
We use cookies to ensure our website works properly and to personalise your experience. Cookies policy
Genesis Institute of pharmacy, Radhanagari.529/30, Near Gaibi Titta, Radhanagari Road, Opposite to Bharat Petroleum, Tal-Radhanagari, Dist-Kolhapur Pin: 416212
This review examines the diabetes mellitus epidemic across various geographic regions, highlighting significant disparities in prevalence rates. The Western Pacific region reports the highest number of adults diagnosed with diabetes, with a staggering prevalence rate of 37.5%, while the Middle East and North Africa exhibit the highest prevalence of adult diabetes at 10.9%. A comparative analysis of the different types of diabetes mellitus—namely type 1, type 2, and gestational diabetes—emphasizes their genetic underpinnings, etiological factors, and diagnostic criteria. Recent advancements in molecular genetics have provided insights into the early identification of type 1 diabetes (T1D), which can be detected up to two years prior to the onset of abnormal insulin secretion, while the pathophysiology of type 2 diabetes (T2D) is characterized by the impairment of insulin secretion in response to fluctuating insulin sensitivity. Additionally, gestational diabetes mellitus (GDM), defined as hyperglycemia occurring during pregnancy, is highlighted, with an estimated 7% of pregnancies affected, typically diagnosed in the second and third trimesters. This comprehensive review underscores the urgent need for targeted interventions and research to address the evolving landscape of diabetes mellitus globally.
The peculiarities of the diabetes mellitus epidemic in various geographic locations are the main subject of this review. While the Western Pacific region has the biggest number of adults with a diagnosis and includes nations with a prevalence rate of 37.5%, the Middle East and North Africa region has the highest prevalence of adult diabetes (10.9%). The many types of diabetes mellitus, including type 1, type 2, gestational diabetes, and others, are compared in terms of their genetic components, etiology, and diagnostic standards.
In recent years, the molecular genetics of diabetes has garnered significant attention from numerous leading researchers and research teams within the biomedical sector. This review encompasses a wide range of mutations and single nucleotide polymorphisms in genes that are integral to various processes and pathways related to glucose metabolism, as well as the development, regulation, and functionality of pancreatic cells at multiple levels. Here, we provide a concise overview of the key advancements in our molecular understanding of diabetes, particularly in relation to its different types, compared to previous knowledge in this area. Despite the wealth of data accumulated at both molecular and cellular levels, the mechanisms underlying the onset of diabetes and its complications remain incompletely understood. Clearly, further in-depth research is essential in this domain, with the ultimate aim of enhancing diagnostic methods, therapeutic strategies, and reducing the risk of chronic complications. [1]
Diabetes in India:
Diabetes is increasingly becoming a significant issue in India, with recent estimates indicating that around 285 million individuals worldwide (6.6%) aged between 20 and 79 were anticipated to have diabetes in 2010. This figure is projected to escalate to 438 million (7.8%) by 2030 among adults. India has unfortunately earned the designation of the "diabetes capital of the world," as it has the highest number of diabetes cases globally. According to the International Diabetes Federation's Diabetes Atlas 2006, the current diabetic population in India, estimated at 40.9 million, could increase to 69.9 million by 2025 in the absence of immediate preventive measures. "Asian Indian Phenotype" refers to certain biochemical and clinical characteristics that are commonly seen among Indians, including greater insulin resistance, decreased adiponectin, elevated levels of high-sensitivity C-reactive protein, and more belly fat despite a lower body mass index. Among urban dwellers, dietary changes and a decline in physical activity are often associated with the rising incidence of diabetes mellitus. With over 62 million individuals diagnosed with diabetes, there may be an epidemic in India right now. India topped the global diabetes case count in 2000 with 31.7 million patients. The United States ranked third with 17.7 million, followed by China with 20.8 million. By 2030, there will likely be 366 million diabetics worldwide, up from 171 million in 2000, with India expected to have the largest growth, according to research by Wild et al. According to estimates, by 2030, up to 79.4 million Indians may develop diabetes, and China and the US are also predicted to see sharp increases in the number of diabetics. [2]
Diabetes:
A group of metabolic conditions characterized by increased blood glucose levels is known as diabetes mellitus, or simply diabetes. The body's insufficient production of insulin or the cells' insufficient response are the two causes of this condition. Characterized by common symptoms include polyphagia (strong hunger), polydipsia (extreme thirst), and polyuria (frequent urine). [3]
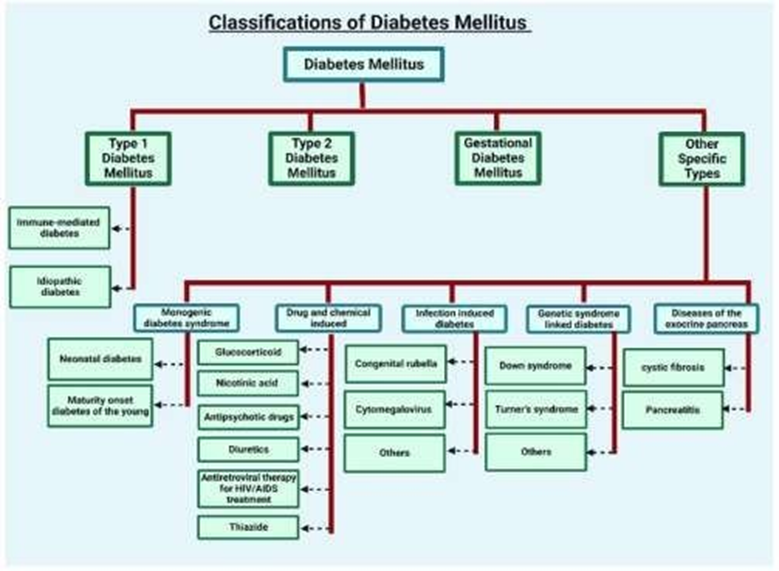
Classification:
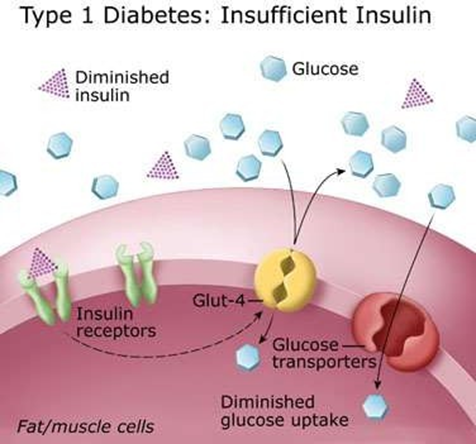
Type 1 diabetes:
It is possible to identify type 1 diabetes (T1D) well before the aberrant insulin secretion starts, as the condition gradually deteriorates for at least two years before a diagnosis is made. The sensitivity of β-cells to glucose also decreases throughout this time. A potential compensatory mechanism is suggested by the fact that the following insulin response frequently rises as the first insulin response declines. Insulin responsiveness declines more quickly in the early post diagnosis period. Insulin secretion decreases in two phases within the first few years after diagnosis, with the first year experiencing a larger reduction than the second. Following diagnosis, there may be a few years of decreased insulin secretion before there is little to no insulin produced at all. Even if blood glucose levels stay within the normal range, elevated levels can indicate type 1 diabetes. The beginning of type 1 diabetes is characterized by significant variations in blood glucose levels. In at-risk people, the use of metabolic markers like dysglycemia may help anticipate when diabetes will manifest. Additionally, to improve predictive accuracy, risk assessments can make use of variations in glucose and C-peptide levels.
Type 2 diabetes:
Insulin secretion impairment is a key component of the pathophysiology of type II diabetes (T2D). The amount of insulin secreted to maintain proper glucose levels varies greatly depending on insulin sensitivity. The disposition index serves as an indicator Type 2 diabetics also exhibit a lower disposition index, which hinders their ability to properly increase insulin production in response to insulin resistance. Although lean control subjects with insulin-sensitive type 2 diabetes may have higher insulin levels than obese patients with insulin-resistant type 2 diabetes, these levels are nonetheless insufficient.
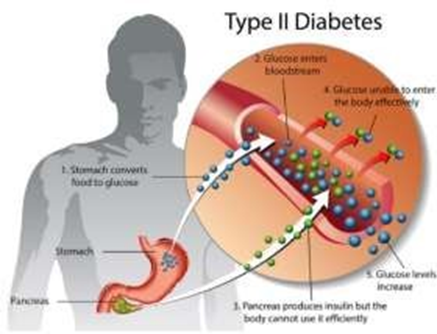
Glucose stimulation results in a marked reduction or absence of the early stage of insulin production. A higher ratio of proinsulin to insulin (C-peptide) is seen in patients with Type 2 Diabetes (T2D). Moreover, they have significantly reduced capacity to increase insulin responses to stimuli other than glucose and to manufacture insulin at optimal levels, especially during hyperglycemia. The management of hyperglycemia usually becomes increasingly difficult as time goes on. An further noteworthy aspect of T2D progression is a progressive loss of functioning.
Classification:
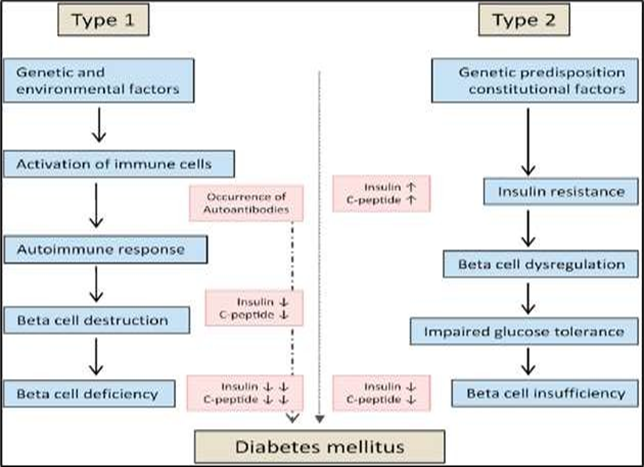
Pathophysiology:
Gestational diabetes mellitus:
The first diagnosis of hyperglycemia in pregnant women is gestational diabetes mellitus (GDM), another name for hyperglycemia in pregnancy. Although GDM can develop at any moment during pregnancy, it is most commonly identified during the second and third trimesters. The American Diabetes Association estimates that 7% of pregnancies are affected with GDM. Women who have type 2 diabetes mellitus and their children are at a higher risk of developing the disease in the future Complications linked to GDM may include hypertension, preeclampsia, and hydramnios, which can increase the chances of requiring surgical procedures. Furthermore, the fetus may be larger than average, leading to macrosomia and potential congenital anomalies. After birth, these infants may experience respiratory distress syndrome and are at an elevated risk of obesity during their infantile and teenage years. Factors that elevate the danger of GDM include older motherly stage, overweightness, excessive weight gain during gravidness, a history of hereditary anomalies in previous children, death of a fetus, and a domestic history of diabetes.
Monogenic Diabetes
Monogenic Diabetes is a type of diabetes that results from a singular hereditary change in an autosomal leading genetic factor. Prominent examples of this condition include neonatal diabetes mellitus besides maturity-onset diabetes of the early (MODY). This form of diabetes signifies near 1 to 5% of all diabetes belongings. MODY is inherited and frequently offerings itself earlier the stage of 25.
Secondary diabetes results from side effects related to other medical conditions that affect the pancreas, such as pancreatitis, hormonal imbalances similar to Cushing's disease, or the use of specific drugs, such as corticosteroids. [4]
Preventive Drugs for Diabetes Verbal and injectable non-insulin pills designed to advance body fluid glucose organization are listed in the following table. The scenario explains the types of pharmaceuticals, the specific medications in each category, their effects, any side effects, and safety factors. [5]
Table no.1Effects and Adverse Effect: [6]
|
Substance Group |
Particular Substance |
Impacts
|
Consequences |
Keeping safe |
|
Biguanides
|
Metformin
|
decrease in HbA1c values Weight loss decreased cancer incidence Reduced risk of heart attacks |
Increased severity of gastrointestinal diseases Increased reversibility of vitamin B12 insufficiency |
No one |
|
Glinides |
Repaglinide Nateglinide |
Reduction in HbA1c Rise in body weight |
Rise in hypoglycaemia Surge in headache frequency Increased cases of upper respiratory tract infections |
Nothing |
|
Alpha- Glucosidase inhibitors |
Acarbose
|
Reduction in HbA1c levels Decrease in body weight |
There is a rise in serum transaminases (AST, ALT) in patients with gastrointestinal disorders. |
None |
|
SGLT2-I |
Empagliflozin Dapagliflozin Canagliflozin |
HbA1c levels decreased Body weight reduced Blood pressure lowered Major adverse cardiovascular events diminished Fewer hospitalizations for heart failure Progression of renal disease slowed |
The occurrence Of diabetic ketoacidosis has risen. There is a rise in genital infections. Urinary tract infections are also elevated. Hypovolemia is increased. Acute kidney injury is heightened, Related to hypovolemia. Canagliflozin: The risk of amputation is elevated. The probability of bone fractures has increased. |
None |
A recent study into the molecular mechanisms of insulin interaction has revealed the existence of a small particle known as Co-Insulin. This compound preferentially bind toward insulin rather than to the insulin receptor (IR). [7] With a mass of 222 Da, Co-Insulin attaches to a specific site on the A-chain of insulin, promoting the interaction between the A and B chains, which in turn activates the insulin receptor. This activation initiates a series of events, including the autophosphorylation of the insulin receptor, the phosphorylation of IRS proteins, and insulin actions that manifest as both 'Immediate' and 'Delayed' responses. The 'Immediate' response is marked by the well-known hypoglycemic effect mediated by Glut-4, influenced by a phosphorylated IRS molecule. Conversely, the 'Delayed' response entails the translocation of certain wreckages of the phosphorylated insulin receptor into the nucleus, potentially aided through additional phosphorylated IRS. It is important to highpoint that Co-Insulin purposes solely by activating insulin signaling pathways. This groundbreaking research raises the possibility of investigating whether alike unimportant molecules could also enhance the effects of other peptide hormones in mammals, potentially leading to new diabetes treatment strategies. [8]
Genetic Syndromes Related to Diabetes:
MODY refers to a collection of monogenic methods of diabetes that typically manifest before the age of 25. This disorder is produced by changes cutting-edge a single genetic factor, which affects either the production of insulin or its effectiveness. Notable mutations include: - HNF1A (MODY3): This is the most common mutation associated with MODY, which hinders the pancreas's ability to produce insulin. - HNF4A (MODY1): This gene is essential for regulating insulin secretion and glucose metabolism. - Glucokinase (MODY2): Mutations in this gene result in mild hyperglycemia, often detected during childhood. [9]
Klinefelter syndrome is a chromosomal anomaly in males characterized by the presence of an extra X chromosome. This condition is allied by an augmented jeopardy of type 2 diabetes due to factors such as insulin resistance and obesity. Mechanisms: The testosterone deficiency linked to Klinefelter syndrome contributes to obesity, particularly the accumulation of visceral fat, which exacerbates insulin resistance and raises the likelihood of developing diabetes. [10]
Down syndrome, or trisomy 21, is related with an advanced danger of developing type 2 diabetes, particularly in adulthood. Insulin resistance is a significant factor in this increased risk. Mechanisms: Individuals with Down syndrome often face obesity, thyroid dysfunction, and other metabolic disorders that heighten their vulnerability to diabetes. [11]
Turner condition is a chromosomal disorder affecting ladies, linked by an augmented hazard of type 2 diabetes, especially cutting-edge those who are obese or have other metabolic issues. Mechanisms: Individuals with Turner syndrome frequently experience growth hormone deficiency and hypothyroidism, which may lead to heightened insulin resistance. [12]
Prader-Willi condition is a hereditary disorder marked by obesity, developmental delays, and hyperphagia, all of which significantly increase the likelihood of developing type 2 diabetes. Mechanisms: Those affected by Prader-Willi syndrome frequently encounter insulin resistance, which is likely a consequence of obesity and hormonal imbalances. [13]
The condition affects both the lungs and the digestive system. As it progresses, it may result in cystic fibrosis-related diabetes (CFRD), which shares characteristics of together category 1 and category 2 diabetes. The underlying mechanisms embrace pancreatic damage leading to insulin deficiency and resistance, alongside chronic inflammation and high glucose levels that may exacerbate insulin resistance. [14]
Dietary Management:
Pharmacological Treatments
Continuous Glucose Monitoring (CGM): CGM devices enable continuous observation of glucose levels, allowing for more accurate adjustments to insulin dosages. [16]
In individuals with obesity and Type 2 diabetes, bariatric surgery, including procedures like gastric bypass, has proven to be effective in enhancing or potentially curing diabetes by promoting weight loss and altering gut hormone levels. [18]

CONCLUSION:
In conclusion, this review examines the diabetes mellitus epidemic, revealing disparities in prevalence rates across different regions. The Western Pacific region reports a staggering 37.5% prevalence rate, while the Middle East and North Africa exhibit the highest prevalence at 10.9%. The analysis of type 1, type 2, and gestational diabetes emphasizes genetic underpinnings, etiological factors, and diagnostic criteria. Recent advancements enable early detection of type 1 diabetes (T1D), while impaired insulin secretion characterizes type 2 diabetes (T2D). The review also highlights gestational diabetes mellitus (GDM), affecting an estimated 7% of pregnancies, and underscores the urgent need for targeted interventions and research globally.
REFERENCES





Ritesh Telavekar*, Harshad Patil, Umesh Kolap, Dr. Shobharaj Malavi, Dr. Pratik Maske, Diabetes Mellitus Prevalence and Diagnostic Advances, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 2851-2860. https://doi.org/10.5281/zenodo.15271477
 10.5281/zenodo.15271477
10.5281/zenodo.15271477