S. V. U. College of Pharmaceutical Sciences, S. V. University, Tirupati, Andhra Pradesh, India 517502
Polycystic Ovarian Syndrome (PCOS) is a complex endocrine metabolic disorder also known as Hyperandrogenic Anovulation (HA) or Stein–Leventhal syndrome. It is the fourth gynecological problem of hospital admission and affects 6-15% of women of reproductive age worldwide. Characterized by Hyperandrogenism, chronic Anovulation and polycystic ovarian morphology, with symptoms of weight gain, irregular periods, acne and hirsutism. PCOS is a leading cause of infertility and a major risk factor for long-term complications such as type 2 diabetes, cardiovascular disease and endometrial cancer. The etiology of PCOS is multifactorial, involving genetic, hormonal, metabolic and environmental contributors. Insulin resistance and elevated Luteinizing Hormone (LH) levels are central to the pathophysiology, exacerbating ovarian androgen production and disrupting normal follicular development. The cure for PCOS is not known perfectly, but the manageable treatments are defined. In this article we review the epidemiology, etiology, pathophysiology, signs and symptoms and mainly the manageable treatment for PCOS which includes various medicinal systems such as Allopathy, Homeopathy, Ayurveda and Unani systems. Previous studies reviewed that the natural sources of treatment such as Ayurveda and Homeopathy have better curing capability when compared with Allopathy and Unani, including modifications in lifestyle.
Polycystic Ovarian Syndrome (PCOS), is the most common endocrine pathology in the female reproductive system and is the fourth gynecological problem in hospital admission. It is known that 22.5% (about one in four) are affected in India, 11% in Australia, 8% in the UK and 4% in the US. Based on the National Institute of Health (NIH) it is estimated that 4-10 % of women of reproductive age and urban middle class women are suffering with this syndrome [1]. Stein and Leventhal (1935), describes that PCOS represents a condition in which 10 small cysts with a diameter ranging between 2-9 mm develop on one or both the ovaries and the ovarian volume exceeds at least 10 ml in each ovary.
Previously it was considered as a disorder of adult women, but recent studies explain that PCOS is a lifelong syndrome. PCOS is associated with an increase in the production of androgens (male hormones) by the ovaries which shows male characteristic patterns like excess hair growth (hirsutism). Thick, pigmented hair growth occurs on the upper lip, chin, around the nipples and on the lower abdomen. And lack of ovulation results in formation of ovarian cysts which have a higher risk of getting ovarian cancer [2].
Research found that about 50% of married women are affected with PCOS. The desire for pregnancy is a factor that prompts many women with PCOS to first seek medical attention [3].
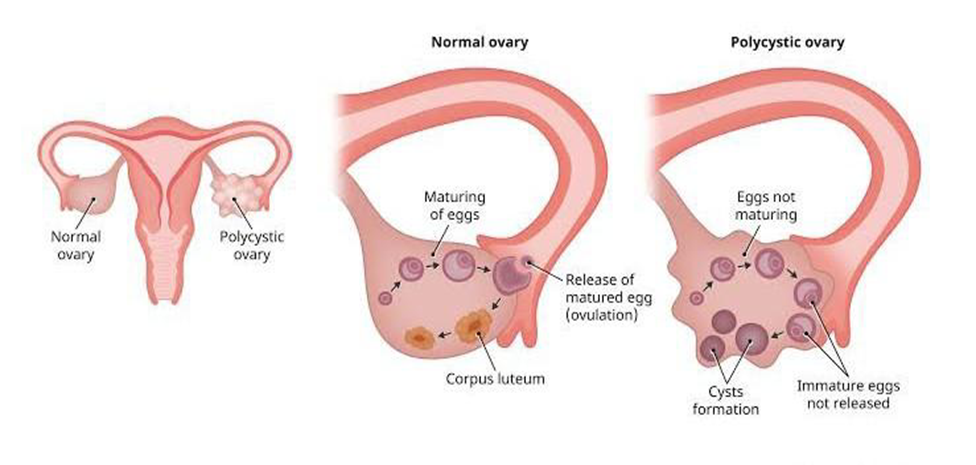
Fig 1: Polycystic Ovarian Syndrome (PCOS)
EPIDEMIOLOGY
According to the Rotterdam diagnostic criteria, the prevalence of PCOS in adolescents varies between a minimum of 3% and a maximum of 26%. In India females of reproductive age, at nearly 9.13% are affected. And in the South Asian population about 90% are found to be affected with PCOS. Younger ones are more likely to be affected due to their lifestyle and food habits. According to marital status married and unmarried women are equally affected [2]. Insulin resistance, weight gain, and obese women are affected more. Studies found that 50% of women with PCOS are obese.
ETIOLOGY
The etiology of this condition is not known perfectly. But it may believe that these were the etiological factors which are responsible for the condition, the factors follow:
PATHOPHYSIOLOGY
Various hypotheses trying to explain the pathophysiology of PCOS. Which includes
SIGNS AND SYMPTOMS
DIAGNOSIS
Women with PCOS may or may not show any symptoms according to their phenotype. But most of the women who were diagnosed with PCOS show clinical representation of elevated levels of LH, FSH and insulin levels. Increases in weight, alopecia and the women may suffer with the problem of menstrual irregularities (mainly shipped Periods for many months), multiple cysts are found in ultrasonography, and ovaries seems to be 1.5 -3 times larger in size rather than the normal ones.
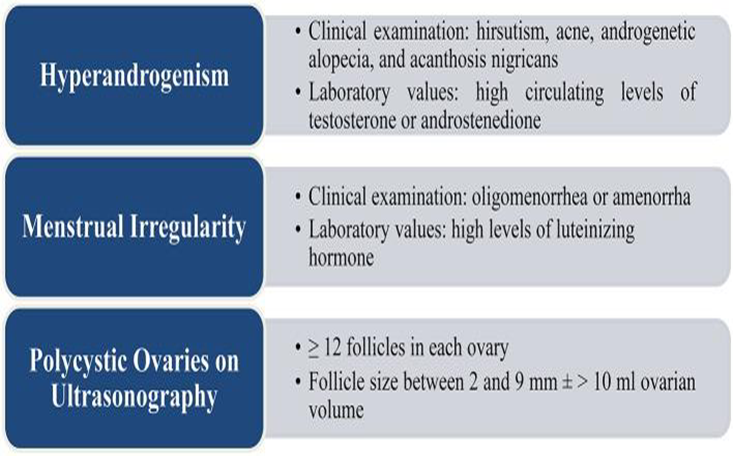
Fig 2: Diagnostic criteria
MEDICAL TREATMENT
Various medicinal systems are available like Allopathy, Homeopathy, Ayurveda, Unaninand Siddha. In order to improve or to cure the condition but not every woman will respond the same to these treatments. The healing capability is based upon the individual’s disease condition, their BMI and many factors based upon it the treatment may vary accordingly. A study states that among the survey conducted on 657 women about 638 (97%) are aware of PCOS [12]. They got to know about the condition from different sources such as Doctors (gynecologists), TV, relatives, radio, friends etc. [6].
A. ALLOPATHY
It is a hormonal therapy treatment in which the cure is done through decrease in the raised hormone levels. The allopathic treatment includes treating with drugs such as Antiandrogens (Spironolactone), [5] Gonadotropin releasing hormones Antagonists [4], oral contraceptives or Birth control pills, Glucocorticoids, Aromatase inhibitors, Insulin sensitizers, are generally used [13].
Anti Androgens
Spironolactone: women with PCOS show high bone mineral density due to the presence of high androgens [11]. So when those women are treated with Anti androgens like spironolactone that shows a significant lowering of bone mineral density and hence Andragonesin is reduced [5].
Gonadotropin Releasing Hormone Antagonist (GnRH)
Cetrorelix: GnRH-antagonists analogue competitively inhibits GnRh and suppress the pituitary gonadotropin output, resulting in decrease of FSH and LH levels. It is proven that usage of gonadotropin releasing hormones decreases the chances of PCOS [4].
Oral Contraceptives
Clomiphene citrate: In general, the oral contraceptive pills reduce the ovarian activity, but it does not improve insulin resistance, obesity, fertility. It is said that clomiphene citrate does not show any effective results when it is used in single [14] but the combination with metformin shows increase in conception rate and decrease in PCOS symptoms. Birth control pills are generally prescribed by the doctors in order to prevent ovulation because absence of ovulation results in lowering chances of formation of newer cysts [12].
Insulin Sensitizers
Insulin plays an important role in PCOS by the stimulation of cytochrome P450c17 [13] which is responsible for the increase in androgen production. May also become obese due to hyperinsulinemia and becomes insulin sensitive. In such cases insulin sensitizers are generally prescribed such as Metformin [14] and Myoinositol (MI), which is used for treating infertility, hyperandrogenism, irregular menses etc. [15].
Aromatase Inhibitors
Anastrozole and Letrozole: They are the selective aromatase inhibitors which induce ovulation by blocking the passage of androgens to estrogens and reducing the quantity of estrogens which produces positive feedback to pituitary results in increase in FSH and provokes ovulation.
In addition to these medication glucocorticoids, IVF therapy, bariatric surgery is included in treatment procedures [16].
Surgery
If the cyst doesn’t go away after several menstrual periods they become larger, look unusual on the ultrasound and cause severe pain, then the women are suggested to remove the cyst by two main surgical procedures. Namely, Laparoscopy, Laparotomy [9].
B. AYURVEDA
Ayurveda classifies PCOS as a kapha disorder/doshas (because it inhibits ovulation). There are eight types of menstrual disorders stated by Sushrutha based on predominance i.e., vataja, pittaja, kaphaja, raktaja, vata-pitta, pitta-kapha, vata-kapha, sannipata [17]. According to Ayurveda, arthava (menstrual blood) is formed from rasa (primary waters of the body) and blood (rakta) [18]. Results in granthiadhar [cystic swelling], arbuda [glandular swelling] [tumors formation], apanavayudushti or margavarodhajanya [obstructed channels and transformation process is suppressed] [19]. The accumulated kapha is expressed in formation of cyst in the ovary as it takes on heavy white sticky quality expressing kapha and ama. The treatment is long term in nature apart from being cost effective with no side effects [20].
The patients with complaints of PCOS (irregular menses, hirsutism, hypertension, hyperinsulinemia, high serum testosterone level, sleeplessness, emotional weakness, depressive and obsessive thoughts, mood swings;) underwent yagya therapy shows 75% relief from the condition. This therapy includes getting the coarse powder from medicinal plants (triphala, shatapuspha etc.) and undergoing a vapor phase followed by sublimation. This medication is released slowly by yagva fire, these vapors will have medicinal values and healthy constituents released in this process impart therapeutic advantage.
Several herbal medicines can be useful in the management of symptoms associated with PCOD; these included in Yagya therapy: Shatavari (Asparagus racemosus), Shatapushpa (Anethum graveolens), Guduchi (Tinospora cordifolia), Atibala (Abutilon indicum), Krishna Jeeraka (Carum carvi), Sahachara (Barleria prionitis), Symplocos racemosa Kuntze (Lodh tree) [21].
In addition, to this yagya therapy the patients are suggested to go for rhythmic deep breathing exercise (pranayama) and chanting of certain Vedic rhymes by the subjects (patients) throughout the duration of the Yagya are included in the treatment [19].
In Ayurveda, the management of PCOS should concentrate on treating Agnimandhya at Jatharagni and Dhatwagni level and alleviating srotavarodhana and ultimately regulating the Apana Vata. Ayurvedic protocol for PCOD includes :
1) Shodhana chikitsa
Shodhana means to purify. This therapy aims to eliminate the accumulated doshas from the body and clear blocked channels (srotas). This chikitsa removes ama (toxins), excess kapha and meda (fat); clears srotorodha (obstruction in rasa and arthava vaha srotas); helps restore normal ovulation and hormonal balance [22, 23].
The treatment involves Panchakarma procedures like Snehana, Swedana, Vamana, Virechana, Basti and Uttara Basti.
2) Shamana chikitsa
Shamana means to pacify or balance. It is aimed at managing symptoms and balancing doshas through herbs, diet and lifestyle. This includes regulating ovulation by using various taila like the satapushpa taila (to reduce the size of ovarian cysts), Narayana taila (to regulate ovulation), castor oil (for dark/clotted menses), triphala and shatapuspha (for amenorrhea, bladder inflammation), aloevera (insulin sensitivity), mentha (histurism) [9].
A study found that the polyherbal treatment with Sharapunkha, Latakaranja, Haridra, Shatapushpa, Shatavari, Trikatu, and Tankan bhasma shows reduction in PCOS chances [24].
Dosha action: Pitta-Kapha shamak
Supports liver function, helps metabolize excess estrogens and reduces hormonal imbalance.
Dosha action: Kapha-Vata shamak
Helps correct oligomenorrhea/amenorrhea, promotes ovulation and supports reproductive balance.
Dosha action: Tridoshaghna (mainly Kapha-Pitta shamak)
Excellent for acne, obesity, insulin resistance and reducing cystic inflammation.
Dosha action: Vata-Kapha shamak
Used in Uttara Basti and oral formulations to regulate menstrual cycles and reduce cysts.
Dosha action: Pitta-Vata shamak
Improves hormonal balance, follicular development and corrects infertility
(Dry ginger + Black pepper + Long pepper)
Dosha action: Kapha-Vata shamak
Reduces Ama, improves digestion, supports weight loss and enhances herbal absorption.
Dosha action: Kapha-Vata shamak
Helps correct oligomenorrhea or amenorrhea, useful in hormonal acne, cyst resolution. Tankan Bhasma should only be taken under medical supervision, as overdose may be toxic. Not recommended during pregnancy or active bleeding. Adjust dose according to prakriti, age and severity of PCOS.
C. HOMEOPATHY
PCOS/PCOD finds promising treatment with homeopathic mode of system. Homeopathic mode of treatment is very safe and free from side effects[24]. Homeopathic medicines are powerful dominant influential drugs in the form of pills, powder and liquids. They regulate hormonal imbalance, regularizing ovulation, restoring menses normalcy. Some homeopaths or proponents of homeopathy also claim that it helps in dissolving or solubilizing the cysts. Homeopathy focuses on treating and curing the root cause of the problem. Combination of homeopathic constitutional treatment with exercise just like 30 minutes’ walk, aerobics, swimming etc.
Homeopathic medicines like Apis, Pulsatilla, Sepia, Lachesis and Graphites[25], Calcarea Carb, Thuja occidentalis, Formica rufa, Janosia asoca treat PCOS with their natural active constituents.
Source: Honeybee (whole body).
Type: Animal-based remedy.
Treatment: Ovarian cysts with stinging pain, bloating, scanty menses.
Source: Wind flower (entire fresh flowering plant).
Type: Plant-based remedy.
Treatment: Irregular, delayed, or suppressed periods; hormonal acne. Suited for young girls or women with soft temperament and changeable symptoms.
Source: Cuttlefish (ink of the cuttlefish).
Type: Animal-based remedy (marine origin).
Treatment: Irregular periods, infertility, hirsutism, pelvic heaviness. Treats women with chronic PCOS, emotionally withdrawn, tired and hormonally imbalanced.
Source: Bushmaster snake (venom).
Type: Animal-based remedy (reptile venom).
Treatment: Left-sided ovarian cysts, suppressed menses, intense premenstrual syndrome.
Source: Pure mineral carbon (natural graphite).
Type: Mineral-based remedy.
Treatment: Obesity, delayed menses, acne, hirsutism.
Source: Calcarea carb. Calcium carbonate from the middle layer of the oyster shell.
Type: Mineral/Animal-based remedy.
Treatment: Weight gain, heavy or irregular menses, infertility, often used when there is excess estrogen or progesterone imbalance.
Source: Fresh green twigs of the Thuja tree.
Type: Plant-based remedy.
Treatment: Multiple ovarian cysts, hirsutism, suppressed menstruation, oily skin and sebaceous disorders.
Source: whole body of red wood ant
Type: Animal-based remedy (insect origin)
Treatment: Formica rufa is not a primary remedy for PCOS, but it is used in cases where PCOS coexists with rheumatic complaints, pelvic congestion and glandular swellings.
It is found that in homeopathic clinical observations, the combination of Lycopodium clavatum and Calcarea carbonica are proven that they removed the cyst totally [25].
D. UNANI
The main cause of the disease is impairment of Humor (akhlat) and Ehtebase Tams ( Suppression of menstruation) which is caused due to domination of Balgham [26]. In Unani literature the complication of prolonged amenorrhoea results in hoarseness of voice, male body contour (hirsutism), acne etc. It was observed by Ibn Sina, Ismail Jurjani and Al Razi that development of masculine features is more common in obese women .
In Unani system of medicine, treatment is based on four categories
1. Ilaj bil Tadbeer (Regimental therapy):
2. Ilaj bil Ghiza (Dietotherapy):
3. Ilaj bid Dawa (Pharmacotherapy):
Treatment with single or combination/compound drugs and local application of herbs to reduce severity of hair growth, acne and hyperpigmentation.
4. Ilaj bil Yad (Surgical Treatment)
Fasd (venesection) of Rag-e-Safin (saphenous vein) to divert the flow of blood towards the uterus to induce menstruation.
Specific Drugs:
Essentially PCOS should be taken care of in the beginning itself. But most of the time it is diagnosed only in a later period or else it is neglected that it is a minor health complaint or simple menstrual irregularity. Early detection and immediate attention will help to cure the disease as well as to avoid complications like infertility.
CONTROL OF PCOD
Maintaining a healthy lifestyle like reducing body weight and abdominal fat, results in reducing testosterone levels and improves both hair growth and insulin resistance.
Losing weight is challenging with PCOS, but doing so can help to reduce the male hormone levels in the body and some women start to ovulate naturally.
Exercise, Yoga and meditation definitely stimulate the endocrine system and may be useful to control PCOD.
DISCUSSION & CONCLUSION:
PCOD is the most emerging gynic problem in women in the current scenario. It involves in the treatment which is helpful in reducing the obese, insulin and hormonal imbalances in the body. The effective treatment is to be done to minimize the condition by using the various treatment methods. Though it is mentioned that PCOS is not curable, it shows 75% cure in Ayurveda and Homeopathy. So, the development of Polyherbal combinations in both Ayurveda and homeopathy may lead to the best cure for the disease.
In this review article we have gone through the various methods of treatment that are included in treatment of PCOS. During the comparative study we found that Ayurveda and Homeopathy are promising and safe Treatments for PCOS, when compared with Allopathy which are having more side effects. So, the development for newer formulations in Ayurveda and Homeopathy which includes polyherbal formulations may show the best cure for PCOS in future.
REFERENCES



Dr. Girish C, Pravallika S, Sindhu G, O. V. S. Reddy, Decoding Polycystic Ovarian Syndrome: A Review of Causes, Consequences and Clinical Approaches, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 308-319. https://doi.org/10.5281/zenodo.17791855
 10.5281/zenodo.17791855
10.5281/zenodo.17791855
