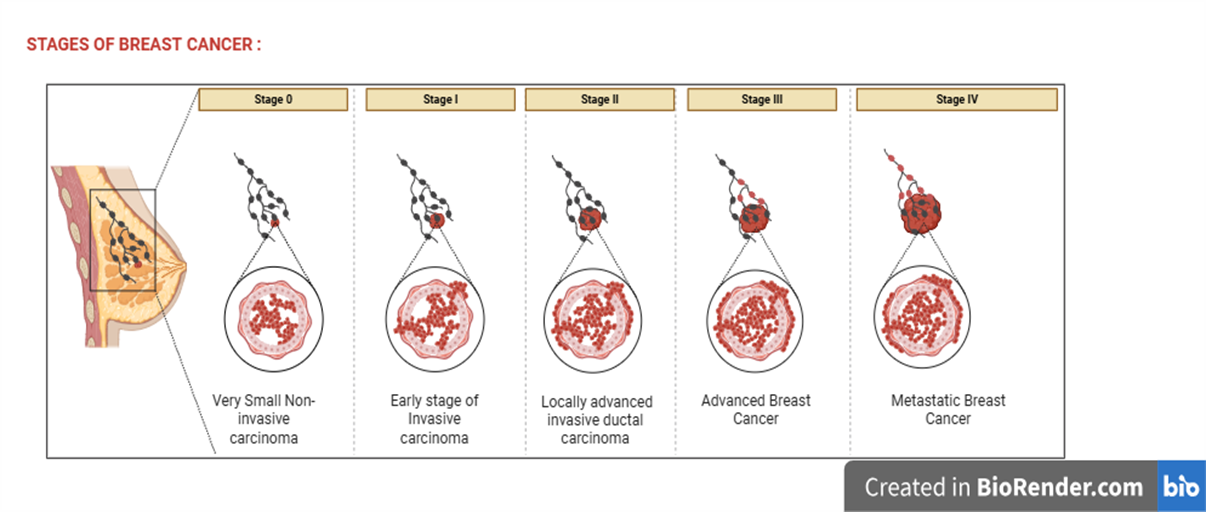
Figure 5: Different stages of Breast Cancer
Breast Cancer Staging and Treatments:
The staging of breast cancer is based on several factors, such as the tumor's size, lymph node involvement, the presence of metastases, and particular biomarkers like estrogen receptors , progesterone receptors, and the ERBB2 receptor, previously known as HER2. Following a histological diagnosis of breast cancer, it is essential to evaluate all pathology samples for the presence of estrogen receptors, progesterone receptors, and ERBB2 status.[53] Breast cancers that do not exhibit any of these markers are identified as triple-negative. Ductal carcinoma in situ (DCIS) is categorized as stage 0, indicating non-invasive breast cancer. Early invasive cancer encompasses stages I, IIa, and IIb, while locally advanced cancer includes stages IIIa, IIIb, and IIIc, all of which are considered nonmetastatic. Stage IV is classified as metastatic breast cancer.[53] The treatments available for the different stages of breast cancer are outlined in Table 1.
Stage 0, DCIS, Non –Invasive Breast Cancer :
Ductal Carcinoma In Situ (DCIS) represents a type of Non-invasive carcinoma that is primarily detected through mammography, which reveals micro calcifications localized within the breast ducts.[54] If not addressed, approximately 40% of DCIS cases may advance to invasive breast cancer.[53]Treatment options for DCIS include lumpectomy, aiming for a surgical margin of 2 mm, accompanied by radiation therapy, or mastectomy. During mastectomy, a sentinel lymph node (SLN) biopsy is performed to assess the rare chance of lymph node involvement, although this procedure may not be feasible post-mastectomy. Patients undergoing lumpectomy are typically offered radiation therapy, as this combination is recognized as a breast-conserving approach. However, radiation may be postponed for those with small, low-grade lesions deemed to have a minimal risk of recurrence, and it is not recommended for individuals who have undergone mastectomy. [53] Furthermore, patients diagnosed with estrogen receptor-positive DCIS who have residual breast tissue are advised to undergo five years of endocrine therapy, which may involve tamoxifen for premenopausal women and either tamoxifen or an aromatase inhibitor for postmenopausal women.[53]
STAGES I-III, Early Invasive and Locally Advanced, Non-Metastatic Breast Cancer :
The management of Non-metastatic breast cancer involves both preoperative and postoperative systemic therapies, which encompass chemotherapy, endocrine therapies, targeted therapies, and immunotherapy utilizing monoclonal antibodies aimed at tumor receptors, alongside surgical intervention and radiation treatment. [53]Molecular testing plays a crucial role in determining the necessity of incorporating chemotherapy into the treatment plan. For individuals diagnosed with hormone receptor-positive, node-negative breast cancer, Including male patients, the 21-gene expression assay known as Oncotype DX is the recommended tool for assessing disease prognosis and making informed decisions regarding the potential addition of chemotherapy.[55,53] It is important to note that when chemotherapy and endocrine therapy are administered in the postoperative setting, chemotherapy is always given prior to endocrine therapy.[55,53]
Preoperative Systemic Therapy:
The objective of preoperative systemic therapy is to reduce the size of resectable breast tumors, making previously unresectable tumors operable, and facilitating sentinel lymph node (SLN) biopsy instead of axillary lymph node dissection (ALND) when axillary nodes are no longer visible. Typically, preoperative therapy is not advised for early invasive breast cancers (stages I, IIa, IIb) as these tumors are usually small enough to be removed via lumpectomy. [53] Preoperative chemotherapy is particularly beneficial for patients with large primary tumors relative to breast size who desire breast-conserving surgery, as well as for those with inoperable conditions. For patients with triple-negative breast cancer, chemotherapeutic agents represent the sole form of systemic therapy available.[55] Additionally, preoperative treatment with trastuzumab (Herceptin) and/or pertuzumab (Perjeta), which are monoclonal antibodies targeting ERBB2, is administered alongside chemotherapy for ERBB2 positive cancers. [53] Patients classified as low-risk with estrogen receptor-positive disease, or older individuals, may qualify for preoperative systemic therapy without the necessity for surgical intervention. A complete response, defined as the absence of detectable tumor, following preoperative systemic therapies correlates with improved disease-free survival and overall survival rates.[55]The extent of tumor response to these therapies is crucial in guiding the need for and effectiveness of any subsequent postoperative systemic treatments.[53]
Surgical Interventions:
Lumpectomy accompanied by radiation therapy should be considered when it is possible to achieve negative margins while maintaining an acceptable cosmetic outcome. In cases where tumors are excessively large, a mastectomy may be necessary to ensure better cosmetic results.[53] Additionally, some women may opt for mastectomy instead of lumpectomy for various reasons, such as a family history of breast cancer, genetic mutations, the desire for peace of mind, or limited access to healthcare facilities that provide radiation therapy. [56]Beyond tumor removal, surgical procedures can also mitigate the risk of breast cancer spreading through the lymphatic system. A sentinel lymph node (SLN) biopsy involves injecting a tracer into the breast and excising the initial axillary nodes that the tracer reaches. This method is favored over axillary lymph node dissection (ALND) for patients who show no clinical signs of nodal disease or have a low nodal burden as indicated by imaging. [53]ALND, which entails the removal of additional lymph nodes and surrounding adipose tissue, is typically reserved for patients with positive nodes identified during SLN biopsy who will undergo mastectomy, those diagnosed with inflammatory breast cancer, or patients with positive nodes following preoperative chemotherapy. Importantly, SLN biopsy does not increase the risk of mortality when compared to ALND.[53]
Postoperative Therapy
Radiation Therapy: Radiation therapy is administered post-surgery for breast cancer to ensure the eradication of any residual subclinical disease. It is typically advised for individuals who have undergone a lumpectomy, as well as for those with high-risk, node-positive conditions who have received a mastectomy.[36] For patients who have had a lumpectomy, the application of radiation significantly reduces the 20-year recurrence rate of ipsilateral breast cancer.[53]
Partial breast irradiation : This approach focuses solely on the lumpectomy site and the adjacent tissue, necessitating fewer sessions of radiation and reducing acute skin toxicity while not elevating the risk of local recurrence.[58]Research indicates that whole breast radiation therapy may yield superior long-term cosmetic outcomes compared to partial breast irradiation.[58] It is essential for shared clinical decision-making regarding radiation to take into account the patient's life expectancy, the tumor's response to preoperative systemic therapies, and the involvement of lymph nodes.[53]
Endocrine therapy:
Approximately two-thirds of breast cancers are classified as hormone receptor-positive, indicating the presence of estrogen receptors, progesterone receptors, or both, and can be effectively treated with endocrine therapies such as tamoxifen and aromatase inhibitors. [53]Women diagnosed with hormone receptor-positive breast cancer while premenopausal should undergo a five-year treatment regimen that includes gonadotropin-releasing hormone (GnRH) for ovarian suppression, in conjunction with either tamoxifen or an aromatase inhibitor.[59] The purpose of ovarian suppression is to inhibit the ovaries from producing estrogen, which can promote the rapid growth of hormone receptor-positive breast cancer. The patient most likely to benefit from the use of GnRH in conjunction with aromatase inhibitors are usually those with hormone receptor-positive . ERBB2-negative breast cancer, particularly those at an increased risk of recurrence. [53]Following a five-year course of tamoxifen therapy, premenopausal patients who initially received tamoxifen will continue with an additional five years of the same treatment, while those who transition to postmenopausal status may opt for either tamoxifen or an aromatase inhibitor for another five years. Additionally, premenopausal patients who were initially treated with aromatase inhibitors may extend their therapy for an additional three to five years.[59] For women diagnosed with breast cancer in a postmenopausal state, a total of up to ten years of endocrine therapy may be administered, which can include tamoxifen alone, an aromatase inhibitor alone, or a combination of both medications. It is important to note that GnRH is not required after menopause.[53]
Targeted therapy : Approximately 15% to 20% of breast cancers demonstrate an overproduction of ERBB2, which is linked to an unfavorable prognosis. However, the prognosis improves with the administration of chemotherapy alongside trastuzumab, given every three weeks for a duration of one year. [60]It is important to note that extending therapy beyond one year does not lead to an increase in long-term disease-free survival.[60]Patients identified as high-risk for ERBB2-positive breast cancer, characterized by larger tumor sizes and positive nodal status, may gain additional benefits from other agents such as pertuzumab and neratinib (Nerlynx), an oral tyrosine kinase inhibitor targeting ERBB2-expressing cells. The inclusion of these therapies in conjunction with a trastuzumab-based regimen has shown a modest improvement in three-year and five-year disease-free survival rates for pertuzumab and neratinib, respectively.[61,62]
Chemotherapy: Chemotherapy is employed to reduce tumor size prior to surgical intervention and is also administered post-surgery to address breast cancers that are hormone receptor-positive and express ERBB2.[59] It serves as a fundamental treatment for triple-negative breast cancer, as neither endocrine therapy nor immunotherapy provides any advantage. [57,59] Taxane-based regimens that do not include anthracyclines are utilized for patients with lower-risk disease, while anthracyclines are incorporated into treatment plans for triple-negative cancers that involve lymph nodes.[53] Furthermore, there is evidence supporting the use of capecitabine (Xeloda) for triple-negative cancers with lymph node involvement, particularly when residual disease is detected at the time of surgery.[53]
Other Treatments: Postmenopausal women undergoing postoperative aromatase inhibitor treatment for nonmetastatic breast cancer should be considered for bisphosphonate therapy, as it seems to reduce the risk of bone metastases and fractures while enhancing survival rates. [53,59,63] Prior to initiating bisphosphonate therapy, it is essential for patients to have a dental assessment and to be on vitamin D and calcium supplementation.[59]
Stage IV Metastatic Breast Cancer
Over the past few decades, the median survival rate for individuals diagnosed with metastatic breast cancer has seen significant improvement due to advancements in treatment options. While a complete cure for metastatic breast cancer remains uncommon, the average survival duration has increased to between 24 and 40 months.[53] The primary objectives of treatment are to alleviate symptoms, prolong life, and maintain a high quality of life. Various therapies, including endocrine therapy, chemotherapy, and immunotherapy, may be utilized to address specific subtypes of breast cancer.[57]In cases where the tumor burden negatively impacts the patient's quality of life, surgical intervention or radiation therapy may be considered following systemic treatment.[64] It is recommended that the 60% to 80% of patients with advanced breast cancer who experience bone metastases receive treatment with denosumab (Prolia) or bisphosphonates such as zoledronic acid (Reclast) or pamidronate (Aredia),[59] as these treatments have demonstrated efficacy in reducing the complications associated with bone metastases, including fractures and hypercalcemia. Additionally, metastases to the liver, lungs, and brain are frequently observed in stage IV breast cancer.[53]
Table 1: Treatment Strategies for Breast Cancer [53]
|
Breast cancer stage |
classification |
Surgery |
Radiation |
Endocrine therapy |
Targeted therapy |
Chemotherapy |
|
0 |
In situ |
Lumpectomy or mastectomy with sentinel lymph node biopsy |
Yes, if lumpectomy |
Tamoxifen : if menopausal
Tamoxifen or aromatase inhibitor :if postmenopausal |
Not commonly used |
Not commonly used |
|
1 and 2
|
Early invasive |
Commonly lumpectomy combined sentinel lymph node biopsy performed. mastectomy may be needed for larger tumors or based on the patient’s preference. |
Yes, if lumpectomy or high-risk, node positive disease with mastectomy |
Tamoxifen: if menopausal Aromatase inhibitor(anastrozole,letrozole,exemestane): if postmenopausal |
Trastuzumab (Herceptin) Pertuzumab (Perjeta)Abemaciclib (verzenio) |
It used for hormone receptor – positive,ERBB2 – positive,TNBC of any stage.(suggest after molecular testing), CMF regimen (cyclophosphamide,methotrexate,fluorouracil) or AC regimen (doxorubicin,cyclophospamide) |
|
3
|
Locally advanced |
Commonly mastectomy plus axillary lymph node dissection |
Yes, if lumpectomy or high-risk, node positive disease with mastectomy |
Tamoxifen: if menopausal
Aromatase inhibitor(anastrozole,letrozole,exemestane): if postmenopausal |
Trastuzumab (Herceptin)
Pertuzumab (Perjeta)
Ado-trastuzumab emtansine (kadcyla) |
Anthracyclines :doxorubicin,epirubicin Taxanes :paclitaxel,docetaxel Other Drugs : cyclophosphamide,carboplatin |
|
4 |
Metastatic |
Mastectomy or lumpectomy may be appropriate when tumor burden impacts quality of life |
Radiation may be appropriate when tumor burden impacts quality of life |
Tamoxifen or fulvestrant : if menopausal Aromatase inhibitor(anastrozole,letrozole,exemestane): if postmenopausal |
Trastuzumab (Herceptin) ,Pertuzumab (Perjeta), Ado-trastuzumab emtansine (kadcyla), Olaparib (Lynparza) |
Anthracyclines :doxorubicin,epirubicin Taxanes :paclitaxel,docetaxel Other drugs:capecitabine,gemcitabine |
Recurrent Breast Cancer:
The management of recurrent breast cancer necessitates a comprehensive, multidisciplinary strategy that evaluates all possible treatment options to achieve the best possible outcomes. [59]For cases of locally recurrent breast cancer that were initially managed with breast-conserving surgery, such as lumpectomy accompanied by radiation, further radiation treatment is not advised; instead, total mastectomy is considered the standard care approach. Nevertheless, a study conducted in 2017 revealed encouraging findings suggesting that local resection followed by partial breast re-irradiation may serve as a viable alternative treatment option.[53,65] In instances of local recurrence post-mastectomy, which typically affects the chest wall, a wide local excision is required. If the patient has not undergone prior radiation therapy, surgical resection followed by radiation is recommended.[53]For regional recurrences that involve the axillary lymph nodes, both surgical resection and radiation therapy are advised. In cases of supraclavicular or internal mammary node recurrence, the standard treatment is radiation therapy without surgical intervention. The management of recurrent disease with distant metastases, classified as stage IV, is determined by the status of estrogen, progesterone, and ERBB2 receptors. Treatment protocols may consist of further endocrine therapy, chemotherapy and therapies that focus on ERBB2. It is essential to conduct regular evaluations with a focus on shared decision-making to monitor ongoing treatment within the context of palliative and supportive care.[53]
CONCLUSION:
Breast cancer represents a significant and prevalent illness impacting numerous women globally. It encompasses various subtypes, including hormone receptor-positive, HER2-positive, and triple-negative breast cancer, each requiring distinct treatment strategies. The implementation of biomarkers such as ER, PR, and HER2 has facilitated early diagnosis and informed treatment selection. Advances in diagnostic technologies, including mammography, ultrasound, and biopsy, have enhanced the likelihood of early cancer detection. Current treatment modalities comprise surgery, radiation, chemotherapy, hormone therapy, and targeted therapies, all of which have contributed to improved survival rates and quality of life. However, certain types, particularly triple-negative breast cancer, present greater treatment challenges, and drug resistance remains a significant obstacle. Continued research is essential to identify more effective treatments and novel biomarkers. A comprehensive strategy that emphasizes early detection, accurate diagnosis, and tailored treatment is crucial for achieving better outcomes for patients with breast cancer.
REFERENCES


Dhanshri Shelake*, Dipali Wankhade, Shubhangi Bhagat, Breast Cancer: A Comprehensive Review of Types, Diagnostic Advances, Biomarkers, And Treatment Strategies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 395-422. https://doi.org/10.5281/zenodo.15792273
 10.5281/zenodo.15792273
10.5281/zenodo.15792273