
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
1 Department of Pharmacology, D. Y. Patil College of Pharmacy, Kadamwadi, Kolhapur-416003, Maharashtra, INDIA.
2 Department of Pharmaceutical Quality Assurance, Progressive Education Society's Modern College of Pharmacy Nigadi, Pune, INDIA.
3 Department of Pharmacology, Advance Institute of Biotech and Paramedical Sciences (188), Kanpur, INDIA.
4 Department of Pharmacy, Usha Martin university, Ranchi, Jharkhand, 835103, INDIA.
5 Department of Pharmacy, H R Patel Institute of Pharmaceutical Education and Research, Shirpur, INDIA.
6 Department of Pharmacy, Usha Martin university, Ranchi, Jharkhand, 835103, INDIA.
Kidney Stone Disease is a widespread and repetitive epidemiological problem affecting the entire world, and the current methods of management are limited by the complications associated with the procedures, the high rate of recurrence, and the lack of adherence of patients to the preventive treatment. This review clearly looks at the transformative potential of nanotechnology to cover these critical gaps in the entire continuum of stone care. We describe how engineered nanoparticles (NPs) which can be either organic, inorganic, or hybrid take advantage of special properties of nanoscale to apply to a specific purpose. They are nano-enabled biosensors to detect early metabolic risks, advanced imaging and Surface-Enhanced Raman Spectroscopy to characterize the composition of stones precisely and new therapeutic platforms such as photonic lithotripsy and nanofluid enhanced laser lithotripsy to fragment the stones efficiently and without direct contact. Additionally, we discuss nanotechnology to post-procedural issues such as the use of magnetically retrievable remnants and nano-formulations to prevent pharmacologically. These materials are synthesized and rationally designed based on the understanding of stone nanostructure and the principles of the so-called green chemistry. We then examine this strict preclinical assessment route, including in vitro efficacy measures and in vivo safety and biodistribution experiments, and finally catalogue the great challenges, including scalable manufacturing, sterilization, regulatory manoeuvres and clinical integration, which will have to be conquered to bring these promising proof-of-concept breakthroughs to mainstream urology practice. Finally, nanotechnology holds a paradigm shift of individualized, preventive, and minimally invasive care of urolithiasis.
Kidney stone disease is a serious and increasing health problem throughout the world, which has serious clinical and economic implications. Increased prevalence Urolithiasis has been diagnosed to rise significantly over the last few decades, reaching about 10-15 percent of the population in developed countries, and the incidence has been seen to rise in traditionally low-risk populations such as Asia and the Middle East [1]. This epidemic is closely linked to dietary patterns, climatic changes and rising obesity and metabolic syndrome. The financial toll is quite phenomenal; in the United States alone, annual expenditure on management of stone disease runs past 10 billion dollars including direct medical care, surgery, office visits and high indirect costs due to productivity loss. The need is not limited to acute, painful episodes, clinically. The recurrence is more than 50 percent lifetime risk without preventive actions in stone formers and it is a cycle of chronic disease that requires repeat interventions and follow-ups. The high recurrence rate is an important indication of a serious unmet need to develop more effective preventive and treatment methods that address the underlying pathophysiological mechanisms of stone formation. Existing management tools, though usually competent in the acute environment, are afflicted by tremendous constraints which nanotechnology aims to resolve [2]. Symptomatic stone First-line therapies, including extracorporeal shock wave lithotripsy and ureteroscopy with laser lithotripsy, are successful, but also have the risk of complications. There are also the residual fragments of stones, the clinically insignificant fragments that are likely to become the nidus to rapid recurrence, ureteral injury, stricture formation, and renal injury of tissue. In addition, the interventions are purely mechanical; that is, they eliminate or fragment the already present stones, but do not alter the underlying biochemical milieu which favors crystallization. The use of pharmacologic prevention, mainly with potassium citrate or thiazide diuretics, is limited by the low adherence levels of the patient to a long-term treatment because of adverse effects and the requirement of taking it multiple times per day [3]. This disparity of what is effectively removable and what cannot be prevented in the long term is what makes the clinical imperative to seek out patient-friendly therapeutic solutions that are targeted and sustained, and this is the main reason as to why nanotechnology should be considered. Nanomedicine principles provide a revolutionary set of tools to address such challenges by taking advantage of the unique physicochemical properties that are found at the nanoscale (1-100 nm). One of the most important characteristics is that surface area-to-volume ratio is outstanding and increases the reactivity and functional capacity of nanoparticles (NPs). This can be densely surface functionalized with targeting ligands, therapeutic agents or imaging moieties. Also, nanomaterials are size dependent which has optical, magnetic, and acoustic properties not found in their bulk counterparts. An example is gold nanoparticles that are effective in transforming absorbed near-infrared light to localized heat (photothermal effect) and superparamagnetic iron oxide nanoparticles that can be moved about using external magnetic fields. These properties form the basis of non-invasive therapy and targeted delivery systems design. NPs have been designed to move about the renal environment, respond to external stimuli such as light or magnetic fields, and react to a specific environment such as stone components or renal epithelium in urological applications [4].
The nanoparticles used in controlling kidney stones can be broadly classified as either organic, inorganic or hybrid and each has its own benefits. Organic NPs, such as liposomes and polymeric NPs (e.g., of PLGA or chitosan) and dendrimers, have the strength of being biodegradable, biocompatible, and capable of loading hydrophilic or hydrophobic drugs to be released on demand. Inorganic NPs, which include silica, gold, iron oxide, and carbon-based structures (fullerenes, graphene oxide), offer stable platforms with shape control (spheres, rods, flowers) and outstanding physical performance of imaging, hyperthermia, and fragmentation. Hybrid or composite NPs make use of the two best of both worlds; a typical example is the magnetic hydrogel, which consists of the iron oxide NPs, which are embedded in a chitosan polymer mesh, allowing both magnetic retrieval and biocompatible coating of stone fragments. These materials are very important in terms of the strategic choice and design which must guarantee effectiveness, urine stability and eventual elimination by the body to reduce toxicity [5].
It is highly informed that the advanced nanostructural characterization of kidney stones themselves is the rational design of these nanotechnology interventions. Instead of bulk composition analysis (e.g., calcium oxalate, uric acid), other methods such as Small-Angle X-ray Scattering (SAXS) and Nitrogen Porosimetry identify the fine-scale nano-architecture of stones. SAXS can be used to determine the size, orientation and density of nanocrystalline domains and the organic matrix that bonds them, a blueprint of the integrity of stone in the nanoscale. Nitrogen porosimetry is used to map pore structure and surface area structure of the stone. This is a nano-structural intelligence that is vital. A heavy, high-density stone can be targeted using a disruptive strategy on the nanoscale (e.g., photothermal fragmentation with ultra-penetrative gold nanorods), whereas a porous, highly porous one can be targeted using a weakening strategy with a therapeutic nanofluid. The control of the nano-architecture enables engineers to control the size, shape, and surface chemistry of nanoparticles to enhance penetration, binding, and energy transfer. This intersection of high-value diagnostic characterization and high-precision nanomaterial production ultimately offers a new realm of customized, mechanism-based kidney stone disease management to turn the disease into a regular surgical disorder instead of a controlled, highly minimized nano-therapy [6-8].
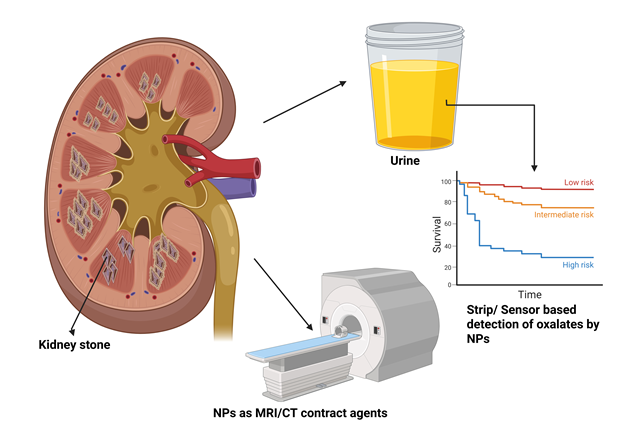
Fig: 1 Detection and monitoring of kidney stones using nanoparticles
MATERIAL & METHODS
A targeted literature search was conducted using electronic databases including Google Scholar, PubMed, Scopus, and ScienceDirect, covering publications published between 2017 and 2024.
Nanotechnology enabled diagnostics and monitoring
Nanotechnology in diagnostics and monitoring is transforming the kidney stone disease management, including by making it possible to detect risks earlier and giving an unprecedented level of detail to the imagery. This change in the treatment process of reactivity to proactive and individualized management is vital to the fight against the high recurrence rates that are typical of urolithiasis. The development of Biosensors to detect early risk is a paradigm shift to preventive care. Monitoring of lithogenic risk factors of the urine (increased calcium, oxalate, and uric acid) is the backbone of metabolic prevention. The conventional 24-hours urine collecting and lab testing are not only cumbersome but also gives out delayed results. Biosensors developed using nanotechnology are fast, sensitive and may be continuous. The electrochemical sensors have nanomaterial modified electrodes to sense a particular ion. As an illustration, a sensor that has been functionalized with oxalate oxidase is able to electrochemically detect the concentration of oxalate in urine with a high level of specificity. Colorimetric sensors are the visual or smartphone-readable sensor that produces a result upon color change of the target analyte with nanostructures to permit point-of-care or home testing. The reason why these devices are extraordinary sensitive is because of the nanomaterials that make them so. Measurement Semiconductor nanocrystals Quantum dots are size-tunable semiconductor fluorescence tags used as brilliant tags in multiplexed detection. Others More recently, more sophisticated morphologies such as vanadium disulfide (VS2) nanoflowers and iron molybdate (FeMoO4) nanospheres were developed. Such materials offer huge, catalytically active surfaces that boost the binding and detection of the target molecules to clinically relevant nanomolar concentrations and allow identifying the at-risk patients prior to the development of symptoms in very large initial stages [9].
In the field of Enhanced Medical Imaging, nanotechnology can be used to provide instruments to visualize the stones in a higher level of clarity and its composition, which directly influence treatment strategy. With regard to common anatomical imaging, such as Computed Tomography (CT) which is the current gold standard, high-density gold or bismuth-based nanoparticle contrast agents are being developed. Such agents can be functionalized to specifically target stone surfaces or renal tubules, which may enhance the contrast between stones and surrounding tissue, which will help to detect small or radiolucent stones such as uric acid-comprising stones. In the case of Magnetic Resonance Imaging (MRI), superparamagnetic iron oxide nanoparticles (SPIONs) serve as strong T2 contrast agents, providing an outstanding detail of soft tissues which may be used to examine related renal damage or inflammation due to chronic stone disease [10].
Besides better visualization of the anatomy, nanotechnology provides the ability to conduct the investigation of the stones directly in their location. This is done by Surface-Enhanced Raman Spectroscopy (SERS) which is an influential method in which the plasmonic nanoparticles (usually gold or silver) are presented close to a stone. These nanoparticles enhance significantly the weak intrinsic Raman signal of the molecular constitutes of the stone. What is obtained is a unique spectrogram of vibration fingerprints, which can tell the difference between calcium oxalate monohydrate and dihydrate, or trace bacteria in the rock of infection, or cystine with a very high degree of confidence. Combined with endoscopic probes, SERS-active nanoparticles can self-report compositional analysis in real-time and intraoperative environment to enable a urologist to adjust settings in lithotripsy (e.g., pulse energy, frequency) on a case-by-case basis, depending on the type of stone to select the most efficient and safe lithotripsy [11-13].
In combination, both of these diagnostic and monitoring platforms constitute an integrated nano-enabled strategy. Biosensors enable patient-initiated monitoring of urinary chemistry daily to determine dietary and medical treatment with the goal of avoiding the development of stones. SRS and advanced imaging will give clinicians quality compositional data of high-fidelity to select and implement the best procedure on the existing stones. This two-pronged nanotechnology solution-so that prevention and precision intervention can be given-would help ensure that the adult burden of kidney stone disease in the world is much lessened as the management has much better predictive approaches as well as individualized and efficient practices [14].
Therapeutic nanotechnologies for stone management
Emerging technologies in kidney stone surgery Nanotechnology-based novel fragmentation methods will radically alter the current surgical treatment of kidney stone and provide solutions to the historical shortcomings of mechanical laser lithotripsy and shock wave therapy. They do not operate via direct physical interaction or the high-energy usage of energy, but they utilize the special qualities of nanomaterials that can effectively disrupt the rocks with a high precision that has never been used before with minimum collateral damages. Photonic Lithotripsy A new concept of stone fragmentation. Its fundamental process is that it applies nanoparticles to the surface of the stone with the application of non-contact, and then exposes the surface to low-intensity, uncontacted laser [15]. The nanoparticles are localized transducers which absorb select wavelengths of light and transform the energy into powerful thermal or acoustic forces to mechanically rupture the stone internally. The process is proposed to decouple the fragmentation process and the direct laser-to-stone contact that can possibly be used to treat stones located in hard-to-reach calyces. It is important to select nanoparticle in accordance with the wavelength of the laser. The carbon-based nanomaterials, including polyhydroxy fullerenes (PHF), graphene oxide (GOX), and carbon nanotubes (CNT), are excellent near-infrared (NIR) absorbers [16]. They have high photothermal conversion efficiency, which results in high thermal intensity and explosive vaporization of water in the nano-pores of the stone under stress. Alternatively, nanoparticles made of gold such as nanospheres and nanorods are tunable plasmonic resonance. The size and shape can be optimally adjusted to give rise to their peak optical absorption (e.g., nanorods at 785 nm) to optimize the excitation of low-intensity, non-contact lasers in the near-infrared (i.e. 785 nm or 1320 nm). Evidence of in vitro experiments have shown the promising effectiveness of the method, with >70% of fragmented prevalent types of stones such as calcium oxalate monohydrate being reported. Notably, this success is enabled with laser power densities that are largely lower than those employed in conventional holmium:YAG lithotripsy, and therefore, by default, the risk of retrograde propulsion and ureteral injury is reduced. To supplement this free-standing approach is Nanofluid-Enhanced Laser Lithotripsy, a complementary approach, which is intended to improve the performance of the available clinical laser systems, and not to substitute them [17]. The mechanism corrects a underlying inefficiency of the traditional laser lithotripsy, that is, the loss of laser energy in the irrigant fluid and the poor absorption of some stone compositions. It is a method of spreading large absorbent nanoparticles into the regular saline irrigant that is administered when a ureteroscopy is being performed. As the surgical laser pulse passes through this so-called nanofluid, part of the light energy is absorbed by the suspended particles hence cutting down the attenuation of the pulse. More importantly, these nanoparticles settle on the surface of a stone and penetrate the stone surface forming localized absorption sites that significantly increase the absorption in the stone itself of the laser energy. The most important materials in this application are conducting nanoparticles made of polymer, which can be polyaniline based or PEDOT:PSS based. These organic semiconductors have high, broad-spectrum absorption over a relevant range of laser wavelengths and have good profiles of biocompatibility. The result of this improvement is far reaching. As it has been experimentally demonstrated, a 26-727% increase in the efficiency of stone ablation per laser pulse is possible when optimized nanofluid irrigant is present due to the composition of the stone and the laser parameters. This implies equal / higher fragmentation volume with less pulses and lower total energy which directly convert into shorter procedure times, reduced risk of thermal damage to the urothelium and hopefully, complete dusting of the stones [18-20].
Preclinical and clinical evaluation
In vitro testing and performance metrics: establishing proof of concept
The preclinical evaluation of nanotechnology for kidney stone management begins with rigorous in vitro testing, which establishes fundamental proof of concept, quantifies efficacy, and optimizes parameters before advancing to complex biological systems. These experiments are designed to mimic the clinical environment as closely as possible within a controlled laboratory setting.
Experimental setups: simulated urine and human stone samples
The second aspect that is important in the creation of clinically relevant data is the application of physiologically relevant testing conditions. The simulated urine solutions are used by the researchers with ion concentration (calcium, oxalate, phosphate, citrate), pH, and ionic strength equivalent to human urine. This is necessary since nanoparticles can, in a drastic difference in their performance, especially their stability, aggregation behavior and surface interactions, behave when in urine and when in pure water. As an example, a nanofluid optimized in deionized water can be aggregated and rendered useless instantly as it gets in the high-ionic-strength environment of urine. Human stone samples (obtained during surgery and categorized by composition (e.g., calcium oxalate monohydrate, uric acid, brushite)) will be used as the test substrates. The preservation of the complex nano-architecture, heterogeneity and mechanical properties which synthetic stones cannot reproduce completely is through the use of real stones. This is a requirement because a nanotechnology that is effective against porous uric acid could not be effective against dense and crystalline brushite since it is necessary to test on a library of stone types [21].
Efficacy assessment: core performance metrics
Therapeutic nanotechnologies aim at developing the maximum stone destruction or prevention, which is quantified through quantitative metrics. In case of fragmentation methods such as photonic lithotripsy or nanofluid-enhanced laser lithotripsy, the most important results are; Fragmentation Rate/Success: Percent (e.g. greater than 70) mass of the stone to be broken and the time taken to fully reach a breakage state. Particle Size Reduction: The end size distribution of particles, which would preferably give them a size so tiny (under 100 um) that they would pass by themselves rather than being so large and troublesome as chips. Sieving or dynamic image analysis is usually used to analyze this. Ablation Volume per Energy Unit: In the case of laser-based techniques, the measure is volumetric stone removal (mm3) per unit of laser energy incident. An enhancement of nanoparticle is also supported by statistically significant improvement of this ratio in comparison with the laser-only controls, showing an improvement in energy efficiency. In preventive or retrieval nanotechnologies, the measures become crystal growth growth and aggregation inhibition in metastable urine solutions, or percent capture efficiency of magnetic retrieval systems of fragments of different size [22].
Advanced characterization: understanding the mechanism
In addition to gross measures, advanced analysis software breaks down the mechanism of action down to a micro- and nanoscale level. Micro-Computed Tomography (Micro-CT) is indispensable in the non-destructive visualization of internal fracture network of a stone after treatment. It is capable of measuring the depth of crack propagation and will indicate whether nanoparticles enhanced deep and concentric cracking or if it was superficial surface ablation due to a laser alone. Scanning Electron Microscopy (SEM) allows the surface topography of the sample to be scanned with high resolution, showing the manner in which nanoparticles coating the stone, penetrating the porosity, or localized melting and spallation occur [23]. It is possible to use the Fourier-Transform Infrared Spectroscopy (FTIR) to identify any residual chemical or change on the surface of the stone or fragments after the intervention, ensuring that no undesired chemical products are obtained. It is a multi-modal characterization that fills the gap between observed efficacy and the underlying nanoscale physical event that directs the process of iterative redesign of the nanoparticles Fig.2.

Fig:2 Kidney targeted drug delivery Schematic mechanism.
Drug-carrying nanoparticles are conducted to the afferent arteriole through the renal artery, and are in the blood or filtered out of the blood by the kidneys in the glomerular capillaries to be processed. Renal elements like the endothelial cells, GBM and glycocalyx are all adjustable to help in the process of selecting NPs to be used in the process of filtration. After being filtered, NPs are able to respond to the podocytes within the lumen of the Bowman. The NPs are carried to the proximal tubule, where they are taken up by proximal epithelial cells and could be reabsorbed.
In vivo biocompatibility and safety evaluation: the paramount hurdle
Nanotechnology’s in vitro efficacy is meaningless without a comprehensive safety profile. For urological applications, this evaluation is particularly stringent due to the direct and prolonged contact with the sensitive urothelium lining the urinary tract.
Cytotoxicity assays: first line of safety screening
The first safety test is the cytotoxicity tests with the respective cell lines. The gold standard is immortalized human urothelial cells (e.g., SV-HUC-1, T24), since it is the initial exposure of the tissue. Nanoparticles are administered to cells at different concentrations and over different periods which reflect the possible clinical exposure. Viability is measured through tests such as MTT or LIVE/DEAD staining. More importantly, these tests should look at not only the pristine nanoparticles, but also any breakdown products and the treated "spent" nanoparticles once they have fulfilled their role (e.g. once they have been laser activated), since their properties could altered. Also, tests have to examine the induction of oxidative stress or release of pro-inflammatory cytokines, which might predetermine the appearance of fibrosis or structure [24].
Tissue response studies: assessing the integrated biological reaction
Cell data in vitro is not predictive of the more complicated tissue-level responses. Thus, it is necessary to study the tissue response in the correct animal model (usually, rodent or porcine). In technologies where intrarenal delivery is used (e.g., nanofluids, magnetic retrieval), the effects of the techniques on the acute and sub-chronic effects of the bladder and the urothelium of the upper urinary tract are studied. Animals are treated and histopathological examination of the animal after sacrifice. Investigators seek evidence of inflammation, erosion, hyperplasia or fibrosis of the urothelium and underlying smooth muscle. Pig models, based on their anatomic and physiologic parallel of the human kidneys and ureters are particularly useful in assessing the safety of the endoscopic delivery and irrigation procedures. The research on magnetic retrieval systems should also ensure that the magnetic forces applied do not lead to mechanical damage to the walls of the ureters or pelvis [25].
Biodistribution and clearance profiles: the ultimate fate of nanomaterials
To determine whether radiolabeled or fluorescently labelled nanoparticles accumulate in non-target organs, especially, the liver, spleen, and kidneys themselves, studies of biodistribution follow radiolabeled or fluorescently labelled nanoparticles over time. The desirable characteristics of a urologic nanoparticle are a quick and full excretion through the urine to reduce systemic exposures. Critical factors are size, surface charge and coating; smaller, neutral and negatively charged nanoparticles have higher chances to get filtered and excreted. In case of the nanoparticles that are not to be cleared (e.g., permanently entraped in a hydrogel to be retrieved by the fragments), long-term biostability and absence of degradation to toxic constituents shall be demonstrated. Knowledge of clearance pathways is not only a safety imperative but can be used to inform dosing and possible contraindications to patients with problems in renal or hepatic clearance [26].
Current status: a landscape of promise
The field currently is at the stage of predominantly in the proof-of-concept and preclinical stage. The highest technologies, including some nanofluid formulations and magnetic retrieval systems, are finishing all in vivo safety and efficacy research in large animals. None of the kidney stone fragmentation or kidney stone retrieval nanotechnology has been subjected to Phase I human clinical trials as of now so the field is about 5-10 years away before it can be used in large quantities by most clinical applications, should there be targeted investment and translational efforts [27].
Key challenges for translation
To bridge this translational gap, it is necessary to deal with interdependent scientific, manufacturing, and regulatory issues: Scalable and Reproducible Synthesis: The process of producing kilogram-sized batches of clinical drugs (and, in fact, at least 10-100 grams) is complicated by multi-step processes which are not economically and technically viable at laboratory-scale (producing milligrams). The transition of batch manufacturing to continuous flow manufacturing with a close control of nanoparticle size, shape, coating thickness, and functionalization is a significant engineering challenge. The standards of Good Manufacturing Practice (GMP) are required at the beginning of the process development. Sterilization and Stability: Nanomaterials are delicate to normal sterilization procedures. Autoclaving (heat and pressure) can also fuse the particles together, gamma irradiation can degrade coating of polymers or form free radicals, and ethylene oxide gas needs to be completely wiped out of porous nanostructures. One of the major non-trivial steps is the development of a terminal sterilization procedure that would not modify the main physicochemical and functional characteristics of the nanomaterial. Moreover, stability in a liquid or a lyophilized formulation in terms of long shelf-life (e.g., 24 months) should be established. Regulatory Pathways and Characterization: Nanotherapeutics are considered to be new chemical substances by regulatory agencies (FDA, EMA), and have to be exhaustively characterized. It is necessary to create a strong Critical Quality Attributes (CQA) dossier that will specify the acceptable measures of such parameters as particle size distribution, zeta potential, drug loading efficiency (if needed), sterility, endotoxin content, and impurity profiles. In the case of composite or hybrid materials, the characterization load is increased. The actual mechanism of action and main efficacy endpoint of clinical trials may be complicated, too, e.g. whether a nano-enhancer is a device that when added to existing laser can make it work better or is a drug that can biologically interact. Commercial and Clinical Adoption: Lastly, translation needs a good value presentation in order to be successfully translated to cross the barrier of clinical inertia. The technology should have proven to enhance patient outcomes (e.g. reduce recurrence, zero fragments), decreased the overall cost of the procedure or have a much shorter learning curve by the surgeons. A smooth integration into the current surgical processes (e.g., a nanofluid that is compatible with the existing laser systems and irrigants) will have fewer barriers to adoption than the platform that would need new capital equipment altogether [28-30].
Synthesis and design considerations
The engineering basis of useful and translational nanotechnology in management of kidney stones is the rational design of nanomaterials and sustainable synthesis of nanomaterials. This process consists of two very important and interdependent steps: the first step is strategic selection and functionalization of materials to serve specific purposes in the specific biological and physicochemical environment of the urinary tract; the second step involves the development of manufacturing processes that are safety-friendly, scalable, and environmentally friendly.
Material selection and functionalization: engineering for precision in the renal environment
The choice of core material of nanoparticle used and its surface functionalization depends on the particular task of therapeutic or diagnostic, fragmentation, retrieval or drug delivery. One of the major design approaches is the coating of the nanoparticles on their surfaces with targeting moieties to bind to the stones. This guarantees high localization of the same in the area of pathology and maximization of effectiveness and minimization of the exposure to the system. In the case of the most used calcium based stones, carboxylic acid groups (-COOH) or phosphonate groups are functionalized onto nanoparticles. These groups are high-affinity multidentate Chelation of calcium ions on the surface of the stone, which is effective in the anchoring of the nanoparticle. In the case of uric acid stone, the required chemistry is different, since nanoparticles can be modified with polymers with amine moieties, which are capable of building hydrogen bonds with the carbonyl and imide groups of uric acid. This molecular recognition idea is what turns nanoparticles into active, targetable therapeutics capable of localizing itself on stones in even diluted urine flow, which is the most significant demand of effective photonic lithotripsy or local drug delivery. In addition to targeting, thorough optimization of intrinsic physicochemical characteristics is required, such as size, surface charge and hydrophobicity, to achieve performance and biocompatibility during renal use. The most important parameter is probably size. Nanoparticle should be small (usually less than 100 nm) because it should have a potential to penetrate the nanoporous structure of the stone and also, to prevent a quick clearance by the reticuloendothelial system in case it is introduced systemically. When it comes to intraoperative irrigation (e.g. nanofluids) a small bit larger size may be tolerated, although it must be stable against aggregation. Zeta potential, which is the measure of surface charge is the determiner of colloidal stability and biological interactions. A negative or positive charge that is very strong (generally more than -30 mV) inhibits aggregation of ionic fluids such as urine by repulsion due to electrostatic charges. Also, charge can affect the interaction with the anionic glycosaminoglycan layer of the healthy urothelium; a negative charge might allow it to exhibit stealth, as well as slightly negative charge may reduce the non-specific adhesion, whereas a positive charge would be exploited to bind negatively charged stone or cellular surface, although attention is paid to possible cytotoxicity. Control of protein adsorption is by engineering hydrophobicity using surface coatings (e.g. polyethylene glycol or PEG). The protein corona is quickly deposited on hydrophobic surfaces in the protein-rich urine environment, and may induce alteration of the desired function of the nanoparticle and unwanted immune response. A PEGylated hydrophilic coating is thus common so as to increase stability, increase circulation as well as make the nanoparticle work as intended [31].
Green synthesis and sustainable nanomanufacturing: a path to clinical and environmental safety
Although the conventional techniques of synthesis can make high quality nanomaterials, they usually make use of toxic reducing agents, consume high levels of energy and the products are also hazardous wastes. In medical use, this is a twofold issue: toxic residues left on the surface of the nanoparticle would compromise the biocompatibility, and the scale effect makes the knowledge of environmentally friendly production difficult to achieve [32]. This has motivated the accelerated growth of green synthesis and sustainable nanomanufacturing that involve use of biological resources as green factories. One of the best examples is the synthesis is a plant synthesis of zinc oxide nanoparticles (ZnO NPs) using plant extracts of plants such as Cymbopogon proximus (a type of lemongrass). Aqueous plant extracts containing abundant phytochemical compounds, including polyphenols, flavonoids and terpenoids, play a dual role in this process [33]. They are benign reducing agents which convert zinc salts into zinc oxide nuclei and natural capping agents which stabilize the growing nanoparticles and functionalize their surface. The given one-pot synthesis technique is commonly carried out at room temperature and pressure which minimizes energy input considerably. The green-synthesized ZnO NPs have inherent benefits to be used in medicine. The phytochemical capping coating usually imparts superior biocompatibility and inherent biological functions, including antioxidant and anti-inflammatory action, which is very desirable in inhibiting the inflammatory cascade in the formation and recurrence of stones [34]. It has been demonstrated that ZnO NPs produced through Cymbopogon proximus have anti-lithogenic properties in animal models that reduce crystal deposition and oxidative stress in renal tissue-effectiveness that can be partly explained by their surface chemistry synthesized by green synthesis. Moreover, this technique is compatible with the concepts of sustainable chemistry, in which hazardous substances are minimized in the initial stages, which makes it easier to purify, has better safety profiles, and has a simpler way to be approved by the regulatory authorities [35].
CONCLUSION
The discussion of nanotechnology in the treatment of kidney stones indicates a sector of phenomenal innovation that is at the crossroads of materials science, urology, and molecular diagnostics. Nano-engineered solutions provide a promising, multi-faceted approach to dismantle the problems of urolithiasis that have endured over time: not only can they allow to monitor the disease and diagnose it more accurately, but also can also allow to support more effective, less invasive, more efficient treatment and cure the cause of its recurrence. The paradigm shift is based on the reactive, mechanical model of stone removal to the predictive, preventive, and personalized approach. The ability of nanoscale biosensors and advanced imaging agents to provide unprecedented data enables cases to be intervened at earlier stages giving patients and clinicians power. Such therapeutic approaches as photonic lithotripsy and nanofluid-enhanced procedures prove that the process of surgery may be made much more efficient, and the collateral tissue injury may be minimized. Moreover, the introduction of the magnetic retrieval systems and specific anti-lithogenic nanoformulations address directly the two issues of residual fragments and biochemical predisposition in an attempt to eliminate the phenomenon of recurrence. Nevertheless, the path between the impressive laboratory results and the popular clinical use is not smooth and is full of difficulties. The present situation in the field is well in the proof-of-concept and preclinical phases. The road to translation is characterized by a valley of death in which scientific promise has to be answered by high demands of practicality. The key to success is to overcome interrelated issues: scaling up, reproducible, and green synthesis; long-term stability and sterile formulations; getting around the complex regulatory environment of novel nano-entities; and lastly, proving undeniable clinical usefulness to obtain acceptance and incorporation into current work processes by surgeons.
REFERENCES

Samruddhi Patil, Omprakash Swami, Mohd. Zubair Arshad, Rashmi Kumari, Hemant Chaudhari, Divya Shikha, Design and Evaluation of Nanotechnology Approaches for Kidney Stone Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 496-509. https://doi.org/10.5281/zenodo.18480983
 10.5281/zenodo.18480983
10.5281/zenodo.18480983