
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Aadhi Bhagawan College of Pharmacy, Rantham, Vembakkam T.K, Thiruvannamalai, Tamilnadu, India.
The present study aimed to develop and evaluate a pH-triggered ophthalmic in-situ gel containing Ofloxacin to enhance ocular bioavailability and prolong drug retention. Formulations were developed using sodium alginate, HPMC, and HPMC K15 in varying concentrations. The calibration curve was established at 295 nm and 365 nm using UV spectrophotometry for accurate drug quantification. FTIR confirmed the compatibility between Ofloxacin and selected polymers. Among four formulations (IGO-1 to IGO-4), IGO-3 exhibited the highest drug content, viscosity, and gelling strength, with sustained drug release up to 12 hours. Sterility testing by direct inoculation showed no microbial contamination. These findings support the potential of Ofloxacin in-situ gels as effective ocular drug delivery systems.
Topical ophthalmic drug delivery is widely preferred due to its ease and localized effect, but it suffers from poor bioavailability because of rapid tear drainage, limited corneal permeability, and short residence time. While systemic administration (oral or injectable) is an option, it often leads to side effects due to systemic exposure. To overcome these challenges, novel delivery systems aim to prolong drug contact time on the ocular surface and enhance corneal absorption. Factors like tear dynamics, drug loss, and limited permeability reduce drug effectiveness. Improved formulations—like in situ gels—help extend drug retention in the conjunctival sac, improving absorption and therapeutic outcomes.
The human eye is a complex organ responsible for vision, functioning like a camera. It captures light through the cornea and lens, focusing it onto the retina at the back of the eye. The retina converts light into electrical signals, which are sent to the brain via the optic nerve. Structures like the iris, pupil, aqueous humor, and vitreous body help regulate light entry, pressure, and shape. Due to its delicate structure and protective barriers, drug delivery to the eye—especially to internal parts—can be challenging, requiring specialized formulations for effective treatment.
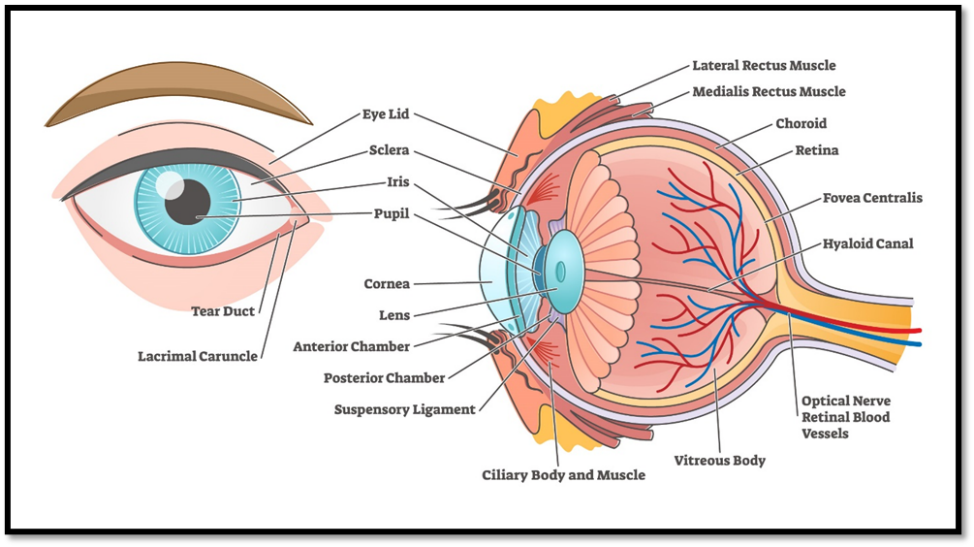
Fig: 1 Human Eye
In situ gels are liquid formulations that transform into a gel upon exposure to specific physiological conditions such as pH, temperature, or ions. In ophthalmic drug delivery, pH-sensitive in situ gels remain as drops during administration and quickly gel upon contact with the eye’s natural pH. This transition helps prolong the drug's residence time on the ocular surface, enhances absorption, and reduces dosing frequency, making them more effective and patient-friendly than conventional eye drops.
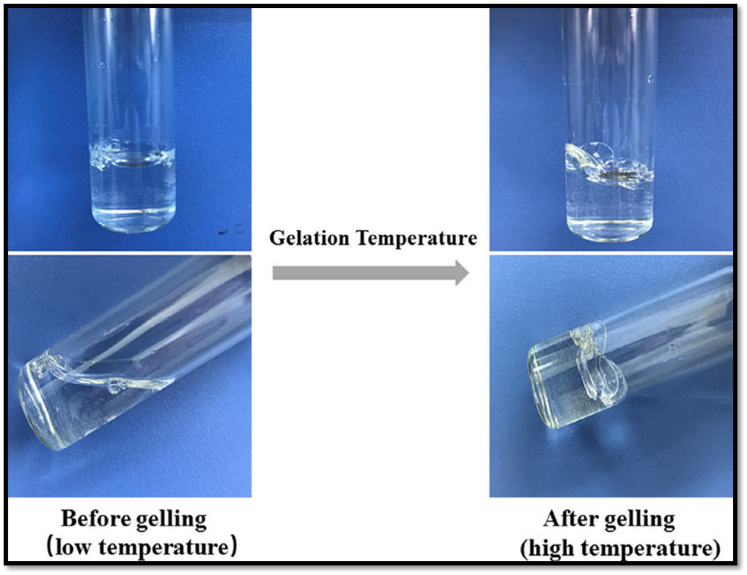
Fig: 2 In - Situ Gel
1.2.1 Advantages of In Situ Gels:
1.2.2 Disadvantages of In Situ Gels:
1.2.3 Ideal Properties of In Situ Gels:
1.2.4 Types of In Situ Gels (Based on Stimuli):
1.2.5 Classification of In Situ Gelling Systems:
Ofloxacin is a broad-spectrum antibiotic belonging to the fluoroquinolone class. It works by inhibiting bacterial DNA gyrase and topoisomerase IV, enzymes essential for DNA replication and cell division. Ofloxacin is effective against a wide range of Gram-positive and Gram-negative bacteria and is commonly used to treat bacterial infections of the eyes, ears, respiratory tract, urinary tract, and skin. In ophthalmology, it is used topically to treat conditions like conjunctivitis and corneal ulcers due to its strong antibacterial activity and low resistance potential.
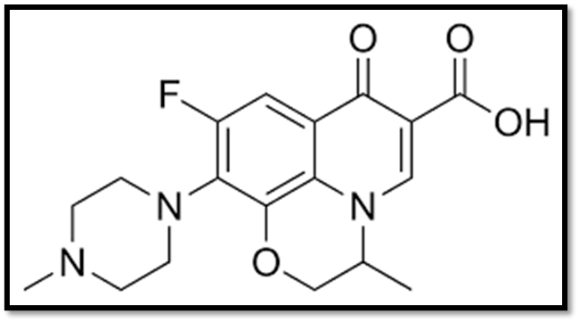
Fig: 3 Structure of Ofloxacin
2.2 Physicochemical Properties of Ofloxacin:
2.3 Pharmacology:
Pharmacodynamics: Ofloxacin is a fluoroquinolone antibiotic that exerts its bactericidal effect by inhibiting bacterial DNA gyrase, an enzyme essential for DNA replication. This inhibition prevents the unwinding of DNA strands, blocking bacterial cell division. Ofloxacin has a high selectivity for bacterial enzymes, being approximately 100 times more active against bacterial DNA gyrase than its mammalian counterpart. It is a broad-spectrum agent effective against both Gram-positive and Gram-negative bacteria.
Mechanism Of Action: During DNA replication and transcription, ofloxacin inhibits excessive DNA supercoiling by targeting bacterial enzymes DNA gyrase and topoisomerase IV. By interfering with these enzymes, ofloxacin prevents normal bacterial cell division, leading to the inhibition of bacterial growth.
Absorption: In the tablet formulation, ofloxacin has an approximate bioavailability of 98%, which is quite good.
Distribution: The consumption of ofloxacin leads to its widespread distribution throughout various organs and tissues of the body.
Protein Binding: 32%
Metabolism: Quinolones (QNs), including ofloxacin, are widely used for their strong antimicrobial properties; however, their use in immature animals is limited due to QN-induced arthropathy. The exact mechanism of this chondrotoxicity remains unclear. In a study, juvenile rabbit joint chondrocytes cultured in alginate microspheres were exposed to varying concentrations of ofloxacin (0, 2, 5, 10, 20, and 40 µg/mL) for 96 hours. At 10 µg/mL, ofloxacin induced apoptosis in chondrocytes, evidenced by increased caspase-3 activity and DNA fragmentation. Immunoblotting revealed significant reductions in growth factor receptor-bound protein 2 (Grb2) and phosphorylated extracellular signal-regulated kinase 1/2 (phospho-ERK1/2), while beta(1)-integrin mRNA levels remained unchanged. Apoptosis was shown to be caspase-8-dependent, and inhibition of caspase-8 did not affect phospho-ERK1/2 or beta(1)-integrin expression. Notably, supplementation with Mg²? prevented ofloxacin-induced apoptosis, suggesting that suppression of beta(1)-integrin function leads to caspase-8-dependent apoptosis after 48 hours of exposure.
Excretion: The majority of ofloxacin is eliminated via renal excretion within 48 hours of oral administration, with approximately 65% and 80% excreted unchanged. There is minimal biliary excretion of ofloxacin, which excretes 4-8% of the dose in the feces.
Toxicity: Mild increases in ALT and alkaline phosphatase levels occur in 1–2% of patients taking ofloxacin, usually asymptomatic and transient, resolving with continued treatment. However, rare cases of severe liver injury, including fatal outcomes, have been reported with high doses. Symptoms such as nausea, fatigue, abdominal pain, and jaundice typically appear within 2 days to 2 weeks of treatment. Hepatotoxicity is considered a class effect shared by ofloxacin and other fluoroquinolones.
Uses: The antibacterial agent ofloxacin is used to treat a number of bacterial infections in the body, such as infection in the eye, respiratory tract, kidney, skin, soft tissue, and urinary tract. It is used to treat bacterial infections in many parts of the body.
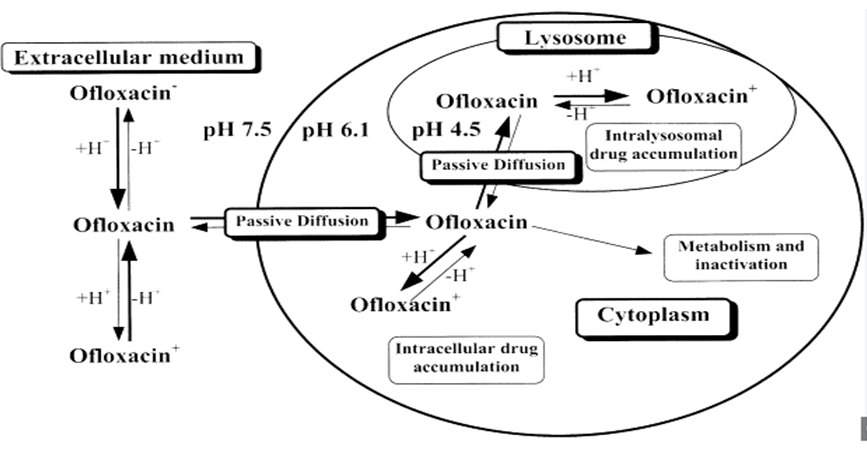
Fig: 4 MOA Of Ofloxacin
Preparation of Ofloxacin Stock Solution: A known amount of Ofloxacin was dissolved in a sodium hydroxide solution. The resulting solution was then diluted with simulated tear fluid to prepare the stock solution.
Preparation of Different Concentrations: Using the Ofloxacin stock solution and simulated tear fluid, solutions with concentrations of 5, 10, 15, 20, Up to 50 μg/ml were prepared.
UV Spectrophotometer Analysis: Each prepared solution was scanned using a UV spectrophotometer to determine the λmax (wavelength of maximum absorption). The absorbance of each solution was then measured at λmax (295 nm).
Construction of Standard Curve: The concentrations of the Ofloxacin solutions were plotted on the X-axis, and their corresponding absorbance values were plotted on the Y-axis to construct the standard curve.
Estimation of Drug Content and Percentage Drug Release: Samples containing unknown concentrations of Ofloxacin were analyzed by measuring their absorbance. The standard curve was used to determine the concentrations of Ofloxacin in these unknown samples. Based on the known and determined concentrations, the drug content and percentage drug release were calculated.
Preparation of Primary Stock Solution and Standard Curve at 365 nm for Ofloxacin: Accurately weigh 100 mg of Ofloxacin and dissolve it in 30 ml of distilled water. Make up the volume to 100 ml with distilled water to obtain the primary stock solution.
Sample Solution Preparation: Dilute 1 ml of the primary stock solution to 10 ml with distilled water to obtain a solution with a concentration of 100 μg/ml. From this, pipette 1 ml and dilute it to 10 ml to obtain a concentration of 10 μg/ml. To prepare solutions with concentrations of 2, 4, 6, 8, and 10 μg/ml, pipette 0.2, 0.4, 0.6, 0.8, and 1 ml, respectively, of the 10 μg/ml solution and dilute each to 10 ml with distilled water. In the standard graph, the X-axis represents the known concentrations of Ofloxacin, and the Y-axis represents the corresponding absorbance values.
Fourier-transform infrared spectroscopy (FTIR) is a technique that produces an interferogram when two beams of radiation interfere. The resulting signal depends on variations in the path length of the beams. Through Fourier transformation, these signals are converted from the time domain to the frequency domain using mathematical methods. FTIR analysis was conducted to evaluate the compatibility between the drug and its excipients. The spectral characteristics of the pure drug and its physical mixture with excipients were analyzed to identify any potential chemical interactions. Infrared (IR) spectral analysis is commonly used to detect chemical changes that may occur when a drug is combined with excipients.
Considering the physical, chemical, and biological properties of both the drug and excipients is essential when formulating an effective and stable dosage form. Compatibility between these components is crucial to ensure the final product is safe, effective, and stable. In this study, the KBr (potassium bromide) dispersion method was used to evaluate the interactions within in situ gel formulations. The FTIR spectra were recorded in the wavelength range of 4000–400 cm?¹ for samples containing the drug alone, the excipients, and their mixtures with potassium bromide.
Table: 1 Formulation Of In-Situ Gel
|
Ingredients |
IGO-1 |
IGO-2 |
IGO-3 |
IGO-4 |
|
Ofloxacin |
0.5 |
0.5 |
0.5 |
0.5 |
|
Sodium Alginate(gm) |
1 |
1 |
1 |
1 |
|
HPMC (gm) |
1.2 |
- |
- |
1.3 |
|
HPMC K15(gm) |
- |
1.3 |
1.2 |
- |
|
NaCl (gm) |
0.9 |
0.9 |
0.9 |
0.9 |
|
Methyl Paraben (gm) |
0.02 |
0.02 |
0.02 |
0.02 |
|
Distilled water |
Q.S to 100ml |
Q.S to 100ml |
Q.S to 100ml |
Q.S to 100ml |
Formulation of Ofloxacin Gels by pH-Induced Method: Different formulations of Ofloxacin gels were prepared using the pH-induced method with varying ratios of sodium alginate, HPMC, and HPMC K15. The required quantities of these polymers were slightly heated and stirred for 15 minutes, then allowed to cool. Once the polymer solution cooled, sodium chloride, methylparaben, and the Ofloxacin drug solution were added gradually with continuous stirring to ensure uniform mixing. The final solution was then filtered through filter paper with a pore size of 0.2 mm to obtain a clear formulation. The total volume of each formulation was adjusted to 100 ml
3.4.1 Visual Appearance and Clarity: Visual inspection of the formulations was performed under alternating light conditions on white and black backgrounds to assess clarity and brightness before and after gelation.
3.4.2 pH Measurement: For ocular formulations, maintaining a non-irritating pH close to that of lacrimal fluid is essential. To achieve this, dropwise additions of 0.1 M NaOH were made to each formulation while stirring continuously. The pH of the solutions was measured using an Ecolab Digital pH Meter to ensure compatibility with the ocular environment.
3.4.3 Drug Content Uniformity: To determine drug content, 1 ml of in situ gel was diluted with simulated tear fluid in a 100 ml volumetric flask. An additional dilution was performed by taking 1 ml of this solution and diluting it to 10 ml with simulated tear fluid. The percentage of drug content was then determined by measuring absorbance at 295 nm using a UV spectrophotometer.
3.4.4 Viscosity Measurement: Viscosity was measured using a Brookfield DV III Programmable Rheometer. The viscosity of each formulation was recorded at various spindle speeds after the addition of simulated lacrimal fluid. Upon increasing the pH to 7.4, all formulations rapidly transitioned to a gel state. The formulations exhibited pseudo-plastic behavior, characterized by a decrease in viscosity with increasing shear rate (shear-thinning).
3.4.5 In-vitro Diffusion Studies: An in-vitro diffusion study of the in-situ gel formulation was carried out using a Franz diffusion cell. Freshly prepared simulated tear fluid was placed in the receptor compartment, while the formulation was introduced into the donor compartment. A dialysis membrane with a pore size of 0.22?μm was positioned between the donor and receptor compartments. The entire setup was placed on a thermostatically controlled magnetic stirrer, and the temperature was maintained at 37?±?0.5?°C to simulate physiological conditions. At hourly intervals over a period of 8 hours, 1 ml samples were withdrawn from the receptor compartment and replaced with an equal volume of fresh medium to maintain sink conditions. The withdrawn samples were analyzed using a UV spectrophotometer at the specific absorbance wavelength (λmax) for Ofloxacin. Appropriate solvent concentrations and volumetric flask dilutions were used for accurate measurement. A previously constructed standard calibration curve was used to calculate the drug concentration in each sample, and the cumulative drug release percentage (%CDR) was calculated accordingly.
3.4.6 Sterility Testing (Direct Inoculation Technique): To ensure the sterility and microbiological safety of the formulation, the direct inoculation technique was employed. A specified volume of the sample was aseptically withdrawn using a sterile syringe and transferred into two sterile media: Fluid Thioglycollate Medium (FTM) and Soybean Casein Digest Medium (SCDM).
The FTM was incubated at 30–35?°C for 14 days to detect the presence of anaerobic and aerobic bacteria. The SCDM was incubated under conditions suitable for fungal and bacterial growth, with periodic observations made over 14 days to assess any signs of microbial contamination. These procedures ensured that the formulation met sterility requirements for ophthalmic use.
Table: 2 Calibration Curve
|
CONCENTRATION (µg\ml) |
ABSORBANCE |
|
0.2 0.4 0.6 0.8 1.0 |
0.188 0.278 0.431 0.598 0.706 |
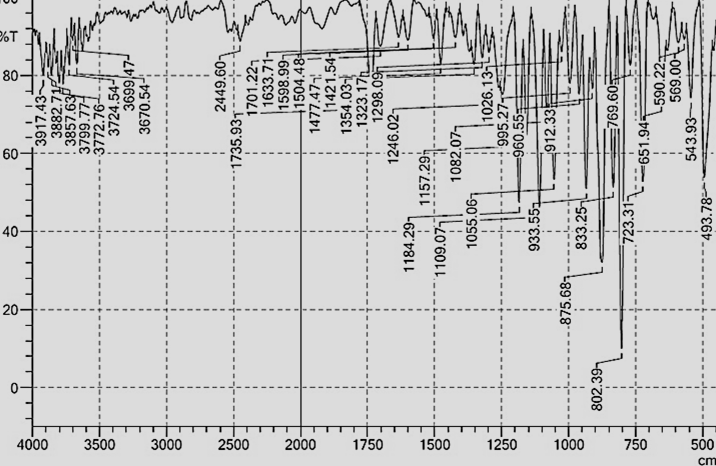
Fig: 4 IR Spectra of Ofloxacin
Table: 3 Physical Parameters
|
Formulation |
Appearance |
pH |
Ofloxacin Drug Content % |
Gelling Strength |
Duration Of Gelling |
|
IGO-1 |
White |
4.48 |
99.66 |
++ |
7hrs |
|
IGO-2 |
White |
4.35 |
99.35 |
++ |
8hrs |
|
IGO-3 |
White |
4.56 |
99.98 |
++++ |
10hrs |
|
IGO-4 |
White |
4.55 |
99.45 |
+++ |
9hrs |
Table: 4 Viscosity
|
RPM |
IGO - 1 |
IGO - 2 |
||
|
Viscosity at pH 4.4(cps) |
Viscosity at pH 7.4(cps) |
Viscosity at pH 4.4(cps) |
Viscosity at pH 7.4(cps) |
|
|
5 |
21.8 |
5799 |
25.2 |
6319 |
|
10 |
16.3 |
4122 |
19.3 |
4485 |
|
20 |
9.33 |
2283 |
15.7 |
3867 |
|
30 |
6.31 |
1445 |
13.5 |
2431 |
|
50 |
3.35 |
665 |
9.35 |
2001 |
|
RPM |
IGO - 3 |
IGO - 4 |
||
|
Viscosity at pH 4.4(cps) |
Viscosity at pH 7.4(cps) |
Viscosity at pH 4.4(cps) |
Viscosity at pH 7.4(cps) |
|
|
5 |
23.41 |
6321 |
26.43 |
5765 |
|
10 |
18.44 |
5762 |
21.31 |
5008 |
|
20 |
14.33 |
5296 |
16.33 |
4561 |
|
30 |
13.11 |
4432 |
10.31 |
3693 |
|
50 |
8.25 |
3376 |
7.21 |
2976 |
Table: 5 In-Vitro Drug Release
|
Time (hrs) |
IGO-1 %CDR |
IGO-2 %CDR |
IGO-3 %CDR |
IGO-4 %CDR |
|
1 |
27.9 |
25.4 |
19.5 |
21.5 |
|
2 |
49.4 |
35.6 |
22.2 |
25.4 |
|
3 |
61.5 |
43.7 |
29.2 |
29.8 |
|
4 |
69.4 |
59.2 |
35.1 |
35.6 |
|
5 |
73.4 |
68.4 |
47.2 |
43.7 |
|
6 |
83.5 |
78.2 |
57.1 |
51.6 |
|
7 |
91.6 |
87.1 |
63.2 |
63.7 |
|
8 |
95.6 |
95.5 |
70.3 |
71.6 |
|
9 |
|
97.2 |
78.2 |
83.3 |
|
10 |
|
|
85.2 |
96.5 |
|
11 |
|
|
90.2 |
|
|
12 |
|
|
98.4 |
|
Table: 6 Direct Inoculation
|
Formulation code |
Day of incubation |
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
12 |
|
IGO-1 |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
|
IGO-2 |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
|
IGO-3 |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
|
IGO-4 |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
DISCUSSION:
The formulation of Ofloxacin-loaded in-situ gel aimed to improve the precorneal residence time, therapeutic efficacy, and patient compliance. The calibration curve constructed for Ofloxacin showed linearity, enabling accurate measurement of unknown drug concentrations for in-vitro release and drug content estimation.
FTIR Compatibility Studies: The FTIR spectra revealed no significant shifts or disappearance of characteristic peaks when Ofloxacin was mixed with polymers, confirming chemical compatibility. This ensured formulation stability without potential degradation or interaction.
Formulation Optimization: The pH-induced gelation method allowed sol-to-gel transition upon contact with simulated tear fluid (pH 7.4). All formulations were clear, with pH values (4.35–4.56) within the acceptable ophthalmic range, reducing the risk of irritation.
Drug Content and Viscosity: All formulations demonstrated high drug content (~99%), confirming uniform drug dispersion. Viscosity analysis showed a pseudo-plastic (shear-thinning) behavior, essential for ocular comfort and ease of administration. Notably, IGO-3 had the highest viscosity post-gelation, attributed to the balanced combination of sodium alginate and HPMC K15.
In-Vitro Drug Release: Ofloxacin release was prolonged across all formulations. IGO-3 exhibited the slowest and most sustained release, reaching 98.4% over 12 hours. The matrix-forming polymers effectively controlled drug diffusion, supporting a once- or twice-daily dosing regimen.
Sterility Testing: No microbial growth was observed in FTM or SCDM media over 12 days, confirming aseptic formulation procedures and suitability for ophthalmic application.
CONCLUSION:
The study successfully developed a stable and effective Ofloxacin in-situ gel formulation for ophthalmic delivery. Among all, IGO-3 emerged as the optimal formulation due to its high viscosity, superior gelling strength, and sustained drug release. FTIR confirmed no drug-polymer interactions, and sterility testing ensured microbiological safety. The pH-triggered sol-to-gel transition mimics physiological conditions and supports better drug retention on the ocular surface. These findings suggest that this in-situ gel formulation could improve therapeutic efficacy and patient adherence in the treatment of ocular infections.
REFERENCES


M. Nithish Khanna, L. Gopi, Dr. V. Kalvi Moorthi, Dr. K. Kaveri, Design and Characterization of an In Situ Gelling Ophthalmic System for Ofloxacin, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 2839-2849. https://doi.org/10.5281/zenodo.16268767
 10.5281/zenodo.16268767
10.5281/zenodo.16268767